
Segregated by Wealth, Health, and Development: An Analysis of Pre-School Child Health in a Medium-Sized German City

 ,
,
Abstract
1. Introduction
1.1. The School Entry Examination
1.2. Aim of the Study
2. Materials and Methods
2.1. Data
2.2. Variables
2.3. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics of the Study Population
3.2. Health Disparities across the Quarters
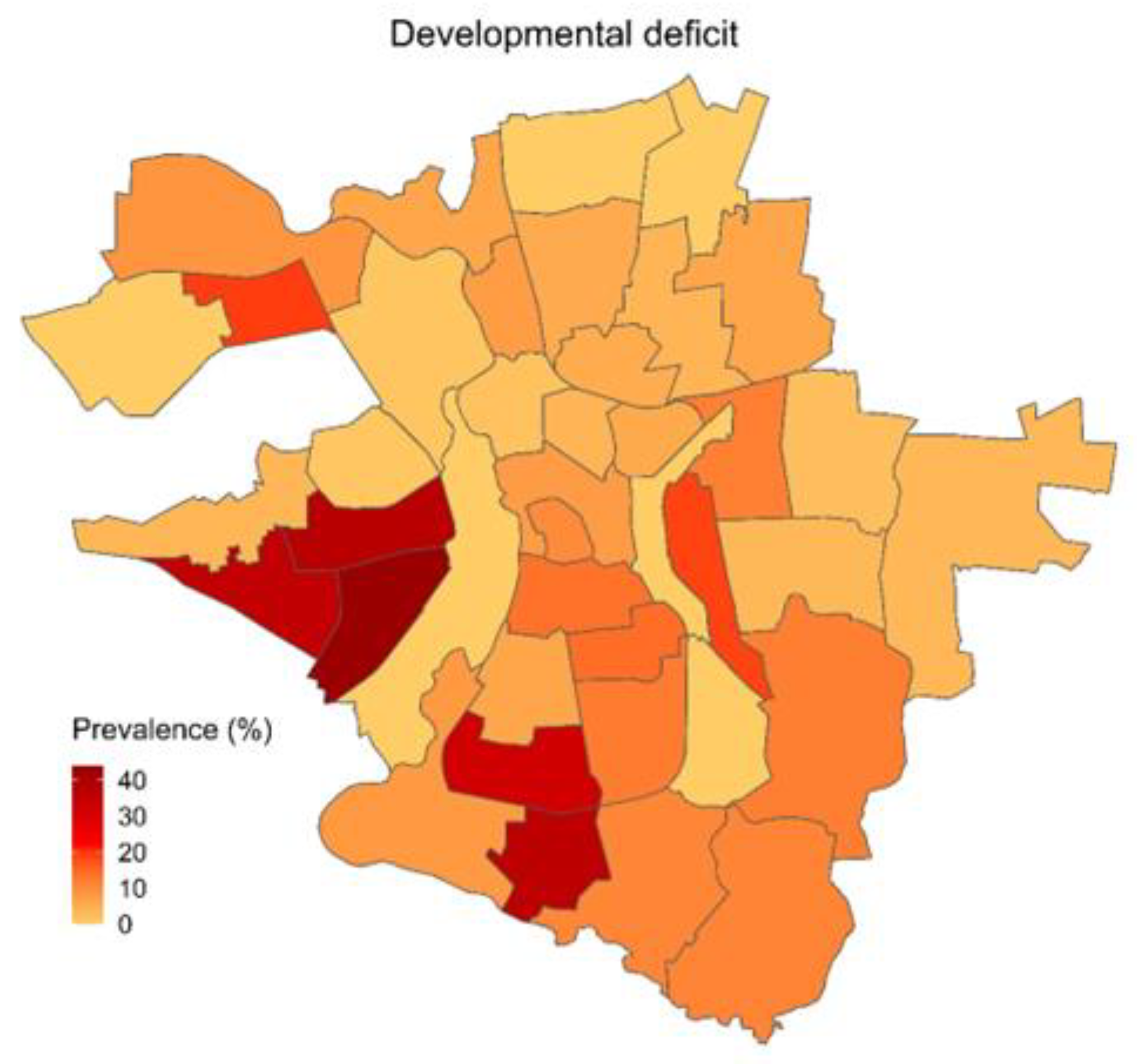
3.2.1. Developmental Tests
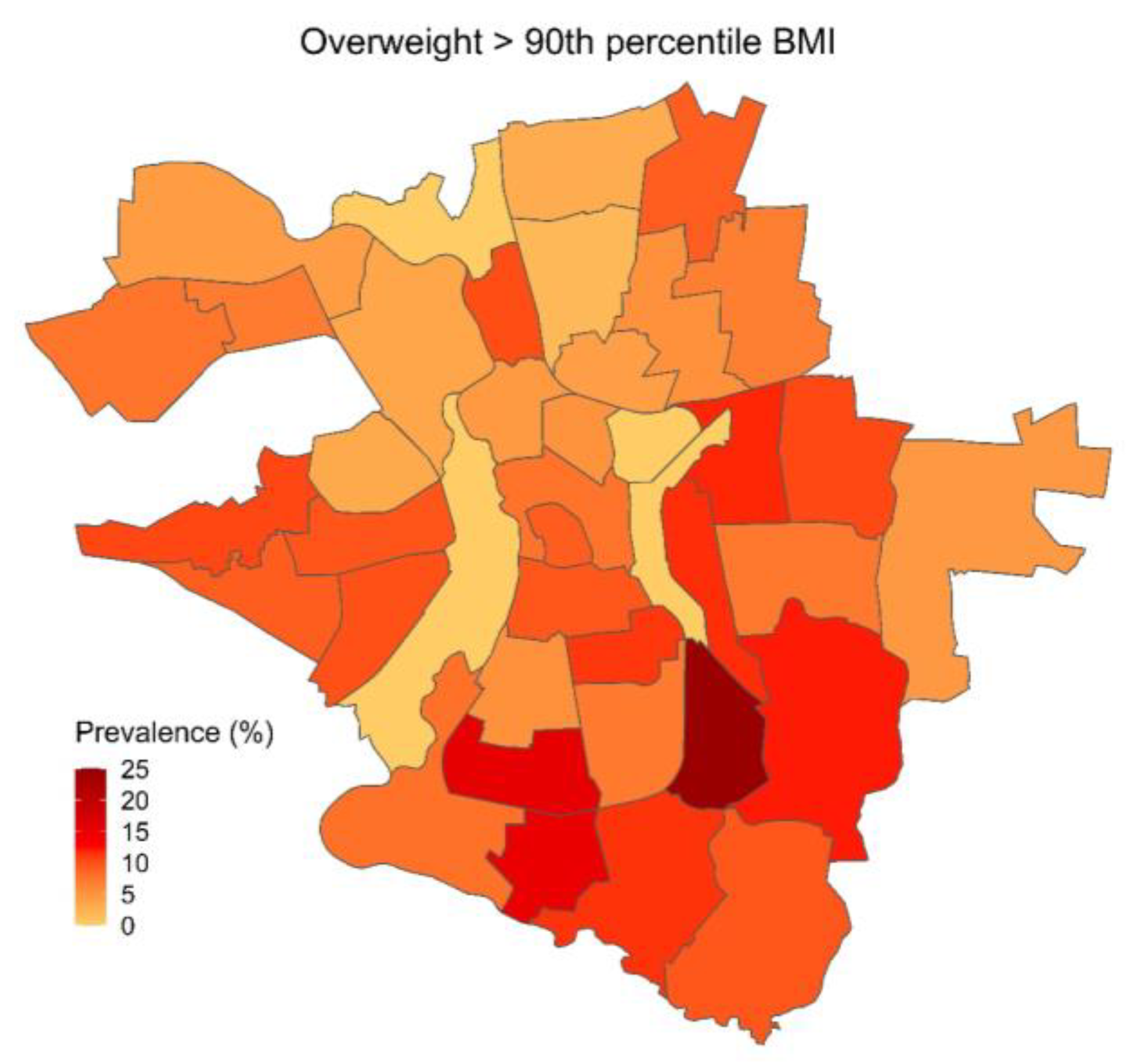
3.2.2. Physical Risk Factors
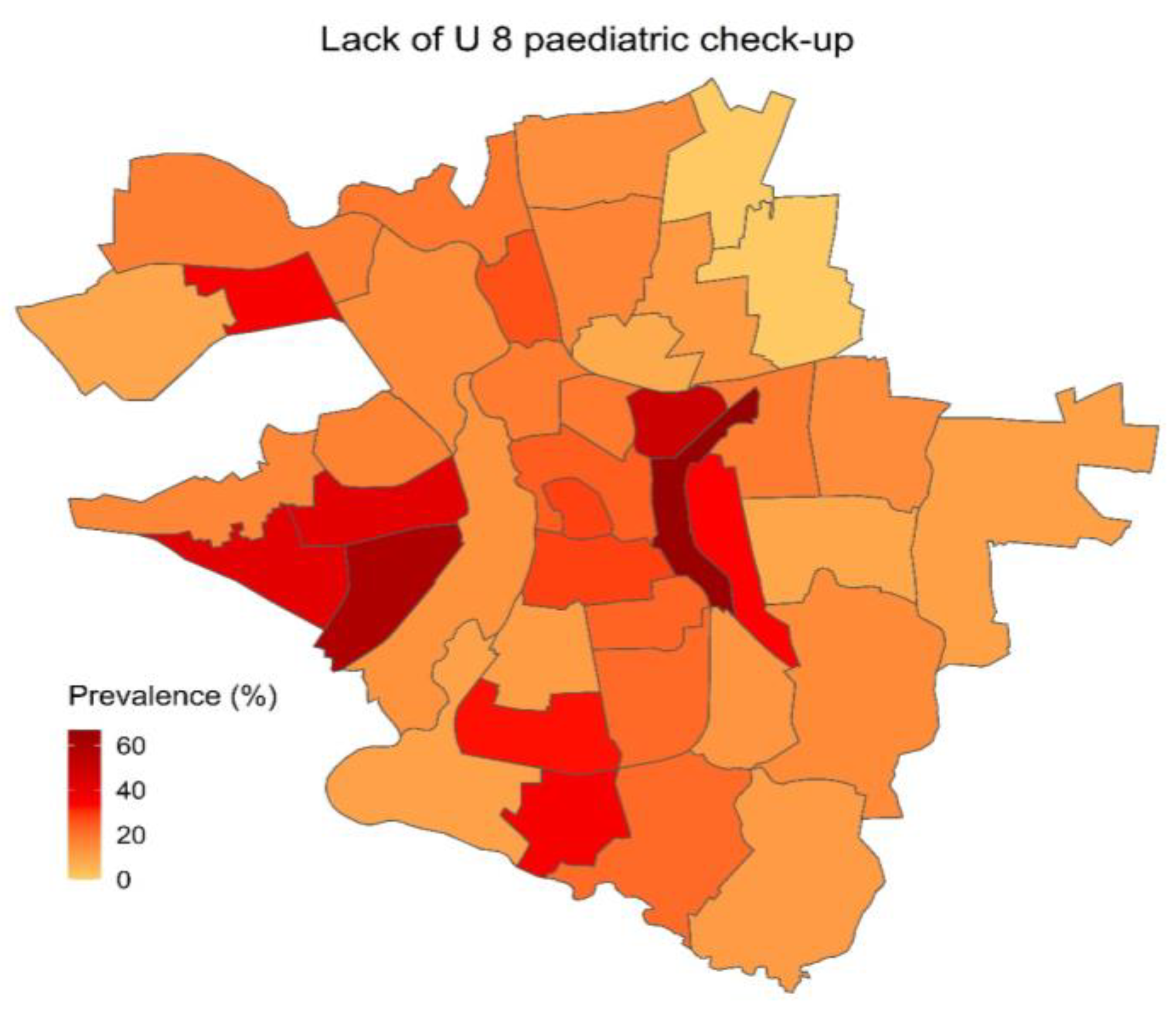
3.2.3. Utilization of Health Care and Social Institutions
3.3. Regression Results
4. Discussion
4.1. Residence in Neighborhoods with High Socioeconomic Burden and Perinatal Parameters
4.2. Growing up in a Deprived Environment
4.3. The Potentially Mitigating Role of Social Institutions and Healthcare
4.4. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of In Utero and Early-Life Conditions on Adult Health and Disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef]
- Shaw, S.H.; Herbers, J.E.; Cutuli, J.J. Medical and Psychosocial Risk Profiles for Low Birthweight and Preterm Birth. Women’s Health Issues 2019, 29, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Brumberg, H.L.; Shah, S.I. Born Early and Born Poor: An Eco-Bio-Developmental Model for Poverty and Preterm Birth. J. Neonatal-Perinat. Med. 2015, 8, 179–187. [Google Scholar] [CrossRef]
- Raphael, D. Poverty in Childhood and Adverse Health Outcomes in Adulthood. Maturitas 2011, 69, 22–26. [Google Scholar] [CrossRef]
- Bradley, R.H.; Corwyn, R.F. Socioeconomic Status and Child Development. Annu. Rev. Psychol. 2002, 53, 371–399. [Google Scholar] [CrossRef] [PubMed]
- Duval, E.R.; Garfinkel, S.N.; Swain, J.E.; Evans, G.W.; Blackburn, E.K.; Angstadt, M.; Sripada, C.S.; Liberzon, I. Childhood Poverty Is Associated with Altered Hippocampal Function and Visuospatial Memory in Adulthood. Dev. Cogn. Neurosci. 2017, 23, 39–44. [Google Scholar] [CrossRef]
- Hair, N.L.; Hanson, J.L.; Wolfe, B.L.; Pollak, S.D. Association of Child Poverty, Brain Development, and Academic Achievement. JAMA Pediatr. 2015, 169, 822. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Hurrelmann, K. (Eds.) Soziologie von Gesundheit und Krankheit; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2016; ISBN 9783658110093. [Google Scholar]
- Richter, M.; Hurrelmann, K. (Eds.) Gesundheitliche Ungleichheit; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2006; ISBN 9783531149844. [Google Scholar]
- Factsheet-Neue Zahlen zur Kinder- und Jugendarmut: Jetzt Braucht es die Kindergrundsicherung. Available online: https://www.bertelsmann-stiftung.de/de/themen/aktuelle-meldungen/2023/januar/neue-zahlen-zur-kinder-und-jugendarmut-jetzt-braucht-es-die-kindergrundsicherung (accessed on 16 April 2023).
- Ärzteblatt, D.Ä.G. Redaktion Deutsches Mehr als Jedes Vierte Kind in Europa von Armut Bedroht. Available online: https://www.aerzteblatt.de/nachrichten/69834/Mehr-als-jedes-vierte-Kind-in-Europa-von-Armut-bedroht (accessed on 16 April 2023).
- Halle (Saale)-Händelstadt: Bevölkerungsprognose 2030. Available online: https://m.halle.de/de/Verwaltung/Stadtentwicklung/Bevoelkerungsprognos-08622/ (accessed on 16 April 2023).
- Tagesschau.de Studie zur Kinderarmut-Arm Bleibt Arm. Available online: https://www.tagesschau.de/inland/kinderarmut-deutschland-101.html (accessed on 16 April 2023).
- Bernt, M.; Hausmann, P. Studie Zur. Kleinräumlichen Untersuchung Sozialstruktureller Veränderungen in Halle (Saale); Leibnitz Institut für Raumbezogene Sozialforschung: Erkner, Germany, 2019. [Google Scholar]
- Fischer, A.; Schulte, T.; Brüwer, O.; Lorenz, I. Entwicklungs- Und Handlungskonzept Für Eine Gesundheitsfördernde Stadtteilentwicklung in Billstedt Und Horn Kleinräumige Analyse Der Bedarfssituation; OptiMedis AG: Hamburg, Germany, 2015. [Google Scholar]
- Bopp, A.; Schmidt-Troschke, S. Gesundheit Für Billstedt/Horn" in Hamburg: Ein Gesundes Projekt Für Einen Benachteiligten Stadtteil; Gesundheit Aktiv: Das Magazin: Berlin, Germany, 2017. [Google Scholar]
- Shankardass, K.; Jerrett, M.; Dell, S.D.; Foty, R.; Stieb, D. Spatial Analysis of Exposure to Traffic-Related Air Pollution at Birth and Childhood Atopic Asthma in Toronto, Ontario. Health Place 2015, 34, 287–295. [Google Scholar] [CrossRef]
- He, M.; Tucker, P.; Irwin, J.D.; Gilliland, J.; Larsen, K.; Hess, P. Obesogenic Neighbourhoods: The Impact of Neighbourhood Restaurants and Convenience Stores on Adolescents’ Food Consumption Behaviours. Public Health Nutr. 2012, 15, 2331–2339. [Google Scholar] [CrossRef]
- Algren, M.H.; Ekholm, O.; Nielsen, L.; Ersbøll, A.K.; Bak, C.K.; Andersen, P.T. Associations between Perceived Stress, Socioeconomic Status, and Health-Risk Behaviour in Deprived Neighbourhoods in Denmark: A Cross-Sectional Study. BMC Public Health 2018, 18, 250. [Google Scholar] [CrossRef]
- Wahl, G. Handreichung Für Die Schuleingangsuntersuchung in Sachsen-Anhalt (Auszug); Landesamt für Verbraucherschutz Sachsen-Anhalt: Dessau-Roßlau, Germany, 2018. [Google Scholar]
- Führer, A.; Tiller, D.; Brzoska, P.; Korn, M.; Gröger, C.; Wienke, A. Health-Related Disparities among Migrant Children at School Entry in Germany. How Does the Definition of Migration Status Matter? Int. J. Environ. Res. Public Health 2019, 17, 212. [Google Scholar] [CrossRef] [PubMed]
- Führer, A.; Wienke, A.; Tiller, D. Die Schuleingangsuntersuchung als subsidiäre Vorsorgeuntersuchung: Eine risikobasierte Herangehensweise. Präv. Gesundh. 2019, 14, 198–204. [Google Scholar] [CrossRef]
- Führer, A.; Wienke, A.; Wiermann, S.; Gröger, C.; Tiller, D. Risk-Based Approach to School Entry Examinations in Germany—A Validation Study. BMC Pediatr. 2019, 19, 448. [Google Scholar] [CrossRef]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; Von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Mon. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef]
- Bensley, J.G.; De Matteo, R.; Harding, R.; Black, M.J. The Effects of Preterm Birth and Its Antecedents on the Cardiovascular System. Acta Obstet. Et Gynecol. Scand. 2016, 95, 652–663. [Google Scholar] [CrossRef] [PubMed]
- Jakubowski, K.P.; Cundiff, J.M.; Matthews, K.A. Cumulative Childhood Adversity and Adult Cardiometabolic Disease: A Meta-Analysis. Health Psychol. 2018, 37, 701–715. [Google Scholar] [CrossRef]
- Rosenkötter, N.; Van Dongen, M.C.J.M.; Hellmeier, W.; Simon, K.; Dagnelie, P.C. The Influence of Migratory Background and Parental Education on Health Care Utilisation of Children. Eur. J. Pediatr. 2012, 171, 1533–1540. [Google Scholar] [CrossRef]
- Böhm, A.; Ellsäßer, G.; Lüdecke, K. Der Brandenburger Sozialindex: Ein Werkzeug für die Gesundheits- und Sozialberichterstattung auf Landes- und kommunaler Ebene bei der Analyse von Einschülerdaten. Gesundheitswesen 2007, 69, 555–559. [Google Scholar] [CrossRef]
- Janghorbani, M.; Stenhouse, E.; Millward, A.; Jones, R.B. Neighborhood Deprivation and Preterm Birth in Plymouth, UK. J. Matern. Fetal Neonatal Med. 2006, 19, 85–91. [Google Scholar] [CrossRef]
- Luo, Z.-C.; Kierans, W.J.; Wilkins, R.; Liston, R.M.; Mohamed, J.; Kramer, M.S.; the British Columbia Vital Statistics Agency. Disparities in Birth Outcomes by Neighborhood Income: Temporal Trends in Rural and Urban Areas, British Columbia. Epidemiology 2004, 15, 679. [Google Scholar] [CrossRef]
- Ncube, C.N.; Enquobahrie, D.A.; Albert, S.M.; Herrick, A.L.; Burke, J.G. Association of Neighborhood Context with Offspring Risk of Preterm Birth and Low Birthweight: A Systematic Review and Meta-Analysis of Population-Based Studies. Soc. Sci. Med. 2016, 153, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Van Ewijk, R. Long-Term Health Effects on the Next Generation of Ramadan Fasting during Pregnancy; CEP Discussion Paper No 926; Centre for Economic Performance London School of Economics and Political Science: London, UK, 2009. [Google Scholar]
- Almond, D.; Mazumder, B. Health Capital and the Prenatal Environment: The Effect of Ramadan Observance During Pregnancy. Am. Econ. J. Appl. Econ. 2011, 3, 56–85. [Google Scholar] [CrossRef]
- Algren, M.H.; Ekholm, O.; Van Lenthe, F.; Mackenbach, J.; Bak, C.K.; Andersen, P.T. Health-Risk Behaviour among Residents in Deprived Neighbourhoods Compared with Those of the General Population in Denmark: A Cross-Sectional Study. Health Place 2017, 45, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Leppert, B.; Junge, K.M.; Röder, S.; Borte, M.; Stangl, G.I.; Wright, R.J.; Hilbert, A.; Lehmann, I.; Trump, S. Early Maternal Perceived Stress and Children’s BMI: Longitudinal Impact and Influencing Factors. BMC Public Health 2018, 18, 1211. [Google Scholar] [CrossRef]
- Wei, J.-N.; Sung, F.-C.; Li, C.-Y.; Chang, C.-H.; Lin, R.-S.; Lin, C.-C.; Chiang, C.-C.; Chuang, L.-M. Low Birth Weight and High Birth Weight Infants Are Both at an Increased Risk to Have Type 2 Diabetes Among Schoolchildren in Taiwan. Diabetes Care 2003, 26, 343–348. [Google Scholar] [CrossRef]
- Lamerz, A.; Kuepper-Nybelen, J.; Wehle, C.; Bruning, N.; Trost-Brinkhues, G.; Brenner, H.; Hebebrand, J.; Herpertz-Dahlmann, B. Social Class, Parental Education, and Obesity Prevalence in a Study of Six-Year-Old Children in Germany. Int. J. Obes. 2005, 29, 373–380. [Google Scholar] [CrossRef]
- Phipps, S.A.; Burton, P.S.; Osberg, L.S.; Lethbridge, L.N. Poverty and the Extent of Child Obesity in Canada, Norway and the United States. Obes. Rev. 2006, 7, 5–12. [Google Scholar] [CrossRef]
- Laville, S. Air Pollution a Cause in Girl’s Death, Coroner Rules in Landmark Case. Available online: https://www.theguardian.com/environment/2020/dec/16/girls-death-contributed-to-by-air-pollution-coroner-rules-in-landmark-case (accessed on 15 April 2023).
- Morgan Hughey, S.; Kaczynski, A.T.; Child, S.; Moore, J.B.; Porter, D.; Hibbert, J. Green and Lean: Is Neighborhood Park and Playground Availability Associated with Youth Obesity? Variations by Gender, Socioeconomic Status, and Race/Ethnicity. Prev. Med. 2017, 95, S101–S108. [Google Scholar] [CrossRef]
- Xu, H.; Wen, L.M.; Hardy, L.L.; Rissel, C. Mothers’ Perceived Neighbourhood Environment and Outdoor Play of 2- to 3.5-Year-Old Children: Findings from the Healthy Beginnings Trial. Int. J. Environ. Res. Public Health 2017, 14, 1082. [Google Scholar] [CrossRef]
- Khanam, R.; Nghiem, S. Family Income and Child Cognitive and Noncognitive Development in Australia: Does Money Matter? Demography 2016, 53, 597–621. [Google Scholar] [CrossRef]
- Cortés-Albornoz, M.C.; García-Guáqueta, D.P.; Velez-van-Meerbeke, A.; Talero-Gutiérrez, C. Maternal Nutrition and Neurodevelopment: A Scoping Review. Nutrients 2021, 13, 3530. [Google Scholar] [CrossRef] [PubMed]
- Dufford, A.J.; Evans, G.W.; Dmitrieva, J.; Swain, J.E.; Liberzon, I.; Kim, P. Prospective Associations, Longitudinal Patterns of Childhood Socioeconomic Status, and White Matter Organization in Adulthood. Hum. Brain Mapp. 2020, 41, 3580–3593. [Google Scholar] [CrossRef] [PubMed]
- Noble, K.G.; Farah, M.J. Neurocognitive Consequences of Socioeconomic Disparities: The Intersection of Cognitive Neuroscience and Public Health. Dev. Sci. 2013, 16, 639–640. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, R.C.; Burt, S.A.; Waller, R.; Jonides, J.; Miller, A.L.; Gearhardt, A.N.; Peltier, S.J.; Klump, K.L.; Lumeng, J.C.; Hyde, L.W. Neighborhood Poverty Predicts Altered Neural and Behavioral Response Inhibition. NeuroImage 2020, 209, 116536. [Google Scholar] [CrossRef]
- Weisleder, A.; Mazzuchelli, D.S.R.; Lopez, A.S.; Neto, W.D.; Cates, C.B.; Gonçalves, H.A.; Fonseca, R.P.; Oliveira, J.; Mendelsohn, A.L. Reading Aloud and Child Development: A Cluster-Randomized Trial in Brazil. Pediatrics 2018, 141, e20170723. [Google Scholar] [CrossRef]
- Healey, A.; Mendelsohn, A. COUNCIL ON EARLY CHILDHOOD Selecting Appropriate Toys for Young Children in the Digital Era. Pediatrics 2019, 143, e20183348. [Google Scholar] [CrossRef]
- Stich, H.L.; Baune, B.T.; Caniato, R.N.; Krämer, A. Associations between Preschool Attendance and Developmental Impairments in Pre-School Children in a Six-Year Retrospective Survey. BMC Public Health 2006, 6, 260. [Google Scholar] [CrossRef]
- Stich, H.L.; Caniato, R.N.; Krämer, A.; Baune, B. Influence of Kindergarten on Numbers of Multiple Developmental Delays in Preschoolers: An Analysis over 14 Years. Int. J. Public Health 2017, 62, 613–621. [Google Scholar] [CrossRef]
- Knollmann, C.; Thyen, U. Einfluss des Besuchs einer Kindertagesstätte (Kita) auf den Entwicklungsstand bei Vorschulkindern. Gesundheitswesen 2019, 81, 196–203. [Google Scholar] [CrossRef]
- Glass, T.A.; Bilal, U. Are Neighborhoods Causal? Complications Arising from the ‘Stickiness’ of ZNA. Soc. Sci. Med. 2016, 166, 244–253. [Google Scholar] [CrossRef]
- Laurin, I.; Guay, D.; Fournier, M.; Bigras, N.; Solis, A. Attendance in Educational Preschool Services: A Protective Factor in the Development of Children from Low-Income Families? Can. J. Public Health 2015, 106, eS14–eS20. [Google Scholar] [CrossRef]
- Berchick, E.R. The Relationship between Maternal Education and Reported Childhood Conditions. Soc. Sci. Med. 2016, 170, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.D.; Lakerveld, J.; Van Oostveen, Y.; Compernolle, S.; De Bourdeaudhuij, I.; Bárdos, H.; Rutter, H.; Glonti, K.; Oppert, J.-M.; Charreire, H.; et al. The Mediating Role of Social Capital in the Association between Neighbourhood Income Inequality and Body Mass Index. Eur. J. Public Health 2016, ckw157. [Google Scholar] [CrossRef] [PubMed]
- Sandel, M.; Faugno, E.; Mingo, A.; Cannon, J.; Byrd, K.; Garcia, D.A.; Collier, S.; McClure, E.; Jarrett, R.B. Neighborhood-Level Interventions to Improve Childhood Opportunity and Lift Children Out of Poverty. Acad. Pediatr. 2016, 16, S128–S135. [Google Scholar] [CrossRef] [PubMed]
- Blair, A.; Marryat, L.; Frank, J. How Community Resources Mitigate the Association between Household Poverty and the Incidence of Adverse Childhood Experiences. Int. J. Public Health 2019, 64, 1059–1068. [Google Scholar] [CrossRef]
- mdr.de Von der Silberhöhe in Bessere Viertel: Was Gegen Kinderarmut in Städten wie Halle Helfen Könnte|MDR.DE. Available online: https://www.mdr.de/nachrichten/sachsen-anhalt/halle/halle/jedes-dritte-kind-in-halle-arm-100.html (accessed on 16 April 2023).
- Wiech, U. Migration Aus Großwohnsiedlungen–Umzugsmotive Seit 2010 Abgewanderter Aus Halle-Neustadt; Martin-Luther-University Halle-Wittenberg: Halle, Germany, 2022. [Google Scholar] [CrossRef]
- Wudy, L. Halle-Neustadt als Dynamisches Ankunftsquartier nach dem Langen Sommer der Migration–Migrantische Aushandlungs- und Aneignungspraktiken in Einer Ostdeutschen Großwohnsiedlung; Martin-Luther-University Halle-Wittenberg: Halle, Germany, 2021. [Google Scholar] [CrossRef]
- Bernt, M.; Förste, D.; Colini, L.; Hebsaker, J. Kleinräumliche Untersuchung Sozialstrukturellen Veränderungen Halle (Saale); Leibnitz Institut für Raumbezogene Sozialforschung: Erkner, Germany, 2014. [Google Scholar]
- Mau, S. Lütten Klein: Leben in Der Ostdeutschen Transformationsgesellschaft; 3. Auflage; Suhrkamp: Berlin, Germany, 2019; ISBN 9783518428948. [Google Scholar]
- Cheng, T.L.; Johnson, S.B.; Goodman, E. Breaking the Intergenerational Cycle of Disadvantage: The Three Generation Approach. Pediatrics 2016, 137, e20152467. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Low Socioeconomic Burden Quarters (n = 552) | Medium Socioeconomic Burden Quarters (n = 4316) | High Socioeconomic Burden Quarters (n = 2686) | City of Halle (n = 8417) | |||||
|---|---|---|---|---|---|---|---|---|
| % | N | % | N | % | N | % | N | |
| Female sex | 49.5 | 273 | 47.8 | 2061 | 49.2 | 1321 | 48.5 | 4081 |
| High BS | 54.5 | 301 | 41.5 | 1789 | 8.5 | 228 | 28.9 | 2435 |
| Medium BS | 16.5 | 91 | 23.0 | 993 | 24.5 | 659 | 21.9 | 1846 |
| Low BS | 2 | 11 | 7.4 | 318 | 31.3 | 841 | 14.7 | 1238 |
| Unknown BS | 25.0 | 149 | 28.2 | 1216 | 35.7 | 958 | 34.4 | 2898 |
| Single parent households | 8.9 | 48 | 17.0 | 735 | 32.4 | 869 | 21.77 | 1832 |
| Both parents in household | 84.8 | 468 | 73.8 | 3187 | 53.5 | 1438 | 67.3 | 5668 |
| Attending Kindergarten | 97.6 | 539 | 94.9 | 4096 | 80.7 | 2168 | 90.4 | 807 |
| Smoking household | 18.1 | 100 | 30.6 | 1319 | 49.9 | 1341 | 36.2 | 3048 |
| Child born in Germany | 96.7 | 534 | 92.4 | 3986 | 75.7 | 2032 | 86.7 | 7296 |
| Born prematurely < 37 weeks | 6.9 | 36 | 9.1 | 345 | 11.2 | 210 | 9.4 | 646 |
| Low birthweight < 2500 g | 4.9 | 26 | 6.7 | 257 | 9.9 | 188 | 7.3 | 514 |
| Currently overweight BMI > 90th percentile | 5.3 | 29 | 8.0 | 341 | 11.3 | 295 | 8.9 | 731 |
| No U 8 health screening | 13.2 | 73 | 21.8 | 942 | 42.6 | 1151 | 28.6 | 2406 |
| Sub-par grammar | 1.8 | 10 | 8.5 | 367 | 35.6 | 957 | 17.4 | 1460 |
| Sub-par fine motor skills | 3.8 | 21 | 6.2 | 266 | 17.2 | 461 | 9.7 | 816 |
| Sub-par gross motor skills | 2.5 | 14 | 2.3 | 97 | 7.7 | 206 | 4.2 | 357 |
| Sub-par cognitive development | 1.5 | 8 | 3.9 | 170 | 17.2 | 462 | 8.2 | 691 |
| Sub-par overall development | 3.3 | 18 | 8.7 | 375 | 35.8 | 962 | 17.7 | 1490 |
| New specialist referral | 7.8 | 43 | 8.4 | 364 | 16.2 | 434 | 11.2 | 943 |
| Crude Model OR, 95% CI | Model A * OR, 95% CI | Model B ** OR, 95% CI | |
|---|---|---|---|
| Medium socioeconomic burden quarters vs. low socioeconomic burden quarters | 2.8 (1.7–4.6) | 2.4 (1.5–3.9) | 1.9 (1.1–3.0) |
| High socioeconomic burden quarters vs low socioeconomic burden quarters | 16.5 (10.3–26.6) | 8.5 (5.2–13.8) | 4.9 (3.0–8.1) |
| Unknown BS vs. High BS | 5.9 (4.6–7.6) | ||
| Medium BS vs. High BS | 2.4 (1.8–3.1) | ||
| Low BS vs. High BS | 9.9 (7.6–12.9) | ||
| Father: Education level unknown vs. more than 10 years of education | 2.0 (1.4–2.7) | ||
| Father: 10 years of education vs. more than 10 years of education | 1.4 (1.1–1.7) | ||
| Father: Less than 10 years of education vs. more than 10 years of education | 2.3 (1.8–2.9) | ||
| Mother: Education level unknown vs. more than 10 years of education | 1.9 (1.4–2.7) | ||
| Mother: 10 years of education vs. more than 10 years of education | 1.0 (0.8–1.2) | ||
| Mother: Less than 10 years of education vs. more than 10 years of education | 1.9 (1.5–2.4) | ||
| Father: Employment status unknown vs. employed | 0.9 (0.7–1.2) | ||
| Father: Unemployed vs. employed | 1.5 (1.3–1.9) | ||
| Mother: Employment status unknown vs. employed | 3.6 (2.6–5.0) | ||
| Mother: Unemployed vs. employed | 3.8 (3.2–4.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, K.; Wienke, A.; Gröger, C.; Klusmann, J.-H.; Führer, A. Segregated by Wealth, Health, and Development: An Analysis of Pre-School Child Health in a Medium-Sized German City. Children 2023, 10, 865. https://doi.org/10.3390/children10050865
Wagner K, Wienke A, Gröger C, Klusmann J-H, Führer A. Segregated by Wealth, Health, and Development: An Analysis of Pre-School Child Health in a Medium-Sized German City. Children. 2023; 10(5):865. https://doi.org/10.3390/children10050865
Chicago/Turabian StyleWagner, Karoline, Andreas Wienke, Christine Gröger, Jan-Henning Klusmann, and Amand Führer. 2023. "Segregated by Wealth, Health, and Development: An Analysis of Pre-School Child Health in a Medium-Sized German City" Children 10, no. 5: 865. https://doi.org/10.3390/children10050865
APA StyleWagner, K., Wienke, A., Gröger, C., Klusmann, J.-H., & Führer, A. (2023). Segregated by Wealth, Health, and Development: An Analysis of Pre-School Child Health in a Medium-Sized German City. Children, 10(5), 865. https://doi.org/10.3390/children10050865