Abstract
Background: The appropriate alignment of the lower teeth is indicated by the Curve of Spee (COS), which can be observed in the sagittal profile view of human skulls. Graf Von Spee made the initial observation on this occlusal curvature. Through this systematic review and meta-analysis, we evaluated studies that looked at how COS affected masticatory activities. Methods: The databases PubMed-MEDLINE, Web of Science, Cochrane, and Scopus were all searched. A total of 12 documents were ultimately picked because they met the necessary inclusion and exclusion requirements. The data was then loaded into the RevMan 5 programme for meta-analysis after being chosen for information on the sample size, variables analyzed, and various aspects of the research. Results: The Curve of Spee was found to have a noticeable impact on both the masticatory efficiency as well as dentofacial alignment in the 12 studies that we selected for the review and meta-analysis. In addition, other occlusal curvatures such as the Curve of Monson and the Curve of Wilson were found to be of vital importance on a similar level to the COS. The meta-analysis further revealed that seven of the included clinical trials had mentioned the noticeable impact on masticatory efficiency. Conclusions: This study focused on the significance of the COS on force distribution in the oral cavity as well as the necessity of COS corrections after receiving full orthodontic care. Following orthodontic treatment, the COS, along with other occlusal curves such as the Curve of Wilson and the Curve of Monson, is essential in removing strains from the condyle, as well as the maxilla and mandible, which enhances masticatory effectiveness and lessens the overall strain on a patient’s oral cavity.
1. Introduction
Orthodontic remedial treatment is increasingly expensive but essential in many people’s lives. To rectify malocclusions in the dentition, the primary goal is to align the teeth and jaws [1]. Given how commonplace it is in the contemporary Western world, one might wonder why we do not observe the need for this correction in the vast majority of the ancient world. Although there may have been the occasional case of a misaligned orofacial complex in the past, it is now fairly rare for a post-industrial adolescent to not need any kind of dental intervention. The link between this and nutrition is strongly supported by the data. Increased bite force and chewing cycles brought on by a harsh or abrasive diet during growth leads to a flatter Curve of Spee (COS), more sub-nasal prognathism, and more dental attrition [1,2]. Because these characteristics encourage better dental and skeletal occlusion, the current post-industrial diet causes an epidemiological transition in occlusion, which substantially increases malocclusion in modern populations.
The Curve of Spee (COS), which is visible in the sagittal profile image of human skulls, indicates the exact alignment of the lower teeth. Graf Von Spee made the initial remark in 1890 [2]. Recent research has revealed that it had a curvature that extends from the centre teeth’s incisor edges to their distobuccal cusps [3]. The literature claims that the mesial inclination of the lower molar teeth’s long axis caused the masticatory muscles to function improperly, which led to the development of the COS [4,5,6]. One study suggested that the Curve of Spee may play a biomechanical role in the processing of food by enhancing the crush/shear ratio between the posterior teeth and the efficiency of occlusal pressures during the masticatory process [4]. This suggestion alluded to the idea of “masticatory efficiency.” The COS permits unrestricted lower jaw motions while enhancing food chewing by maintaining upper and lower tooth contacts throughout operation [2]. By pursuing an aesthetic grin, the COS also enhances face aesthetics [7]. There are two main ways to evaluate the COS. The anterior Condyle border, the buccal cusps of the second and first molars, the cusp tips of the canine and premolars, and the incisor edge of the two central incisors are all included in the first illustration of the inferior radius of a circle [8]. The second method of COS assessment was built on the occlusal plane as well as the width and depth of the posterior teeth’s arches [9]. Yet there is disagreement on how to quantify the COS. Some authors did not quantify COS using the lower incisors [10]. Thanks to recent technological developments and the use of a three-dimensional (3D) scanner, COS measurement when using a digital cast analysis is now easier and more accurate. Previously, all measurements were performed using a divider, calipers, and a coordinate apparatus on hard study models or pictures of the models [11]. To accomplish the proper incisor relation and posterior teeth occlusion during full orthodontic treatment, the COS of the mandibular teeth must be levelled [12,13]. However, there is still debate over the COS levelling methods used to increase the stability of orthodontic outcomes [14]. We must also consider the disadvantages pertaining to an accentuation in the COS. An accentuated Curve of Spee can create occlusal interferences between the upper and lower teeth, which can cause discomfort, pain, and damage to the teeth. This can further lead to malocclusion, which means that the upper and lower teeth do not fit together properly and can cause problems with mastication, phonation, and oral hygiene, and can increase the risk of tooth decay and gum disease. An accentuated curve of Spee can also put excessive stress on the TMJ, which is the joint that connects the jaw to the skull. This can lead to TMJ disorders, which can cause pain, clicking, popping, and limited range of motion in the jaw. This also increases the risk of bruxism, which is a condition where people grind or clench their teeth unconsciously. This can lead to tooth wear, jaw pain, headaches, and other complications. Moreover, an accentuated Curve of Spee can make orthodontic treatment more challenging, as it can require more complex movements to correct the malocclusion, issues which can be resolve by carefully flattening of the COS as recommended by certain studies [14,15,16]. Regardless of the effect on the mandible, the Temporomandibular Joint (TMJ), or even the lower teeth, since 1972 Andrews [15] has recommended levelling the COS to a flat surface in order to assist in the formation of an ideal occlusion. Kanavakis and Mehta [16] discovered a connection between the flatness of the COS and the TMJ sound.
In order to determine whether the COS had any observable effects on the occlusal curvature/malocclusion in the oral cavity as well as the effects of the COS on enhancing masticatory functions, the aim of this systematic review and meta-analysis was to examine the available literature. The primary variable that we examined through the studies that we chose for review and later meta-analysis was the impact of the COS on masticatory efficiency.
2. Materials and Methods
This review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42023389852).
2.1. Protocols Employed
The Orderly Reviews in Health Care: Meta-Examination book and the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) criteria were followed in the conduct of this systematic review [17].
2.2. Review Hypotheses
By the means of this systematic review and meta-analysis, we assessed studies that ascertained whether the COS had any discernible impacts on the occlusal curvature/malocclusion in the oral cavity as well as the effects of the COS on enhancing masticatory functions. The effect of the COS on masticatory efficiency was the main variable that we examined through the papers that we chose for review and subsequent meta-analysis, and this was the main goal of the study.
2.3. Inclusion Criteria
Articles that featured material relevant to the review’s objectives and covered all age groups were chosen for full-text screening. We considered including articles that presented randomized/non-randomized investigations, systematic reviews with large sample sizes, in-depth case reports, and validated questionnaire-based studies.
2.4. Exclusion Criteria
Studies involving animal subjects, seminar presentations, academic publications, opinion pieces, and incomplete data were not included in the scope of our systematic examination.
Our search did not limit the selection of studies based on their year of publication; instead, we considered all publications that had been released in connection with our topic (where the number of papers itself was found to be quite sparse in number). This is a result of the dearth of literature on the topic that is pertinent to the objective of our inquiry.
Studies using placebos were not included in the study. All reviews of the literature and cases that were written in languages other than English were also disregarded.
2.5. Data Selection and Coding
Two independent reviewers searched through pertinent papers in various databases and online search engines using MeSH terms such as “Curve of Spee,” “Dentofacial anatomy,” “Masticatory efficiency,” “Occlusal curvature,” and “Wilson’s curve.” The chosen papers were compared, and a third reviewer was consulted if there was a dispute.
The same two reviewers separately extracted the following information after selecting the articles: author, year of publication, nation, type of publication, study topic, population demographics (n, age), outcome measure(s), pertinent result(s), and conclusion(s). A third reviewer was consulted once the data were compared to go through any discrepancies.
2.6. Study Selection
A thorough search of the online journals turned up 482 documents in total, and 169 of the papers were first selected. After removing 111 articles that were identical to or duplicates of each other, only 58 original papers remained. In total, 46 further articles were excluded after the abstracts and titles of the submissions were examined. Ultimately, 12 documents—mostly in-vitro experiments, literature reviews, and comparative analyses—were chosen that satisfied the essential inclusion and exclusion criteria. (Figure 1) Using relevant keywords, reference searches, and citation searches, the databases PubMed-MEDLINE, Web of Science, Cochrane, and Scopus were all searched. “Curve of Spee,” “Dentofacial anatomy,” “Masticatory efficiency,” “Occlusal curvature” and “Wilson’s curve” were the search terms used to search the database. The keywords were used as filters in the above-listed databases.
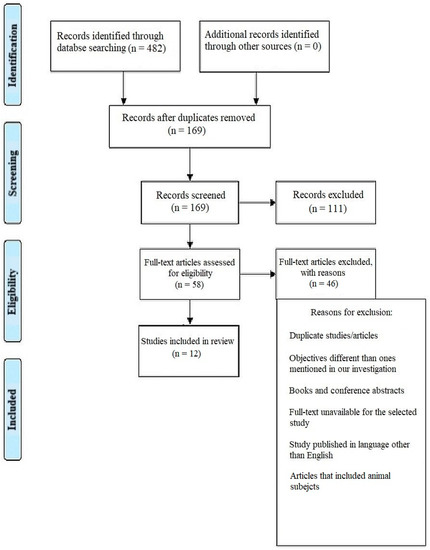
Figure 1.
Representation of selection of articles through PRISMA framework.
2.7. Statistical Analysis
The data was then loaded into the RevMan 5 programme for meta-analysis after being chosen for information on the sample size, variables analyzed, and various aspects of this research. As part of the meta-analysis for our investigation, forest plots showing the odds ratio, risk ratio, and risk difference (using a fixed effects model) of the different treatment modalities were generated. These plots are given in Figure 2, Figure 3 and Figure 4 respectively assuming a 95% confidence interval.
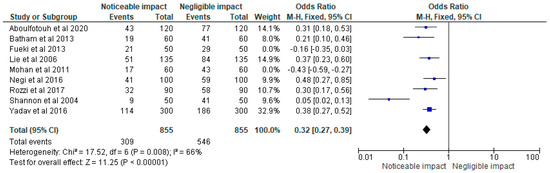
Figure 2.
Forest plot of the odds ratio representing the impact status of COS accentuation on masticatory efficiency in the clinical trials [2,18,19,20,21,22,23,24,25] selected for our meta-analysis (assuming a 95% confidence interval).
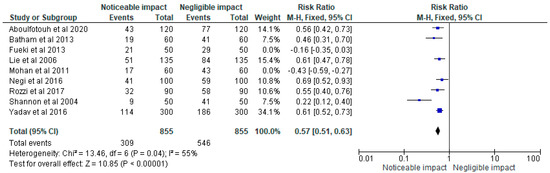
Figure 3.
Forest plot of the risk ratio representing the impact status of COS accentuation on masticatory efficiency in the clinical trials [2,18,19,20,21,22,23,24,25] selected for meta-analysis (assuming a 95% confidence interval).
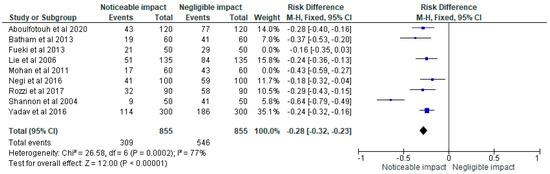
Figure 4.
Risk difference representing the impact status of COS accentuation on masticatory efficiency in the clinical trials [2,18,19,20,21,22,23,24,25] selected for meta-analysis on a forest plot (assuming a 95% confidence interval.
2.8. Risk of Bias Assessment
The AMSTAR-2 approach was used to evaluate the studies we chose for Table 1 for bias [26]. In addition to a number of other instruments that have served the same goal, AMSTAR 2 has been made accessible as a critical evaluation tool for systematic reviews. As seen in Table 2 below, it is a 16-point checklist. Two extremely noticeable devices served as the foundation for the creation of the first AMSTAR tool. The original AMSTAR was duplicated by two new instruments. The AMSTAR 2 risks of bias items identify the domains specified in the Cochrane risk of bias instruments for systematic reviews. These demonstrate that a decision was made in each instance after feedback from more than 30 methodological specialists.

Table 1.
AMSTAR-2 16-point checklist of risk of bias assessment in studies selected for the review.
Table 2.
Description and outcomes as observed in the studies selected for the systematic review.
3. Results
The various characteristics of the studies selected after implementation of the requisite inclusion/exclusion criterion, such as sample size, mean age of the study participants, study objectives, and their respective inferences/outcomes [2,18,19,20,21,22,23,24,25,27,28] are displayed in Table 2.
4. Discussion
The relationship between an individual’s occlusal curvature and the masticatory strain brought on by nutrition during development is obvious. Changes in prehistoric populations, contemporary people, and studies using animal models all reflect this. Mandibular and dental traits might reveal information about the types of diet ingested during a person’s growth and development [29]. Understanding the causes of the aesthetic and health problems that result from malocclusion today depends critically on understanding secular patterns in malocclusion. We can improve our understanding of how the COS controls not only masticatory efficiency but also other aspects of occlusion by taking an anthropological approach to dentofacial misalignment in the archaeological record and in the present.
The effect of the COS on masticatory efficiency was the primary variable on the basis of which the meta-analysis was conducted. All the studies concerning the review objectives were considered except for studies by Fueki et al. [20] and Mohan et al. [23], since the study done by Fueki et al. [20] was primarily concerned with investigating the link between occlusal curvature and the ability of young adults with permanent teeth to mix and comminute food using a masticatory performance test that did not directly assess a relationship between the COS and mastication. As for the study by Mohan et al. [23], the participants were primarily divided into two distinct age groups without mentioning/taking into account the pre/post differences of COS correction on occlusal movement. Additionally, the lack of a proper follow-up record made it ineligible for it to be included in the meta-analysis. As such, these two studies were reviewed but they carried no weight in the meta-analysis as evident in the forest plots.
The number of participants in each of the studies has been included in the meta-analysis, with the effect of the COS on masticatory performance assessed by the number of noticeable and negligible events in each of the trials. The risk of bias pertaining to the mta-analysis is moderately high, which can be attributed to the heterogeneity percentage, which happens to be fairly high for a systematic review such as this, but the studies that we reviewed as per our objectives were varied in their methodologies and, although the variable of our concern was examined in all of them, the study designs and protocols that they followed were somewhat different from one another.
The majority of occlusal macrowear, it is commonly believed, is produced during chewing food, with the exception of people who grind their teeth out of habit [30]. In a 1999 study, Sengupta and associates [31] examined the COS, third molar occurrence, and occlusal macrowear. When compared to normal pre-industrialized dentitions, the modern dentition is linked to a higher frequency of third molar impaction and agenesis, as well as mild wear rates [30,32,33]. Because of this, the authors postulate that historically high rates of wear brought on by abrasive diets kept the COS flat. Their argument that any damage in the current era is caused by sustained use rather than by abrasive diets is probably a sound one [30]. The findings, however, showed that there was no direct correlation between the COS and macrowear; the COS was not sustained by wear. Although the authors sought to ascertain if a deeply arched COS should be incorporated into dental prosthetic designs, this evidence can potentially be interpreted in other ways. Given that the mandibular structure is often established by the time the dentition exhibits considerable wear, it is unlikely that this wear will have a significant impact on COS depth. Given this, it is plausible to infer that mastication of food is the common source of both wear and the COS. The mandibular morphology is altered to produce a flatter COS by chewing abrasive and difficult foods during growth; if a similar diet is followed in adulthood, more severe wear may be visible. COS depth and tooth wear are probably connected, although perhaps not in the way that Sengupta and colleagues have suggested [31].
Dietary consistency changes have an impact on occlusion because they influence orofacial morphology. This is due to its effect on chewing, which ultimately has an impact on the biomechanical stress placed on the jaw. The strain is affected by the differential between difficult and abrasive foods. Tough foods, such as meat, require more bite force and more chewing cycles before swallowing, whereas abrasive foods, such as nuts, produce more friction and wear with each bite [34,35]. Because it measures how hard the muscles must work to chew food, bite force is significant [35]. The growth and preservation of alveolar bone are impacted by the tension caused by bite force. The fact that a deeper curve might enhance the force potential for each chewing cycle provides proof that the COS has a role in determining biting force potential [20]. As determined by a single occlusion of the opposing dental arcades, a chewing cycle is the movement of the food bolus around the mouth [20]. Certain foods take longer to digest, which has an impact on how much muscle is used and how the orofacial bones are stimulated. There is proof that a person’s biological capacity for performing each of these characteristics is significantly influenced by their jaw morphology. Greater sub-nasal prognathism has been linked to the capacity to carry out more chewing cycles at a greater biting force. This is made possible by a stronger jaw and a more acute gonial angle [20,34]. This combination of characteristics would improve occlusion and result in higher levels of tooth macrowear. Diet has a big impact on these bone and muscle elements, which are crucial for growing and maintaining a normal dental complex.
In a geometric-morphometric investigation, Laird and colleagues [1] correlated the COS and prognathism in contemporary humans and archaic Homo Sapiens. As a whole, contemporary humans were more orthognathic, although there are still variations amongst populations, according to their findings. People with a deeply curved COS are orthognathic, but those with a flattened COS were more prognathic. The COS and alveolar prognathism co-varied [1]. Although their analysis is thorough, they may want to reconsider their conclusion that the COS and prognathism are population-specific markers in modern humans [1]. Metric measurements and a qualitative review of bite alignment may be some of these characteristics. There is reason to suppose that by using traits such as these in conjunction with other dietary reconstruction techniques, one can deduce details about the diet ingested during development, though this would need further testing to be confirmed [36]. This is useful in supporting assertions about nutrition and food processing made on the basis of stable isotope studies and archaeological interpretations because it is not always obvious how a group subsisted.
The fact that we did not assess the other occlusal curvatures (such as the Curve of Monson and the Curve of Wilson) as well as the COS could be deemed to be one of the flaws of our systematic review, since the various curvatures combine to influence the dentofacial anatomy and other aspects of malocclusion. Furthermore, our meta-analysis did not include a lot of studies with a higher sample size than what could be considered ideal and that might pose a question upon the credibility of the results and might have introduced a certain degree of bias as far as the meta-analysis is concerned. Hence, we recommend more studies that assess the various occlusal curvatures individually so that their impact on the patient undergoing any form of orthodontic treatment is clearly evaluated and clinically implemented.
5. Conclusions
The importance of the COS on force distribution in the oral cavity and the requirement for COS corrections following comprehensive orthodontic treatment were the main subjects of this investigation. Following orthodontic treatment, the COS is crucial in removing strains from the condyle, as well as the maxilla and mandible, which improves masticatory effectiveness and reduces the overall strain on a patient’s oral cavity. This is true of other occlusal curves as well, such as the Curve of Wilson and the Curve of Monson, although they were not assessed as rigorously as the COS for the sake of the major objectives of our investigation.
Author Contributions
Conceptualization, Z.A.A., M.G.S., R.I., K.K.G., N.N.A., R.M.A., M.R.S.A., M.F.A., M.A.R.A. and M.K.A.; methodology, Z.A.A., M.G.S., R.I. and M.K.A.; software, Z.A.A., M.G.S., R.I. and M.K.A.; validation, Z.A.A., M.G.S., R.I. and M.K.A.; formal analysis, Z.A.A., R.I., and M.K.A.; investigation, Z.A.A., R.I., and M.K.A.; resources, Z.A.A., M.G.S., R.I. and M.K.A.; data curation, Z.A.A., M.G.S., R.I. and M.K.A.; writing—original draft preparation, Z.A.A., M.G.S., R.I., K.K.G., N.N.A., R.M.A., M.R.S.A., M.F.A., M.A.R.A. and M.K.A.; writing—review and editing, Z.A.A., M.G.S., R.I., K.K.G., N.N.A., R.M.A., M.R.S.A., M.F.A., M.A.R.A. and M.K.A.; visualization, M.G.S. and M.K.A.; supervision, M.G.S. and M.K.A.; project administration, M.G.S. and M.K.A.; funding acquisition, None. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42023389852).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data set used in the current study will be made available on request from Zainab A. Alkhalaf; dr.zainab.alkhalaf@jodent.org.
Conflicts of Interest
The authors report no conflict of interest in the conduction of this systematic review and meta-analysis.
References
- Laird, M.F.; Holton, N.E.; Scott, J.E.; Franciscus, R.G.; Marshall, S.D.; Southard, T.E. Spatial determinants of the mandibular curve of Spee in modern and archaic Homo. Am. J. Phys. Anthr. 2016, 161, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Shannon, K.R.; Nanda, R.S. Changes in the curve of Spee with treatment and at 2 years posttreatment. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 589–596. [Google Scholar] [CrossRef]
- Spee, G.; Biedenbach, A.; Hotz, M.; Hitchcock, P. The gliding path of the mandible along the skull. J. Am. Dent. Assoc. 1890, 100, 670–675. [Google Scholar] [CrossRef]
- Tamizharasi, S.; Kumar, K.P.S. Significance of curve of Spee: An orthodontic review. J. Pharm. Bioallied Sci. 2012, 4 (Suppl. S2), S323–S328. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, R.; Clay, S.M.; Yoo, S.; Hlusko, L.J. Conserved and Taxon-Specific Patterns of Phenotypic Modularity in the Mammalian Dentition. Integr. Org. Biol. 2022, 4, 7obac01. [Google Scholar] [CrossRef]
- Choy, S.E.M.; Lenz, J.; Schweizerhof, K.; Schmitter, M.; Schindler, H.J. Realistic kinetic loading of the jaw system during single chewing cycles: A finite element study. J. Oral Rehabil. 2017, 44, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.D.; Caspersen, M.; Hardinger, R.R.; Franciscus, R.G.; Aquilino, S.A.; Southard, T.E. Development of the curve of Spee. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 344–352. [Google Scholar] [CrossRef]
- Dawson, E. Functional Occlusion: From TMJ to Smile Design, 1st ed.; Elsevier: St. Louis, MO, USA, 2006; p. 450. [Google Scholar]
- Xu, H.; Suzuki, T.; Muronoi, M.; Ooya, K. An evaluation of the curve of Spee in the maxilla and mandible of human permanent healthy dentitions. J. Prosthet. Dent. 2004, 92, 536–539. [Google Scholar] [CrossRef]
- Baydaş, B.; Yavuz, I.; Atasaral, N.; Ceylan, I.; Dağsuyu, I.M. Investigation of the changes in the positions of upper and lower incisors, overjet, overbite, and irregularity index in subjects with different depths of curve of Spee. Angle Orthod. 2004, 74, 349–355. [Google Scholar] [CrossRef]
- Harris, F.; Corruccini, E. Quantification of dental occlusal variation: A review of methods. Dent. Anthr. 2008, 21, 1–11. [Google Scholar] [CrossRef]
- Kumari, N.; Fida, M.; Shaikh, A. Exploration of variations in positions of upper and Lower incisors, overjet, overbite, and irreg-ularity Index in orthodontic patients with dissimilar depths of Curve of spee. J. Ayub. Med. Coll Abbottabad. 2016, 28, 766–772. [Google Scholar]
- Yu, Z. Question about relapse of corrected deepbites. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 152. [Google Scholar] [CrossRef]
- Cordon, N.E. Post Treatment Stability of Deep Bite Malocclusions. Ph.D. Thesis, The University of Oklahoma, Oklahoma City, OK, USA, 1996. [Google Scholar]
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. 1972, 62, 296–309. [Google Scholar] [CrossRef]
- Kanavakis, G.; Mehta, N. The role of occlusal curvatures and maxillary arch dimensions in patients with signs and symptoms of temporomandibular disorders. Angle Orthod. 2014, 84, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Aboulfotouh, M.H.; El-Dawlatly, M.M. The relationship between the depth of the curve of Spee and different types of malocclusion. Egypt. Orthod. J. 2020, 58, 19–25. [Google Scholar] [CrossRef]
- Batham, P.R.; Tandon, P.; Sharma, V.P.; Singh, A. Curve of Spee and Its Relationship with Dentoskeletal Morphology. J. Indian Orthod. Soc. 2013, 47, 128–134. [Google Scholar] [CrossRef]
- Fueki, K.; Yoshida, E.; Igarashi, Y. Association between occlusal curvature and food comminution and mixing in human young adults with permanent dentitions. Arch. Oral Biol. 2013, 58, 377–383. [Google Scholar] [CrossRef]
- Lie, F.; Kuitert, R.; Zentner, A. Post-treatment development of the curve of Spee. Eur. J. Orthod. 2006, 28, 262–268. [Google Scholar] [CrossRef]
- Mohan, M.; D′souza, M.; Kamath, G.; Parolia, A. Comparative evaluation of the curve of Spee in two age groups and its relation to posterior teeth disclusion. Indian J. Dent. Res. 2011, 22, 179. [Google Scholar] [CrossRef]
- Negi, S.K.; Shukla, L.; Sandhu, G.P.S.; Aggarwal, M. Investigation of variation in curve of Spee, over jet and overbite among class-I and class-II malocclusion subjects and to find sexual dimorphism, if any. J. Adv. Med. Dent. Sci. Res. 2016, 4, 21. [Google Scholar]
- Yadav, K.; Tondon, R.; Singh, K.; Azam, A.; Kulshrestha, R. Evaluation of skeletal and dental parameters in individuals with variations in depth of Curve of Spee. Indian J. Orthod. Dentofac. Res. 2016, 2, 184–189. [Google Scholar] [CrossRef]
- Rozzi, M.; Mucedero, M.; Pezzuto, C.; Cozza, P. Leveling the curve of Spee with continuous archwire appliances in different vertical skeletal patterns: A retrospective study. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 758–766. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Hasan, L.A.; Al Qassar, S.S.S.; Alrawi, M.N.; Alhajar, E.H. Does the flatting of the curve of spee affect the chewing force distribution in the mandible? (3D finite element study). J. Orthod. Sci. 2021, 10, 1. [Google Scholar] [PubMed]
- Marshall, S.D.; Kruger, K.; Franciscus, R.G.; Southard, T.E. Development of the mandibular curve of spee and maxillary compensating curve: A finite element model. PLoS ONE 2019, 14, e0221137. [Google Scholar] [CrossRef]
- Rando, C.; Hillson, S.; Antoine, D. Changes in mandibular dimensions during the mediaeval to post-mediaeval transition in London: A possible response to decreased masticatory load. Arch. Oral Biol. 2014, 59, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Kaifu, Y.; Kasai, K.; Townsend, G.C.; Richards, L.C. Tooth wear and the “design” of the human dentition: A perspective from evolutionary medicine. Am. J. Phys. Anthr. 2003, 122 (Suppl. 37), 47–61. [Google Scholar] [CrossRef]
- Sengupta, A.; Whittaker, D.K.; Barber, G.; Rogers, J.; Musgrave, J.H. The effects of dental wear on third molar eruption and on the curve of Spee in human archaeological dentitions. Arch. Oral Biol. 1999, 44, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Boughner, J.C.; Dean, M. Does space in the jaw influence the timing of molar crown initiation? A model using baboons (Papio anubis) and great apes (Pan troglodytes, Pan paniscus). J. Hum. Evol. 2004, 46, 253–275. [Google Scholar] [CrossRef] [PubMed]
- von Cramon-Taubadel, N. Global human mandibular variation reflects differences in agricultural and hunter-gatherer subsistence strategies. Proc. Natl. Acad. Sci. USA 2011, 108, 19546–19551. [Google Scholar] [CrossRef] [PubMed]
- Ingervall, B.; Bitsanis, E. A pilot study of the effect of masticatory muscle training on facial growth in long-face children. Eur. J. Orthod. 1987, 9, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Ledogar, J.A.; Dechow, P.C.; Wang, Q.; Gharpure, P.H.; Gordon, A.D.; Baab, K.L.; Smith, A.L.; Weber, G.W.; Grosse, I.R.; Ross, C.F.; et al. Human feeding biomechanics: Performance, variation, and functional constraints. PeerJ 2016, 4, e2242. [Google Scholar] [CrossRef]
- Sella-Tunis, T.; Pokhojaev, A.; Sarig, R.; O’Higgins, P.; May, H. Human mandibular shape is associated with masticatory muscle force. Sci. Rep. 2018, 8, 6042. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).