
Endogenous Opioids in Crohn’s Disease

{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Studied Groups
2.2. Laboratory Testing
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
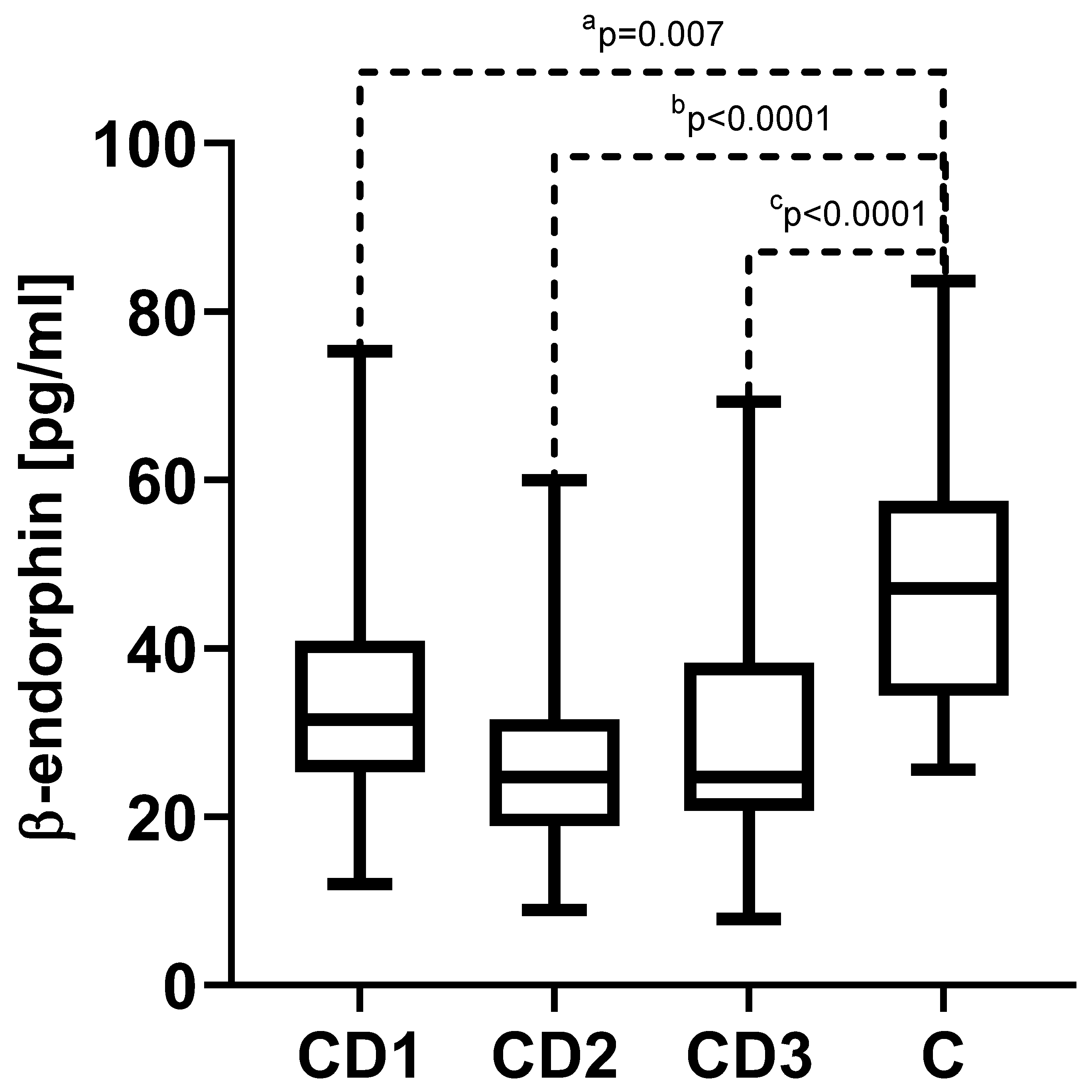
3.2. β-Endorphin
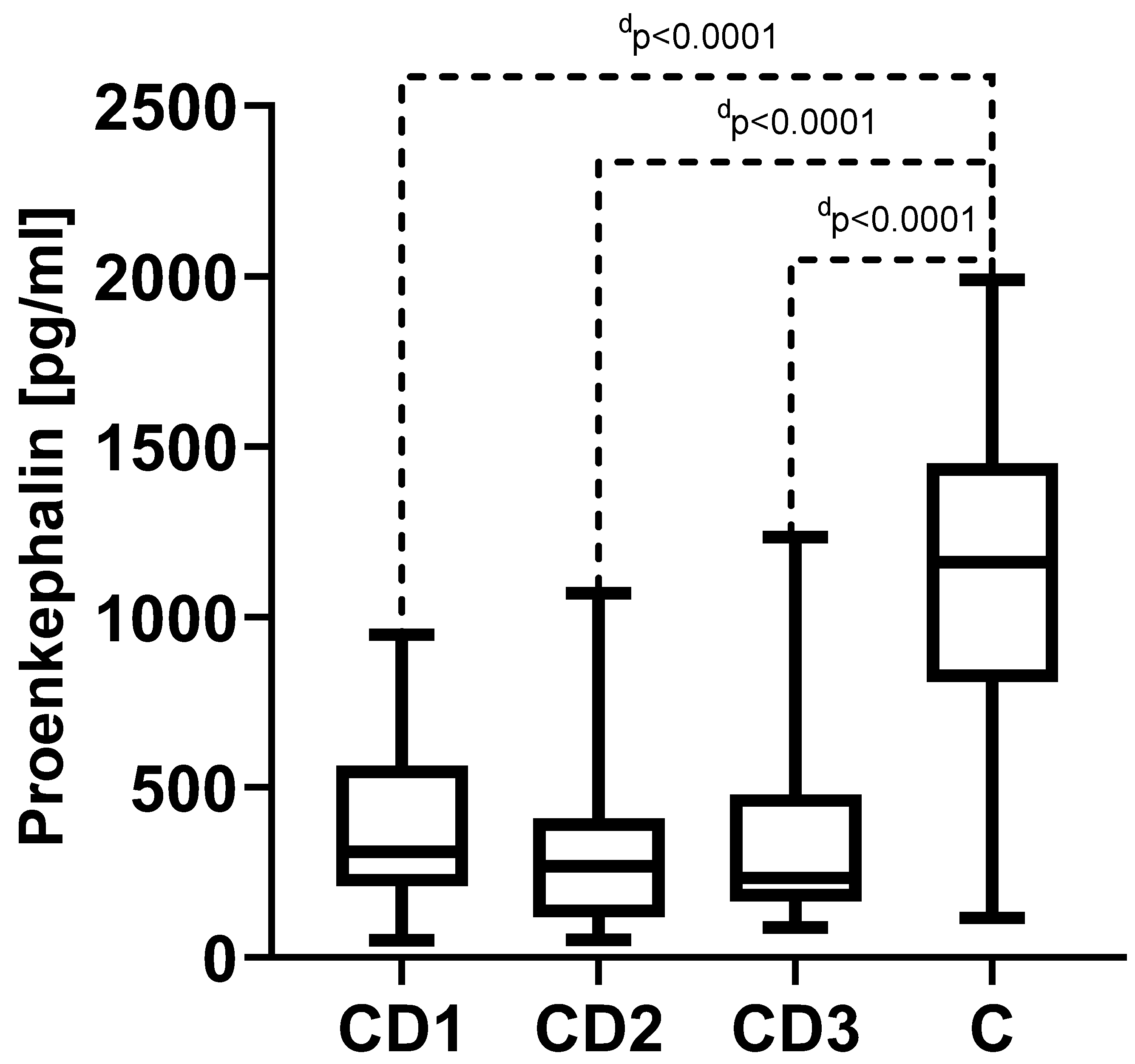
3.3. Proenkephalin (PENK)
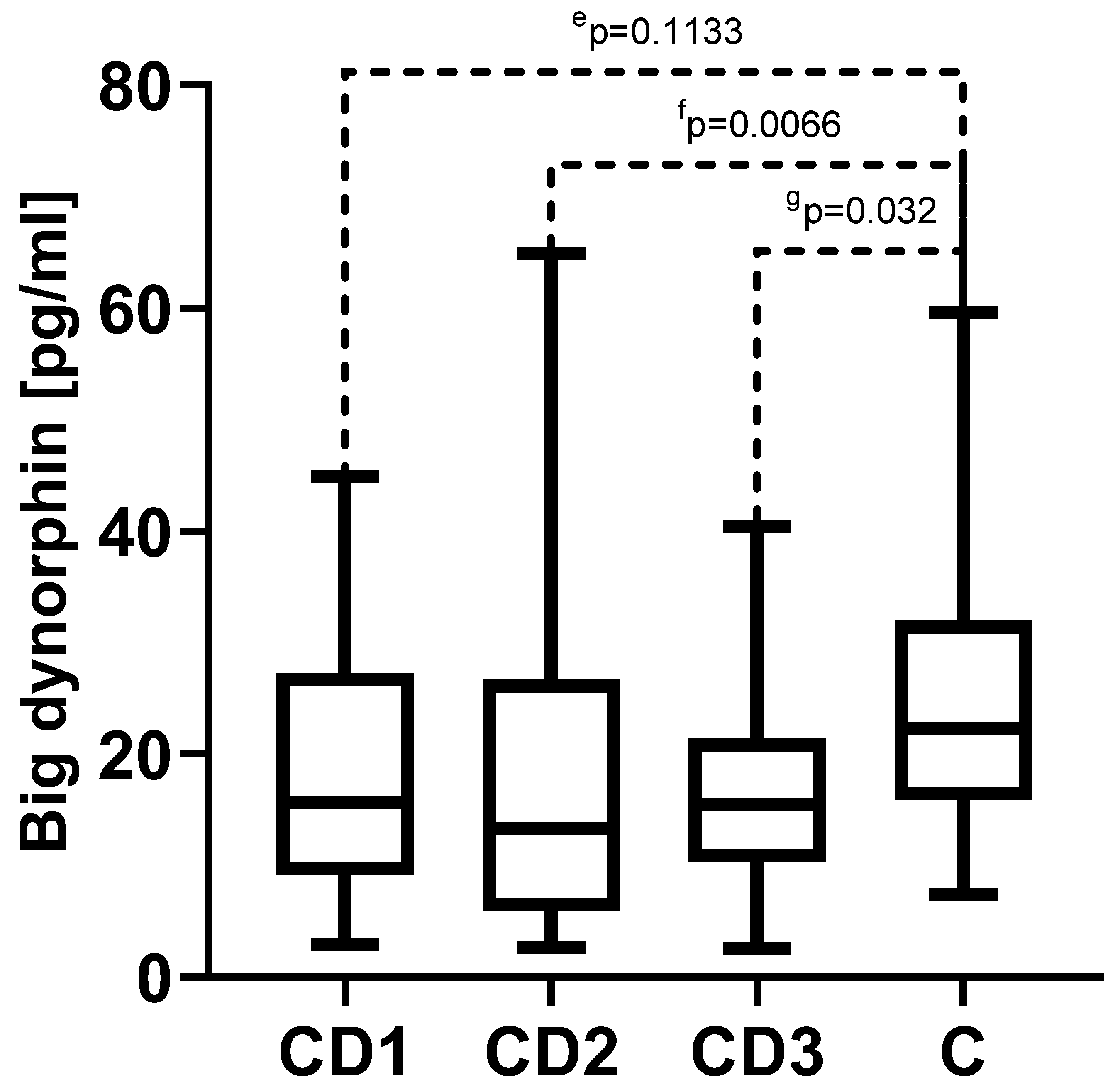
3.4. Big Dynorphin
4. Discussion
4.1. β-Endorphin
4.2. Enkephalins
4.3. Big Dynorphin
4.4. Limitations of this Study
4.5. Links to the Crohn’s Disease Course and Treatment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing Incidence and Prevalence of the Inflammatory Bowel Diseases with Time, Based on Systematic Review. Gastroenterology 2012, 142, 46–54.e42. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide Incidence and Prevalence of Inflammatory Bowel Disease in the 21st Century: A Systematic Review of Population-Based Studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Day, A.S.; Ledder, O.; Leach, S.T.; Lemberg, D.A. Crohn’s and Colitis in Children and Adolescents. World J. Gastroenterol. 2012, 18, 5862–5869. [Google Scholar] [CrossRef]
- Adolescent Health. Available online: https://www.who.int/health-topics/adolescent-health (accessed on 16 July 2023).
- Swidsinski, A.; Ladhoff, A.; Pernthaler, A.; Swidsinski, S.; Loening-Baucke, V.; Ortner, M.; Weber, J.; Hoffmann, U.; Schreiber, S.; Dietel, M.; et al. Mucosal Flora in Inflammatory Bowel Disease. Gastroenterology 2002, 122, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Nishida, A.; Inoue, R.; Inatomi, O.; Bamba, S.; Naito, Y.; Andoh, A. Gut Microbiota in the Pathogenesis of Inflammatory Bowel Disease. Clin. J. Gastroenterol. 2018, 11, 1–10. [Google Scholar] [CrossRef]
- Kowalska-Duplaga, K.; Gosiewski, T.; Kapusta, P.; Sroka-Oleksiak, A.; Wędrychowicz, A.; Pieczarkowski, S.; Ludwig-Słomczyńska, A.H.; Wołkow, P.P.; Fyderek, K. Differences in the Intestinal Microbiome of Healthy Children and Patients with Newly Diagnosed Crohn’s Disease. Sci. Rep. 2019, 9, 18880. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s Disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Frigstad, S.O.; Høivik, M.L.; Jahnsen, J.; Cvancarova, M.; Grimstad, T.; Berset, I.P.; Huppertz-Hauss, G.; Hovde, Ø.; Bernklev, T.; Moum, B.; et al. Pain Severity and Vitamin D Deficiency in IBD Patients. Nutrients 2019, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Patten, D.K.; Schultz, B.G.; Berlau, D.J. The Safety and Efficacy of Low-Dose Naltrexone in the Management of Chronic Pain and Inflammation in Multiple Sclerosis, Fibromyalgia, Crohn’s Disease, and Other Chronic Pain Disorders. Pharmacotherapy 2018, 38, 382–389. [Google Scholar] [CrossRef]
- Szigethy, E.; Knisely, M.; Drossman, D. Opioid Misuse in Gastroenterology and Non-Opioid Management of Abdominal Pain. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 168–180. [Google Scholar] [CrossRef]
- Stein, C. Opioids, Sensory Systems and Chronic Pain. Eur. J. Pharmacol. 2013, 716, 179–187. [Google Scholar] [CrossRef]
- Li, J.-P.; Wang, X.-Y.; Gao, C.-J.; Liao, Y.-H.; Qu, J.; He, Z.-Y.; Zhang, T.; Wang, G.-D.; Li, Y.-Q. Neurochemical Phenotype and Function of Endomorphin 2-Immunopositive Neurons in the Myenteric Plexus of the Rat Colon. Front. Neuroanat. 2014, 8, 149. [Google Scholar] [CrossRef]
- Kocot-Kępska, M.; Zajączkowska, R.; Przeklasa-Muszyńska, A.; Dobrogowski, J. The Role of Oxycodone/Naloxone in Pain Management. BÓL 2017, 17, 26–40. [Google Scholar] [CrossRef]
- Holzer, P. Opioid Receptors in the Gastrointestinal Tract. Regul. Pept. 2009, 155, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, R.J. Endogenous Opiates and Behavior: 2016. Peptides 2018, 101, 167–212. [Google Scholar] [CrossRef]
- Kromer, W. Endogenous Opioids, the Enteric Nervous System and Gut Motility. Dig. Dis. 1990, 8, 361–373. [Google Scholar] [CrossRef]
- Zollner, C.; Shaqura, M.A.; Bopaiah, C.P.; Mousa, S.; Stein, C.; Schafer, M. Painful Inflammation-Induced Increase in Mu-Opioid Receptor Binding and G-Protein Coupling in Primary Afferent Neurons. Mol. Pharmacol. 2003, 64, 202–210. [Google Scholar] [CrossRef]
- Stein, C. Opioid Receptors on Peripheral Sensory Neurons. In Madame Curie Bioscience Database [Internet]; Landes Bioscience: Austin, TX, USA, 2013. [Google Scholar]
- Sternini, C.; Patierno, S.; Selmer, I.-S.; Kirchgessner, A. The Opioid System in the Gastrointestinal Tract. Neurogastroenterol. Motil. 2004, 16 (Suppl. S2), 3–16. [Google Scholar] [CrossRef]
- Rueda-Ruzafa, L.; Cruz, F.; Cardona, D.; Hone, A.J.; Molina-Torres, G.; Sánchez-Labraca, N.; Roman, P. Opioid System Influences Gut-Brain Axis: Dysbiosis and Related Alterations. Pharmacol. Res. 2020, 159, 104928. [Google Scholar] [CrossRef]
- Thompson, G.L.; Canals, M.; Poole, D.P. Biological Redundancy of Endogenous GPCR Ligands in the Gut and the Potential for Endogenous Functional Selectivity. Front. Pharmacol. 2014, 5, 262. [Google Scholar] [CrossRef] [PubMed]
- Toubia, T.; Khalife, T. The Endogenous Opioid System: Role and Dysfunction Caused by Opioid Therapy. Clin. Obstet. Gynecol. 2019, 62, 3. [Google Scholar] [CrossRef] [PubMed]
- Mani, A.R.; Moore, K.P. New Insights into the Role of Endogenous Opioids in the Pathogenesis of Gastrointestinal and Liver Disease. Gut 2009, 58, 893–895. [Google Scholar] [CrossRef] [PubMed]
- Kienzl, M.; Storr, M.; Schicho, R. Cannabinoids and Opioids in the Treatment of Inflammatory Bowel Diseases. Clin. Transl. Gastroenterol. 2020, 11, e00120. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Liu, R.; Chen, C.; Ji, F.; Li, T. Opioid System Modulates the Immune Function: A Review. Transl. Perioper. Pain. Med. 2016, 1, 5–13. [Google Scholar]
- Plein, L.M.; Rittner, H.L. Opioids and the Immune System–Friend or Foe. Br. J. Pharmacol. 2018, 175, 2717–2725. [Google Scholar] [CrossRef]
- Stein, C. Opioid Receptors. Annu. Rev. Med. 2016, 67, 433–451. [Google Scholar] [CrossRef]
- Fricker, L.D.; Margolis, E.B.; Gomes, I.; Devi, L.A. Five Decades of Research on Opioid Peptides: Current Knowledge and Unanswered Questions. Mol. Pharmacol. 2020, 98, 96–108. [Google Scholar] [CrossRef]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.-L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar] [CrossRef]
- Bagley, E.E.; Ingram, S.L. Endogenous Opioid Peptides in the Descending Pain Modulatory Circuit. Neuropharmacology 2020, 173, 108131. [Google Scholar] [CrossRef]
- Wiedermann, C.J.; Sacerdote, P.; Propst, A.; Propst, T.; Judmaier, G.; Kathrein, H.; Vogel, W.; Panerai, A.E. Decreased Beta-Endorphin Content in Peripheral Blood Mononuclear Leukocytes from Patients with Crohn’s Disease. Brain Behav. Immun. 1994, 8, 261–269. [Google Scholar] [CrossRef]
- Kuroki, T.; Ohta, A.; Sherriff-Tadano, R.; Matsuura, E.; Takashima, T.; Iwakiri, R.; Fujimoto, K. Imbalance in the Stress-Adaptation System in Patients with Inflammatory Bowel Disease. Biol. Res. Nurs. 2011, 13, 391–398. [Google Scholar] [CrossRef]
- Owczarek, D.; Cibor, D.; Mach, T.; Cieśla, A.; Pierzchała-Koziec, K.; Sałapa, K.; Kuśnierz-Cabała, B. Met-Enkephalins in Patients with Inflammatory Bowel Diseases. Adv. Med. Sci. 2011, 56, 158–164. [Google Scholar] [CrossRef]
- Zatorski, H.; Sałaga, M.; Fichna, J. Role of Glucagon-like Peptides in Inflammatory Bowel Diseases-Current Knowledge and Future Perspectives. Naunyn Schmiedebergs Arch. Pharmacol. 2019, 392, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Eberlin, M.; Chen, M.; Mueck, T.; Däbritz, J. Racecadotril in the Treatment of Acute Diarrhea in Children: A Systematic, Comprehensive Review and Meta-Analysis of Randomized Controlled Trials. BMC Pediatr. 2018, 18, 124. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, Y.; Gong, J.; Zhu, W. Frequency and Risk Factors of Surgical Recurrence of Crohn’s Disease after Primary Bowel Resection. Turk. J. Gastroenterol. 2018, 29, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Battat, R.; Parker, C.E.; Khanna, R.; Jairath, V.; Feagan, B.G. Update on C-Reactive Protein and Fecal Calprotectin: Are They Accurate Measures of Disease Activity in Crohn’s Disease? Expert. Rev. Gastroenterol. Hepatol. 2019, 13, 319–330. [Google Scholar] [CrossRef]
- Faouzi, A.; Varga, B.R.; Majumdar, S. Biased Opioid Ligands. Molecules 2020, 25, 4257. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, X.; Liu, C.; Kang, J.; Yang, J.; Pei, G.; Wu, C. Improvement of Morphine-Mediated Analgesia by Inhibition of β-Arrestin 2 Expression in Mice Periaqueductal Gray Matter. Int. J. Mol. Sci. 2009, 10, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-H.; Huang, H.-W.; Chen, K.-H.; Chen, Y.-S.; Sheen-Chen, S.-M.; Lin, C.-R. Antinociceptive Potentiation and Attenuation of Tolerance by Intrathecal β-Arrestin 2 Small Interfering RNA in Rats. Br. J. Anaesth. 2011, 107, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Ehrich, J.M.; Messinger, D.I.; Knakal, C.R.; Kuhar, J.R.; Schattauer, S.S.; Bruchas, M.R.; Zweifel, L.S.; Kieffer, B.L.; Phillips, P.E.M.; Chavkin, C. Kappa Opioid Receptor-Induced Aversion Requires P38 MAPK Activation in VTA Dopamine Neurons. J. Neurosci. 2015, 35, 12917–12931. [Google Scholar] [CrossRef]
- Moran, G.W.; Leslie, F.C.; McLaughlin, J.T. Crohn’s Disease Affecting the Small Bowel Is Associated with Reduced Appetite and Elevated Levels of Circulating Gut Peptides. Clin. Nutr. 2013, 32, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Matafome, P.; Seiça, R. The Role of Brain in Energy Balance. Adv. Neurobiol. 2017, 19, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Anbazhagan, A.N.; Priyamvada, S.; Alrefai, W.A.; Dudeja, P.K. Pathophysiology of IBD Associated Diarrhea. Tissue Barriers 2018, 6, e1463897. [Google Scholar] [CrossRef]
- Lee, M.Y.; Eads, R.; Yates, N.; Liu, C. Lived Experiences of a Sustained Mental Health Recovery Process without Ongoing Medication Use. Community Ment. Health J. 2021, 57, 540–551. [Google Scholar] [CrossRef]
- Hegadoren, K.M.; O’Donnell, T.; Lanius, R.; Coupland, N.J.; Lacaze-Masmonteil, N. The Role of Beta-Endorphin in the Pathophysiology of Major Depression. Neuropeptides 2009, 43, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Dinas, P.C.; Koutedakis, Y.; Flouris, A.D. Effects of Exercise and Physical Activity on Depression. Ir. J. Med. Sci. 2011, 180, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Quezada, S.M.; Cross, R.K. Cannabis and Turmeric as Complementary Treatments for IBD and Other Digestive Diseases. Curr. Gastroenterol. Rep. 2019, 21, 2. [Google Scholar] [CrossRef] [PubMed]
- Jeske, N.A. Dynamic Opioid Receptor Regulation in the Periphery. Mol. Pharmacol. 2019, 95, 463–467. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martyniak, A.; Wędrychowicz, A.; Tomasik, P.J. Endogenous Opioids in Crohn’s Disease. Biomedicines 2023, 11, 2037. https://doi.org/10.3390/biomedicines11072037
Martyniak A, Wędrychowicz A, Tomasik PJ. Endogenous Opioids in Crohn’s Disease. Biomedicines. 2023; 11(7):2037. https://doi.org/10.3390/biomedicines11072037
Chicago/Turabian StyleMartyniak, Adrian, Andrzej Wędrychowicz, and Przemysław J. Tomasik. 2023. "Endogenous Opioids in Crohn’s Disease" Biomedicines 11, no. 7: 2037. https://doi.org/10.3390/biomedicines11072037
APA StyleMartyniak, A., Wędrychowicz, A., & Tomasik, P. J. (2023). Endogenous Opioids in Crohn’s Disease. Biomedicines, 11(7), 2037. https://doi.org/10.3390/biomedicines11072037