
Human Periapical Odontogenic Granulomas: Aspects of Microvessel Density (MVD), Heterogeneity of Blood Vessels and Mast Cells Density (MCD)

 ,
,  ,
,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Data
- Age: 18–70 years;
- Both genders;
- Scheduled patients with the indication of tooth extractions;
- The presence of periapical granuloma identified on the Panoramic Dental X-ray.
- Age under 18 years;
- Patients diagnosed with neoplasms;
- Patients with acute diseases of the oral mucosa;
- Patients with altered general conditions: leukemia, recent myocardial infarction or stroke in the last 6 months;
- Patients undergoing drug treatment for bone pathologies (e.g., bisphosphonates).
2.2. Tooth Extraction
2.3. Primary Processing
2.4. Morphologic Analysis
2.5. Immunohistochemical Technique
2.6. Microscopic Evaluation and Image Analysis
2.7. Quantification Method
2.8. Statistical Analysis
3. Results
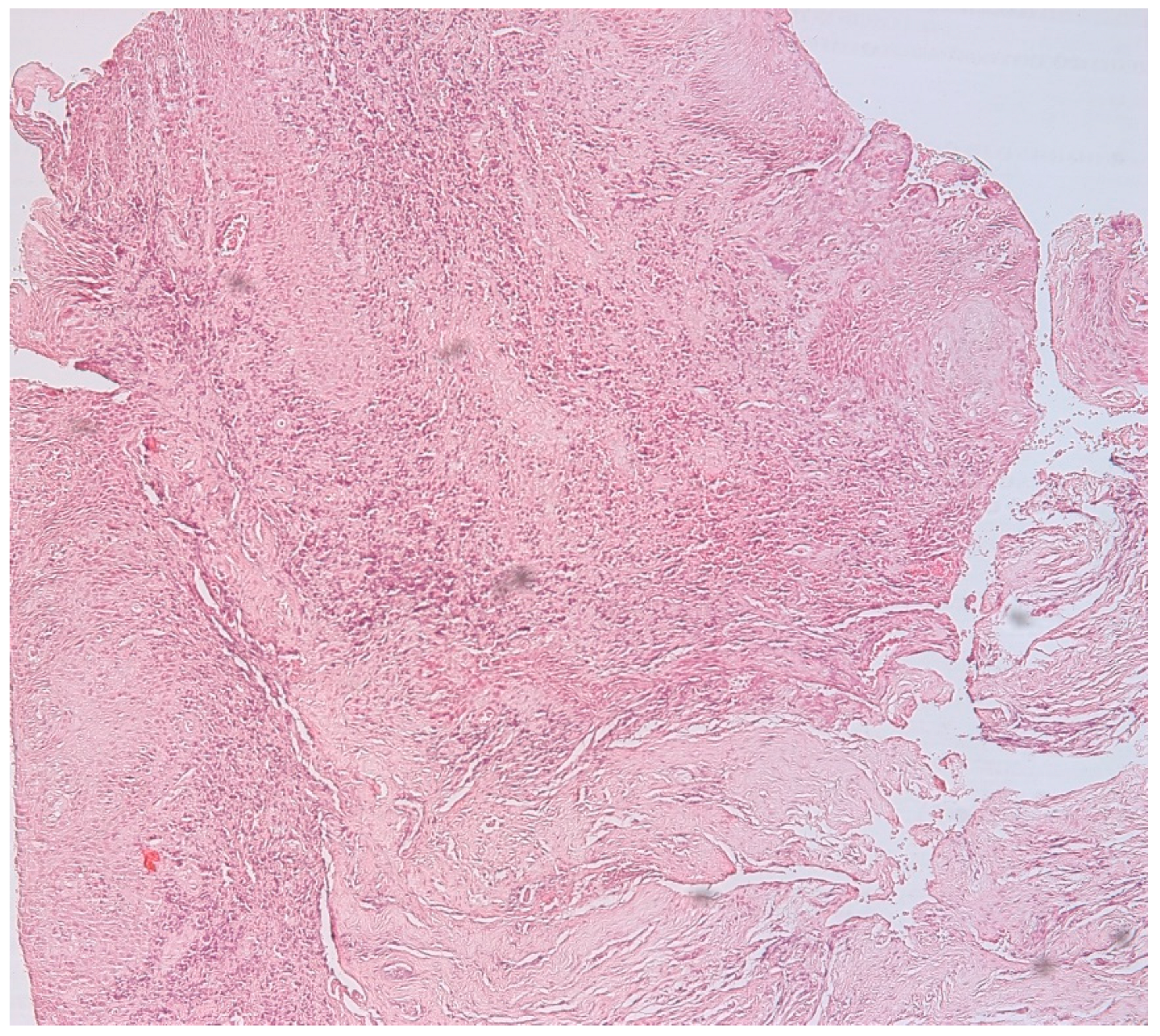
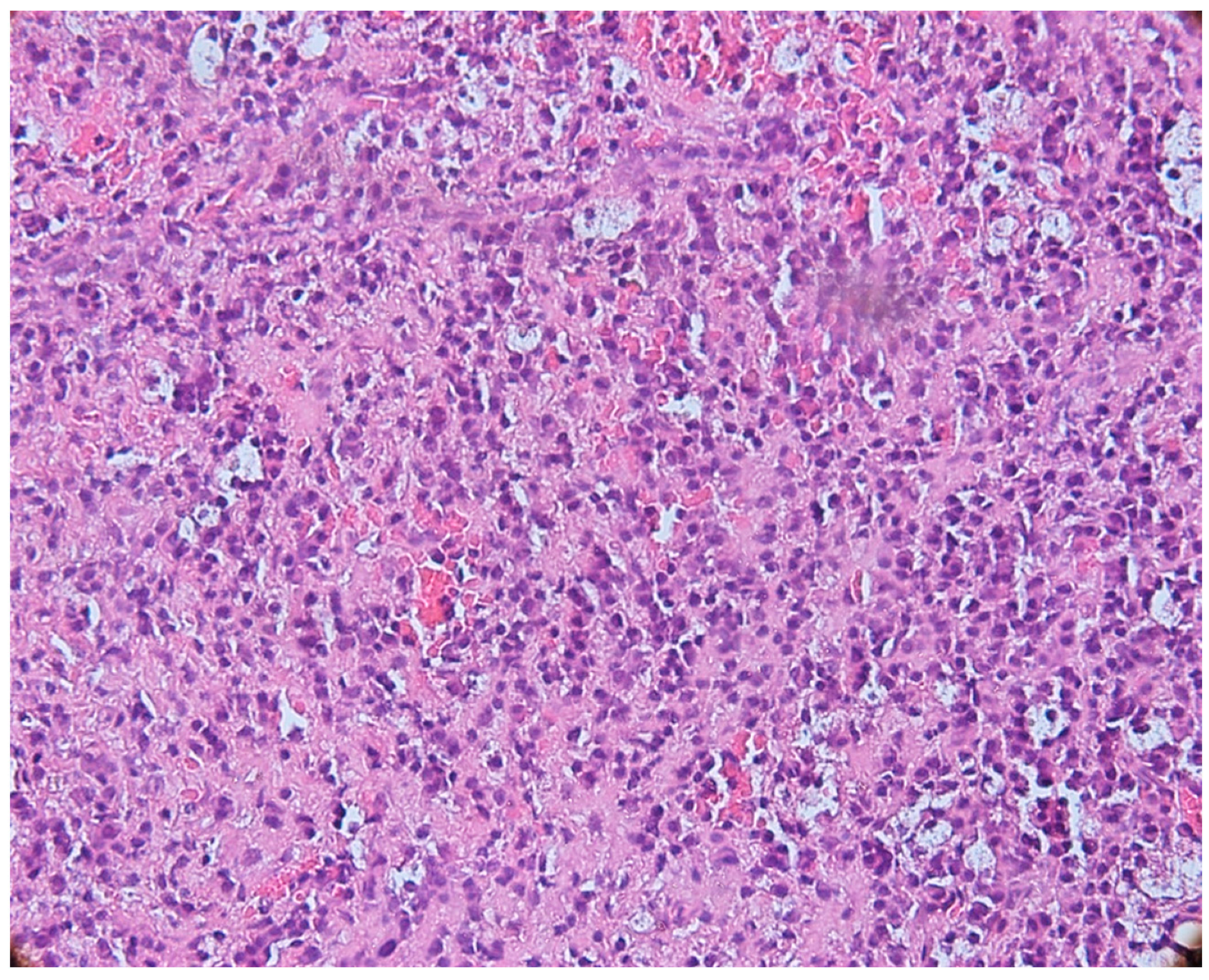
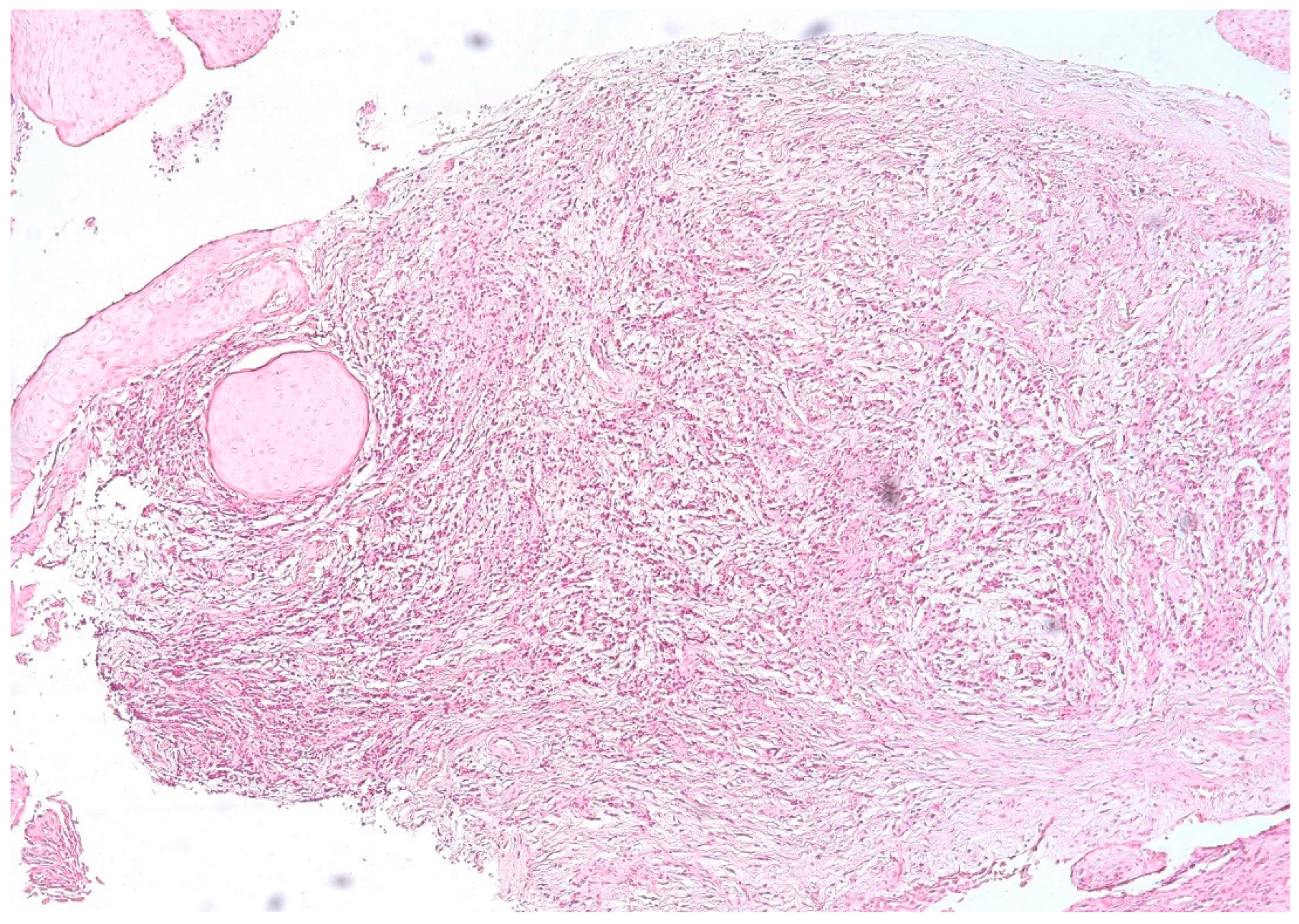
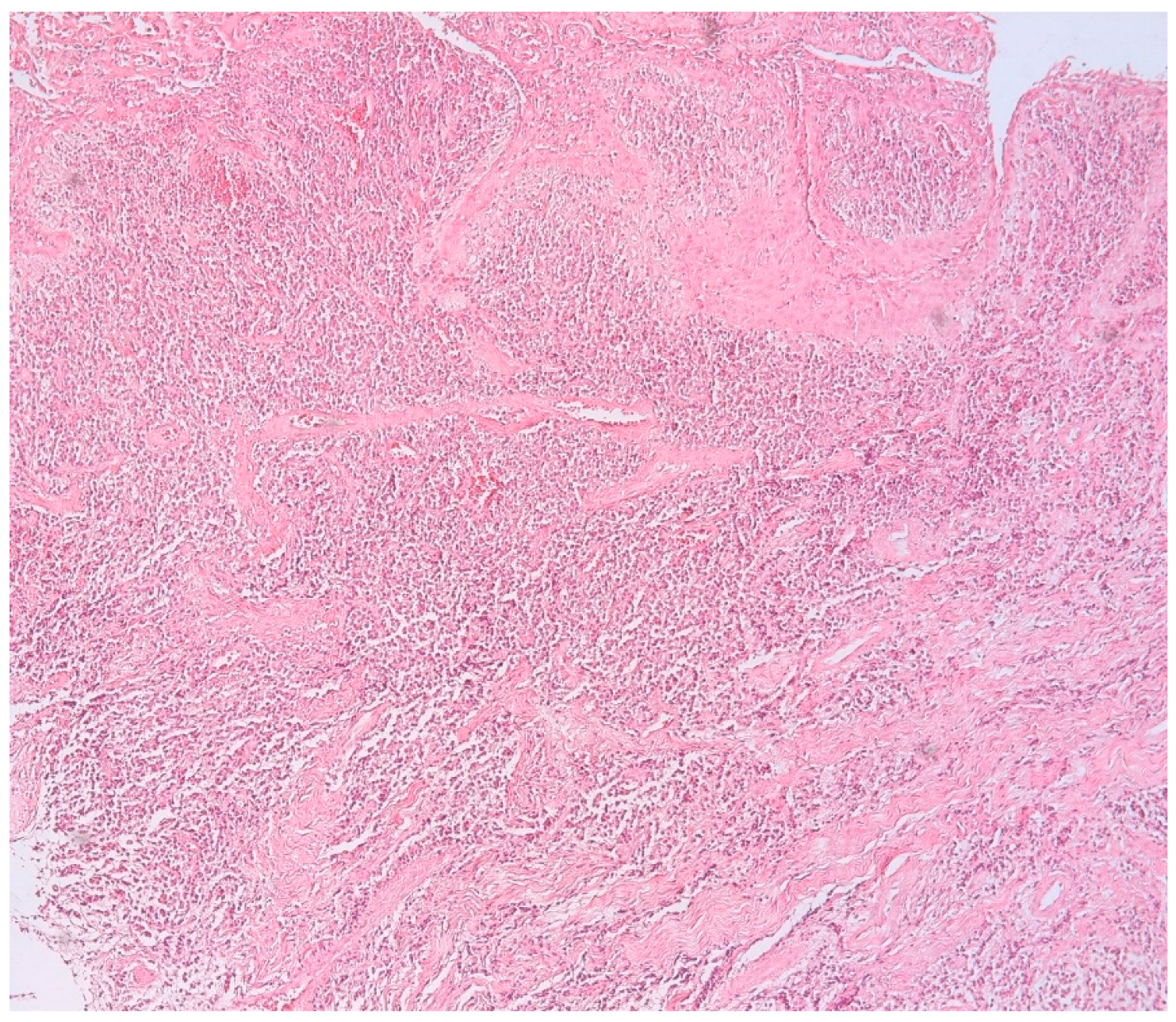
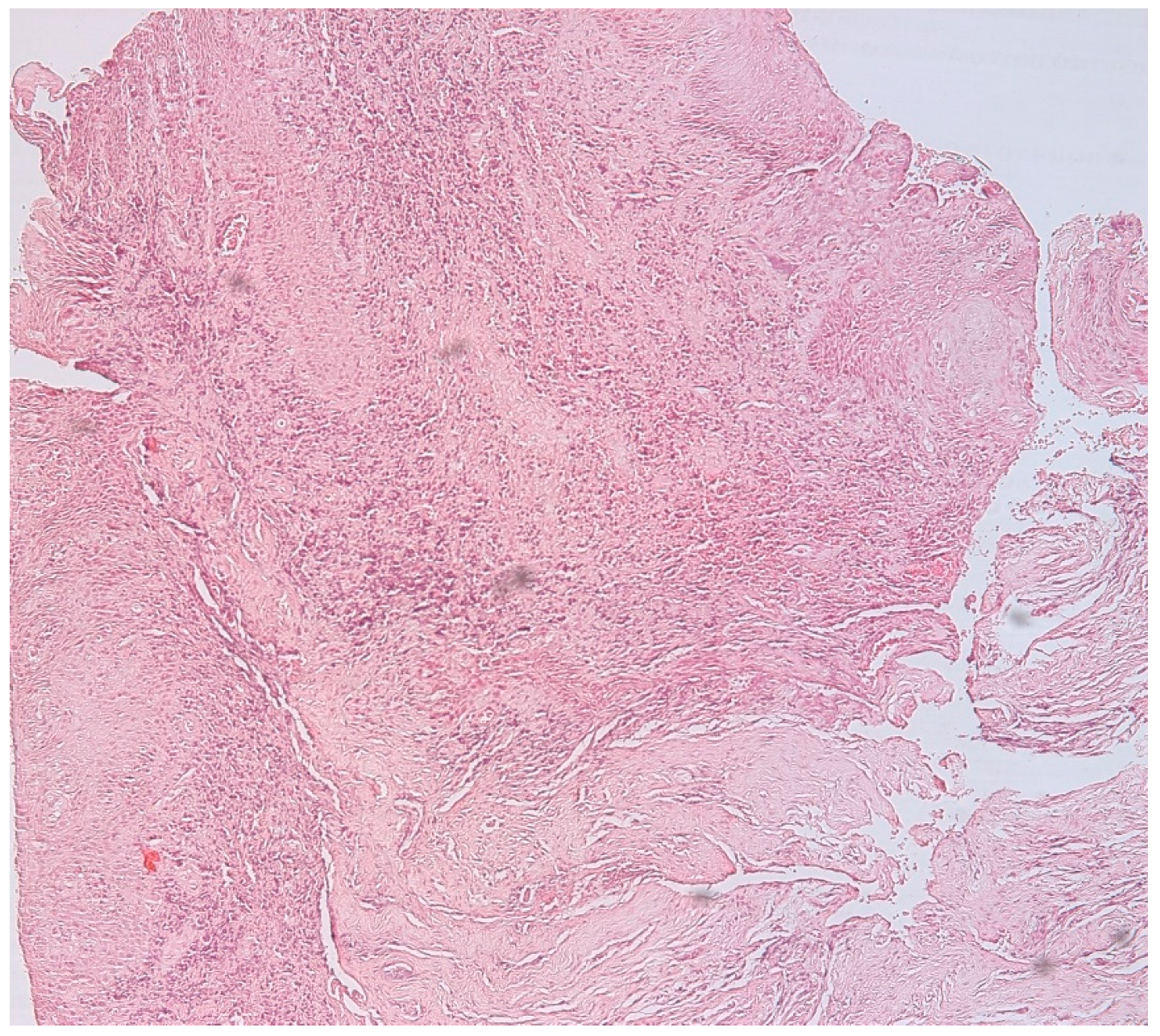
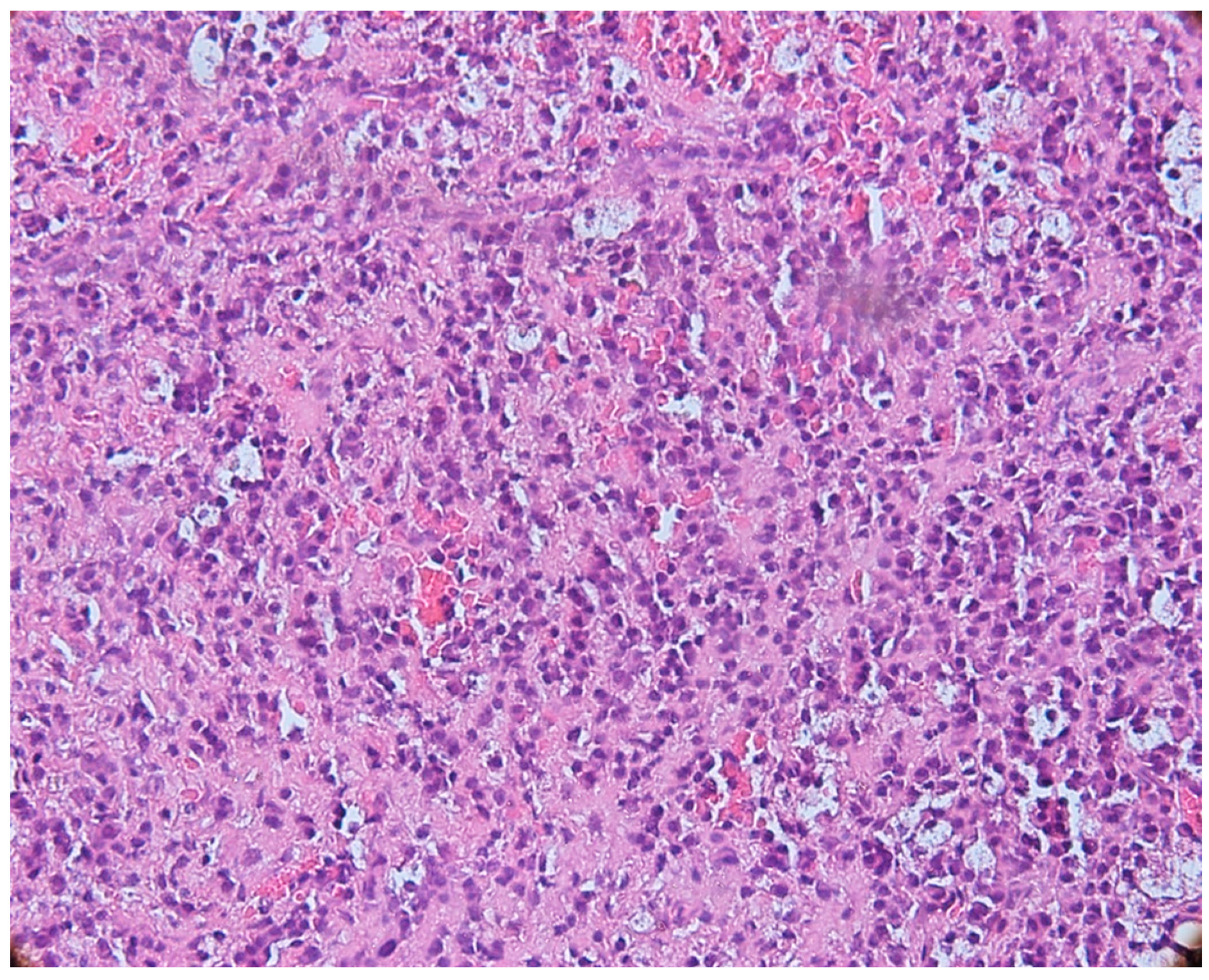
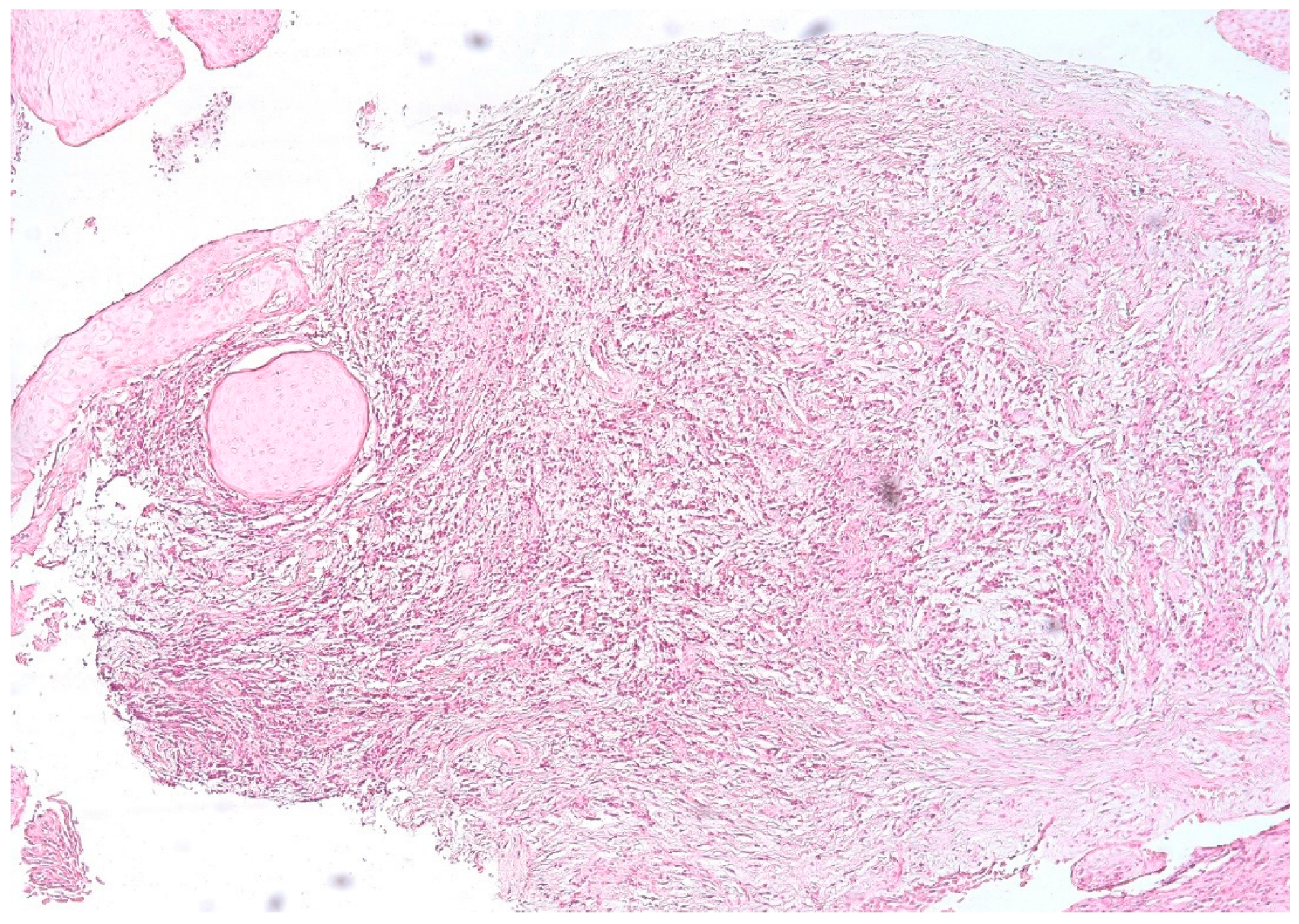
3.1. Morphologic Analysis
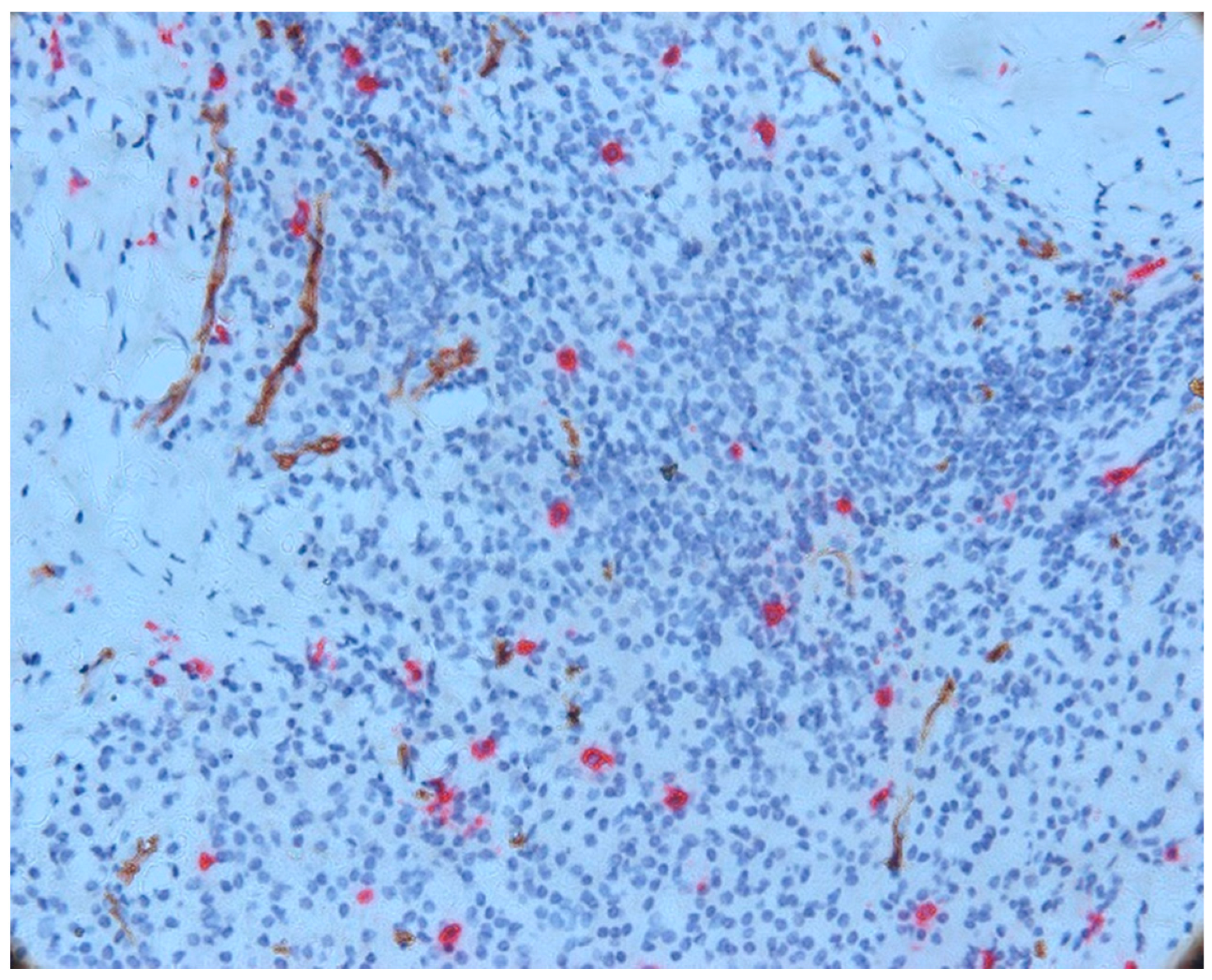
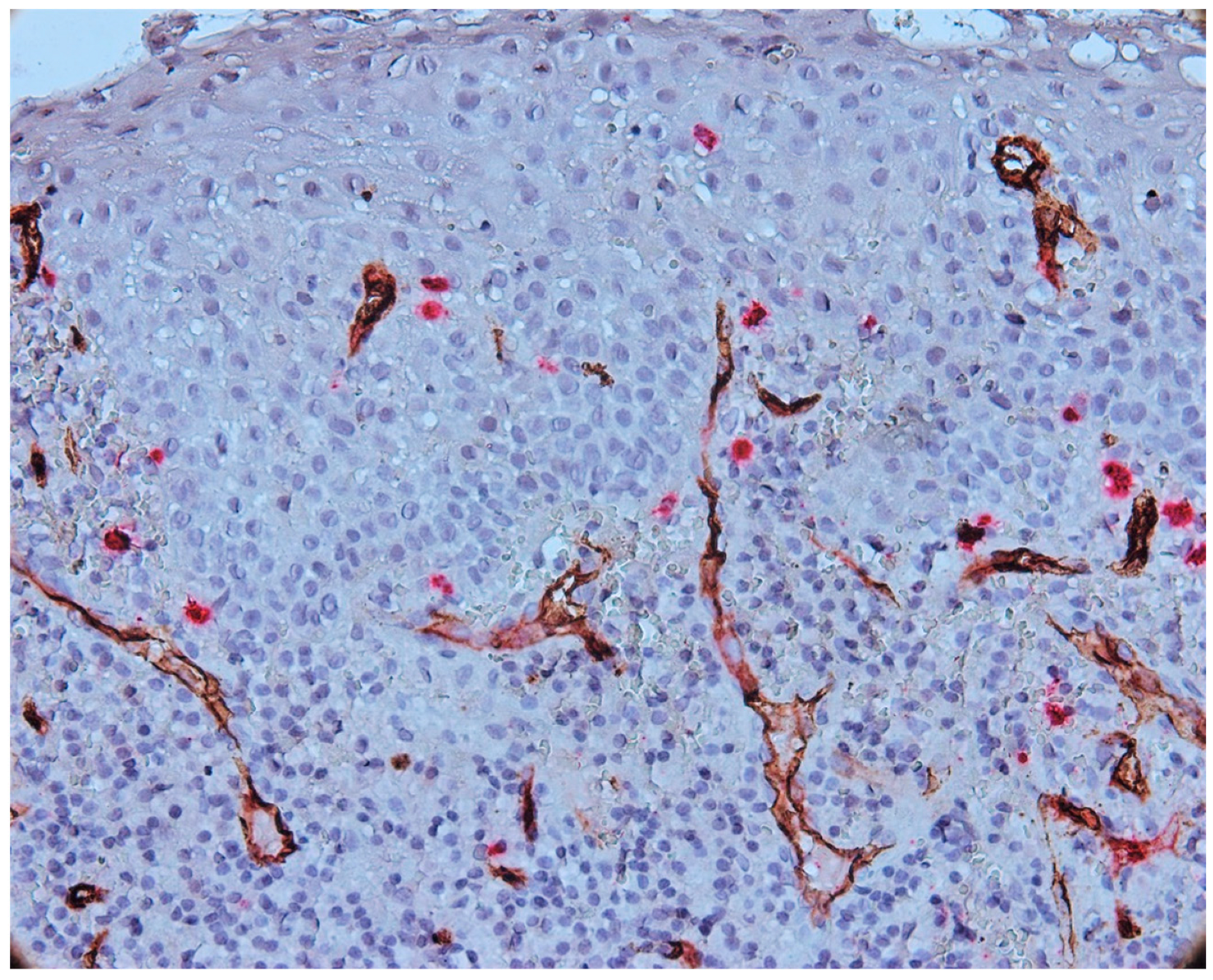
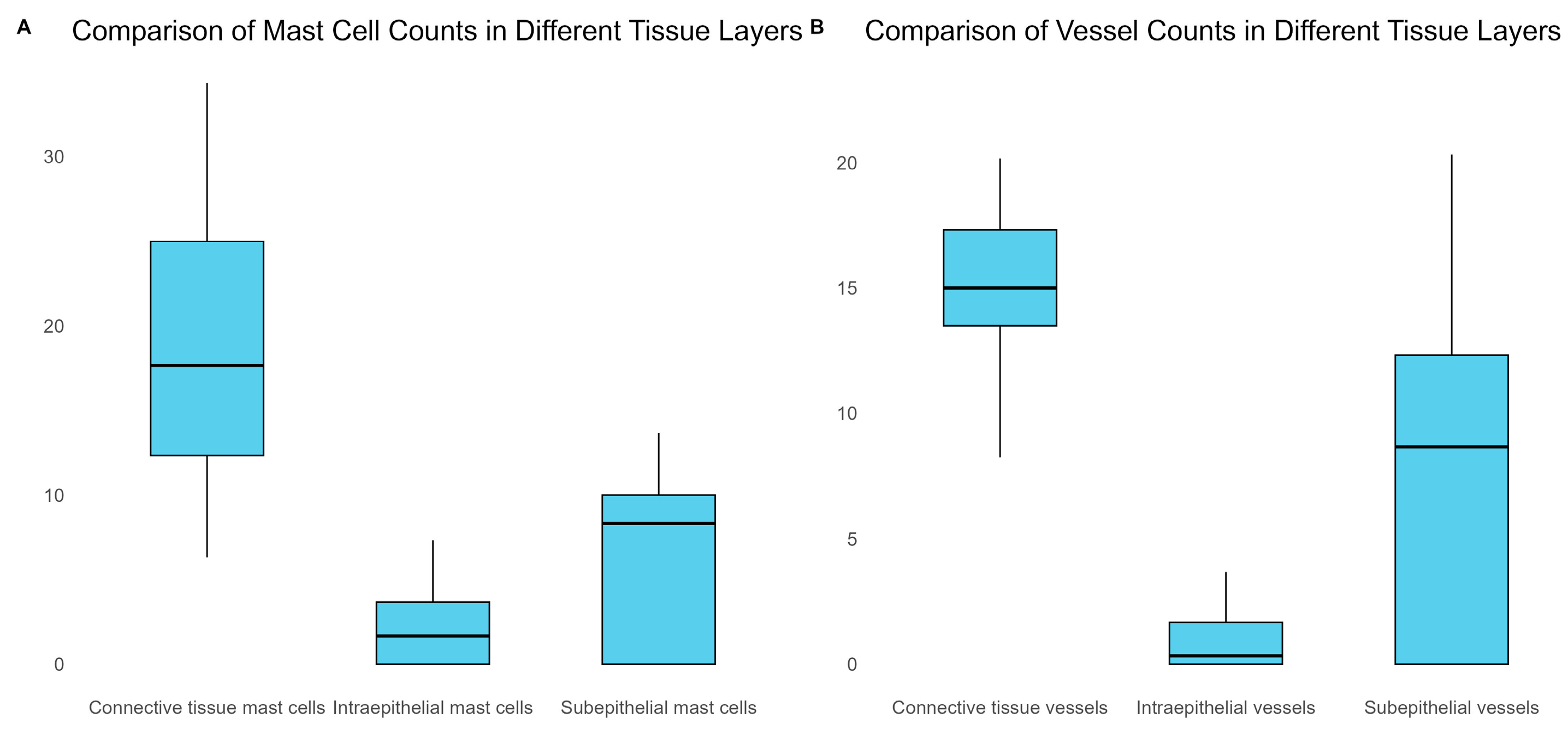
3.2. Mast Cells
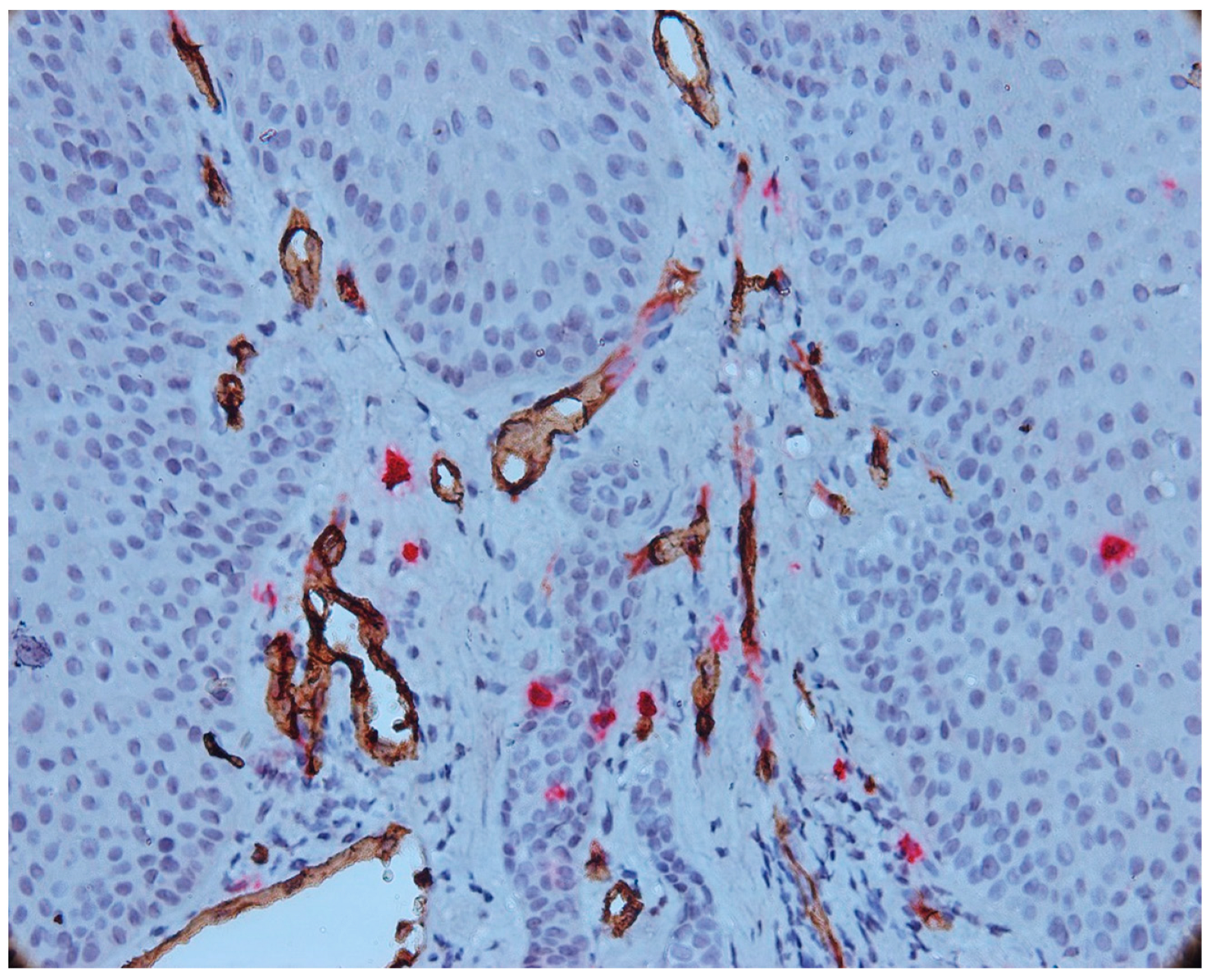
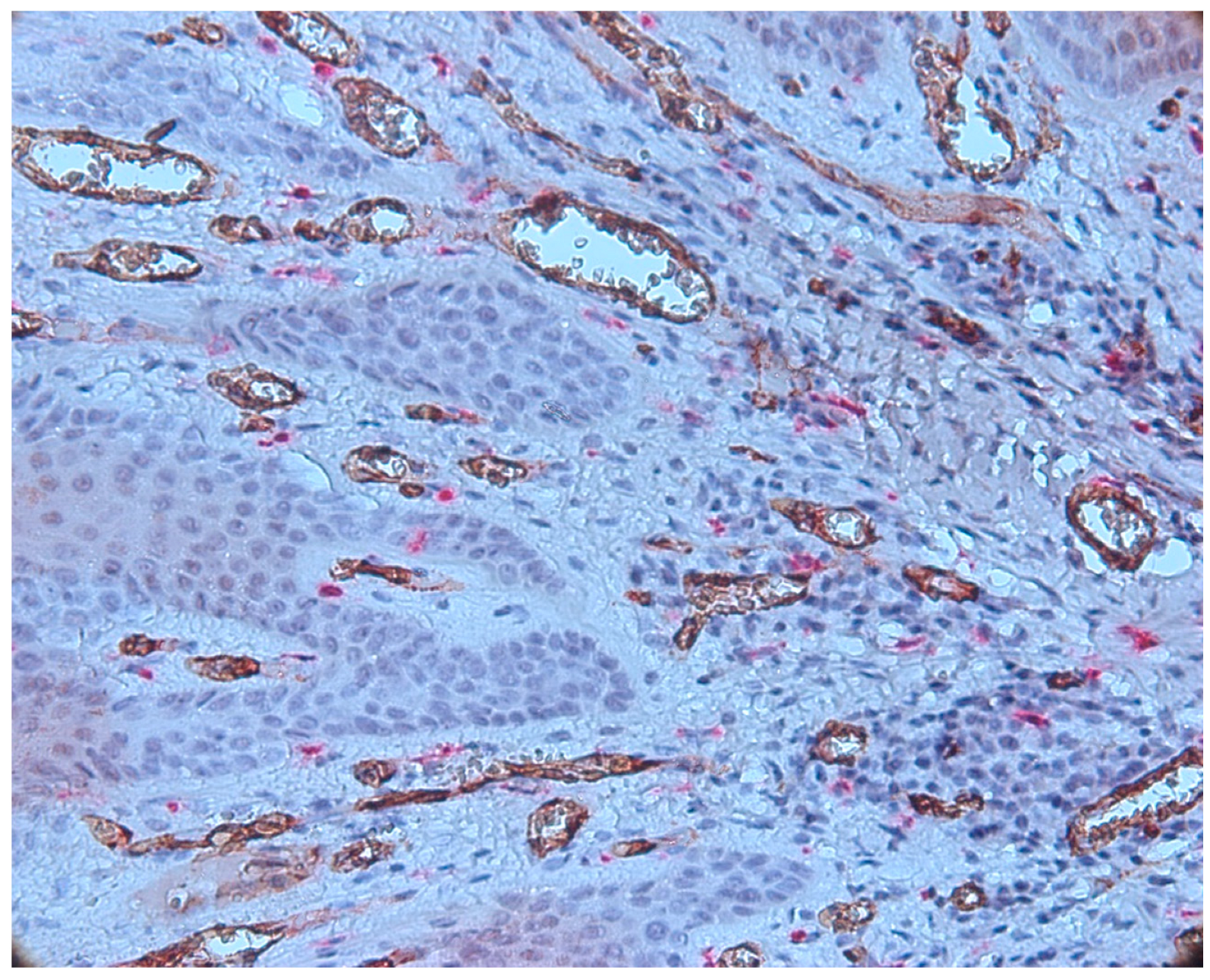
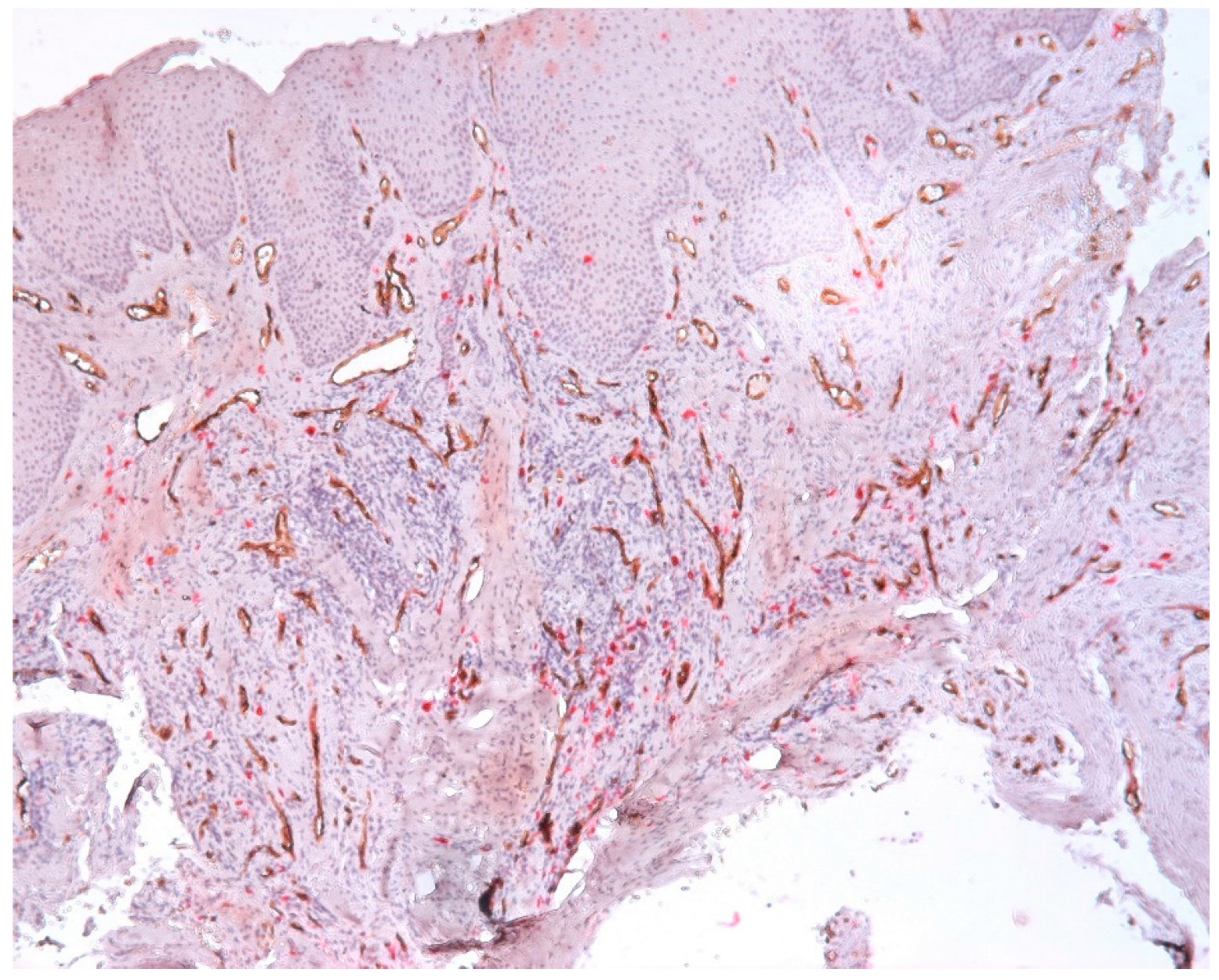
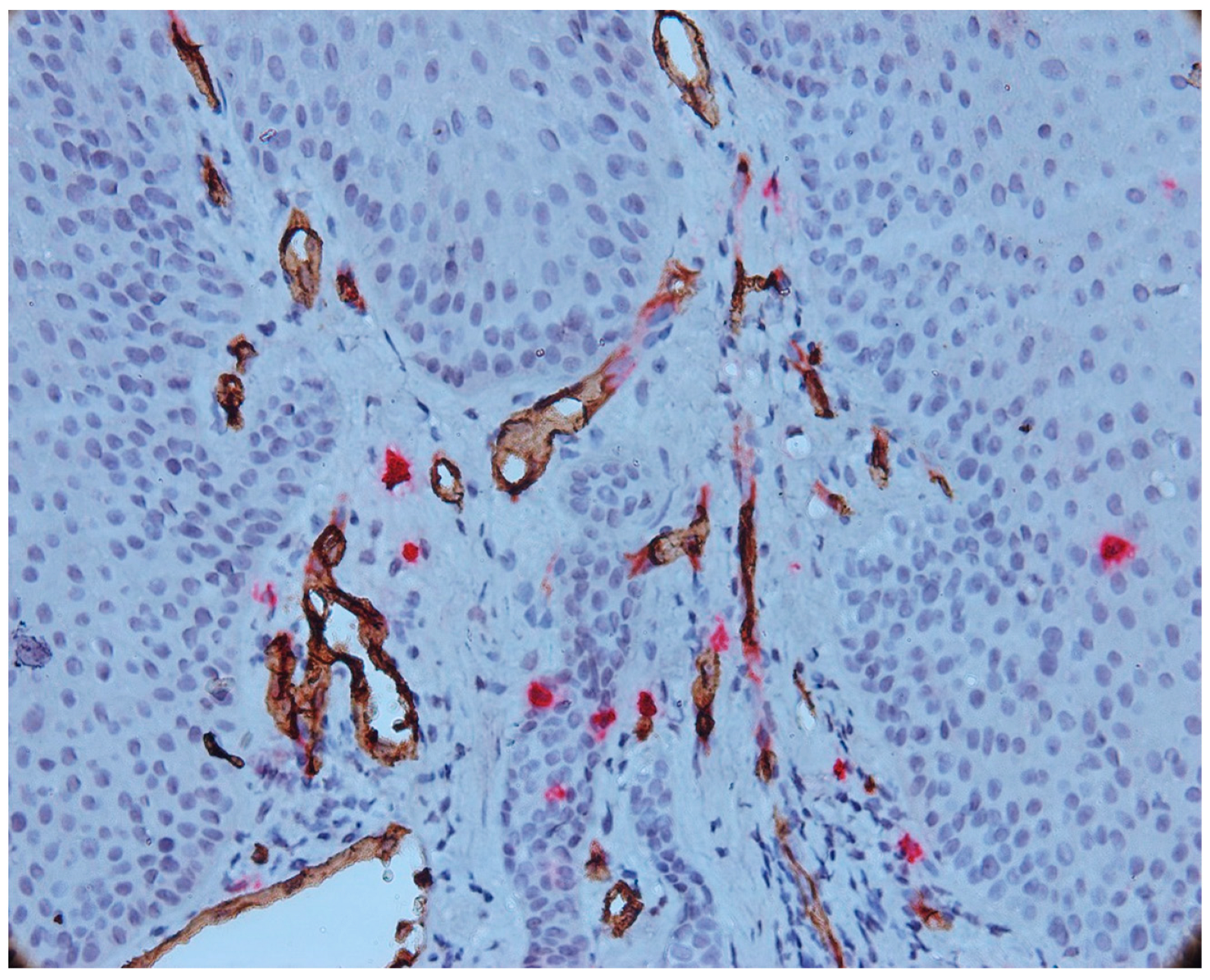
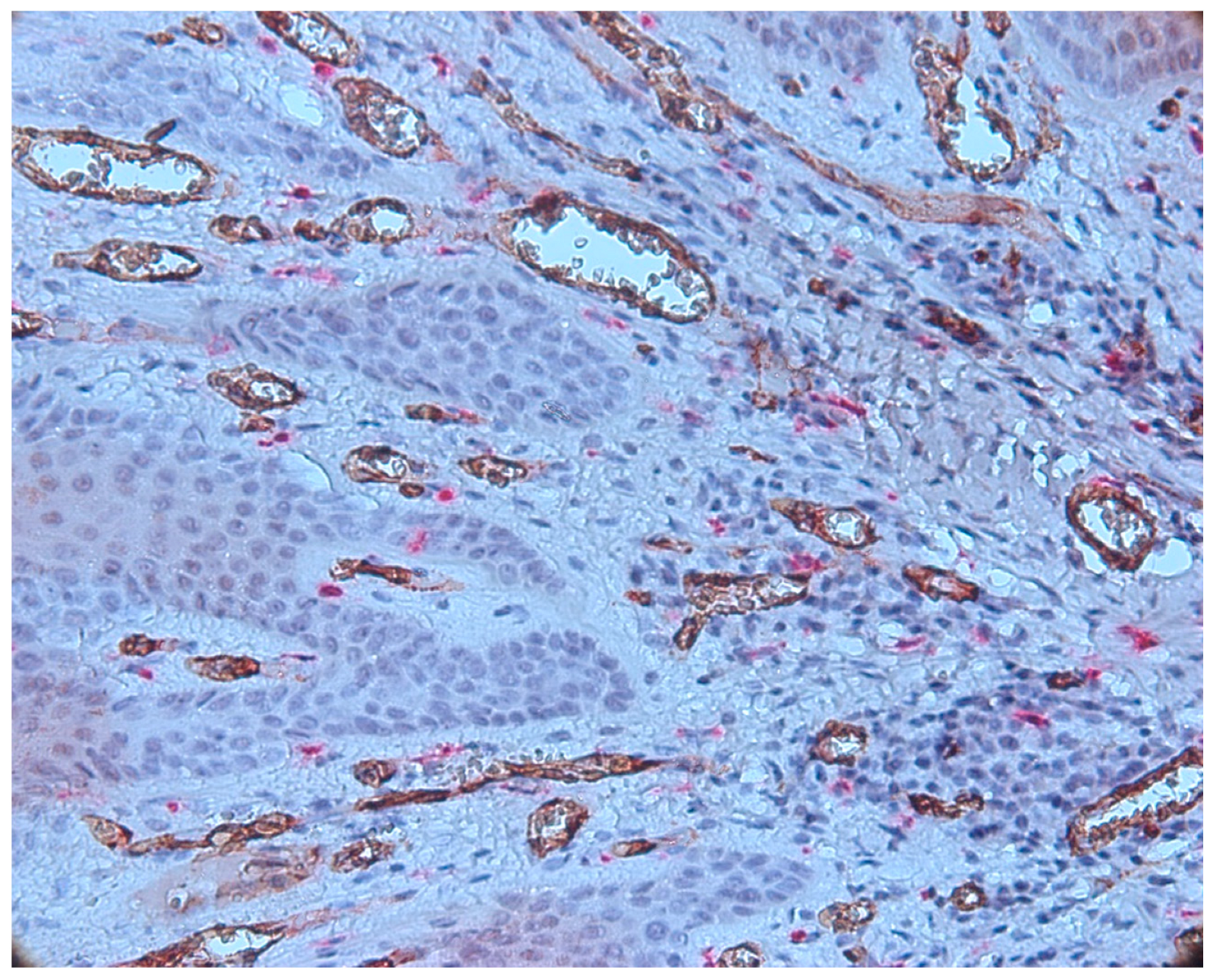
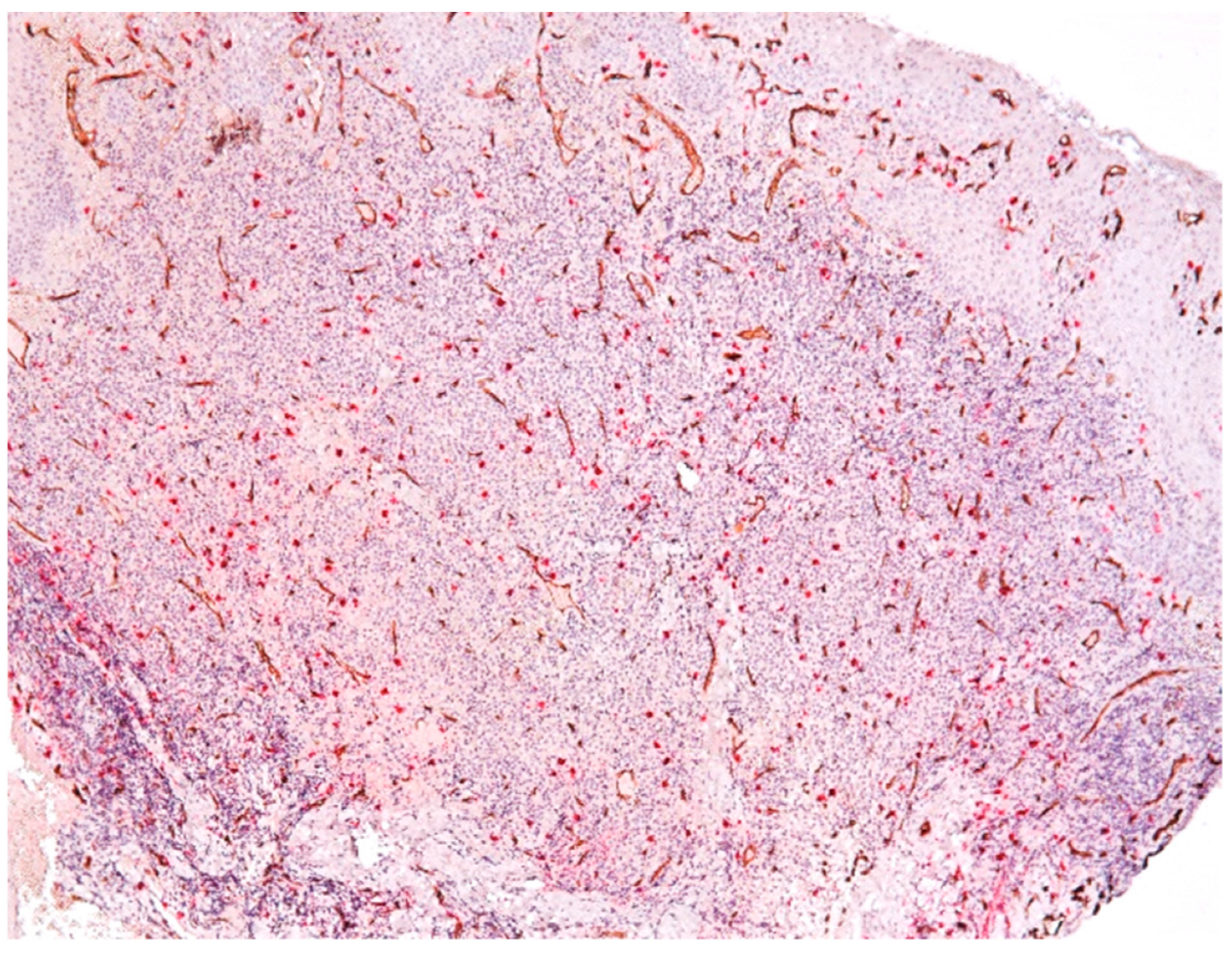
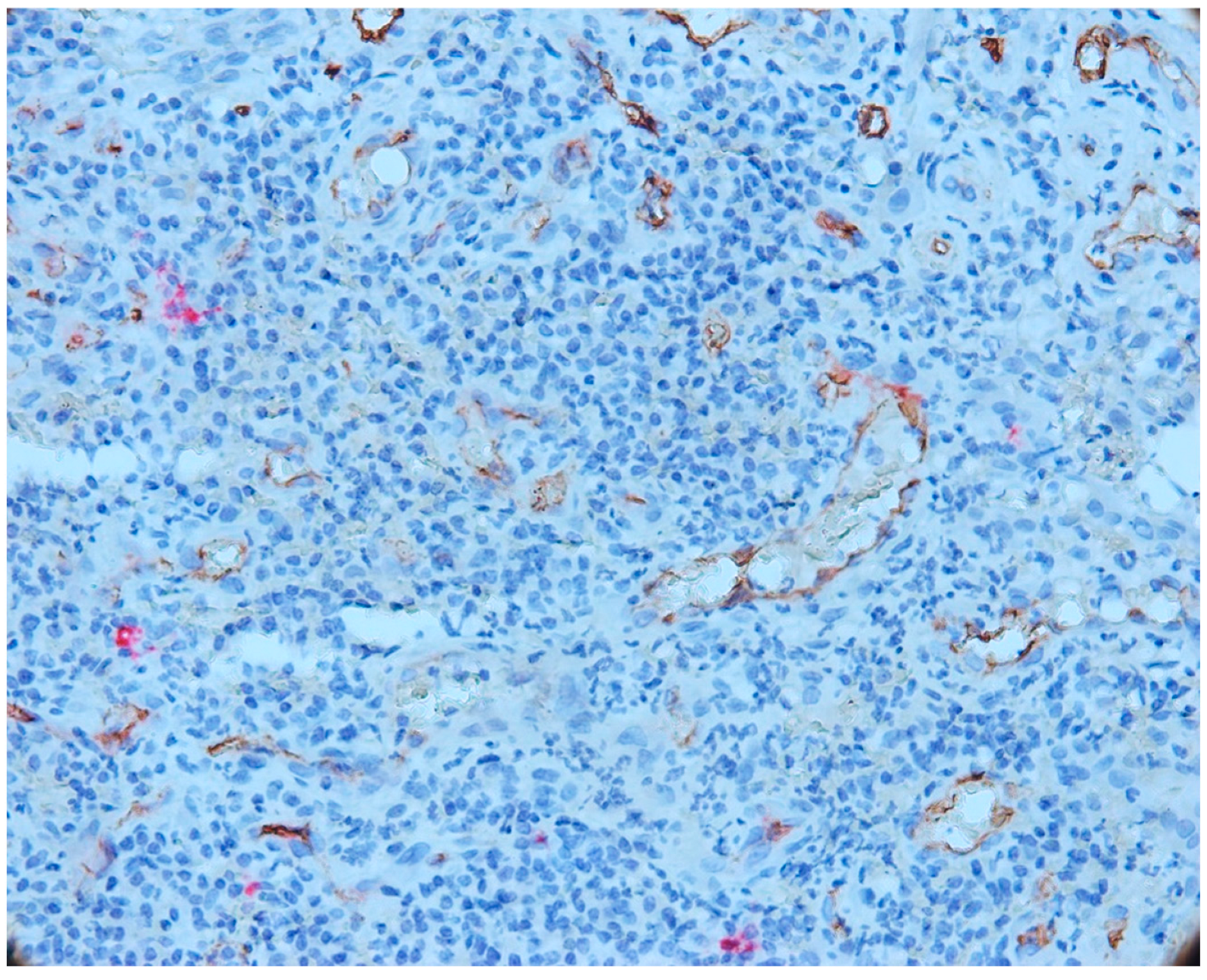
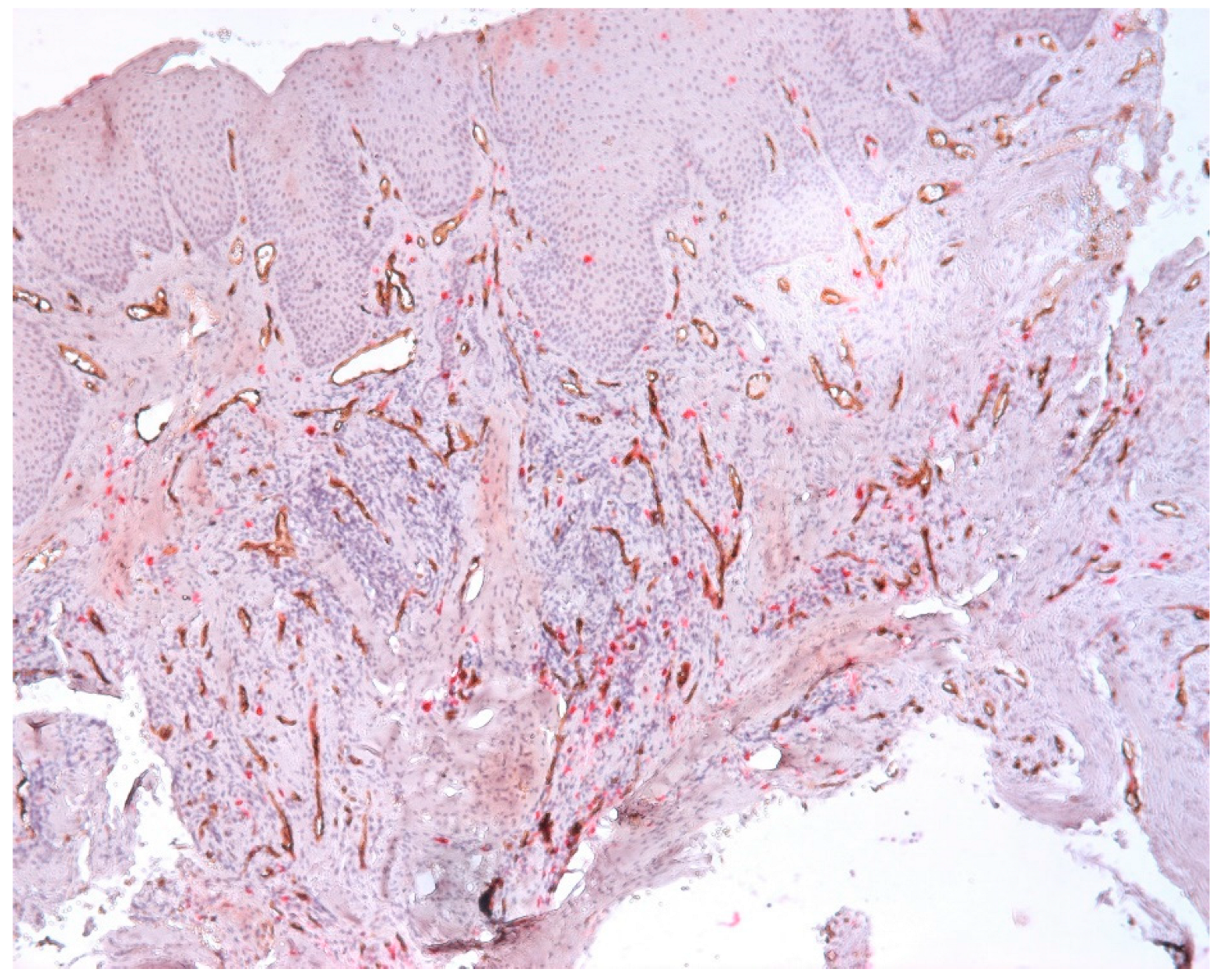
3.3. Aspects of Microvessels
3.4. MCD and MVD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diegues, L.L.; Colombo Robazza, C.R.; Costa Hanemann, J.A.; Costa Pereira, A.A.; Silva, C.O. Correlation between clinical and histopathological diagnoses in periapical inflammatory lesions. J. Investig. Clin. Dent. 2011, 2, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Berar, A.M.; Bondor, C.I.; Matroş, L.; Câmpian, R.S. Radiological, histological and immunohistochemical evaluation of periapical inflammatory lesions. Rom. J. Morphol. Embryol. 2016, 57, 419–425. [Google Scholar]
- Yamanaka, Y.; Kaneko, T.; Yoshiba, K.; Kaneko, R.; Yoshiba, N.; Shigetani, Y.; Nör, J.E.; Okiji, T. Expression of angiogenic factors in rat periapical lesions. J. Endod. 2012, 38, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Stashenko, P.; Teles, R.; D’Souza, R. Periapical inflammatory responses and their modulation. Crit. Rev. Oral Biol. Med. 1998, 9, 498–521. [Google Scholar] [CrossRef] [PubMed]
- Legorreta-Villegas, I.; Trejo-Remigio, D.A.; Ramírez-Martínez, C.M.; Portilla-Robertson, J.; Leyva-Huerta, E.R.; Jacinto-Alemán, L.F. Análisis de microdensidad vascular y factores de crecimiento en carcinoma oral de células escamosas. Rev. ADM 2020, 77, 287–294. [Google Scholar]
- Roi, C.; Gaje, P.N.; Ceaușu, R.A.; Roi, A.; Rusu, L.C.; Boia, E.R.; Boia, S.; Luca, R.E.; Riviș, M. Heterogeneity of Blood Vessels and Assessment of Microvessel Density-MVD in Gingivitis. J. Clin. Med. 2022, 11, 2758. [Google Scholar] [CrossRef]
- Fonseca-Silva, T.; Santos, C.C.; Alves, L.R.; Dias, L.C.; Brito, M., Jr.; De Paula, A.M.; Guimarães, A.L. Detection and quantification of mast cell, vascular endothelial growth factor, and microvessel density in human inflammatory periapical cysts and granulomas. Int. Endod. J. 2012, 45, 859–864. [Google Scholar] [CrossRef]
- Gaje, P.N.; Ceaușu, A.R.; Jitariu, A.; Stratul, S.I.; Rusu, L.C.; Popovici, R.A.; Raica, M. Mast Cells: Key Players in the Shadow in Oral Inflammation and in Squamous Cell Carcinoma of the Oral Cavity. Biomed. Res. Int. 2016, 2016, 9235080. [Google Scholar] [CrossRef]
- De-Freitas, C.T.; de-França, G.M.; Gordón-Núñez, M.A.; Santos, P.P.; de-Lima, K.C.; Galvão, H.C. Myofibroblasts and increased angiogenesis contribute to periapical cystic injury containment and repair. Med. Oral. Patol. Oral. Cir. Bucal 2020, 25, e584–e591. [Google Scholar] [CrossRef]
- Sheethal, H.S.; Uma, K.; Rao, K.; Priya, N.S.; Umadevi, H.S.; Smitha, T. A quantitative analysis of mast cells in inflammatory periapical and gingival lesions. J. Contemp. Dent. Pract. 2014, 15, 300–305. [Google Scholar] [CrossRef]
- Weidner, N.; Semple, J.P.; Welch, W.R.; Folkman, J. Tumor angiogenesis and metastasis—correlation in invasive breast carcinoma. N. Engl. J. Med. 1991, 324, 1–8. [Google Scholar] [CrossRef]
- Juerchott, A.; Pfefferle, T.; Flechtenmacher, C.; Mente, J.; Bendszus, M.; Heiland, S.; Hilgenfeld, T. Differentiation of periapical granulomas and cysts by using dental MRI: A pilot study. Int. J. Oral. Sci. 2018, 10, 17. [Google Scholar] [CrossRef]
- Seifi, S.; Shafaie, S.; Ghadiri, S. Microvessel density in follicular cysts, keratocystic odontogenic tumours and ameloblastomas. Asian Pac. J. Cancer Prev. 2011, 12, 351–356. [Google Scholar]
- Kademani, D.; Lewis, J.T.; Lamb, D.H.; Rallis, D.J.; Harrington, J.R. Angiogenesis and CD34 expression as a predictor of recurrence in oral squamous cell carcinoma. J. Oral Maxillofac. Surg. 2009, 67, 1800–1805. [Google Scholar] [CrossRef]
- Kerdvongbundit, V.; Vongsavan, N.; Soo-Ampon, S.; Hasegawa, A. Microcirculation and micromorphology of healthy and inflamed gingivae. Odontology 2003, 91, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Aspriello, S.D.; Zizzi, A.; Lucarini, G.; Rubini, C.; Faloia, E.; Boscaro, M.; Tirabassi, G.; Piemontese, M. Vascular endothelial growth factor and microvessel density in periodontitis patients with and without diabetes. J. Periodontol. 2009, 80, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Mathiou, V.; Tsiambas, E.; Maipas, S.; Thymara, I.; Peschos, D.; Lazaris, A.C.; Kavantzas, N. Impact of CD34-dependent Micro Vessel Density on Periapical Odontogenic Cysts. Cancer Diagn. Progn. 2023, 3, 189–193. [Google Scholar] [CrossRef]
- Lanza, F.; Healy, L.; Sutherland, D.R. Structural and functional features of the CD34 antigen: An update. J. Biol. Regul. Homeost. Agents. 2001, 15, 1–13. [Google Scholar] [PubMed]
- Sidney, L.E.; Branch, M.J.; Dunphy, S.E.; Dua, H.S.; Hopkinson, A. Concise review: Evidence for CD34 as a common marker for diverse progenitors. Stem Cells 2014, 32, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- Zachrisson, B.U. Mast cells of the human gingiva. 4. Experimental gingivitis. J. Periodontal Res. 2006, 4, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Mahita, V.N.; Manjunatha, B.S.; Shah, R.; Astekar, M.; Purohit, S.; Kovvuru, S. Quantification and localization of mast cells in periapical lesions. Ann. Med. Health Sci. Res. 2015, 5, 115–118. [Google Scholar] [CrossRef]
- Iamaroon, A.; Pongsiriwet, S.; Jittidecharaks, S.; Pattanaporn, K.; Prapayasatok, S.; Wanachantararak, S. Increase of mast cells and tumor angiogenesis in oral squamous cell carcinoma. J. Oral. Pathol. Med. 2003, 32, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sheethal, H.S.; Kn, H.; Smitha, T.; Chauhan, K. Role of mast cells in inflammatory and reactive pathologies of pulp, periapical area and periodontium. J. Oral Maxillofac. Pathol. 2018, 22, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, A.; Kesarwani, P.; Koppula, S.; Verma, S.; Saumya, S.; Srivastava, P. Quantification and distribution of mast cells in oral periapical inflammatory lesions. J. Conserv. Dent. 2021, 24, 580–584. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Gender | Smoking Status | Daily Cigarette Consumption |
|---|---|---|---|
| Mean (SD): 43.2 (11.9) | F: 17 (45.9%) | Non-smoker: 27 (73.0%) | Mean (SD): 17.7 (3.9) |
| Range: 24.0–72.0 | M: 20 (54.1%) | Smoker: 10 (27.0%) | Range: 10.0–20.0 |
| Extracted Tooth | |
|---|---|
| one | 31 (83.8%) |
| two | 5 (13.5%) |
| three | 1 (2.7%) |
| Extracted Tooth | |
|---|---|
| maxilla | 23 (62.1%) |
| mandible | 14 (37.9%) |
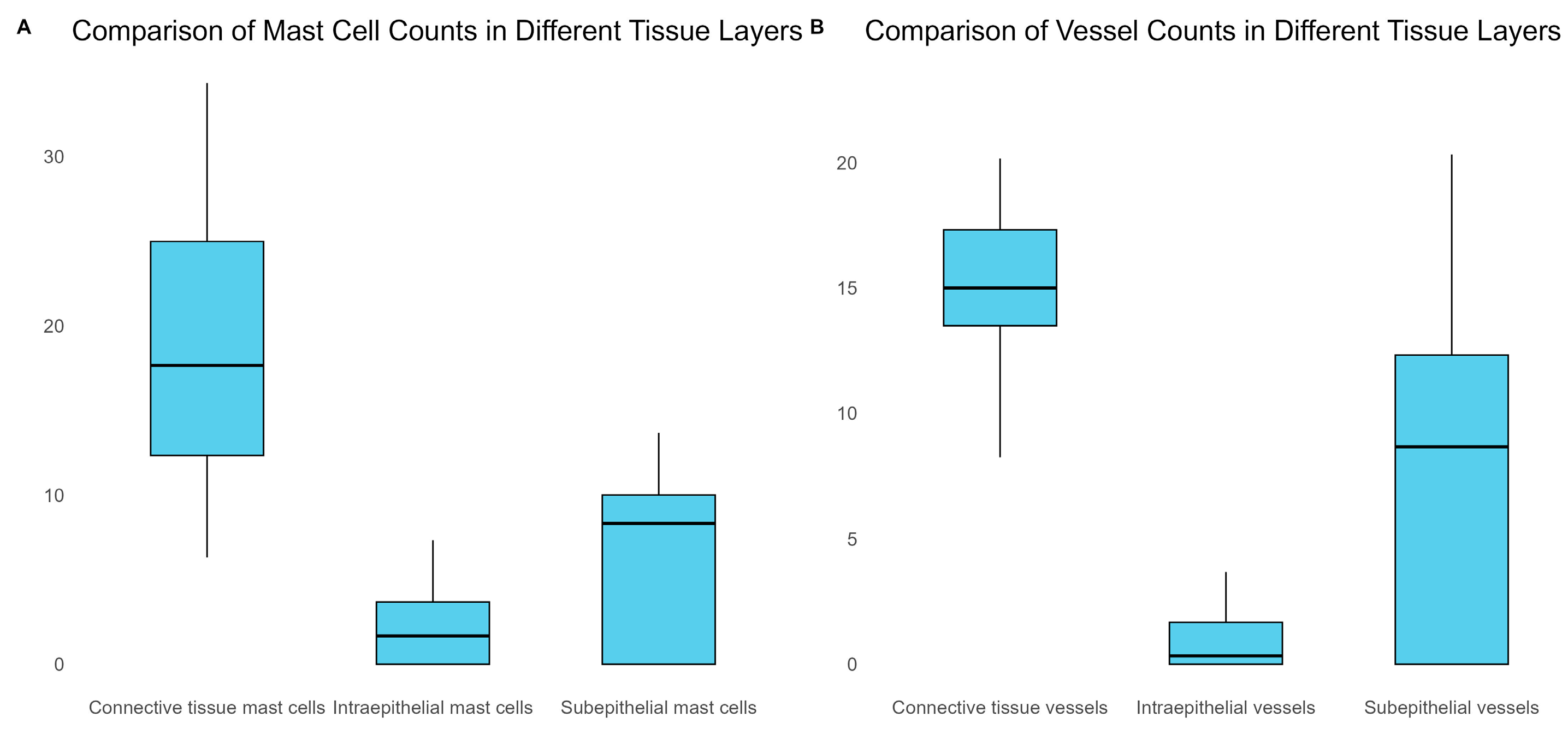
| Intraepithelial Mast Cells | Subepithelial Mast Cells | Connective Tissue Mast Cells |
|---|---|---|
| Mean (SD): 2.1 (1.9) | Mean (SD): 6.5 (4.8) | Mean (SD): 18.7 (7.7) |
| Range: 0.0–7.3 | Range: 0.0–13.7 | Range: 6.3–34.3 |
| Intraepithelial Vessels | Subepithelial Vessels | Connective Tissue Vessels |
|---|---|---|
| Mean (SD): 1.4 (2.2) | Mean (SD): 7.8 (6.5) | Mean (SD): 14.9 (3.9) |
| Range: 0.0–9.7 | Range: 0.0–20.3 | Range: 0.0–23.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roi, C.; Negruțiu, M.L.; Roi, A.; Riviș, M.; Luca, R.E.; Raica, M.; Ceaușu, R.A.; Motofelea, A.C.; Gaje, P.N. Human Periapical Odontogenic Granulomas: Aspects of Microvessel Density (MVD), Heterogeneity of Blood Vessels and Mast Cells Density (MCD). Biomedicines 2023, 11, 2709. https://doi.org/10.3390/biomedicines11102709
Roi C, Negruțiu ML, Roi A, Riviș M, Luca RE, Raica M, Ceaușu RA, Motofelea AC, Gaje PN. Human Periapical Odontogenic Granulomas: Aspects of Microvessel Density (MVD), Heterogeneity of Blood Vessels and Mast Cells Density (MCD). Biomedicines. 2023; 11(10):2709. https://doi.org/10.3390/biomedicines11102709
Chicago/Turabian StyleRoi, Ciprian, Meda Lavinia Negruțiu, Alexandra Roi, Mircea Riviș, Ruxandra Elena Luca, Marius Raica, Raluca Amalia Ceaușu, Alexandru Cătălin Motofelea, and Pușa Nela Gaje. 2023. "Human Periapical Odontogenic Granulomas: Aspects of Microvessel Density (MVD), Heterogeneity of Blood Vessels and Mast Cells Density (MCD)" Biomedicines 11, no. 10: 2709. https://doi.org/10.3390/biomedicines11102709
APA StyleRoi, C., Negruțiu, M. L., Roi, A., Riviș, M., Luca, R. E., Raica, M., Ceaușu, R. A., Motofelea, A. C., & Gaje, P. N. (2023). Human Periapical Odontogenic Granulomas: Aspects of Microvessel Density (MVD), Heterogeneity of Blood Vessels and Mast Cells Density (MCD). Biomedicines, 11(10), 2709. https://doi.org/10.3390/biomedicines11102709