
Systematic Review of RCTs Assessing the Effectiveness of mHealth Interventions to Improve Statin Medication Adherence: Using the Behaviour-Change Technique Taxonomy to Identify the Techniques That Improve Adherence



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Intervention and Comparator
2.3. Outcome
2.4. Study Design
3. Results
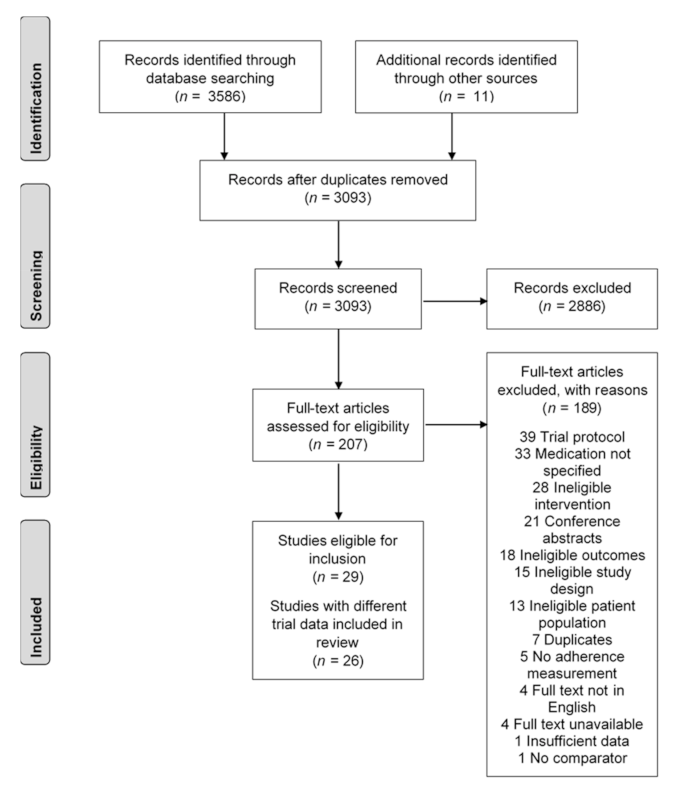
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Inclusion Criteria
3.2.2. Exclusion Criteria
3.3. Effectiveness of Interventions to Improve Statin Adherence
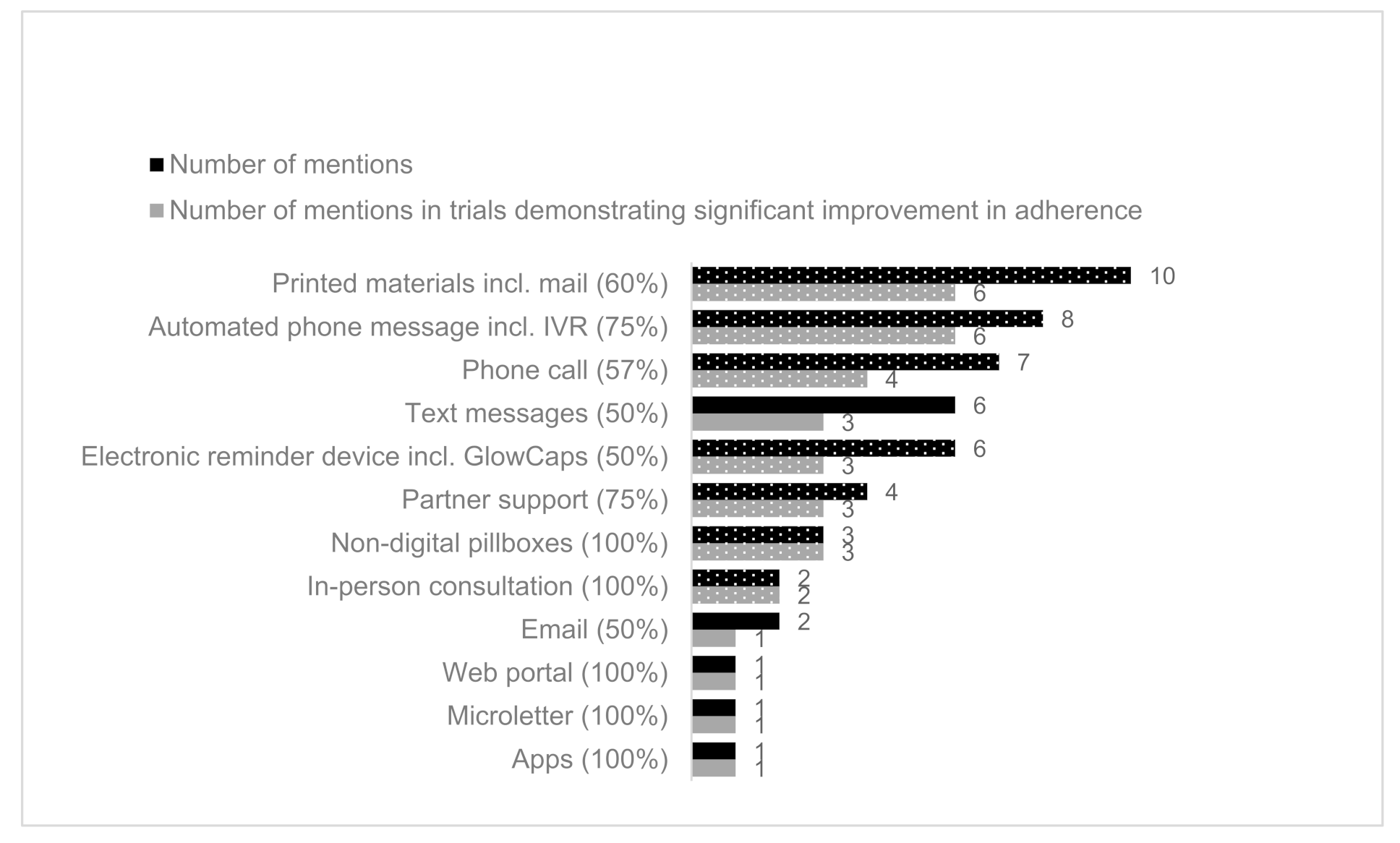
3.4. Intervention Characteristics
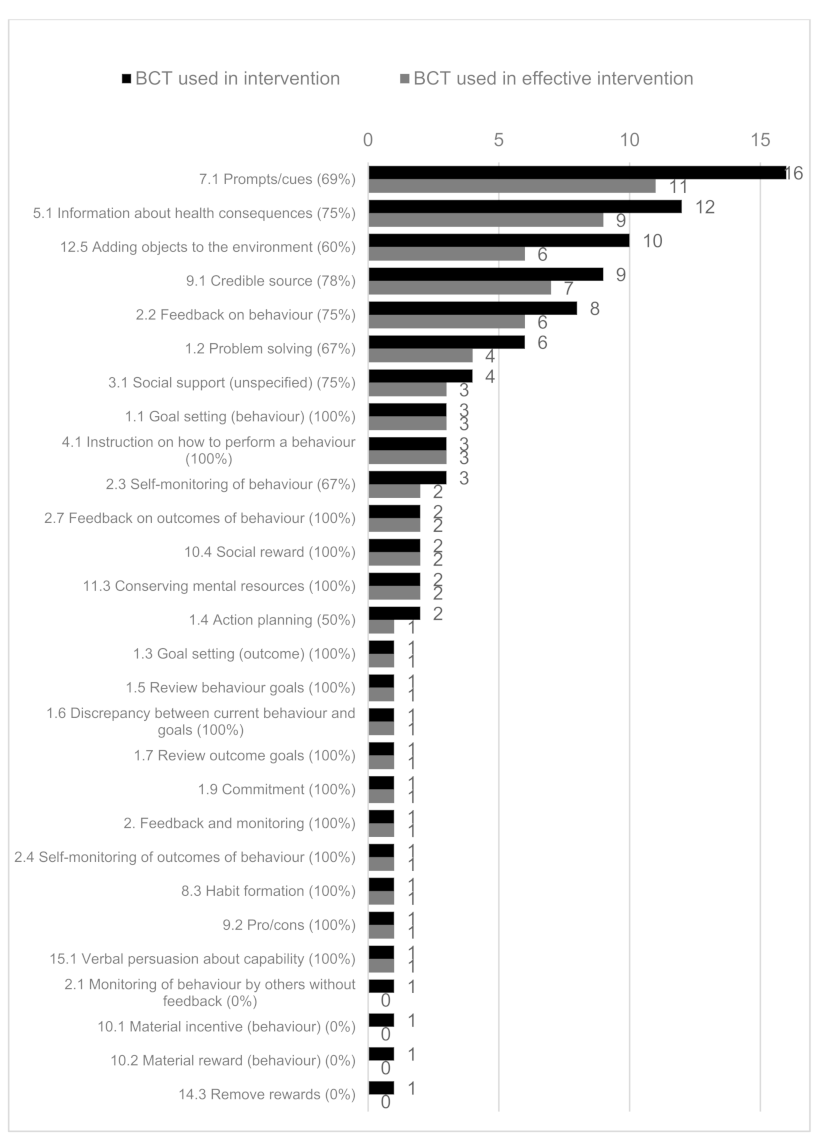
3.5. Behaviour-Change Techniques (BCTs) Used in Included Studies
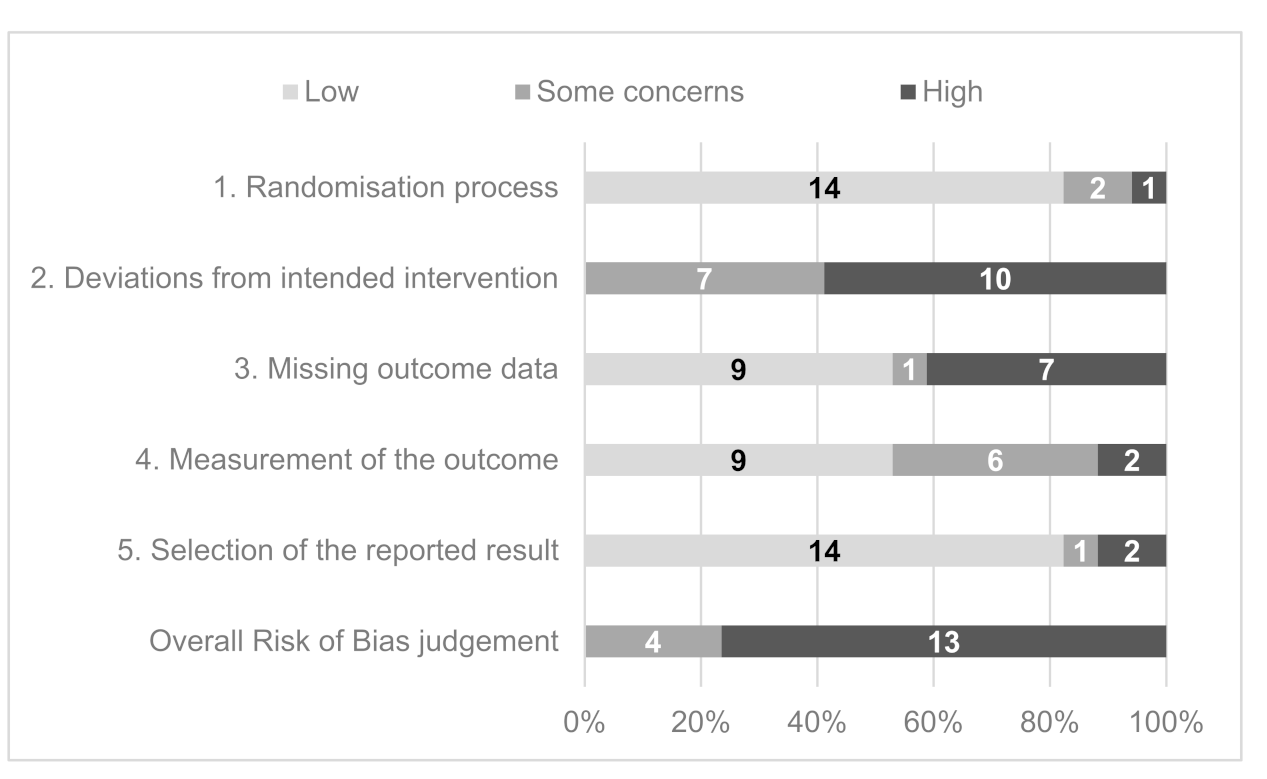
3.6. Study Quality and Risk of Bias
4. Discussion
4.1. Summary of Evidence
4.2. Strengths and Limitations
4.3. Implications for Research and Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Framework Element | # | Search Strategy |
|---|---|---|
| Population Those prescribed statins for the primary or secondary prevention of CVD/dyslipidaemia. | 1 | Statin *.ti,ab,kw. |
| 2 | Atorvastatin *.ti,ab,kw. | |
| 3 | Cerivastatin *.ti,ab,kw. | |
| 4 | Fluvastatin *.ti,ab,kw. | |
| 5 | Fluindostatin *.ti,ab,kw. | |
| 6 | Lovastatin *.ti,ab,kw. | |
| 7 | Mevastatin *.ti,ab,kw. | |
| 8 | Pitavastatin *.ti,ab,kw. | |
| 9 | Pravastatin *.ti,ab,kw. | |
| 10 | Rosuvastatin *.ti,ab,kw. | |
| 11 | Simvastatin *.ti,ab,kw. | |
| 12 | HMG CoA reductase inhibitor *.ti,ab,kw. | |
| 13 | Exp Hydroxymethylglutaryl-CoA Reductase Inhibitors/ | |
| 14 | Hypercholesterol?emia.ti,ab,kw. | |
| 15 | Exp Hypercholesterolemia/ | |
| 16 | Dyslipid?emia.ti,ab,kw. | |
| 17 | Cholesterol *.ti,ab,kw. | |
| 18 | Cardiovascular disease.ti,ab,kw. | |
| 19 | Cardiovascular disease/ | |
| 20 | CVD.ti,ab,kw. | |
| 21 | Heart disease.ti,ab,kw. | |
| 22 | CHD.ti,ab,kw. | |
| 23 | Coronary artery disease.ti,ab,kw. | |
| 24 | CAD.ti,ab,kw. | |
| 25 | Acute coronary syndrome *.ti,ab,kw. | |
| 26 | ACS.ti,ab,kw. | |
| 27 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 | |
| Intervention mHealth | 28 | Mobile health.ti,ab,kw. |
| 29 | mHealth.ti,ab,kw. | |
| 30 | M?health.ti,ab,kw. | |
| 31 | Telehealth *.ti,ab,kw. | |
| 32 | Telemedicine.ti,ab,kw. | |
| 33 | Exp Telemedicine/ | |
| 34 | Telecomm *.ti,ab,kw. | |
| 35 | Telecommunication/ | |
| 36 | Telephone *.ti,ab,kw. | |
| 37 | Phone *.ti,ab,kw. | |
| 38 | Ehealth.ti,ab,kw. | |
| 39 | Electronic health *.ti,ab,kw. | |
| 40 | Digital health *.ti,ab,kw. | |
| 41 | Web?based.ti,ab,kw. | |
| 42 | Internet.ti,ab,kw. | |
| 43 | Online.ti,ab,kw. | |
| 44 | Wireless technolog *.ti,ab,kw. | |
| 45 | Health Information Technology.ti,ab,kw. | |
| 46 | Mobile technolog *.ti,ab,kw. | |
| 47 | Text messag *.ti,ab,kw. | |
| 48 | Texting.ti,ab,kw. | |
| 49 | Text-based.ti,ab,kw. | |
| 50 | SMS.ti,ab,kw. | |
| 51 | Short messag *.ti,ab,kw. | |
| 52 | MMS.ti,ab,kw. | |
| 53 | Multimedia messag *.ti,ab,kw. | |
| 54 | (Mobile adj1 app *).ti,ab,kw. | |
| 55 | Exp Mobile application/ | |
| 56 | Mobile phone *.ti,ab,kw. | |
| 57 | Exp Mobile phone/ | |
| 58 | Cell phone *.ti,ab,kw. | |
| 59 | Cellular phone *.ti,ab,kw. | |
| 60 | Smartphone *.ti,ab,kw. | |
| 61 | Exp Smartphone/ | |
| 62 | iPhone *.ti,ab,kw. | |
| 63 | (Handheld adj1 computer *).ti,ab,kw. | |
| 64 | (Handheld adj1 device *).ti,ab,kw. | |
| 65 | (Tablet adj1 computer *).ti,ab,kw. | |
| 66 | iPad *.ti,ab,kw. | |
| 67 | Smart watch *.ti,ab,kw. | |
| 68 | Smart device *.ti,ab,kw. | |
| 69 | Interactive voice respons *.ti,ab,kw. | |
| 70 | IVR.ti,ab,kw. | |
| 71 | Exp Reminder system/ | |
| 72 | 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55 or 56 or 57 or 58 or 59 or 60 or 61 or 62 or 63 or 64 or 65 or 66 or 67 or 68 or 69 or 70 or 71 | |
| Outcome Medication adherence | 73 | Adheren *.ti,ab,kw. |
| 74 | Nonadheren *.ti,ab,kw. | |
| 75 | Complian *.ti,ab,kw. | |
| 76 | Noncomplian *.ti,ab,kw. | |
| 77 | Persistence.ti,ab,kw. | |
| 78 | Concordance.ti,ab,kw. | |
| 79 | Treatment refusal.ti,ab,kw. | |
| 80 | Drop out.ti,ab,kw. | |
| 81 | Exp Patient compliance/ | |
| 82 | exp Medication compliance/ | |
| 83 | 73 or 74 or 75 or 76 or 77 or 78 or 79 or 80 or 81 or 82 | |
| Study design RCTs | 84 | Randomized controlled trial.pt |
| 85 | Controlled clinical trial.pt | |
| 86 | Randomi?ed.ab | |
| 87 | Placebo.ab | |
| 88 | Drug therapy.fs | |
| 89 | Randomly.ab | |
| 90 | Trial.ab | |
| 91 | Groups.ab | |
| 92 | 85 or 86 or 87 or 88 or 89 or 90 or 91 or 92 | |
| COMBINE TERMS | 93 | 27 and 72 and 83 and 92 |
| 94 | limit 93 to yr = ”2000 − Current” |
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- How Statin Drugs Protect the Heart|Johns Hopkins Medicine. Available online: https://www.hopkinsmedicine.org/health/wellness-and-prevention/how-statin-drugs-protect-the-heart (accessed on 19 November 2020).
- National Institute for Health and Care Excellence. Cardiovascular Disease Prevention Overview—NICE Pathways. 2017. Available online: https://pathways.nice.org.uk/pathways/cardiovascular-disease-prevention (accessed on 13 April 2020).
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 73, e285–e350. [Google Scholar] [CrossRef]
- Sabaté, E. Prevention of Cardiovascular Disease Guidelines for Assessment and Management of Cardiovascular Risk WHO Library Cataloguing-in-Publication Data. World Health Organization, 2007. Available online: www.inis.ie (accessed on 13 April 2020).
- Martin-Ruiz, E.; Olry-de-Labry-Lima, A.; Ocaña-Riola, R.; Epstein, D. Systematic Review of the Effect of Adherence to Statin Treatment on Critical Cardiovascular Events and Mortality in Primary Prevention. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 200–215. [Google Scholar] [CrossRef]
- Taylor, F.; Huffman, M.D.; Macedo, A.F.; Moore, T.H.M.; Burke, M.; Davey Smith, G.; Ward, K.; Ebrahim, S. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Vrecer, M.; Turk, S.; Drinovec, J.; Mrhar, A. Use of statins in primary and secondary prevention of coronary heart disease and ischemic stroke. Meta-analysis of randomized trials. Int. J. Clin. Pharmacol. Ther. 2003, 41, 567–577. [Google Scholar] [CrossRef]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef]
- Brown, M.T.; Bussell, J.K. Medication adherence: WHO cares? Mayo Clin. Proc. 2011, 86, 304–314. [Google Scholar] [CrossRef]
- World Health Organization. Evidence for Action. 2003, pp. 1–198. Available online: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf (accessed on 13 April 2020).
- Perreault, S.; Dragomir, A.; Blais, L.; Bérard, A.; LaLonde, L.; White, M.; Pilon, D. Impact of better adherence to statin agents in the primary prevention of coronary artery disease. Eur. J. Clin. Pharmacol. 2009, 65, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Poluzzi, E.; Strahinja, P.; Lanzoni, M.; Vargiu, A.; Silvani, M.C.; Motola, D.; Gaddi, A.; Vaccheri, A.; Montanaro, N. Adherence to statin therapy and patients’ cardiovascular risk: A pharmacoepidemiological study in Italy. Eur. J. Clin. Pharmacol. 2008, 64, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.M.; Allegrante, J.; Natarajan, S.; Halm, E.A.; Charlson, M. Predictors of Adherence to Statins for Primary Prevention. Cardiovasc. Drugs Ther. 2007, 21, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.P.; Alexander, K.P.; Lytle, B.; Heiss, G.; Peterson, E.D. Long-term adherence with cardiovascular drug regimens. Am. Hear. J. 2006, 151, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Abbass, I.; Revere, L.; Mitchell, J.; Appari, A. Medication Nonadherence: The Role of Cost, Community, and Individual Factors. Health Serv. Res. 2016, 52, 1511–1533. [Google Scholar] [CrossRef]
- Nelson, A.J.; Puri, R.; Nissen, S.E. Statins in a Distorted Mirror of Media. 2020, Volume 22, pp. 1–8. Available online: https://link.springer.com/article/10.1007/s11883-020-00853-9 (accessed on 12 January 2020).
- Ingersgaard, M.V.; Andersen, T.H.; Norgaard, O.; Grabowski, D.; Olesen, K. Reasons for Nonadherence to Statins—A Systematic Review of Reviews. Patient Prefer Adherence 2020, 14, 675–691. [Google Scholar] [CrossRef] [PubMed]
- Vicki, F.; Sinclair, F.; Wang, H.; Dailey, D.; Hsu, J.; Shaber, R. Patients’ Perspectives on Nonadherence to Statin Therapy: A Focus-Group Study. Perm. J. 2010, 14, 4. [Google Scholar]
- Rash, J.A.; Campbell, D.J.; Tonelli, M.; Campbell, T.S. A systematic review of interventions to improve adherence to statin medication: What do we know about what works? Prev. Med. 2016, 90, 155–169. [Google Scholar] [CrossRef]
- Costa, E.; Giardini, A.; Savin, M.; Menditto, E.; Lehane, E.; Laosa, O.; Pecorelli, S.; Monaco, A.; Marengoni, A. Interventional tools to improve medication adherence: Review of literature. Patient Prefer. Adherence 2015, 9, 1303–1314. [Google Scholar] [CrossRef]
- Xiong, S.; Berkhouse, H.; Schooler, M.; Pu, W.; Sun, A.; Gong, E.; Yan, L.L. Effectiveness of mHealth Interventions in Improving Medication Adherence Among People with Hypertension: A Systematic Review. Curr. Hypertens. Rep. 2018, 20, 1–15. [Google Scholar] [CrossRef]
- Gellad, W.F.; Grenard, J.; McGlynn, E.A. A Review of Barriers to Medication Adherence: A Framework for Driving Policy Options; RAND Corporation PP: Santa Monica, CA, USA, 2009; Available online: https://www.rand.org/pubs/technical_reports/TR765.html (accessed on 12 January 2020).
- Ju, A.; Hanson, C.S.; Banks, E.; Korda, R.; Craig, J.C.; Usherwood, T.; Macdonald, P.; Tong, A. Patient beliefs and attitudes to taking statins: Systematic review of qualitative studies. Br. J. Gen. Pr. 2018, 68, e408–e419. [Google Scholar] [CrossRef]
- Brown, M.T.; Bussell, J.; Dutta, S.; Davis, K.; Strong, S.; Mathew, S. Medication Adherence: Truth and Consequences. Am. J. Med. Sci. 2016, 351, 387–399. [Google Scholar] [CrossRef]
- Michie, S.; Johnston, M. Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychol. Rev. 2012, 6, 1–6. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. Available online: https://academic.oup.com/abm/article/46/1/81-95/4563254 (accessed on 16 April 2020). [CrossRef]
- World Health Organization. mHealth New Horizons for Health through Mobile Technologies; WHO: Geneva, Switzerland, 2011; Available online: http://www.who.int/about/ (accessed on 13 April 2020).
- Car, J.; Tan, W.S.; Huang, Z.; Sloot, P.; Franklin, B.D. eHealth in the future of medications management: Personalisation, monitoring and adherence. BMC Med. 2017, 15, 1–9. Available online: https://pubmed.ncbi.nlm.nih.gov/28376771 (accessed on 14 April 2020). [CrossRef] [PubMed]
- Zhao, Y.Y.; Dang, F.P.; Zhai, T.T.; Li, H.J.; Wang, R.J.; Ren, J.J. The effect of text message reminders on medication adherence among patients with coronary heart disease: A systematic review and meta-analysis. Medicine (Baltimore) 2019, 98, e18353. [Google Scholar] [CrossRef]
- Kavradim, S.T.; Özer, Z.; Boz, I. Effectiveness of telehealth interventions as a part of secondary prevention in coronary artery disease: A systematic review and meta-analysis. Scand. J. Caring Sci. 2019, 34, 585–603. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/scs.12785 (accessed on 14 April 2020). [CrossRef] [PubMed]
- Coorey, G.M.; Neubeck, L.; Mulley, J.; Redfern, J. Effectiveness, acceptability and usefulness of mobile applications for cardiovascular disease self-management: Systematic review with meta-synthesis of quantitative and qualitative data. Eur. J. Prev. Cardiol. 2018, 25, 505–521. Available online: http://journals.sagepub.com/doi/10.1177/2047487317750913 (accessed on 14 April 2020). [CrossRef] [PubMed]
- Palmer, M.J.; Barnard, S.; Perel, P.; Free, C. Mobile phone-based interventions for improving adherence to medication prescribed for the primary prevention of cardiovascular disease in adults. Cochrane Database Syst. Rev. 2018, 2018, CD012675. [Google Scholar] [CrossRef]
- Gandhi, S.; Chen, S.; Hong, L.; Sun, K.; Gong, E.; Li, C.; Yan, L.Y.; Schwalm, J.-D. Effect of Mobile Health Interventions on the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Can. J. Cardiol. 2017, 33, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Gandapur, Y.; Kianoush, S.; Kelli, H.M.; Misra, S.; Urrea, B.; Blaha, M.J.; Graham, G.; Marvel, F.A.; Martin, S.S. The role of mHealth for improving medication adherence in patients with cardiovascular disease: A systematic review. Eur. Heart J. Qual. Care Clin. Outcomes 2016, 2, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Dale, L.P.; Dobson, R.; Whittaker, R.; Maddison, R. The effectiveness of mobile-health behaviour change interventions for cardiovascular disease self-management: A systematic review. Eur. J. Prev. Cardiol. 2016, 23, 801–817. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26490093 (accessed on 14 April 2020). [CrossRef]
- Sua, Y.S.; Jiang, Y.; Thompson, D.R.; Wang, W. Effectiveness of mobile phone-based self-management interventions for medication adherence and change in blood pressure in patients with coronary heart disease: A systematic review and meta-analysis. Eur. J. Cardiovasc. Nurs. 2020, 19, 192–200. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31856596 (accessed on 14 April 2020). [CrossRef]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: A Systematic Review. PLoS Med. 2013, 10, e1001362. Available online: https://dx.plos.org/10.1371/journal.pmed.1001362 (accessed on 14 April 2020). [CrossRef]
- van Driel, M.L.; Morledge, M.D.; Ulep, R.; Shaffer, J.P.; Davies, P.; Deichmann, R. Interventions to improve adherence to lipid-lowering medication. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef]
- Morrissey, E.C.; Corbett, T.K.; Walsh, J.C.; Molloy, G.J. Behavior change techniques in apps for medication adherence: A content analysis. Am. J. Prev. Med. 2016, 50, e143–e146. [Google Scholar] [CrossRef]
- Armitage, L.C.; Kassavou, A.; Sutton, S. Do mobile device apps designed to support medication adherence demonstrate efficacy? A systematic review of randomised controlled trials, with meta-analysis. BMJ Open 2020, 10, 32045. Available online: http://bmjopen.bmj.com/content/early/by/section (accessed on 14 April 2020). [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. Available online: https://dx.plos.org/10.1371/journal.pmed.1000097 (accessed on 15 April 2020). [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. Available online: https://dx.plos.org/10.1371/journal.pmed.1000100 (accessed on 15 April 2020).
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.S.J. Chapter 8: Assessing risk of bias in a randomized. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.0; Wiley: Hoboken, NJ, USA, 2019; Available online: www.training.cochrane.org/handbook (accessed on 15 April 2020).
- BCT Taxonomy Starter Pack. Available online: http://www.bct-taxonomy.com/pdf/StarterPack.pdf (accessed on 19 November 2020).
- Choudhry, N.K.; Isaac, T.; Lauffenburger, J.C.; Gopalakrishnan, C.; Lee, M.; Vachon, A.; Iliadis, T.L.; Hollands, W.; Elman, S.; Kraft, J.M.; et al. Effect of a Remotely Delivered Tailored Multicomponent Approach to Enhance Medication Taking for Patients With Hyperlipidemia, Hypertension, and Diabetes: The STIC2IT Cluster Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1182–1189. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med15&NEWS=N&AN=30083727 (accessed on 20 August 2020). [CrossRef] [PubMed]
- Derose, S.; Green, K.; Marrett, E.; Tunceli, K.; Cheetham, T.C.; Chiu, V.Y.; Harrison, T.N.; Reynolds, K.; Vansomphone, S.S.; Scott, R.D. Automated outreach to increase primary adherence to cholesterol-lowering medications. JAMA Intern. Med. 2013, 173, 38–43. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med10&NEWS=N&AN=23403978 (accessed on 20 August 2020). [CrossRef] [PubMed]
- Reddy, A.; Huseman, T.; Canamucio, A.; Marcus, S.C.; Asch, D.A.; Volpp, K.G.; Long, J. Evaluating individual feedback and partner feedback to improve statin medication adherence. J. Gen. Intern. Med. 2016, 31, S213. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01160482/full (accessed on 20 August 2020).
- Salisbury, C.; O’Cathain, A.; Thomas, C.; Edwards, L.; Gaunt, D.; Dixon, P.; Hollinghurst, S.; Nicholl, J.; Large, S.; Yardley, L.; et al. Telehealth for patients at high risk of cardiovascular disease: Pragmatic randomised controlled trial. BMJ 2016, 353, i2647. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medc&NEWS=N&AN=27252245 (accessed on 20 August 2020). [CrossRef] [PubMed]
- Santo, K.; Singleton, A.; Rogers, K.; Thiagalingam, A.; Chalmers, J.; Chow, C.; Redfern, J. Medication reminder apps to improve medication adherence in coronary heart disease patients (MedApp-CHD): A randomised clinical trial. Eur. Heart J. 2018, 39, 226. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01935827/full (accessed on 20 August 2020). [CrossRef][Green Version]
- Stacy, J.N.; Schwartz, S.M.; Ershoff, D.; Shreve, M.S. Incorporating tailored interactive patient solutions using interactive voice response technology to improve statin adherence: Results of a randomized clinical trial in a managed care setting. Popul. Health Manag. 2009, 12, 241–254. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med7&NEWS=N&AN=19848566 (accessed on 20 August 2020). [CrossRef]
- Vollmer, W.M.; Owen-Smith, A.A.; Tom, J.O.; Laws, R.; Ditmer, D.G.; Smith, D.H.; Waterbury, A.C.; Schneider, J.L.; Yonehara, C.Y.; Williams, A.; et al. Improving adherence to cardiovascular disease medications with information technology. Am. J. Manag. Care 2014, 20, SP502–SP510. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed15&NEWS=N&AN=606829929 (accessed on 20 August 2020). [PubMed]
- Volpp, K.G.; Troxel, A.B.; Mehta, S.J.; Norton, L.; Zhu, J.; Lim, R.; Wang, W.; Marcus, N.; Terweisch, C.; Caldarella, K.; et al. Effect of electronic reminders, financial incentives, and social support on outcomes after myocardial infarction the heartstrong randomized clinical trial. JAMA Intern. Med. 2017, 177, 1093–1101. Available online: http://jamanetwork.com/journals/jamainternalmedicine/data/journals/intemed/936414/jamainternal_volpp_2017_oi_170046.pdf (accessed on 20 August 2020). [CrossRef] [PubMed]
- Vrijens, B.; Belmans, A.; Matthys, K.; de Klerk, E.; Lesaffre, E. Effect of intervention through a pharmaceutical care program on patient adherence with prescribed once-daily atorvastatin. Pharmacoepidemiol. Drug Saf. 2006, 15, 115–121. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-00561702/full (accessed on 20 August 2020). [CrossRef]
- Fang, R.; Li, X. Electronic messaging support service programs improve adherence to lipid-lowering therapy among outpatients with coronary artery disease: An exploratory andomized control study. J. Clin. Nurs. 2016, 25, 664–671. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med13&NEWS=N&AN=26522838 (accessed on 20 August 2020). [CrossRef] [PubMed]
- Harrison, T.N.; Green, K.R.; Liu, I.-L.A.; Vansomphone, S.S.; Handler, J.; Scott, R.D.; Cheetham, T.C.; Reynolds, K. Automated Outreach for Cardiovascular-Related Medication Refill Reminders. J. Clin. Hypertens. 2016, 18, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.M.; Lambert-Kerzner, A.; Carey, E.P.; Fahdi, I.E.; Bryson, C.L.; Melnyk, S.D.; Bosworth, H.B.; Radcliff, T.; Davis, R.; Mun, H.; et al. Multifaceted intervention to improve medication adherence and secondary prevention measures after acute coronary syndrome hospital discharge: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 186–193. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-00978324/full (accessed on 20 August 2020). [CrossRef]
- Ivers, N.; Schwalm, J.-D.; Bouck, Z.; McCready, T.; Taljaard, M.; Grace, S.L.; Cunningham, J.; Bosiak, B.; Presseau, J.; Witteman, H.O.; et al. Interventions supporting long term adherence and decreasing cardiovascular events after myocardial infarction (ISLAND): Pragmatic randomised controlled trial. BMJ 2020, 369, m1731. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=medl&NEWS=N&AN=32522811 (accessed on 20 August 2020). [CrossRef]
- Kessler, J.B.; Troxel, A.B.; Asch, D.A.; Mehta, S.J.; Marcus, N.; Lim, R.; Zhu, J.; Shrank, W.; Brennan, T.; Volpp, K.G. Partners and Alerts in Medication Adherence: A Randomized Clinical Trial. J. Gen. Intern. Med. 2018, 33, 1536–1542. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med15&NEWS=N&AN=29546659 (accessed on 20 August 2020). [CrossRef]
- Kooy, M.J.; Van Wijk, B.; Heerdink, E.R.; De Boer, A.; Bouvy, M.L. A community pharmacist-led intervention to improve adherence to lipid-lowering treatment by counseling and an electronic reminder device: Results of a randomized controlled trial in The Netherlands. Int. J. Clin. Pharm. 2013, 35, 879–880. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01006236/full (accessed on 20 August 2020).
- Park, L.G.; Howie-Esquivel, J.; Chung, M. A text messaging intervention improves medication adherence for patients with coronary heart disease: A randomized controlled trial. Circulation 2013, 128, 261–268. Available online: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed14&NEWS=N&AN=71338098 (accessed on 20 August 2020).
- Párraga-Martínez, I.; Rabanales-Sotos, J.; Lago-Deibe, F.; Téllez-Lapeira, J.M.; Escobar-Rabadán, F.; Villena-Ferrer, A.; Blasco-Valle, M.; Ferreras-Amez, J.M.; Morena-Rayo, S.; del Campo-del Campo, J.M.; et al. Effectiveness of a Combined Strategy to Improve Therapeutic Compliance and Degree of Control Among Patients With Hypercholesterolaemia. BMC Cardiovasc Disord. 2015, 15, 8. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-02026850/full (accessed on 20 August 2020). [CrossRef]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR mHealth uHealth 2018, 6, e23. Available online: https://pubmed.ncbi.nlm.nih.gov/29343463 (accessed on 20 August 2020). [CrossRef]
- Kassavou, A.; Sutton, S. Automated telecommunication interventions to promote adherence to cardio-metabolic medications: Meta-analysis of effectiveness and meta-regression of behaviour change techniques. Health Psychol. Rev. 2018, 12, 25–42. [Google Scholar] [CrossRef] [PubMed]




| Author, Setting (shown in bold if sig. Improvement in Adherence) | Population Characteristics (n, Age of Eligible Participants, Average Age, % of Male Participants, Eligibility Criteria) | Trial Arms, Overall Risk of Bias (RoB) Score | Intervention Description, Delivery Method (Bold), Intervention Provider (Italic) | Adherence (SR = Self-Reported) | BCTs used in mHealth Intervention |
| Choudhry et al. 2018 * [46] Boston, USA | n = 4078, age 18–85, 60 y, 55% male Diagnosis of hypertension, hyperlipidaemia, or diabetes and evidence of worsening disease control Non-adherent to statins | 1. Pharmacist intervention 2. Usual care RoB: Some concerns | Telephone calls with clinical pharmacist based on semi structured guide tailored to patient’s activation level and identified adherence barriers Daily or weekly text messages Non-digital pillboxes Mailed progress reports at 6 and 9 months | Mean adherence over 12 months (SD) 42.7% (33.4) intervention 35.9% (33.0) usual care Absolute difference 8.5% (5.4–11.7% CI) unadjusted 7.6% (4.1–11.1% CI) adjusted | 1.1 Goal setting (behaviour) 1.2 Problem solving 1.4 Action planning 5.1 Information about health consequences 7.1 Prompts/cues 9.1 Credible source 10.4 Social reward |
| Deroseet al. 2013 * [47] California, USA | n = 522, age ≥ 24, 56 y, 49% male Evidence of poor or worsening disease control Newly described a statin and have not filled them in 1 to 2 weeks after prescription >1 yr membership in health plan | 1. Automated outreach intervention 2. Usual care RoB: High | Automated phone message to retrieve a personalised message from the healthcare plan staff 1–2 weeks after prescription if missed, if unanswered messages left on machines. Two more call backs attempts if missed. If still unanswered, letters sent 9–11 days after initial outreach. Message states statin prescribed by clinician, importance of drug, and provides number of local health plan pharmacy. | Medication dispensed, 25 days after randomisation (%) 42.3% intervention 26.0% control Relative risk for dispensed medication 1.63 intervention vs control group (1.50–1.76 95% CI, p ≤ 0.001) | 5.1 Information about health consequences. 7.1 Prompts/cues |
| Fang and Li 2015 * [55] Chengdu City, China | n = 280, adults, 54 y, 70% male Coronary artery disease diagnosis treated in General Medicine Department | 1. Text message 2. Text message + Microletter (ML) 3. Usual care (phone) RoB: High | (a) Text message group received medication reminders and educational material. (b) Text message + MicroLetter group received additional educational materials by nurse/doctor including disease-related information; patients can ask questions. (c) Usual care received telephone call to remind of medication schedule and appointments. | SR: Odds ratio of adherence compared to control at 6 months SMS + ML = 0.069 (95% CI, 0.032–0.151) SMS = 0.339 (95% CI, 0.183–0.629) | 4.1 Instruction on how to perform a behaviour 5.1 Information about health consequences. 7.1 Prompts/cues 9.1 Credible source |
| Harrison et al. 2016 * [56] California, USA | n = 41,711, age ≥ 24, 61 y, 53% male Patients in the Kaiser Permanente Cardiovascular Disease registry (composed from diabetes, atherosclerotic CVD, heart failure, and chronic failure registries. Prescription for statin was 2–6 weeks overdue for refill | 1. Automated telephone messaging system 2. Usual care RoB: High | Automated telephone messaging system from healthcare plan—delivered to live person or voicemail system. Instructed member to order a refill of their prescription by calling number or using online system. | Refilled prescription within 2 wks. after intervention 30.3% intervention 24.9% usual care p < 0.0001 Time from intervention to first refill (median days) 29 d intervention 36 d usual care p < 0.0001 Time from first refill to second refill (median days) 118 d intervention 115 d usual care p < 0.0001 | 7.1 Prompts/cues 9.1 Credible source |
| Ho et al. 2014 * [57] Colorado, Washington, North Carolina, Arkansas, USA | n = 253, not provided, 64 y, 98% male Acute Coronary Syndrome (myocardial infarction or unstable angina) as primary reason for hospital admission | 1. Multifaceted intervention 2. Usual care RoB: Some concerns | (a) Medication reconciliation and tailoring. Addressed problems, adverse effects, adherence issues, synchronised prescription refill times after 1 month, answered questions, and emphasised importance of adherence. In person or via telephone call. Provided non-digital pillbox for those without one. (b) Patient education. Provided at discharge in person and in pharmacist interactions via telephone call. One week and 1 month following discharge, further info. (c) Collaborative care. Pharmacist notified primary care clinician and/or cardiologist about adherence intervention. (d) Automated phone messaging Reminder calls made monthly. Refill calls synchronised to 14 days before, 7 days before, on refill due date. | Composite adherence at 12 mo. (PDC > 0.8) 93.2% intervention 71.3% usual care p < 0.001 Average composite PDC (mean, SD) 0.95 (0.12) intervention 0.84 (0.21) usual care p < 0.001 | 5.1 Information about health consequences 7.1 Prompts/cues |
| Ivers et al. 2020 [58] Ontario, Canada | n = 2632, adults, 67 y, 70% male Had coronary angiogram after myocardial infarction with evidence of obstructive artery disease and discharged from cardiac centre after procedure | 1. Mail-outs 2. Mail-outs plus automated phone calls 3. Usual care RoB: High | (a) Mailed booklets encouraged participants in rehabilitation and long-term adherence to cardiac drugs. First two booklets enclosed a letter to take to the doctor (b) Automated phone calls system one to two weeks after each mail-out. If could not be contacted through this system, received telephone call by a trained lay health worker. | SR: Odds ratio vs usual care at 12 mo. Statin adherence in the past 7 days 1.02 (0.78–1.32) Mailouts p = 0.91 0.95 (0.68–1.10) Mail-outs/calls p = 0.73 Persistence with statins 1.00 (0.72–1.40) Mailouts p = 0.99 1.00 (0.75–1.32) Mail-outs/calls p = 0.99 Adherence to statins (PDC < 0.8) 0.89 (0.69–1.16) Mail-outs p = 0.39 1.04 (0.75–1.30) Mail-outs/calls p = 0.78 | 1.2 Problem solving 7.1 Prompts/cues |
| Kessler et al. 2018 † [59] Philadelphia, USA | n = 179, age ≥ 18, 52 y, 65% male CVS Health employees or their dependents with active CVS Caremark prescription coverage Excluding diabetes patients Non-adherent to statins (Medication Possession Ratio <80%) | 1. Partner 2. Alert 3. Alert and Partner 4. Usual care RoB: High | (a) Friend and family acting as medication adherence partner (b) Electronic reminder device (wireless pill bottle) with automated message sent to individual via email, text, or automated phone call (or multiple) (c) Wireless pill bottle with automated message. Individual and partner both received alerts. | Overall 6 mo. average 36.0% Usual care 52.9% Alert (p = 0.002) 43.2% Partner (p = 0.25) 54.5% Alert and Partner (p = 0.003) Daily adherence (Odds ratio vs usual care, unadjusted) 2.75 Alert (p = 0.001) 1.53 Partner (p = 0.23) 2.92 Alert and Partner (p = 0.002) | 2.2 Feedback on behaviour 3.1 Social support (unspecified) 7.1 Prompts/cues 12.5 Adding objects to the environment |
| Kooy et al. 2013 [60] The Netherlands | n = 381, not provided, 73 y, 61% male Non-adherent patients taking statins (refill rate between 50–80%) Started statins >1 year prior to inclusion | 1. Counselling with electronic reminder device (ERD) 2. ERD only 3. Usual care RoB: High | (a) Counselling session by pharmacists via telephone call: received feedback on data, asked if they were aware they were non-adherent and reasons for this, informed about benefits of statin use, received an electronic reminder device, informed they would be invited for follow up after one year. Ten-min counselling session made 14 days after written invitation. (b) ERD beeps until patient switches it off. It beeps every day at same time, patient can adjust the time | No. of adherent subjects at 360 days 83% usual care 90% counselling with ERD 89% ERD only p > 0.05 | 7.1 Prompts/cues 9.1 Credible source 12.5 Adding objects to the environment |
| Park et al. 2013 [61] California, USA | n = 90, age ≥ 21, 58 y, 77% male History of myocardial infarction and/or Percutaneous Coronary Intervention and taking antiplatelet and statin medications | 1. Text message (TM) Reminders and Education 2. TM Education Alone 3. Usual care RoB: High | (a) Received text messages for medication reminders and health education. Patients could select when they receive these reminders and required patients to confirm receipt. (b) Received text messages for health education on cardiovascular risk reduction. All patients received electronic pill bottles as electronic reminder devices | Mean doses taken at 30 days 27.7 TM Reminders/Education 27.1 TM Education Alone 25.0 usual care p = 0.28 Percent doses taken 92.4% TM Reminders/Education 90.1% TM Education Alone 83.3% usual care p = 0.28 SR: MMAS-8 at 30 days 6.43 ± 1.22 TM Rem/Ed 6.73 ± 1.49 TM Ed 6.96 ± 1.44 usual care p = 0.37 | 2.1 Monitoring of behaviour by others without feedback 5.1 Information about health consequences 7.1 Prompts/cues 12.5 Adding objects to the environment |
| Párraga-Mártinez et al. 2017 [62] Castile-La Mancha, Aragon, Galicia, Spain | n = 358, age ≥ 18, 59 y, 44% male Diagnosed with hypercholesterolemia whether receiving prior therapy or not | 1. Multifaceted intervention 2. Usual care RoB: High | Intervention patients received written information on disease and its treatment and self-completed registration cards on adherence. Text messages with summaries of recommendations, reminders of appointments, and in-person consultations. | SR: Adherence at 1 year 78.5% intervention 64.9% usual care p = 0.025 SR: Adherence at 2 years 77.2% intervention 64.1% usual care p = 0.029 | 7.1 Prompts/cues |
| Reddy et al. 2016 † [48] Philadelphia, USA | n = 126, age 30–75, 65 y, 96% male Veteran patients with diagnosis of coronary artery disease with documented poor adherence to statin therapy | 1. Glowcap and partner feedback 2. Glowcap with individual feedback 3. Usual care RoB: Some concerns | (a) Received electronic reminder device GlowCap with alarm activated and weekly adherence feedback printed report to partner. GlowCap bottle changes colour 1 h before time to take medication. If not taken, it flashes and sounds alarm. (b) Received GlowCap with alarm activated and weekly adherence feedback report to individual (c) All patients received GlowCap and educational materials on importance of adherence to statins. GlowCap features not activated in usual care group. | Adherence rate (0–3 months) 0.86 Partner feedback (p = 0.001) 0.89 Individual feedback (p < 0.001) 0.67 Usual care Adherence rate (4–6 months) 0.52 Partner feedback (p = 0.95) 0.60 Individual feedback (p = 0.75) 0.54 Usual care | 1.6 Discrepancy between current behaviour and goal 2.2 Feedback on behaviour 3.1 Social support (unspecified) 7.1 Prompts/cues 10.4 Social reward 12.5 Adding objects to the environment |
| Salisbury et al. 2016 * [49] Bristol, Sheffield, Southampton, UK | n = 641, age 40–74, 68 y, 48% male Patients with >1 modifiable risk factor and QRISK2 score of a cardiovascular event in next 10 years of ≥20% | 1. Cardiovascular disease risk intervention 2. Usual care RoB: High | Multifaceted intervention including regular telephone calls from a lay health worker supported by tailored algorithms and standardised scripts tailored to participants needs/goals. Linked advisors to online resources and applications to support management, which were sent to patients. Provided access to internet portal to monitor behaviour and outcomes. (Two-third of patients experienced some disruption over 2 months caused by provider switch) | SR: MMAS-4 at 12 months 3.8 intervention 3.6 usual care p = 0.005 | 1.1 Goal setting (behaviour) 1.3 Goal setting (outcome) 1.5 Review behaviour goals 1.7 Review outcome goals 2.3 Self-monitoring of behaviour 2.4 Self-monitoring of outcomes of behaviour 5.1 Information about health consequences 9.1 Credible source |
| Santo et al. 2018 * [50] Sydney, Australia | n = 166, age ≥ 18, 58 y, 87% male Patients with Coronary Heart Disease | 1. Basic medication reminder app 2. Advanced medication reminder app 3. Usual care RoB: High | (a) Basic app provided simple daily reminders to prompt participants to take medications. (b) Advanced app provided interactivity including daily reminders, default settings, refill reminders, adherence stats, ability to export info, and alert partners. Apps available on Australian iTunes and Google app stores | SR: Mean MMAS-8 at 3 months 7.11 app user (basic/advanced) 6.63 usual care p = 0.008 SR: Mean MMAS-8 at 3 months 7.19 basic app group 7.02 advanced app group 6.63 usual care p = 0.023 | 2.2 Feedback on behaviour 3.1 Social support (unspecified) 7.1 Prompts/cues |
| Stacy et al. 2009 * [51] USA | n = 578, age ≥ 21, 55 y, 38% male Patients newly prescribed statins and members of large health benefits plan | 1. Experimental group 2. Enhanced care control group RoB: High | (a) Experimental group who received up to 3 separate tailored behavioural support interactions delivered via Automated phone messages including Interactive Voice Recognition (IVR) and printed material (b) Enhanced care control groups received non-tailored behavioural advice from a single IVR call with a generic guide in the mail. Calls referred to respondents to the health place internet site for additional information. | 6-mo. point prevalence persistency 70.4% intervention 60.7% enhanced care p < 0.05 Continuous persistence 52.5% experimental 44.3% enhanced care p < 0.10 MPR ≥ 80% 47.0% experimental 38.9% enhanced care p < 0.10 | 1.1 Goal setting (behaviour)1.2 Problem solving 1.9 Commitment 2. Feedback and monitoring 5.1 Information about health consequences 7.1 Prompts/cues 8.3 Habit formation 9.2 Pros/cons 15.1 Verbal persuasion about capability |
| Vollmer et al. 2014† [52] Northwest, Hawaii and Georgia, USA | n = 16,380, age ≥ 40, 64 y, 54% male Statin users from Kaiser Permanente regions who were nonadherent <90% to treatment | 1. Interactive Voice Recognition (IVR) 2. Enhanced Interactive Voice Recognition (IVR+) 3. Usual care RoB: Some concerns | (a) IVR participants received automated phone calls when refill due/overdue and to educate patients and help them refill prescriptions (separate calls). Both call types offered a transfer to automated pharmacy refill line. Accompanied with mailed printed materials. (b) IVR+ participants also received personalised reminder letter if 60–89 d overdue and a live telephone call from local pharmacy staff if they were ≥90 d overdue as well as EMR-based feedback to their primary care provider. Received personalised health report, non-digital pillbox, and bimonthly mailings. | Statin adherence at 12 months 0.57 IVR 0.58 IVR+ 0.55 Usual care p-value for IVR/IVR+ vs UC < 0.000 Statin users with ≥80% adherence 35.9% IVR 35.8% IVR+ 32.9% Usual care p-value for IVR/IVR+ vs UC < 0.002 This relationship is not stat significant in those with adherence <0.4 at start of trial | 5.1 Information about health consequences 7.1 Prompts/cues 9.1 Credible source |
| Volpp et al. 2017 [53] Pennsylvania, USA | n = 1509, age 18–80, 61 y, 66% male Patients with Acute Myocardial Infarction immediately post-hospitalisation and currently prescribed >2 secondary prevention medications | 1. Multifaceted intervention 2. Usual care RoB: High | Intervention included provision of up to 4 electronic reminder devices (Vitality GlowCaps or MedSignal device). Assignment of an engagement advisor who would attempt to contact patients via telephone call or mail letter they had not opened device in 6 days. Enlisting a family member or friend as a support partner. Engagement incentives that will use lotteries dependent on adherence. Self-service/customisation of Way to Health platform communication methods including text message, automated phone message, email. | PDC (strict definition) at 12 months 0.72 intervention 0.69 usual care p = 0.23 PDC (intermediate def.) at 12 months 0.80 intervention 0.78 usual care p = 0.26 PDC (relaxed def.) at 12 months 0.83 intervention 0.81 usual care p = 0.27 | 1.2 Problem solving 2.2 Feedback on behaviour 3.1 Social support (unspecified) 7.1 Prompts/cues 10.1 Material incentive (behaviour) 10.2 Material reward (behaviour) 12.5 Adding objects to the environment14.3 Remove rewards |
| Vrijens et al. 2006 * [54] Flanders, Wallonia, Belgium | n = 429, age ≥ 18, 62 y, 52% male Patients who have been taking atorvastatin for at least three months | 1. Pharmaceutical care program 2. Usual care RoB: High | In-person consultation with the patient’s pharmacist reviewing the electronically compiled dosing history and discussing educational message and provided printed materials. An electronic reminder device beep-card that reminds patient of dosing time. | Adherence after 90 days 96.43% intervention 94.33% usual care p = 0.003 Adherence after 300 days 95.89% intervention 89.37% usual care p < 0.001 | 2.2 Feedback on behaviour 2.3 Self-monitoring of behaviour 7.1 Prompts/cues 9.1 Credible source 12.5 Adding objects to the environment |
| Adherence Measurement | Usual Care | Intervention | SD | Effect Size | Relative Improvement | ||
|---|---|---|---|---|---|---|---|
| Choudhry * | Mean PDC over 12 months | 36% | 46% | 36% | 0.28 | 28% | |
| Derose * | % participants who had medication dispensed | 26% | 42% | 63% | |||
| Fang and Li * | MMAS-4 | SMS/ML | −2.674 | −6.71 | 0.40 | ||
| SMS | −1.082 | −3.43 | 0.32 | ||||
| Harrison * | % participants who had filled prescription | 25% | 30% | 22% | |||
| Ho * | PDC > 80% | 71% | 93% | 31% | |||
| Mean PDC | 84% | 95% | 21% | 0.52 | 13% | ||
| Kessler † | Mean % pill bottle openings in 6 months | Partner + alert | 36% | 55% | 25% | 0.75 | 51% |
| Alert | 36% | 53% | 25% | 0.69 | 47% | ||
| Reddy † | % pill bottle openings | Partner feedback | 67% | 89% | 33% | ||
| Individual feedback | 67% | 86% | 28% | ||||
| Salisbury * | MMAS-4 | 3.6 | 3.8 | 0.8 | 0.25 | 6% | |
| Santo * | MMAS-8 | 6.63 | 7.11 | 7% | |||
| Stacy * | PDC > 80% | 61% | 70% | 16% | |||
| Vollmer † | Modified PDC | IVR+ | 55% | 58% | 35% | 0.09 | 5% |
| IVR | 55% | 57% | 35% | 0.06 | 4% | ||
| Vrijens * | % pill bottle openings | 94% | 96% | 2% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bond, Z.; Scanlon, T.; Judah, G. Systematic Review of RCTs Assessing the Effectiveness of mHealth Interventions to Improve Statin Medication Adherence: Using the Behaviour-Change Technique Taxonomy to Identify the Techniques That Improve Adherence. Healthcare 2021, 9, 1282. https://doi.org/10.3390/healthcare9101282
Bond Z, Scanlon T, Judah G. Systematic Review of RCTs Assessing the Effectiveness of mHealth Interventions to Improve Statin Medication Adherence: Using the Behaviour-Change Technique Taxonomy to Identify the Techniques That Improve Adherence. Healthcare. 2021; 9(10):1282. https://doi.org/10.3390/healthcare9101282
Chicago/Turabian StyleBond, Zoe, Tanya Scanlon, and Gaby Judah. 2021. "Systematic Review of RCTs Assessing the Effectiveness of mHealth Interventions to Improve Statin Medication Adherence: Using the Behaviour-Change Technique Taxonomy to Identify the Techniques That Improve Adherence" Healthcare 9, no. 10: 1282. https://doi.org/10.3390/healthcare9101282
APA StyleBond, Z., Scanlon, T., & Judah, G. (2021). Systematic Review of RCTs Assessing the Effectiveness of mHealth Interventions to Improve Statin Medication Adherence: Using the Behaviour-Change Technique Taxonomy to Identify the Techniques That Improve Adherence. Healthcare, 9(10), 1282. https://doi.org/10.3390/healthcare9101282