Cost Analysis of Selected Radiotherapeutic Modalities for Prostate Cancer Treatment—Czech Republic Case Study for the Purposes of Hospital Based HTA

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Input Data
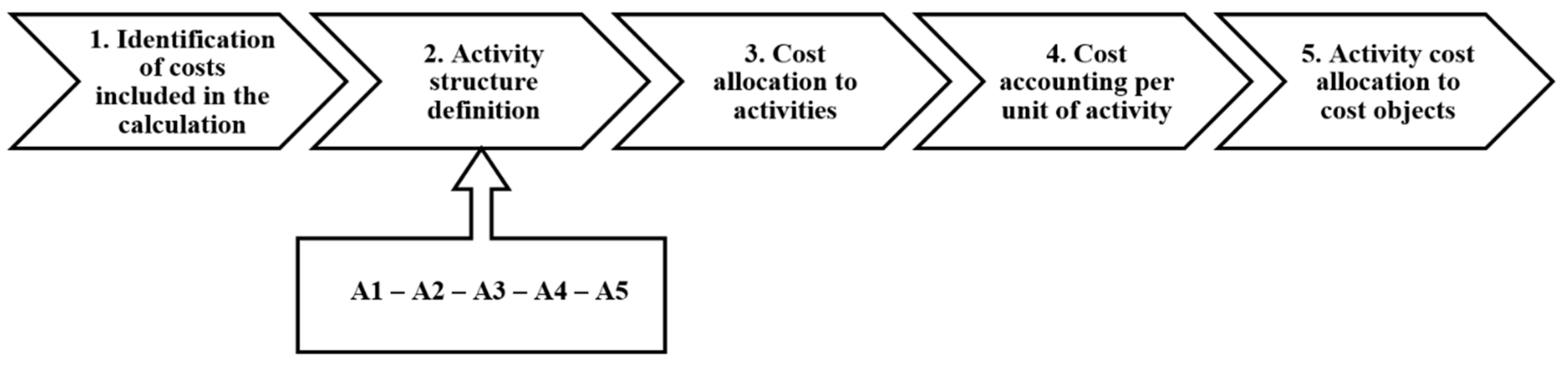
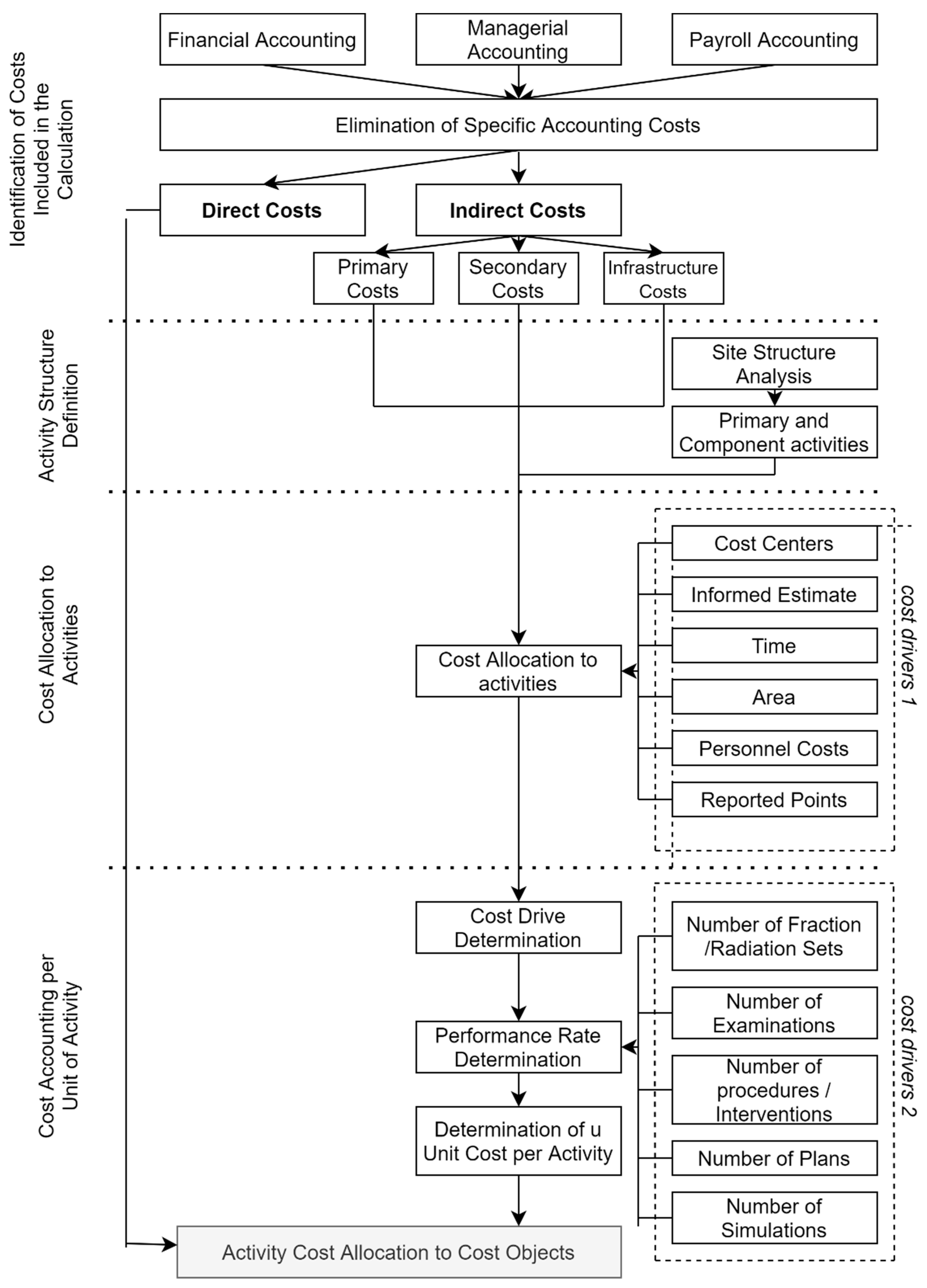
2.2. Description of ABC and Its Application in Radiotherapy
3. Results
3.1. Identification of Costs Included in the Calculation
3.2. Activity Structure Definition
3.3. Cost Allocation to Activities
3.4. Activity Structure Definition
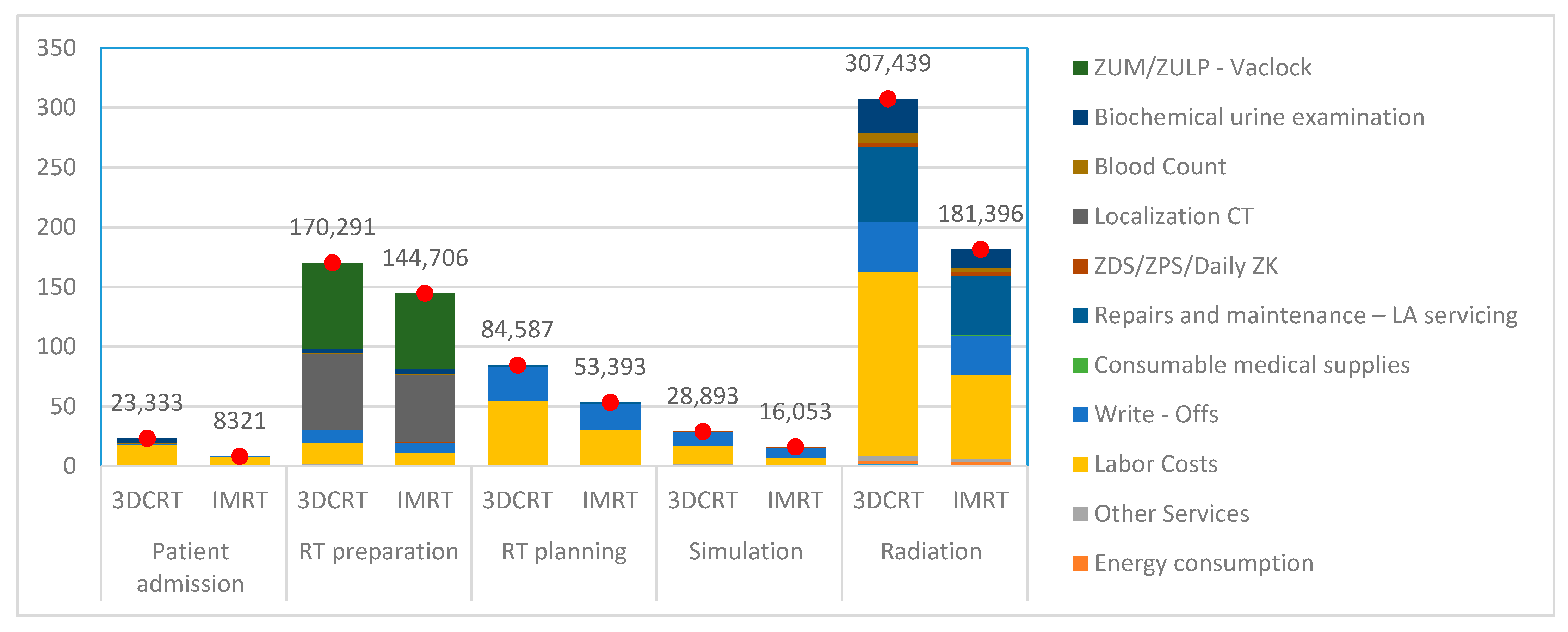
3.5. Activity Cost Allocation to Cost Objects
3.6. Cost Balance and Insurance Reimbursements
3.7. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gagnon, M.-P. Hospital-Based Health Technology Assessment: Developments to Date. Pharmacoeconomics 2014, 32, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, M.-P.; Desmartis, M.; Poder, T.; Witteman, W. Effects and repercussions of local/hospital-based health technology assessment (HTA). Syst. Rev. 2014, 3, 129. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.S.; Porter, M.E. Time-Driven Activity-Based Costing: A Simpler and More Powerful Path to Higher Profits; Harvard Business Press: Brighton, MA, USA, 2007. [Google Scholar]
- Ritrovato, M.; Andellini, M.; di Mauro, R. Hospital based health technology assessment. In Clinical Engineering Handbook; Elsevier: Amsterdam, The Netherlands, 2020; pp. 812–817. [Google Scholar]
- Udba, S. Activity-based costing for hospitals. Health Care Manag. Rev. 1996, 21, 83. [Google Scholar] [CrossRef]
- Baker, J. Activity-Based Costing and Activity-Based Management for Health Care; Jones & Bartlett Learning: Burlington, MA, USA, 1998. [Google Scholar]
- Mwachofi, A.; Al-Assaf, A.F. Health care market deviations from the ideal market. Sultan Qaboos Univ. Med. J. 2011, 11, 328–337. [Google Scholar] [PubMed]
- Popesko, B.; Novák, P.; Papadaki, Š. Measuring diagnosis and patient profitability in healthcare: Economics vs. ethics. Econ. Sociol. 2015, 8, 234–245. [Google Scholar] [CrossRef]
- Zhang, K.; Bangma, C.H.; Roobol, M.J. Prostatecancer screening in Europe and Asia. Asian J. Urol. 2017, 4, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Szymańska, K.; Hainaut, P. Prostate Cancer: Diagnosis and Treatment. In Encyclopedia of Cancer, 3rd ed.; Boffetta, P., Hainau, P., Eds.; Elsevier: Cambridge, MA, USA, 2019; pp. 292–298. [Google Scholar]
- Wong, M.C.S.; Goggins, W.B.; Wang, H.H.X.; Fung, F.D.H.; Leung, C.; Wong, S.Y.S.; Ng, C.; Sung, J.J.Y. Global Incidence and Mortality for ProstateCancer: Analysis of Temporal Patterns and Trends in 36 Countries. Eur. Urol. 2016, 70, 862–874. [Google Scholar] [CrossRef]
- Jiang, P.; Krockenberger, K.; Vonthein, R.; Tereszczuk, J.; Schreiber, A.; Liebau, S.; Huttenlocher, S.; Imhoff, D.; Balermpas, P.; Keller, C.; et al. Hypo-fractionated SBRT for localized prostate cancer: A German bi-center single treatment group feasibility trial. Radiat. Oncol. 2017, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, Y.; Motegi, A.; Akimoto, T.; Mitsuhashi, N.; Iizuka, J.; Tanabe, K.; Ishii, Y.; Kono, S.; Izumi, S.; Karasawa, K. The 5-year outcomes of moderately hypofractionated radiotherapy (66 Gy in 22 fractions, 3 fractions per week) for localized prostate cancer: A retrospective study. Int. J. Clin. Oncol. 2018, 23, 165–172. [Google Scholar] [CrossRef]
- The Institute of Health Information and Statistics of the Czech Republic. TMN Klasifikace Zhoubných Novotvarů, 7th ed.; The Institute of Health Information and Statistics of the Czech Republic: Prague, Czech Republic, 2009. [Google Scholar]
- Gay, H.A.; Michalski, J.M. Radiation Therapy for Prostate Cancer. Mo. Med. 2018, 115, 146–150. [Google Scholar]
- Yong, J.H.E.; Beca, J.; McGowan, T.; Bremner, K.E.; Warde, P.; Hoch, J.S. Cost-effectiveness of Intensity-modulated Radiotherapy in Prostate Cancer. Clin. Oncol. 2012, 24, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Ústav Zdravotnických Informací a Statistiky ČR. Cancer Incidence in the Czech Republic. Available online: https://www.uzis.cz/sites/default/files/knihovna/novotvary2016.pdf (accessed on 28 November 2020).
- Yong, J.H.; McGowan, T.; Redmond-Misner, R.; Beca, J.; Warde, P.; Gutierrez, E.; Hoch, J.S. Estimating the costs of intensity-modulated and 3-dimensional conformal radiotherapy in Ontario. Curr. Oncol. 2016, 23, 228. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.E.; Martin, A.; Schofield, D.; Duchesne, G.; Haworth, A.; Hornby, C.; Sidhom, M.; Jackson, M. A decision model to estimate the cost-effectiveness of intensity modulated radiation therapy (IMRT) compared to three dimensional conformal radiation therapy (3DCRT) in patients receiving radiotherapy to the prostate bed. Radiother. Oncol. 2014, 112, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Konski, A. Cost–effectiveness of intensity-modulated radiation therapy. Expert Rev. Pharmacoecon. Outcomes Res. 2005, 5, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Zemplényi, A.T.; Kalo, Z.; Kovacs, G.; Farkas, R.; Beothe, T.; Banyai, D.; Sebestyen, Z.; Endrei, D.; Boncz, I.; Mangel, L. Cost-effectiveness analysis of intensity-modulated radiation therapy with normal and hypofractionated schemes for the treatment of localised prostate cancer. Eur. J. Cancer Care 2018, 27, e12430. [Google Scholar] [CrossRef]
- Rudat, V.; Nour, A.; Hammoud, M.; Alaradi, A.; Mohammed, A. Image-guided intensity-modulated radiotherapy of prostate cancer. Strahlenther. Onkol. 2016, 192, 109–117. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ślosarek, K. Integral dose: Comparison between four techniques for prostate radiotherapy. Rep. Pract. Oncol. Radiother. 2015, 20, 99–103. [Google Scholar] [CrossRef]
- Sutani, S.; Ohashi, T.; Sakayori, M.; Kaneda, T.; Yamashita, S.; Momma, T.; Hanada, T.; Shiraishi, Y.; Fukada, J.; Oya, M.; et al. Comparison of genitourinary and gastrointestinal toxicity among four radiotherapy modalities for prostate cancer: Conventional radiotherapy, intensity-modulated radiotherapy, and permanent iodine-125 implantation with or without external beam radiotherapy. Radiother. Oncol. 2015, 117, 270–276. [Google Scholar]
- Bauman, G.; Rumble, R.B.; Chen, J.; Loblaw, A.; Warde, P. Intensity-modulated Radiotherapy in the Treatment of Prostate Cancer. Clin. Oncol. 2012, 24, 461–473. [Google Scholar] [CrossRef]
- Schroeck, F.R.; Jacobs, B.L.; Bhayani, S.B.; Nguyen, P.L.; Penson, D.; Hu, J. Cost of New Technologies in Prostate Cancer Treatment: Systematic Review of Costs and Cost Effectiveness of Robotic-assisted Laparoscopic Prostatectomy, Intensity-modulated Radiotherapy, and Proton Beam Therapy. Eur. Urol. 2017, 72, 712–735. [Google Scholar] [CrossRef]
- Popesko, B. Specifics of the Activity-Based Costing applications in Hospital Management. Int. J. Collab. Res. Intern. Med. Public Health 2013, 5, 173. [Google Scholar]
- Drury, C. Management and Cost Accounting, 3rd ed.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Lievens, Y.; van den Bogaert, W.; Kesteloot, K. Activity-based costing: A practical model for cost calculation in radiotherapy. Int. J. Radiat. Oncol. 2003, 57, 522–535. [Google Scholar] [CrossRef]
- Van de Werf, E.; Verstraete, J.; Lievens, Y. The cost of radiotherapy in a decade of technology evolution. Radiother. Oncol. 2012, 102, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Hummel, S.R.; Stevenson, M.D.; Simpson, E.L.; Staffurth, J. A Model of the Cost-effectiveness of Intensity-modulated Radiotherapy in Comparison with Three-dimensional Conformal Radiotherapy for the Treatment of Localised Prostate Cancer. Clin. Oncol. 2012, 24, e159–e167. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Ramakrishna, N.R.; Duff, S.B.; Hughes, K.E.; Sadownik, S.; Smith, J.A.; Tewari, A.K. Primary treatments for clinically localised prostate cancer: A comprehensive lifetime cost-utility analysis. BJU Int. 2013, 111, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Popesko, B.; Novák, P.; Tučková, Z. Kalkulace Nákladů ve Zdravotnických Organizacích; Wolters Kluwer: Prague, Czech Republic, 2014. [Google Scholar]
- Bauer-Nilsen, K.; Hill, C.; Trifiletti, D.M.; Libby, B.; Lash, D.H.; Lain, M.; Christodoulou, D.; Hodge, C.; Showalter, T.N. Evaluation of Delivery Costs for External Beam Radiation Therapy and Brachytherapy for Locally Advanced Cervical Cancer Using Time-Driven Activity-Based Costing. Int. J. Radiat. Oncol. 2018, 100, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Ning, M.S.; Klopp, A.H.; Jhingran, A.; Lin, L.L.; Eifel, P.J.; Vedam, S.; Lawyer, A.A.; Olivieri, N.D.; Guzman, A.B.; Incalcaterra, J.R.; et al. Quantifying institutional resource utilization of adjuvant brachytherapy and intensity-modulated radiation therapy for endometrial cancer via time-driven activity-based costing. Brachytherapy 2019, 18, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Poon, I.; Pintilie, M.; Potvin, M.; McGowan, T. The changing costs of radiation treatment for early prostate cancer in Ontario: A comparison between conventional and conformal external beam radiotherapy. Can. J. Urol. 2004, 11, 2125–2132. [Google Scholar] [PubMed]
- Ploquin, N.P.; Dunscombe, P.B. The cost of radiation therapy. Radiother. Oncol. 2008, 86, 217–223. [Google Scholar] [CrossRef]
- Perrier, L.; Morelle, M.; Pommier, P.; Lagrange, J.L.; Laplanche, A.; Dudouet, P.; Supiot, S.; Chauvet, B.; Nguyen, T.D.; Crehange, G.; et al. Cost of prostate image-guided radiation therapy: Results of a randomized trial. Radiother. Oncol. 2013, 106, 50–58. [Google Scholar] [CrossRef] [PubMed]
- AdHopHTA Project Partners. The AdHopHTA Handbook. Available online: https://www.adhophta.eu/sites/files/adhophta/media/adhophta_handbook_website.pdf (accessed on 25 November 2020).




{kind=link}
{kind=link}
{kind=link}
| Stage | Risk | T (Extent of the Primary Tumor) | PSA | GS | Comments |
|---|---|---|---|---|---|
| 1–3 | Low | T1–T2a | ≤10 ng/mL | ≤7 | in patients with a life expectancy of ≥10 years, radical prostatectomy (RAPE) or curative radiotherapy (EBRT) or brachytherapy (BRT) can be applied separately. 1 |
| Medium | T1–T2a T2b–T2c | 10–20 ≤20 | =7 ≤7 | can be treated separately with RAPE or EBRT, EBRT can be complemented with a short-term neoadjuvant/concomitant LHRH hormone therapy of 4 to 6 months to improve the overall and tumor-specific survival rate. 2 | |
| High | T3a | >20 | 8 and over | RAPE for selected patients only. The recommended treatment is a combination of EBRT and a long-term (2 to 3 years) or short-term (6 months) LHRH hormone therapy. | |
| 4 | Very high | T3b–T4 | n/a | n/a | The appropriate treatment is via hormonal manipulation (orchiectomy or LHRH analogue) in conjunction with external radiotherapy (EBRT) in selected patients (good response to androgen ablation, younger age, solitary or microscopic node metastases). 3 |
| Characteristics | 3D-CRT | IMRT with Rotational VMAT Mondulation |
|---|---|---|
| Total number of patients per department | 1211 | 1407 |
| Number of C61 patients | 312 | 273 |
| Technical equipment | RTG SIM, CT, LU, IGRT | RTG SIM, CT, LU, IGRT |
| Single dose applied | 2 Gy per fraction | 2.5 Gy per fraction |
| Number of radiation fractions | 39 | 28 |
| Fractionation mode | Standard fractionation | HART |
| Total radiotherapeutic dose per patient | 78 Gy | 70 Gy |
| Number of irradiated segments | 7 | 10 |
| Boost | sequential | simultaneous integrated (SIB) |
| Photon radiation energy | 15 MV | 6 MV |
| Staffing | 1 KO, 3 RO, 2 RF, 6 RA, 1 JOP, 1 POP, 1 REF | 1 KO, 3 RO, 2 RF, 6 RA, 1 JOP, 1 POP, 1 REF |
| IGRT | XVI weekly | XVI daily |
| Phase Nr | Phase Description |
|---|---|
| 1 | Total cost classification into direct and indirect costs Adjustment of cost data—bias elimination (contractual fines and sanctions, reinvoicing or adjustments) |
| 2 | Classification of costs into 3 groups: (a) primary—consumed directly by cost objects, (b) secondary—not consumed directly by a specific activity, but representing, for example, complementary diagnostic, hematological or biochemical examinations at a specialized department of the relevant healthcare organization (support activities to facilitate primary activities) (c) infrastructure activities—activities ensuring the operation of the entire department, i.e., maintenance and building administration (e.g., long-term stability tests, operational stability tests, daily instrument/device testing, electrical and gas inspections) |
| 3 | Selection of suitable cost drivers—measurable values (e.g., the number of employees participating in an activity) Work performance time analysis Measuring unit selection (e.g., m2) Direct assignment and determination of qualified estimates Completion of an Activity Cost Matrix (a schematic assigns calculated cost values to individual activities, thereby providing the resulting information concerning their cost structure) |
| 4 | Determination of activity cost drivers (i.e., transaction quantities, time quantities, force quantities, calculation sheets) Determination of an activity performance rate- MVAi (identifying the exact number of cost drivers created by an activity during the relevant reference period) Calculation of activity unit costs—JNA Assignment of support activity costs to primary activities—quantification of the number of secondary activity procedures/interventions required by a primary activity |
| 5 | Preparation of an overview of consumed unit costs of activities on the activity account (the number of specific activity units consumed by a cost object). Cost calculation of individual activities |
| Cost Items | Total Costs per Department | |
|---|---|---|
| 2018 | 2019 | |
| Material consumption | 17,706 | 12,850 |
| Energy consumption | 20,120 | 16,541 |
| Travel expenses | 3427 | 2159 |
| Other services | 22,178 | 13,382 |
| Labor costs | 807,023 | 603,456 |
| Road tax | 16 | 13 |
| Tangible/intangible fixed asset depreciation | 422,962 | 321,227 |
| Repairs and maintenance | 288,701 | 223,063 |
| Total costs | 1,582,132 | 1,192,691 |
| Activity Code | Activity Title | Activity Performed |
|---|---|---|
| A1 | Patient admission | identification, evaluation of the clinical condition of the disease, patient instruction, signature of the IS with the procedure, preparation of RT documentation, making an RT appointment for the patient, data entry in Medicalc and medical documentation |
| A2 | RT preparation | patient identification, acquiring the patient’s photograph, procedural instructions, preparation of fixatives, X-ray of the pelvis, zero point determination, location mark placement, RT report preparation, localization and CT acquisition, data export to the Monaco system, RT report printout, surface disinfection, completion of medical documentation |
| A3 | RT planning | identification, 3D reconstruction, target volume definition, contouring, ROI plotting, dose prescription, isocenter determination, irradiation plan preparation, optimization, RT plan approval, verification, RT plan export to SIM and LU, dosimetric parameter review, RT plan printout |
| A4 | Simulation | identification, chip ID assignment, procedural instructions, patient fixation and alignment, plotting of auxiliary structures in DDR, SIM settings, X-ray, position deviation correction, calculation of the zero position of the table, location mark placement, RT report printout, review, plan verification, export of values to LU, surface disinfection |
| A5 | Radiation | identification, patient instruction, RT plan upload, patient fixation, zero position alignment, departure setting, XVI acquisition, online position correction, irradiation, entry in the RT report, inspection, surfaces disinfection, code reporting to health insurance companies |
| Cost Item | Patient Admission | RT Preparation | RT Planning | Simulation | Radiation |
|---|---|---|---|---|---|
| Material consumption | 5% | 30% | 3% | 20% | 42% |
| Consumable med. Supplies 1 | 5% | 20% | 0% | 20% | 55% |
| Energy consumption 2 | 3% | 10% | 7% | 10% | 70% |
| Other services | 4% | 11% | 5% | 10% | 70% |
| Depreciation 3 | 1% | 12% | 31% | 12% | 45% |
| Repairs and maintenance—LA servicing 4 | 0% | 0% | 2% | 0% | 98% |
| ZDS/ZPS/Daily ZK 5 | 0% | 11% | 0% | 11% | 78% |
| Cost Item | Patient Admission | RT Preparation | RT Planning | Simulation | Radiation |
|---|---|---|---|---|---|
| Localization CT | 0% | 100% | 0% | 0% | 0% |
| Blood count | 10% | 10% | 0% | 0% | 80% |
| Biochemical urine examination | 10% | 10% | 0% | 0% | 80% |
| Activity | Position | Number of Employees | Procedure Duration | ||
|---|---|---|---|---|---|
| 3D-CRT | IMRT | 3D-CRT | IMRT | ||
| A1 | Physician—Clinical Oncologist | 1 | 1 | 35 | 35 |
| Ward Nurse | 1 | 1 | 20 | 20 | |
| General Nurse | 1 | 1 | 15 | 15 | |
| Receptionist | 1 | 1 | 7 | 10 | |
| A2 | Physician—Radiation Oncologist | 1 | 1 | 35 | 35 |
| Radiology Assistant | 1 | 1 | 15 | 15 | |
| CT Radiology Assistant | 1 | 2 | 10 | 5 | |
| A3 | Physician—Radiation Oncologist | 1 | 1 | 90 | 80 |
| Radiology Physicist | 1 | 1 | 120 | 80 | |
| Radiology Assistant | 1 | 1 | 390 | 210 | |
| JOP—verification | 1 | - | 10 | - | |
| Review by another RF | 1 | 1 | 20 | 45 | |
| A4 | Physician—Radiation Oncologist | 1 | 1 | 25 | 25 |
| Radiology Assistant | 1 | 1 | 25 | 25 | |
| JOP (Technician)—inspection | 1 | 15 | 15 | ||
| A5 | Physician—Radiation Oncologist | 1 | 1 | 16 | 20 |
| Radiology Assistant | 3 | 3 | 19 | 15 | |
| Orderly (POP) | 1 | 1 | 5 | 5 | |
| Position | A1 | A2 | A3 | A4 | A5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 3DCRT | IMRT | 3DCRT | IMRT | 3DCRT | IMRT | 3DCRT | IMRT | 3DCRT | IMRT | |
| Physician—Clinical Oncologist | 14 | 14 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Physician—Radiation Oncologist | 0 | 0 | 14 | 23 | 37 | 33 | 10 | 10 | 117 | 71 |
| Ward Nurse | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| General Nurse | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Senior RA | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| RA 1 | 0 | 0 | 6 | 8 | 55 | 30 | 4 | 4 | 314 | 180 |
| Radiology Physicist | 0 | 0 | 0 | 0 | 43 | 39 | 0 | 0 | 0 | 0 |
| Technician (JOP) | 0 | 0 | 0 | 0 | 2 | 0 | 2 | 2 | 0 | 0 |
| Receptionist | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Orderly (POP) | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 28 | 28 |
| Cleaner | 3 | 3 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | 2 |
| Total per patient | 27 | 28 | 25 | 36 | 142 | 108 | 21 | 21 | 465 | 285 |
| Total per C61 diagnosis | 8370 | 7644 | 7750 | 9828 | 44,304 | 29,484 | 6552 | 5733 | 145,080 | 77,805 |
| Cost Items | Type of Radiation Technology | A1 | A2 | A3 | A4 | A5 |
|---|---|---|---|---|---|---|
| Material consumption | 3D-CTR | 196 | 1178 | 118 | 785 | 1649 |
| IMRT | 145 | 869 | 87 | 579 | 1217 | |
| Energy consumption | 3D-CTR | 134 | 446 | 312 | 446 | 3123 |
| IMRT | 112 | 373 | 261 | 373 | 2610 | |
| Other services | 3D-CTR | 197 | 541 | 246 | 492 | 3443 |
| IMRT | 121 | 332 | 151 | 302 | 2112 | |
| Labor costs | 3D-CTR | 17,584 | 17,073 | 53,640 | 15,719 | 154,334 |
| IMRT | 7411 | 9609 | 29,505 | 5667 | 70,702 | |
| Write-offs | 3D-CTR | 628 | 10,983 | 28,991 | 10,983 | 42,206 |
| IMRT | 485 | 8480 | 22,384 | 8480 | 32,587 | |
| Consumable medical supplies | 3D-CTR | 5 | 20 | 0 | 20 | 56 |
| IMRT | 48 | 190 | 0 | 190 | 524 | |
| Repairs and maintenance —LA servicing | 3D-CTR | 0 | 0 | 1280 | 0 | 62,739 |
| IMRT | 0 | 0 | 1006 | 0 | 49,280 | |
| ZDS/ZPS/Daily ZK | 3D-CTR | 0 | 448 | 0 | 448 | 3176 |
| IMRT | 0 | 461 | 0 | 461 | 3269 | |
| Localization CT | 3D-CTR | 0 | 63,249 | 0 | 0 | 0 |
| IMRT | 0 | 56,038 | 0 | 0 | 0 | |
| Blood count | 3D-CTR | 1044 | 1044 | 0 | 0 | 8349 |
| IMRT | 0 | 841 | 0 | 0 | 3362 | |
| Biochemical urine examination | 3D-CTR | 3546 | 3546 | 0 | 0 | 28,365 |
| IMRT | 0 | 3933 | 0 | 0 | 15,734 | |
| ZUM/ZULP 1—Vaclock | 3D-CTR | 0 | 71,763 | 0 | 0 | 0 |
| IMRT | 0 | 63,581 | 0 | 0 | 0 |
| Activity | Cost per Activity (EUR) | Cost Driver | Performance Rate | Unit Costs (EUR) | |||
|---|---|---|---|---|---|---|---|
| 3D-CRT | IMRT | 3D-CRT | IMRT | 3D-CRT | IMRT | ||
| A1 | 23,333 | 8321 | Number of patients | 312 | 273 | 75 | 30 |
| A2 | 170,291 | 144,706 | Number of examinations | 312 | 273 | 546 | 530 |
| A3 | 84,587 | 53,393 | Number of plans | 624 | 410 | 136 | 130 |
| A4 | 28,893 | 16,053 | Number of simulations | 312 | 273 | 93 | 59 |
| A5 | 307,439 | 181,396 | Number of fractions | 12,168 | 7644 | 25 | 24 |
| Activity | Activity Unit Costs (EUR) | Cost Driver | Performance Rate | Total Costs (EUR) | |||
|---|---|---|---|---|---|---|---|
| 3DCRT | IMRT | 3DCRT | IMRT | 3DCRT | IMRT | ||
| A1 | 75 | 30 | Number of patients | 1 | 1 | 75 | 30 |
| A2 | 546 | 530 | Number of examinations | 1 | 1 | 546 | 530 |
| A3 | 136 | 130 | Number of plans | 2 | 2 | 271 | 195 |
| A4 | 93 | 59 | Number of simulations | 2 | 1 | 185 | 59 |
| A5 | 25 | 24 | Radiation set | 39 | 28 | 985 | 664 |
| Total | 2062 | 1479 | |||||
| Costs | Activity | 3D-CRT | IMRT | Difference |
|---|---|---|---|---|
| Costs per patient | A1 | 75 | 30 | 45 |
| A2 | 546 | 530 | 16 | |
| A3 | 271 | 195 | 76 | |
| A4 | 185 | 59 | 126 | |
| A5 | 985 | 664 | 321 | |
| Total (EUR) | 2062 | 1479 | 583 | |
| Costs per annum | Number of patients | 312 | 273 | 39 |
| Total (EUR) | 643,344 | 403,767 | 239,577 | |
| Insurance reimbursement (EUR) | 2,674,064 | 2,217,837 | 456,227 | |
| Resulting balance (EUR) | 2,030,720 | 1,814,070 | n/a |
| Fraction Duration (min) 3D-CRT | Radiation 1 Patient (EUR) | Radiation 312 Patients (EUR) | 19 Min Difference (EUR) | Fraction Duration (min) IMRT | Radiation 1 Patient (EUR) | Radiation 273 Patients (EUR) | 15 Min Difference (EUR) |
|---|---|---|---|---|---|---|---|
| 15 | 248 | 77,443 | 20,652 | 12 | 144 | 39,409 | 9852 |
| 16 | 265 | 82,606 | 15,489 | 13 | 156 | 42,693 | 6568 |
| 17 | 281 | 87,769 | 10 326 | 14 | 168 | 45,977 | 3284 |
| 18 | 298 | 92,932 | 5163 | 15 | 180 | 49,261 | - |
| 19 | 314 | 98,095 | - | 16 | 192 | 52,545 | 3284 |
| 20 | 331 | 103,257 | 5163 | 17 | 205 | 55,829 | 6568 |
| 21 | 348 | 108,420 | 10,326 | 18 | 217 | 59,113 | 9852 |
| 22 | 364 | 113,583 | 15,489 | 19 | 229 | 62,397 | 13,136 |
| 23 | 381 | 118,746 | 20,651 | 20 | 241 | 65,681 | 16,420 |
| 24 | 397 | 123,909 | 25,814 | 21 | 253 | 68,965 | 19,704 |
| Own Resources Ratio for Asset Financing | Costs per 1 Patient (EUR) | Costs per 312 Patients (EUR) |
|---|---|---|
| 15% | 2062 | 643,344 |
| 30% | 2398 | 748,176 |
| 45% | 2734 | 853,008 |
| 60% | 3070 | 957,840 |
| 75% | 3406 | 1,062,672 |
| 100% | 3965 | 1,237,080 |
| Own Resources Ratio for Asset Financing | Costs per 1 Patient (EUR) | Costs per 273 Patients (EUR) |
|---|---|---|
| 15% | 1479 | 403,804 |
| 30% | 1744 | 476,192 |
| 45% | 2009 | 548,580 |
| 60% | 2275 | 620,968 |
| 75% | 2540 | 693,356 |
| 100% | 2982 | 814,003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hospodková, P.; Husár, T.; Klíčová, B.; Severová, L.; Šrédl, K.; Svoboda, R. Cost Analysis of Selected Radiotherapeutic Modalities for Prostate Cancer Treatment—Czech Republic Case Study for the Purposes of Hospital Based HTA. Healthcare 2021, 9, 98. https://doi.org/10.3390/healthcare9010098
Hospodková P, Husár T, Klíčová B, Severová L, Šrédl K, Svoboda R. Cost Analysis of Selected Radiotherapeutic Modalities for Prostate Cancer Treatment—Czech Republic Case Study for the Purposes of Hospital Based HTA. Healthcare. 2021; 9(1):98. https://doi.org/10.3390/healthcare9010098
Chicago/Turabian StyleHospodková, Petra, Tomáš Husár, Barbora Klíčová, Lucie Severová, Karel Šrédl, and Roman Svoboda. 2021. "Cost Analysis of Selected Radiotherapeutic Modalities for Prostate Cancer Treatment—Czech Republic Case Study for the Purposes of Hospital Based HTA" Healthcare 9, no. 1: 98. https://doi.org/10.3390/healthcare9010098
APA StyleHospodková, P., Husár, T., Klíčová, B., Severová, L., Šrédl, K., & Svoboda, R. (2021). Cost Analysis of Selected Radiotherapeutic Modalities for Prostate Cancer Treatment—Czech Republic Case Study for the Purposes of Hospital Based HTA. Healthcare, 9(1), 98. https://doi.org/10.3390/healthcare9010098