COPD: The Annual Cost-Of-Illness during the Last Two Decades in Italy, and Its Mortality Predictivity Power


Abstract
:1. Background
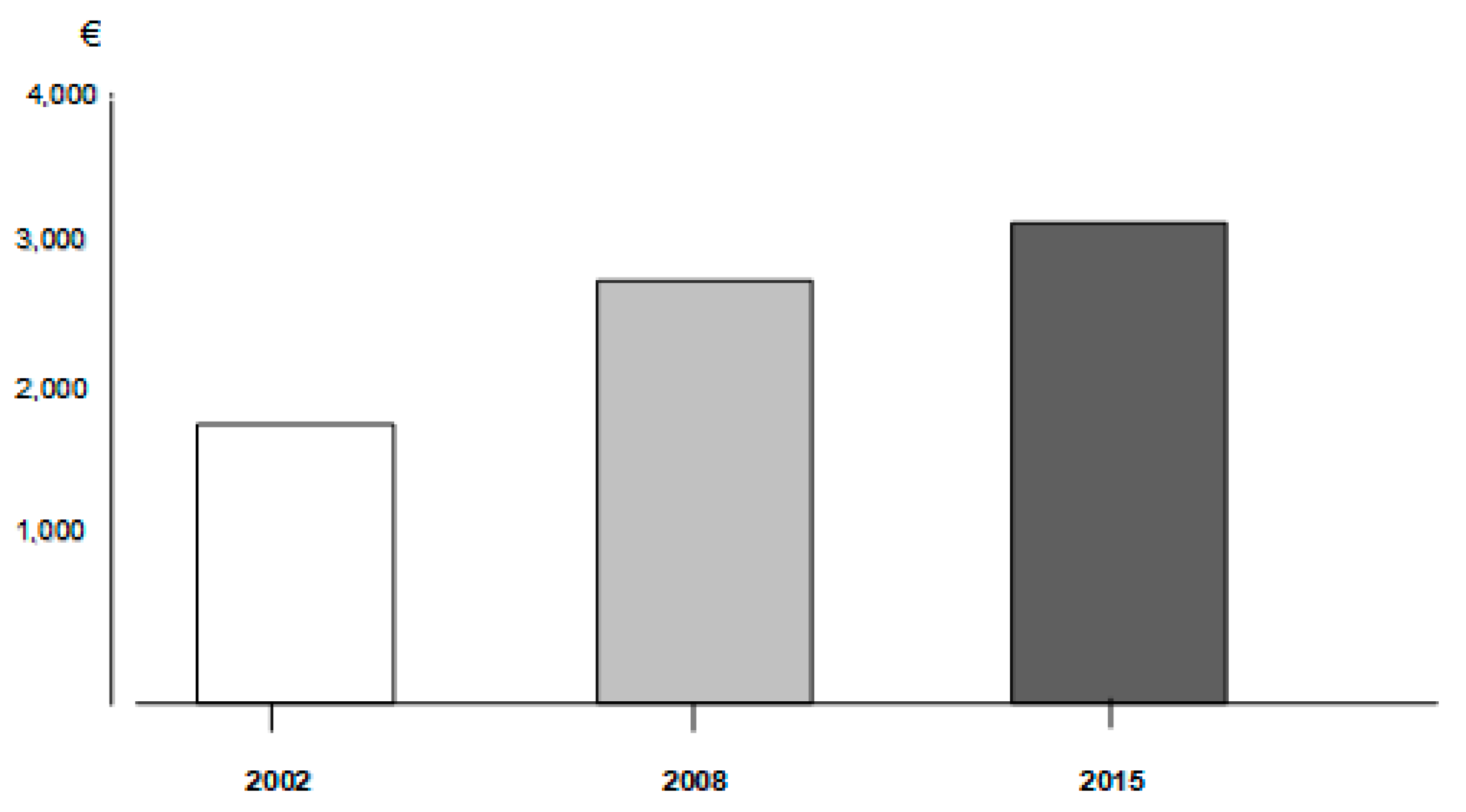
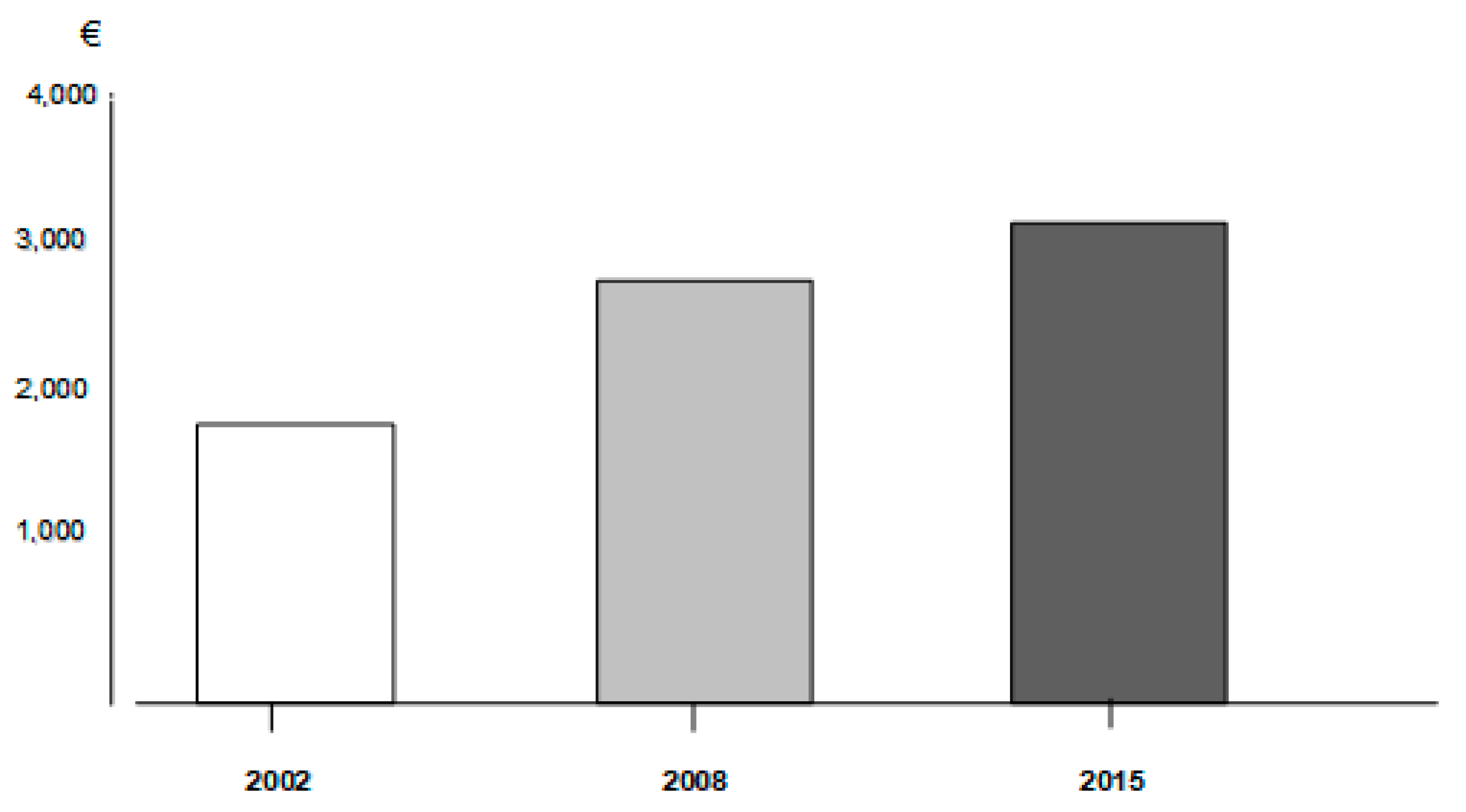
2. Cost Trends in Real Life
3. Conclusions
Funding
Conflicts of Interest
References
- Mannino, D.M.; Higuchi, K.; Yu, T.C.; Zhou, H.; Li, Y.; Tian, H.; Suh, K. Economic burden of chronic obstructive pulmonary disease by presence of comorbidities. Chest 2015, 147, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Available online: http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management-2018.html (accessed on 11 November 2018).
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, T. The state of the art of cost-of-illness estimates. Adv. Econ. Health Serv. Res. 1983, 4, 29–164. [Google Scholar]
- Rice, D.P.; Hodgson, T.A.; Kopstein, A.N. The economic costs of illness: A replication and update. Health Care Financ. Rev. 1985, 7, 61–70. [Google Scholar] [PubMed]
- Dal Negro, R.W.; Berto, P.; Tognella, S.; Quareni, L. Global Outcomes in Lung Disease Study Group. Cost-of-illness of lung disease in the TriVeneto Region, Italy: The GOLD Study. Monaldi Arch. Chest Dis. 2002, 57, 3–9. [Google Scholar] [PubMed]
- Dal Negro, R.W.; Tognella, S.; Tosatto, R.; Dionisi, M.; Turco, P.; Donner, C.F. Costs of chronic obstructive pulmonary disease (COPD) in Italy: The SIRIO study (social impact of respiratory integrated outcomes). Respir. Med. 2008, 102, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Dal Negro, R.W.; Bonadiman, L.; Turco, P.; Tognella, S.; Iannazzo, S. Costs of illness analysis in Italian patients with chronic obstructive pulmonary disease (COPD): An update. Clinicoecon. Outcomes Res. 2015, 7, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Traver, G.A.; Cline, M.G.; Burrows, B. Predictors of mortality in chronic obstructive pulmonary disease. A 15-year follow-up study. Am. Rev. respire. Dis. 1979, 119, 895–902. [Google Scholar]
- Briggs, A.; Spencer, M.; Wang, H.; Mannino, D.; Sin, D.D. Development and validation of a prognostic index for health outcomes in chronic obstructive pulmonary disease. Arch. Intern. Med. 2008, 168, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Halpin, D.M.; Peterson, S.; Larsson, T.P.; Calverly, P.M. Identifying COPD patients at increased risk of mortality: Predictive value of clinical study baseline data. Respir. Med. 2008, 102, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Cote, C.G.; Lareau, S.C.; Meek, P.M. Predictors of survival in COPD: More than just FEV1. Respir. Med. 2008, 102 (Suppl. S1), S27–S35. [Google Scholar] [CrossRef]
- Ko, F.W.; Tam, W.; Tung, A.H.; Ngai, J.; Ng, S.S.; Lai, K.; Au, K.F.; Hui, D.S. A longitudinal study of serial BODE indices in predicting mortality and readmissions for COPD. Respir. Med. 2011, 105, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsson, G.; Ulrik, C.S.; Gislason, T.; Lindberg, E.; Brøndum, E.; Bakke, P.; Janson, C. Long-term survival in patients hospitalized for chronic obstructive pulmonary disease: A prospective observational study in the Nordic countries. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 571–576. [Google Scholar]
- Boutou, A.K.; Shrikrishna, D.; Tanner, R.J.; Smith, C.; Kelly, J.L.; Ward, S.P.; Polkey, M.I.; Hopkinson, N.S. Lung function indices for predicting mortality in COPD. Eur. Respir. J. 2013, 42, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Motegi, T.; Jones, R.C.; Ishii, T.; Hattori, K.; Kusunoki, Y.; Furutate, R.; Yamada, K.; Gemma, A.; Kida, K. A comparison of three multidimensional indices of COPD severity as predictors of future exacerbations. Int. J. Chronic Obstr. Pulm. Dis. 2013, 8, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Moberg, M.; Vestbo, J.; Martinez, G.; Williams, J.E.; Ladelund, S.; Lange, P.; Ringbaek, T. Validation of the i-BODE index as a predictor of hospitalization and mortality in patients with COPD partecipating in pulmonary rehabilitation. COPD J. Chronic Obstr. Pulm. Dis. 2014, 11, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Pedone, C.; Scarlata, S.; Forastiere, F.; Bellia, V.; Antonelli Incalzi, R. BODE index or geriatric multidimensional assessment for the prediction of very-long-term mortality in elderly patients with chronic obstructive pulmonary disease? A prospective cohort study. Age Ageing 2014, 43, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Lombolt, F.K.; Laulund, A.S.; Bjarnason, N.H.; Jorgensen, H.L.; Godtfredsen, N.S. Meta-analysis of routine blood tests as predictors of mortality in COPD. Eur. Clin. Respir. J. 2014, 1, 24110. [Google Scholar] [CrossRef] [PubMed]
- Goossens, L.-M.-A.; Leimer, I.; Metzdorf, N.; Becker, K.; Rutten-van Mölken, M.P. Does the 2013 GOLD classification improve the ability to predict lung function decline, exacerbation and mortality: A post-hoc analysis of the 4-year UPLIFT trial. BMC Pulm. Med. 2014, 163. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Z.; Ou, C.Y.; Yu, C.H.; Yang, S.C.; Chang, H.Y.; Hsiue, T.R. Comparison of global initiative for chronic obstructive pulmonary disease 2013 classification and body mass index, airflow obstruction, dyspnea, and exacerbations index in predicting mortality and exacerbations in elderly adults with chronic obstructive pulmonary disease. J. Am. Geriatr. Soc. 2015, 63, 244–250. [Google Scholar] [PubMed]
- Navarro, A.; Costa, R.; Rodriguez-Carballeira, M.; Yun, S.; Lapuerte, A.; Barrera, A.; Acosta, E.; Vinas, C.; Herdia, J.L.; Almagro, P. Prognostic assessment of mortality and hospitalizations of outpatients with advanced chronic obstructive pulmonary disease. Usefulness of the CODEX index. Rev. Clin. Esp. 2015, 215, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Toy, E.L.; Gallagher, K.F.; Stanley, E.L.; Swensen, A.R.; Duh, M.S. The economic impact of exacerbations of chronic obstructive pulmonary disease and exacerbation definition: A review. COPD J. Chronic Obstr. Pulm. Dis. 2010, 7, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Jahnz-Rozyk, K.; Targowski, T.; From, S. Costs of exacerbations of chronic obstructive pulmonary disease in primary and secondary care in 2007—Results of a multicenter Polish study. Pol. Menkur Lekarski 2009, 26, 208–214. [Google Scholar]
- Seemungal, T.A.; Donaldson, G.C.; Bhowmik, A.; Jeffries, D.J.; Wedzicha, J.A. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care. Med. 2000, 161, 1608–1613. [Google Scholar] [CrossRef] [PubMed]
- Soler-Cataluña, J.J.; Martínez-García, M.A.; Román Sánchez, P.; Salcedo, E.; Navarro, M.; Ochando, R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005, 60, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Simoens, S.; Decramer, M. Pharmacoeconomics of the management of acute exacerbations of chronic obstructive pulmonary disease. Expert Opin. Pharmacother. 2007, 8, 633–648. [Google Scholar] [CrossRef] [PubMed]
- Mapel, D.W.; Schum, M.; Lydick, E.; MArton, J.P. A new method for examining the cost savings of reducing COPD exacerbations. Pharmacoeconomics 2010, 28, 733–749. [Google Scholar] [CrossRef] [PubMed]
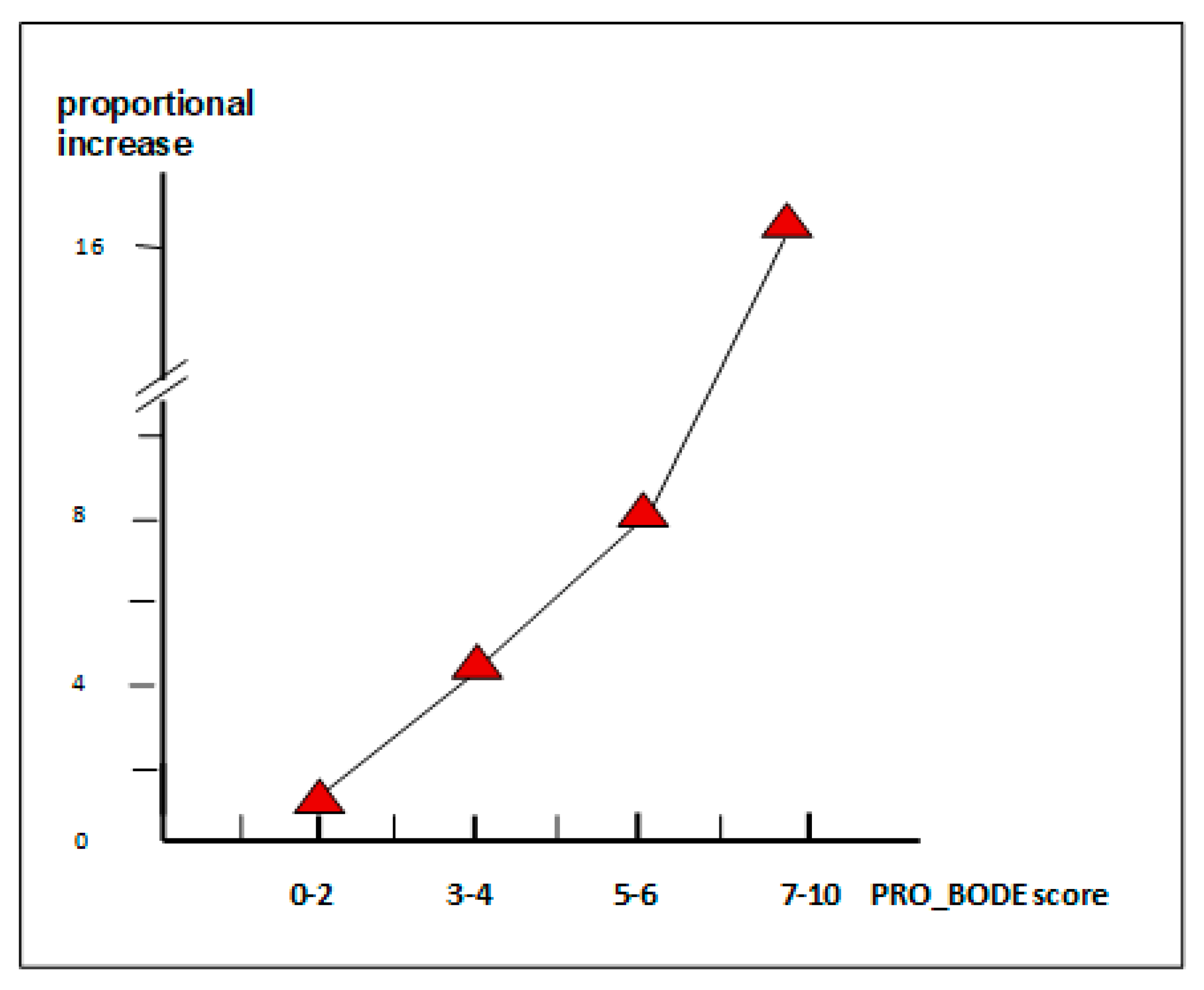
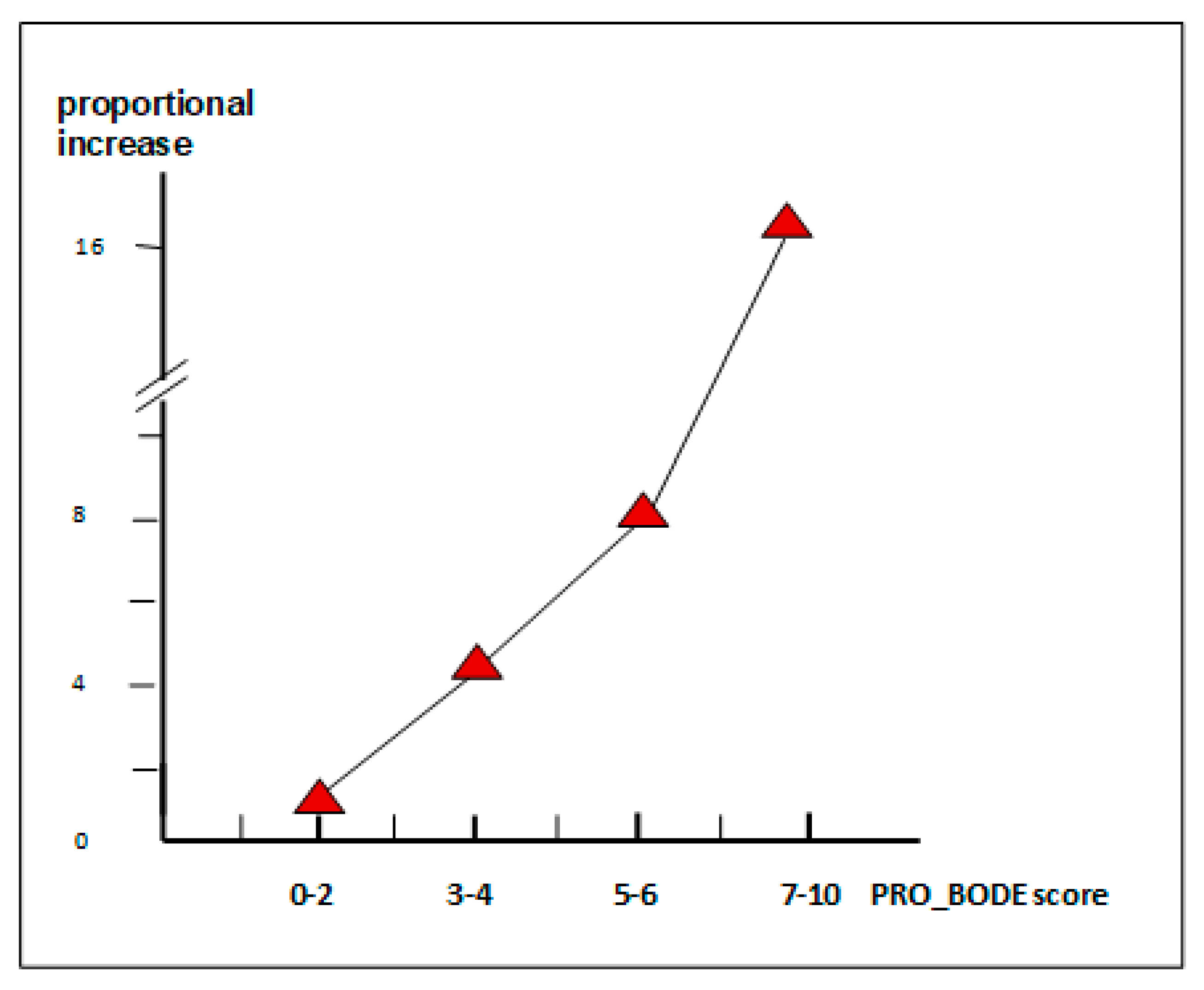
- Dal Negro, R.W.; Celli, B.R. Patient Related Outcomes-BODE (PRO-BODE): A composite index incorporating health utilization resources predicts mortality and economic cost of COPD in real life. Respir. Med. 2017, 131, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Dal Negro, R.W.; Guerriero, M.; Turco, P. COPD and Public Opinion: Results of a Survey in the General Population. J. Pulm. Respir. Med. 2015, 5, 2. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
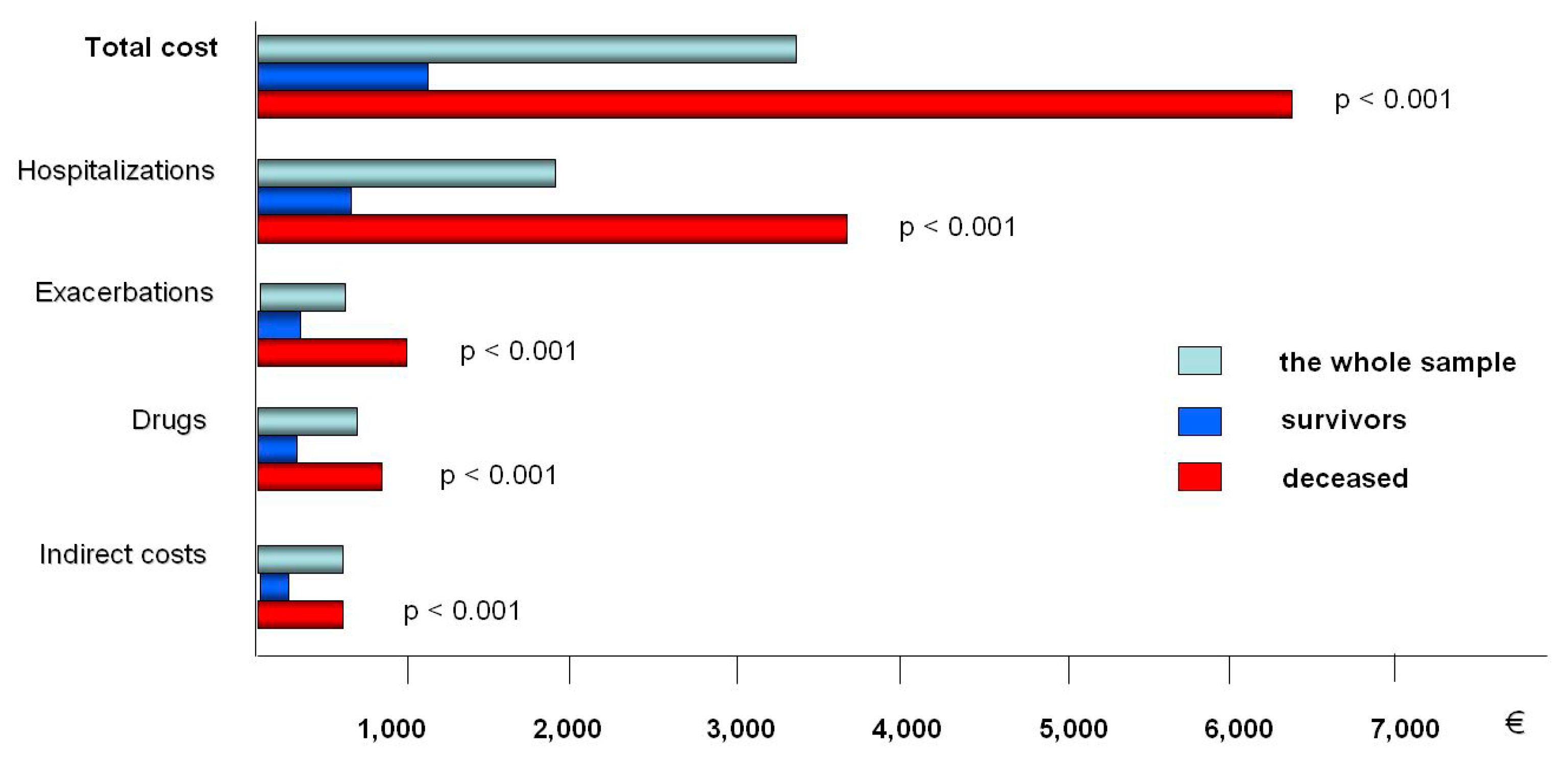
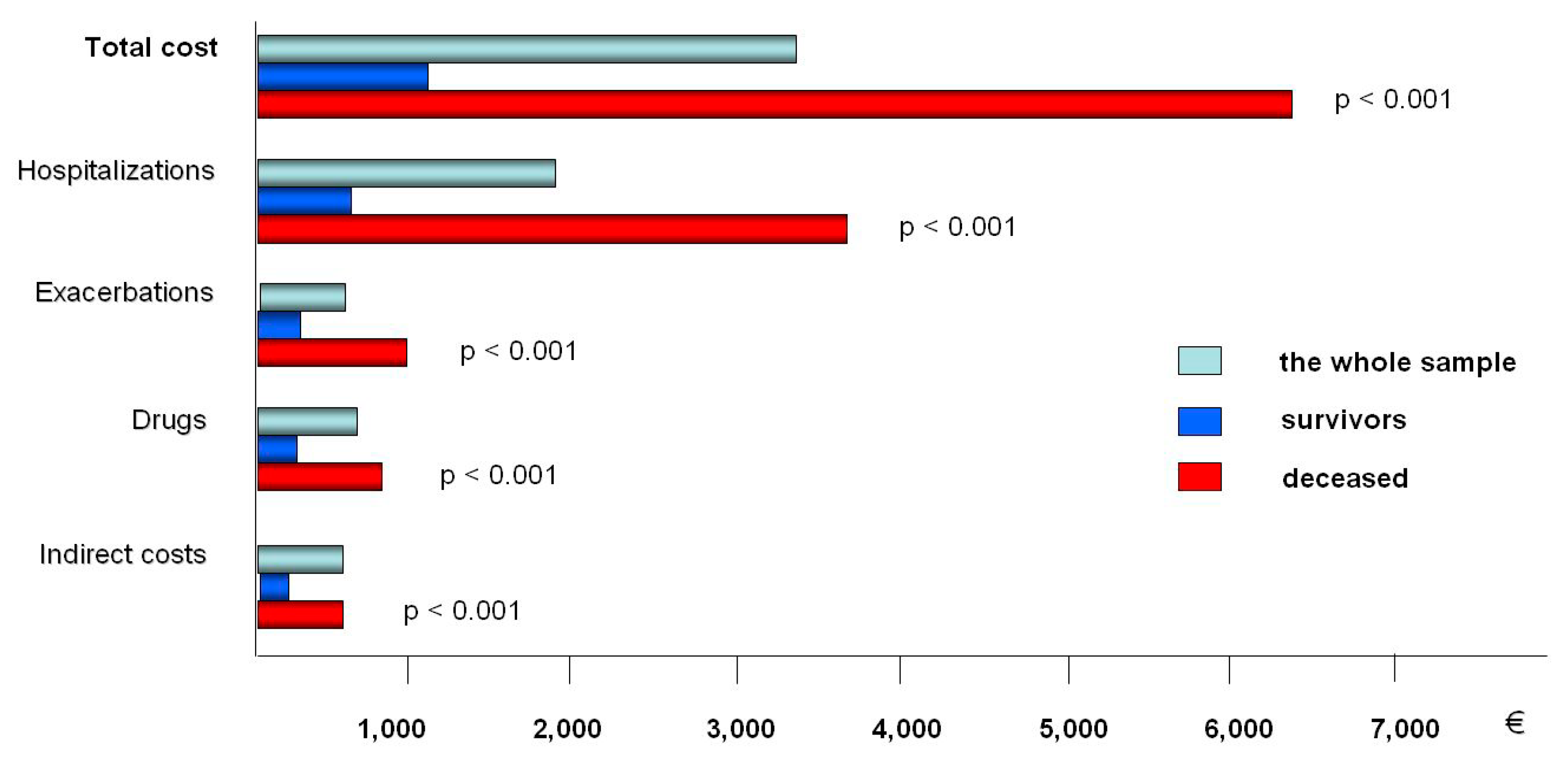
| Classification | Costs (Mean (95% CI)) |
|---|---|
| Direct Costs | 2932.2 (2643.1, 3221.3) |
| Hospitalization Costs | 1970.4 (968.0, 2972.8) |
| Out-patient Costs | 463.2 (207.5, 718.9) |
| Pharmaceutical Costs | 498.6 (252.5, 744.7) |
| Indirect Costs | 358.5 (119.0, 598.0) |
| Total Costs | 3290.7 (2539.9, 4051.2) |
| Pro-Bode Score (Points) | Survival (Days) | Cost (€) |
|---|---|---|
| 0–2 (n = 142) | 1023.8 (198.9) | 494.8 (1,454.2) |
| 3–4 (n = 66) | 889.5 (239.4) | 2040.9 (2079.0) |
| 5–6 (n = 36) | 762.2 (283.4) | 4952.9 (2265.3) |
| 7–10 (n = 31) | 752.1 (226.7) | 9224.9 (7804.2) |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dal Negro, R.W. COPD: The Annual Cost-Of-Illness during the Last Two Decades in Italy, and Its Mortality Predictivity Power. Healthcare 2019, 7, 35. https://doi.org/10.3390/healthcare7010035
Dal Negro RW. COPD: The Annual Cost-Of-Illness during the Last Two Decades in Italy, and Its Mortality Predictivity Power. Healthcare. 2019; 7(1):35. https://doi.org/10.3390/healthcare7010035
Chicago/Turabian StyleDal Negro, Roberto W. 2019. "COPD: The Annual Cost-Of-Illness during the Last Two Decades in Italy, and Its Mortality Predictivity Power" Healthcare 7, no. 1: 35. https://doi.org/10.3390/healthcare7010035
APA StyleDal Negro, R. W. (2019). COPD: The Annual Cost-Of-Illness during the Last Two Decades in Italy, and Its Mortality Predictivity Power. Healthcare, 7(1), 35. https://doi.org/10.3390/healthcare7010035