Abstract
Background: The mirror neuron system (MNS) has been proposed as a key neural mechanism linking action perception, motor representation, and social cognition. This framework has increasingly been applied to pain research, encompassing pain empathy, observational learning of pain, and rehabilitative interventions such as mirror therapy. However, the literature is conceptually heterogeneous, methodologically diverse, and spans experimental, social, and clinical domains. Objective: This scoping review aims to map the extent, nature, and characteristics of the available evidence on the relationship between the MNS and pain, clarifying how MNS-related mechanisms are defined, investigated, and applied across different contexts. Methods: A scoping review was conducted using the methodological framework proposed by the Joanna Briggs Institute and reported in accordance with PRISMA-ScR guidelines. We searched PubMed/MEDLINE, Scopus, Web of Science, and PsycINFO. Studies were included if they addressed MNS-related mechanisms in pain processing, pain empathy, pain modulation, or pain rehabilitation. Eligible studies were charted and synthesized descriptively and thematically. Results: Twenty-one studies met the inclusion criteria. The evidence was predominantly derived from clinical and rehabilitative settings, with most studies focusing on mirror therapy or mirror visual feedback interventions. The majority of included populations consisting of adults with chronic pain conditions, particularly phantom limb pain and complex regional pain syndrome. Pain intensity, assessed mainly through self-reported clinical scales, was the most frequently reported outcome. A smaller number of studies investigated action observation or motor imagery paradigms, primarily in chronic musculoskeletal pain, showing short-term hypoalgesic effects. Across studies, substantial heterogeneity was observed in the conceptualization of MNS-related constructs, intervention protocols, outcome measures, and follow-up duration. Conclusions: Despite extensive theoretical discussion of the MNS, empirical applications are largely confined to clinical mirror-based interventions, with limited use of direct neurophysiological or neuroimaging markers. Since crucial conceptual and methodological gaps constrain comparability and translation into clinical practice, there is a need for clearer operational definitions and more integrated experimental and clinical research approaches.
1. Introduction
Pain is a multidimensional experience shaped by nociceptive input combined with cognitive, affective, and social processes [1]. Beyond individual perception, humans can understand, anticipate, and even modulate pain through social interactions, observation of others, and action-related representations [2,3]. In this context, the observation–action matching system, also referred to as the mirror neuron system (MNS), has been proposed as a neural substrate linking perception and action, supporting shared experiences such as action understanding, imitation, embodied simulation, and broader aspects of social cognition [4].
First described in the premotor and parietal cortices of non-human primates, mirror neurons fire during the execution of a goal-directed action and when observing the same action performed by others, suggesting a mechanism for action understanding and learning through perception–action coupling [5]. In humans, converging neuroimaging and neurophysiological evidence supports the existence of a distributed mirror-related network involving inferior frontal, inferior parietal, and sensorimotor regions [4,6].
In addition to motor representations, the MNS has been discussed within broader theoretical frameworks addressing higher-order cognitive and conscious processes, including awareness, understanding, empathy, and grounded cognition. From this perspective, mirror-related mechanisms have been proposed to contribute to the integration of sensory, motor, and contextual information that underlies embodied representations of the self and others [7]. Notably, alterations in these processes have been examined in neurodevelopmental conditions, such as autism spectrum disorders, further supporting the relevance of mirror-related networks for social cognition [8,9].
Although these broader conceptualizations extend beyond pain research per se, they provide an important theoretical background for interpreting MNS-related frameworks applied to pain, particularly in domains involving empathy, observation, and social modulation of pain experience. Interestingly, within pain research, MNS-related concepts have been applied in different and partially overlapping fields. For example, studies on pain empathy have shown that observing others in pain can activate brain regions involved in affective and, in part, sensorimotor processing, suggesting the role of embodied simulation and sensorimotor resonance in empathic pain responses [10]. Moreover, experimental paradigms of observational learning and social modulation of pain suggest that pain perception can be shaped by observing others’ pain behaviors or relief, potentially through action–perception coupling and expectation-based mechanisms [11,12]. Furthermore, in clinical and rehabilitative settings, interventions such as mirror therapy, mirror visual feedback, and action observation therapy explicitly rely on action observation and motor representation to modulate pain and functional outcomes, particularly in conditions such as phantom limb pain [13] and complex regional pain syndrome (CPRS) [14]. Core principles of the mirror neuron system are schematically illustrated in Figure 1.
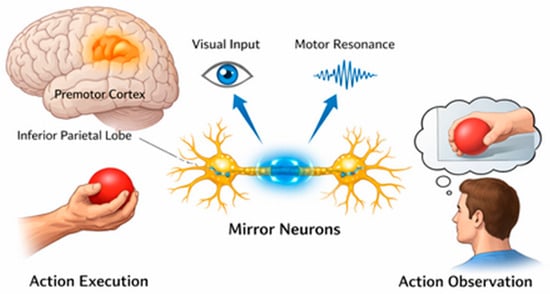
Figure 1.
Schematic representation of the mirror neuron system (MNS). Mirror neurons are classically described within a predominantly contralateral fronto-parietal network, including the premotor cortex and inferior parietal lobule. These neurons are activated both during the execution of a goal-directed action and during the observation of the same action performed by others. Visual input related to action observation is integrated with motor representations, giving rise to sensorimotor resonance and action–perception coupling mechanisms that are thought to support action understanding, imitation, and embodied simulation.
Despite this growing body of literature, the use of the term “mirror neuron system” in pain-related studies is far from uniform. Different studies rely on diverse proxies, such as functional magnetic resonance (fMRI) activation patterns [15] or electroencephalogram (EEG) mu rhythm suppression [16], and often conflate MNS-related mechanisms with broader constructs such as empathy, attention, salience, or expectancy. Moreover, the causal role of mirror mechanisms in pain modulation remains a topic of debate, and the translational relevance of experimental findings to clinical pain management is not always clear [17].
Given this conceptual and methodological heterogeneity, we performed a scoping review to systematically map how mirror neuron-related frameworks have been operationalized in pain research, identify dominant paradigms and outcomes, and highlight gaps requiring further investigation. The aim is to provide an integrative overview of the field and inform future hypothesis-driven and translational studies.
2. Materials and Methods
2.1. Protocol and Registration
This scoping review was conducted following the methodological framework proposed by the Joanna Briggs Institute [18] and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols extension for scoping review [19]. The protocol was registered in the collaborative project management tool Open Science Framework (https://osf.io/tgsj6/overview, accessed on 31 December 2025).
2.2. Eligibility Criteria
To be included in the review, articles needed to explicitly investigate or discuss MNS-related constructs using experimental, neurophysiological, neuroimaging, or clinical paradigms in relation to pain or pain-related outcomes. We considered publications in peer-reviewed journals and written in English. Only primary empirical studies (quantitative and qualitative) were included.
Concerning exclusion criteria, we excluded articles mentioning mirror neurons only tangentially, without empirical or conceptual linkage to pain-related outcomes. We also excluded editorials, commentaries, and opinion pieces without original data. Review articles were screened for citation tracking but were not included as primary evidence.
2.3. Search Strategy
The review was guided by the following research question: “What is known about how mirror neuron-related frameworks are defined, operationalized, and applied in pain research across experimental, social, and clinical contexts?”
The review was structured according to the Population-Concept-Context (PCC) framework:
- Population: Human participants (healthy individuals and/or patients with pain conditions).
- Concept: MNS or closely related constructs (e.g., action observation, motor imagery, mirror visual feedback, embodied simulation), explicitly linked to pain, nociception, analgesia, or pain empathy.
- Context: Experimental laboratory studies, social neuroscience paradigms, and clinical or rehabilitative settings.
The search strategy was developed by M.C. and V.C. following an initial exploratory phase aimed at identifying relevant keywords and minimizing noise and false-positive results. Preliminary searches were conducted to identify relevant literature and to examine keyword behavior, with particular attention to terms that could introduce noise or false-positive results. The search strategy combined terms related to the MNS (e.g., “mirror neuron”, “action observation”, “motor imagery”, “mirror therapy”) with pain-related terms (e.g., “pain”, “nociception”, “analgesia”, “pain empathy”). Based on this assessment, Boolean exclusion operators (NOT) were incorporated to progressively narrow the search and exclude records that were not aligned with the scope of the review. This iterative process allowed the refinement of the search strategy to maximize relevance while maintaining comprehensive coverage of the topic. The final search syntax was formulated using a combination of Boolean operators (AND, OR, and NOT) and truncation techniques (e.g., wildcards and quotation marks) and was applied across eight electronic databases. The full search strategy for at least one database is reported in Supplement S1. Reference lists of included articles were manually screened to identify additional relevant studies.
2.4. Information Sources
A comprehensive literature search was conducted in the following electronic databases: PubMed/MEDLINE, Scopus, Web of Science, and PsycINFO. The bibliographic search was conducted in November 2025 and covered all records available up to December 2024. In addition, the reference lists of all included studies and relevant reviews were manually screened to identify further eligible sources. No direct contact with study authors was undertaken.
Selection of Sources of Evidence
All records retrieved from the searches were imported into reference management software, and duplicates were removed. After duplicate removal, titles and abstracts were independently screened by two reviewers against the eligibility criteria (C.D. and G.S.). Full-text articles were subsequently assessed for eligibility by the same reviewers. Any discrepancies were resolved through discussion, with the involvement of M.C. when consensus could not be reached.
2.5. Data Charting Process
Data charting was independently performed by C.D. and G.S. using a standardized extraction form developed a priori. The following variables were extracted from each included study:
- Bibliographic details (author, year, country);
- Study aims and design;
- Population characteristics (sample size, health status);
- Definition and operationalization of mirror neuron system-related constructs;
- Experimental or clinical paradigm (e.g., fMRI, EEG, mirror therapy, action observation);
- Type and context of pain (e.g., experimentally induced pain, chronic pain, pain empathy);
- Outcomes assessed (neural, behavioral, clinical);
- Main findings related to MNS and pain;
- Reported limitations.
When necessary, data were simplified into broader conceptual categories (e.g., grouping different paradigms under “pain empathy” or “clinical interventions”) to facilitate mapping and synthesis. Reference management and data organization were supported by V.C. using dedicated bibliographic software (EndNote 2025, Clarivate Analytics).
2.6. Critical Appraisal of Individual Sources of Evidence
In accordance with the PRISMA-ScR guidelines, a formal critical evaluation of the methodological quality of the included studies was not planned or conducted. The main objective of this scoping review was to map the available evidence on interventions based on the MNS in the context of pain, rather than to evaluate the efficacy or methodological robustness of the studies. As a result, the evidence sources were summarized descriptively, without applying weighting criteria based on quality. Additionally, in accordance with the usual methodology for scoping reviews, an assessment of the risk of bias of the included studies was not performed.
2.7. Synthesis of Results
Extracted data were synthesized using descriptive statistics and narrative thematic analysis. In line with the objectives of this scoping review, the included studies were grouped based on the conceptual and methodological characteristics of their interventions related to the MNS and pain contexts. Specifically, the synthesis identified three main domains: (i) clinical interventions based on mirror therapy or mirror-based visual feedback, (ii) interventions based on action observation and motor imagery, and (iii) pain type and context, including phantom limb pain, CPRS, neuropathic pain, and musculoskeletal pain conditions.
3. Results
3.1. Selection of Sources of Evidence
The search in the databases identified a total of 2872 records (PubMed: 752; Scopus: 1037; Web of Science: 841; PsycINFO: 242). After the removal of 9 duplicates, 2863 records were screened for title and abstract. Of these, 2819 were excluded because they were not relevant to the PCC criteria. 44 full texts were therefore requested for the evaluation of eligibility; however, 3 items were not recovered. In total, 41 articles were evaluated in full text. Of these, 20 were excluded for the following reasons: inappropriate study design (n = 4), presence of systematic reviews (n = 5), and lack of consistency with PCC criteria (n = 11). Finally, 21 studies were included in the scoping review [20]. The selection process is shown in the PRISMA flowchart (Figure 2).
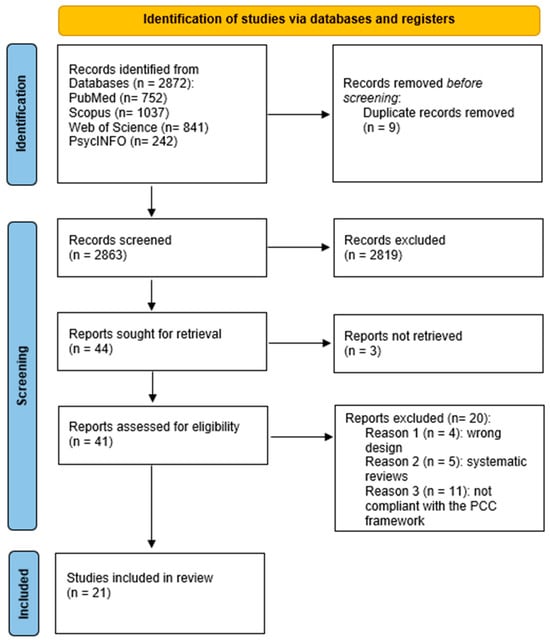
Figure 2.
PRISMA flowchart of the selection process.
3.2. Characteristics of Sources of Evidence
The populations analyzed consist mainly of adult patients suffering from chronic pain conditions, with a prevalence of studies focused on phantom limb pain in amputees [21,22,23,24,25,26,27,28,29,30,31,32]. Other studies included patients with complex regional pain syndrome [33,34,35], neuropathic pain secondary to nerve injury [36], and chronic or post-procedural musculoskeletal pain [37,38,39].
As for mirror neuron (MNS)-related constructs, these have been operationalized predominantly through mirror therapy or mirror visual feedback interventions [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,39,40], while a smaller number of studies have adopted action observation and motor imagery paradigms [37,38]. The interventions were mainly supplied in clinical rehabilitation settings, both outpatient and home-based, with a considerable variability in duration, frequency, and methods of administration. The outcomes assessed primarily included clinical measures of pain intensity, such as the Visual Analogue Scale (VAS) and Numerical Rating Scale (NRS), accompanied or not by functional, behavioral, or quality of life measures. Overall, mirror therapy emerged as the predominant MNS-related intervention, particularly in chronic pain conditions, whereas experimental paradigms directly targeting mirror neuron activity were largely absent (Table 1).

Table 1.
Characteristics of the included studies.
To further clarify the conceptual and methodological heterogeneity of the included studies, a mapping of MNS-related constructs, paradigms, and evidence gaps is presented in Table 2.
Table 2.
Conceptual and methodological mapping of mirror neuron system-related approaches in pain research.
3.3. Results of Individual Sources of Evidence
The included evidence sources examined interventions attributable to the mirror neuron system in relation to pain, using different clinical and experimental paradigms [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. Most studies evaluated mirror therapy or mirror visual feedback interventions applied to populations with chronic pain, particularly individuals with phantom limb pain and CPRS [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]. In these studies, pain intensity was mainly assessed using self-reported clinical scales, such as the VAS or the NRS, comparing the intervention with control conditions or conventional rehabilitation approaches [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35].
Some studies evaluated mirror therapy in combination with other rehabilitation or neuromodulatory interventions, including exercise programs, relaxation techniques, or non-invasive brain stimulation, and reported outcomes related to pain and, in some cases, functional measures [21,36].
Results were generally presented as changes in clinical outcomes over time or as between-group differences, without allowing direct comparisons between the different components of the interventions. A smaller number of studies adopted action observation and motor imagery paradigms, mainly in patients with chronic musculoskeletal pain, such as chronic neck pain [37,38]. In these studies, outcomes included pain intensity and pressure pain threshold, assessed immediately after the intervention or in the short term [27,38].
4. Discussion
Unlike previous reviews focusing on specific interventions or diseases [41], this scoping review maps how the MNS construct itself has been operationalized in pain research across experimental, social, and clinical contexts. In relation to the review question, interventions have been applied across different clinical pain conditions and methodological approaches, with areas that are well explored and others that remain insufficiently investigated. The main finding is that the existing evidence is predominantly focused on clinical and rehabilitative interventions, particularly mirror therapy and mirror visual feedback, rather than on direct experimental investigations of mirror neuron activity. Importantly, in the majority of the studies included, MNS involvement is not directly measured, but inferred indirectly from behavioral outcomes or clinical responses to mirror-based interventions. Neurophysiological or neuroimaging markers typically associated with MNS activities, such as EEG mu rhythm suppression or task-based fMRI activation, are rarely employed. As a result, the link between observed analgesic effects and mirror neuron mechanisms remains largely theoretical or inferential, limiting causal interpretation.
Although the MNS has been extensively discussed in social and affective neuroscience, particularly in relation to pain empathy and embodied simulation [10,17], these conceptual frameworks are rarely translated into empirical pain studies using direct neurophysiological or neuroimaging markers. Instead, MNS-related mechanisms are typically inferred indirectly through clinical interventions based on visual–motor feedback or action observation, consistent with early theoretical accounts of perception–action coupling [4,5,6]. Notably, this imbalance does not reflect a secondary theoretical role of experimental and social neuroscience evidence, highlighting a disconnect between foundational neuroscience models and their empirical application in pain research. Therefore, while experimental and social neuroscience studies have been central in shaping theoretical interpretations of MNS-related mechanisms, their contribution to pain research remains largely indirect, with limited integration into study designs, outcome measures, or mechanistic testing. This gap underscores the need for future research explicitly bridging experimental paradigms and clinical pain investigations.
Within the clinical domain, mirror therapy emerged as the most frequently studied paradigm. Across different settings and populations, several randomized and quasi-experimental studies reported reductions in pain intensity, particularly in phantom limb pain and type I CRPS [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]. However, findings were not uniform, and some well-designed trials failed to demonstrate clinically meaningful differences compared with control conditions or alternative interventions [25,35]. The failure of mirror therapy or mirror visual feedback to produce analgesic effects may arise from multiple, partially overlapping factors. They include, for instance, heterogeneity in intervention protocols, variability in patient characteristics, differences in pain etiology and chronicity, and limited engagement with the approach. Contextual factors and expectancy effects—mediated by cognitive and affective brain mechanisms—are well-established modulators of pain perception and clinical outcomes, independent of specific treatment mechanisms such as mirror neuron activation (e.g., placebo, clinician behavior, and verbal suggestion). A body of evidence suggests that several mechanisms, such as attentional modulation, multisensory integration, and expectation-driven brain responses, contribute substantially to analgesic outcomes [42,43,44]. Experimental evidence indicates that responses to observed pain are shaped by self-related and contextual factors, with key regions such as the anterior mid-cingulate cortex supporting expectancy, salience, and cognitive evaluation in addition to nociceptive processing [45]. Furthermore, studies using images of pain indicate that empathic responses can be elicited even in the absence of clear action-related or sensorimotor cues [46]. This evidence suggests that modulatory effects on pain arise from higher-order contextual and relational mechanisms (i.e., integrative, network-level frameworks of pain modulation) rather than from direct mirror neuron activation.
Action observation and motor imagery paradigms were explored in a smaller number of studies, mainly in chronic musculoskeletal pain conditions [37,38]. These studies suggested short-term hypoalgesia and increased pain thresholds, aligning with experimental evidence on sensorimotor engagement and expectation-driven modulation of pain [8,9]. However, the limited number of studies and the absence of long-term follow-up prevent firm conclusions regarding their sustained clinical relevance.
Overall, the evidence mapped in this review reveals a clear conceptual gap between the theoretical richness of MNS-related models and their empirical application in pain research. Although the language of mirror neurons, embodied simulation, and sensorimotor resonance is frequently employed, operational definitions and methodological approaches remain heterogeneous and often implicit. As a result, the MNS is commonly invoked as a broad explanatory framework rather than being operationalized as a testable and falsifiable neurobiological mechanism. For example, neuroimaging studies showed that observing pain-related facial expressions activates a distributed network overlapping with regions involved in first-hand pain processing and affective appraisal. However, this overlap reflects shared network-level engagement at the spatial resolution of fMRI, rather than direct evidence of identical neural populations or mirror-specific mechanisms underlying pain empathy or recognition [45].
Across studies, MNS-related terminology is used to describe diverse and partially overlapping phenomena—ranging from empathy and attention to expectancy and multisensory integration—without clear specification of the underlying neural processes or measurable markers. This lack of operational precision constrains mechanistic inference, reduces comparability across studies, and ultimately affects the translation of findings into coherent and clinically meaningful frameworks.
From a broader perspective, the role of the MNS in pain research should be interpreted in light of its theoretical evolution over the past two decades. Early models emphasized mirror neurons as discrete neural substrates supporting action understanding and embodied simulation [5,6]. However, more recent frameworks have progressively shifted attention toward distributed, network-level processes underlying perception–action coupling, expectation, and contextual modulation of pain [47,48]. In this context, the relative decline of studies explicitly testing mirror neuron activity in pain paradigms does not necessarily indicate waning interest, but rather reflects a conceptual reframing of MNS-related ideas within predictive processing and integrative brain models. These approaches emphasize how prior beliefs, contextual information, and multisensory integration shape pain experience, often without requiring strict attribution to mirror neuron activation. This view aligns with critical accounts that challenge classical mirror neuron interpretations and emphasize alternative, distributed explanatory mechanisms [17]. Consequently, contemporary pain research increasingly situates MNS-related concepts as part of broader explanatory frameworks rather than as isolated or dominant mechanisms.
4.1. Limitations
This scoping review has several limitations. First, only studies published in English and indexed in selected databases were included, potentially excluding relevant evidence from other sources. Second, consistent with PRISMA-ScR recommendations, no formal assessment of methodological quality or risk of bias was performed; therefore, the strength of evidence supporting individual interventions cannot be inferred. Third, the included studies were highly heterogeneous in terms of design, populations, interventions, and outcomes, which limited the ability to perform quantitative synthesis or direct comparisons.
In addition, although the review aimed to capture experimental, social, and clinical perspectives, the included evidence was largely confined to clinical rehabilitation studies. As a result, experimental neuroimaging and neurophysiological investigations of mirror neuron activity in pain contexts were underrepresented, reflecting a gap in the literature rather than a limitation of the review process itself.
4.2. Implications for Practice
From a clinical and nursing perspective, the findings of this scoping review suggest that MNS-related interventions, particularly mirror therapy and action observation-based approaches, represent low-cost, non-invasive, and potentially scalable strategies for pain management, especially in chronic pain conditions such as phantom limb pain. These interventions can be integrated into multidisciplinary pain management programs and, in some cases, delivered in home-based or self-managed formats [26,27].
However, the current evidence base does not support a one-size-fits-all application. Variability in patient characteristics, pain etiology, and intervention protocols underscores the need for individualized care planning and close monitoring of outcomes. For nursing practice, this highlights the importance of patient education, adherence support, and contextual factors such as therapeutic alliance and expectation management, which are known to influence pain outcomes [2,3,9].
Moreover, the conceptual overlap between MNS-related frameworks and broader constructs such as empathy, attention, and expectancy should not be interpreted as evidence that nursing practice operates through mirror neuron mechanisms. These constructs highlight well-established contextual and relational factors known to influence pain perception and clinical outcomes [49]. From a nursing perspective, contributions to pain management primarily arise from patient education, therapeutic alliance, expectation management, and support of adherence to treatment, rather than from any specific neurobiological mechanism related to mirror neuron activity. Framing these effects in contextual and relational terms avoids mechanistic oversimplification and remains consistent with current evidence on pain modulation.
5. Conclusions
This scoping review provides a comprehensive overview of how mirror neuron-related frameworks have been applied in pain research. The mapped evidence indicates that, despite extensive theoretical discussion of the MNS in neuroscience, empirical applications in pain research are predominantly clinical and centered on mirror therapy-based interventions. While several studies report beneficial effects on pain outcomes, substantial heterogeneity in conceptualization, methodology, and reporting limits the comparability and generalizability of findings.
Future research should aim to bridge the gap between theoretical models and clinical practice by employing clearer operational definitions, incorporating direct neurophysiological or neuroimaging markers when feasible, and designing longitudinal studies with standardized outcomes. Such efforts may help clarify the role of mirror neuron-related mechanisms in pain modulation and support their integration into evidence-based, patient-centered pain management strategies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare14020280/s1. Supplement S1 contains the search string of the consulted databases.
Author Contributions
Conceptualization, M.C. and V.C.; methodology, A.V.; software, P.M.; validation, M.C., V.C. and F.M.; formal analysis, C.D.F.; investigation, G.S.; resources, A.V.; data curation, P.M.; writing—original draft preparation, M.C.; writing—review and editing, V.C.; visualization, V.C.; supervision, F.M.; project administration, V.C.; funding acquisition, F.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing does not apply to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Wiech, K. Deconstructing the sensation of pain: The influence of cognitive processes on pain perception. Science 2016, 354, 584–587. [Google Scholar] [CrossRef]
- Schafer, S.M.; Geuter, S.; Wager, T.D. Mechanisms of placebo analgesia: A dual-process model informed by insights from cross-species comparisons. Prog. Neurobiol. 2018, 160, 101–122. [Google Scholar] [CrossRef]
- Cattaneo, L.; Rizzolatti, G. The mirror neuron system. Arch. Neurol. 2009, 66, 557–560. [Google Scholar] [CrossRef]
- di Pellegrino, G.; Fadiga, L.; Fogassi, L.; Gallese, V.; Rizzolatti, G. Understanding motor events: A neurophysiological study. Exp. Brain Res. 1992, 91, 176–180. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Sinigaglia, C. The functional role of the parieto-frontal mirror circuit: Interpretations and misinterpretations. Nat. Rev. Neurosci. 2010, 11, 264–274. [Google Scholar] [CrossRef]
- Tsytsarev, V. Methodological aspects of studying the mechanisms of consciousness. Behav. Brain Res. 2022, 419, 113684. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.M.Y.; Han, Y.M.Y. Differential mirror neuron system (MNS) activation during action observation with and without social-emotional components in autism: A meta-analysis of neuroimaging studies. Mol. Autism 2020, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; George, T.G.; Sobolewski, C.M.; McMorrow, S.R.; Pacheco, C.; King, K.T.; Rochowiak, R.; Daniels-Day, E.; Park, S.M.; Speh, E.; et al. Mapping brain function underlying naturalistic motor observation and imitation using high-density diffuse optical tomography. Imaging Neurosci. 2025, 3, IMAG.a.153. [Google Scholar] [CrossRef]
- Lamm, C.; Decety, J.; Singer, T. Meta-analytic evidence for common and distinct neural networks associated with directly experienced pain and empathy for pain. Neuroimage 2011, 54, 2492–2502. [Google Scholar] [CrossRef] [PubMed]
- Bieniek, H.; Bąbel, P. The Effect of the Model’s Social Status on Placebo Analgesia Induced by Social Observational Learning. Pain Med. 2022, 23, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Atlas, L.Y. How Instructions, Learning, and Expectations Shape Pain and Neurobiological Responses. Annu. Rev. Neurosci. 2023, 46, 167–189. [Google Scholar] [CrossRef]
- Xie, H.M.; Zhang, K.X.; Wang, S.; Wang, N.; Wang, N.; Li, X.; Huang, L.P. Effectiveness of Mirror Therapy for Phantom Limb Pain: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Khoramdel, F.; Ravanbod, R.; Akbari, H. Effect of high-intensity laser therapy and mirror therapy on complex regional pain syndrome type I in the hand area: A randomized controlled trial. J. Hand Ther. 2025, 38, 791–798. [Google Scholar] [CrossRef]
- Zhou, Z.; Chen, S.; Li, Y.; Zhao, J.; Li, G.; Chen, L.; Wu, Y.; Zhang, S.; Shi, X.; Chen, X.; et al. Comparison of Sensory Observation and Somatosensory Stimulation in Mirror Neurons and the Sensorimotor Network: A Task-Based fMRI Study. Front. Neurol. 2022, 13, 916990. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.A.; Bakermans-Kranenburg, M.J.; Yoo, K.H.; Bowman, L.C.; Cannon, E.N.; Vanderwert, R.E.; Ferrari, P.F.; van Ijzendoorn, M.H. Assessing human mirror activity with EEG mu rhythm: A meta-analysis. Psychol. Bull. 2016, 142, 291–313. [Google Scholar] [CrossRef]
- Hickok, G. Eight problems for the mirror neuron theory of action understanding in monkeys and humans. J. Cogn. Neurosci. 2009, 21, 1229–1243. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Implement. 2021, 19, 3–10. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Abolfazli, M.; Lajevardi, L.; Mirzaei, L.; Abdorazaghi, H.A.; Azad, A.; Taghizadeh, G. The effect of early intervention of mirror visual feedback on pain, disability and motor function following hand reconstructive surgery: A randomized clinical trial. Clin. Rehabil. 2018, 33, 494–503. [Google Scholar] [CrossRef]
- Brunelli, S.; D’Auria, L.; Stefani, A.; Giglioni, F.; Mariani, G.; Ciccarello, M.; Benedetti, M.G. Is mirror therapy associated with progressive muscle relaxation more effective than mirror therapy alone in reducing phantom limb pain in patients with lower limb amputation? Int. J. Rehabil. Res. 2023, 46, 193–198. [Google Scholar] [CrossRef]
- Noureen, A.; Ahmad, A.; Fatima, A.; Fatima, S.N. Effectiveness of mirror therapy on management of phantom limb pain and adjustment to limitation among prosthetic users; A single blinded randomized controlled trial. J. Bodyw. Mov. Ther. 2025, 42, 236–242. [Google Scholar] [CrossRef]
- Ol, H.; Van Heng, Y.; Danielsson, L.; Husum, H. Mirror therapy for phantom limb and stump pain: A randomized controlled clinical trial in landmine amputees in Cambodia. Scand. J. Pain 2018, 18, 603–610. [Google Scholar] [CrossRef]
- Purushothaman, S.; Kundra, P.; Senthilnathan, M.; Sistla, S.C.; Kumar, S. Assessment of efficiency of mirror therapy in preventing phantom limb pain in patients undergoing below-knee amputation surgery-a randomized clinical trial. J. Anesth. 2023, 37, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Rothgangel, A.; Braun, S.; Winkens, B.; Beurskens, A.; Smeets, R. Traditional and augmented reality mirror therapy for patients with chronic phantom limb pain (PACT study): Results of a three-group, multicentre single-blind randomized controlled trial. Clin. Rehabil. 2018, 32, 1591–1608. [Google Scholar] [CrossRef]
- Yıldırım, M.; Kanan, N. The effect of mirror therapy on the management of phantom limb pain. Agri 2016, 28, 127–134. [Google Scholar] [CrossRef]
- Shariaty, S.; Taheri, A. The home-based mirror therapy in the reduction of phantom limb pain in unilateral below-knee amputees. J. Neurosci. Rural Pract. 2024, 15, 552–556. [Google Scholar] [CrossRef]
- Finn, S.B.; Perry, B.N.; Clasing, J.E.; Walters, L.S.; Jarzombek, S.L.; Curran, S.; Rouhanian, M.; Keszler, M.S.; Hussey-Andersen, L.K.; Weeks, S.R.; et al. A Randomized, Controlled Trial of Mirror Therapy for Upper Extremity Phantom Limb Pain in Male Amputees. Front. Neurol. 2017, 8, 267. [Google Scholar] [CrossRef]
- Darnall, B.D.; Li, H. Home-based self-delivered mirror therapy for phantom pain: A pilot study. J. Rehabil. Med. 2012, 44, 254–260. [Google Scholar] [CrossRef]
- Anghelescu, D.L.; Kelly, C.N.; Steen, B.D.; Wu, J.; Wu, H.; DeFeo, B.M.; Scobey, K.; Burgoyne, L. Mirror Therapy for Phantom Limb Pain at a Pediatric Oncology Institution. Rehabil. Oncol. (Am. Phys. Ther. Association. Oncol. Sect.) 2016, 34, 104–110. [Google Scholar] [CrossRef]
- Külünkoğlu, B.A.; Erbahçeci, F.; Alkan, A. A comparison of the effects of mirror therapy and phantom exercises on phantom limb pain. Turk. J. Med. Sci. 2019, 49, 101–109. [Google Scholar] [CrossRef]
- Mallik, A.K.; Pandey, S.K.; Srivastava, A.; Kumar, S.; Kumar, A. Comparison of Relative Benefits of Mirror Therapy and Mental Imagery in Phantom Limb Pain in Amputee Patients at a Tertiary Care Center. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100081. [Google Scholar] [CrossRef]
- Cacchio, A.; De Blasis, E.; De Blasis, V.; Santilli, V.; Spacca, G. Mirror therapy in complex regional pain syndrome type 1 of the upper limb in stroke patients. Neurorehabilit. Neural Repair 2009, 23, 792–799. [Google Scholar] [CrossRef]
- McCabe, C.S.; Haigh, R.C.; Ring, E.F.; Halligan, P.W.; Wall, P.D.; Blake, D.R. A controlled pilot study of the utility of mirror visual feedback in the treatment of complex regional pain syndrome (type 1). Rheumatology 2003, 42, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, E.C.; Elhan, A.H.; Küçükdeveci, A.A. Effects of mirror therapy in post-traumatic complex regional pain syndrome type-1: A randomized controlled study. J. Rehabil. Med. 2024, 56, jrm40417. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.M.; de Carvalho, C.D.; Gomes, R.; Bonifácio de Assis, E.D.; Andrade, S.M. Transcranial Direct Current Stimulation and Mirror Therapy for Neuropathic Pain After Brachial Plexus Avulsion: A Randomized, Double-Blind, Controlled Pilot Study. Front. Neurol. 2020, 11, 568261. [Google Scholar] [CrossRef] [PubMed]
- Al Shrbaji, T.; Bou-Assaf, M.; Andias, R.; Silva, A.G. A single session of action observation therapy versus observing a natural landscape in adults with chronic neck pain–a randomized controlled trial. BMC Musculoskelet. Disord. 2023, 24, 983. [Google Scholar] [CrossRef]
- Suso-Martí, L.; León-Hernández, J.V.; La Touche, R.; Paris-Alemany, A.; Cuenca-Martínez, F. Motor Imagery and Action Observation of Specific Neck Therapeutic Exercises Induced Hypoalgesia in Patients with Chronic Neck Pain: A Randomized Single-Blind Placebo Trial. J. Clin. Med. 2019, 8, 1019. [Google Scholar] [CrossRef]
- Martín Pérez, S.E.; Rodríguez, J.D.; Kalitovics, A.; de Miguel Rodríguez, P.; Bortolussi Cegarra, D.S.; Rodríguez Villanueva, I.; García Molina, Á.; Ruiz Rodríguez, I.; Montaño Ocaña, J.; Martín Pérez, I.M.; et al. Effect of Mirror Therapy on Post-Needling Pain Following Deep Dry Needling of Myofascial Trigger Point in Lateral Elbow Pain: Prospective Controlled Pilot Trial. J. Clin. Med. 2024, 13, 1490. [Google Scholar] [CrossRef]
- Yun, D.-E.P.; Msa, K.; Pt, M.-K. Effects of mirror therapy on muscle activity, muscle tone, pain, and function in patients with mutilating injuries: A randomized controlled trial. Medicine 2019, 98, e15157. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, R.; Platano, D.; Donati, D.; Giorgi, F. Harnessing Mirror Neurons: A New Frontier in Parkinson’s Disease Rehabilitation-A Scoping Review of the Literature. J. Clin. Med. 2024, 13, 4539. [Google Scholar] [CrossRef]
- Rossettini, G.; Carlino, E.; Testa, M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet. Disord. 2018, 19, 27. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y. The neuroscience of placebo effects: Connecting context, learning and health. Nat. Rev. Neurosci. 2015, 16, 403–418. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.Y.; Lapanan, K.; Lin, Y.H.; Huang, C.W.; Lin, W.W.; Lin, M.M.; Lu, Z.L.; Lin, F.S.; Tseng, M.T. Integration of Prior Expectations and Suppression of Prediction Errors During Expectancy-Induced Pain Modulation: The Influence of Anxiety and Pleasantness. J. Neurosci. 2024, 44, e1627232024. [Google Scholar] [CrossRef]
- Benuzzi, F.; Lui, F.; Ardizzi, M.; Ambrosecchia, M.; Ballotta, D.; Righi, S.; Pagnoni, G.; Gallese, V.; Porro, C.A. Pain Mirrors: Neural Correlates of Observing Self or Others’ Facial Expressions of Pain. Front. Psychol. 2018, 9, 1825. [Google Scholar] [CrossRef] [PubMed]
- Schott, G.D. Pictures of pain: Their contribution to the neuroscience of empathy. Brain 2015, 138, 812–820. [Google Scholar] [CrossRef]
- Pessoa, L. Understanding brain networks and brain organization. Phys. Life Rev. 2014, 11, 400–435. [Google Scholar] [CrossRef]
- Heukamp, N.J.; Moliadze, V.; Mišić, M.; Usai, K.; Löffler, M.; Flor, H.; Nees, F. Beyond the chronic pain stage: Default mode network perturbation depends on years lived with back pain. Pain 2024, 166, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Rossettini, G.; Colloca, L.; Testa, M. The impact of contextual factors on nursing outcomes and the role of placebo/nocebo effects: A discussion paper. Pain Rep. 2019, 4, e716. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.