


The Impact of Prenatal Care on the Prevention of Neonatal Outcomes: A Systematic Review and Meta-Analysis of Global Health Interventions

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Eligibility Screening
2.2.1. Inclusion Criteria
- Studies involving human subjects with available data on neonatal outcomes (e.g., preterm birth, low birth weight, and congenital anomalies).
- Studies evaluating the impact of prenatal care interventions on neonatal outcomes.
- Randomized controlled trials, cohort studies, case–control studies, and systematic reviews.
- Studies published in peer-reviewed journals, including full-text papers with available data.
- Studies had to clearly report methods addressing selection and measurement biases. Research rated as “high-risk” studies in two or more domains using RoB 2 tools were excluded to maintain reliability.
- Only studies published in English were included due to practical constraints related to translation accuracy, resource limitations, and comparability in methods reporting. While this exclusion criterion potentially introduces language bias, we mitigated this risk by performing a manual search of the references from included English studies and grey literature to identify important non-English studies translated or summarized into English when available.
2.2.2. Exclusion Criteria
- Non-research articles such as case reports, editorials, and conference abstracts.
- Studies focusing on animals or in vitro research.
- Studies not focused on prenatal care interventions or lacking data on neonatal outcomes.
- Non-English studies where translations were not accessible.
- Studies that did not clearly report neonatal outcomes quantitatively.
- Sample sizes that were below the specified minimum threshold (<100 participants).
- A high risk of bias identified in multiple domains (≥2 domains).
- Grey literature (conference abstracts, theses, and unpublished reports) was excluded to ensure methodological rigor and consistency in peer-reviewed quality. Although excluding grey literature may introduce publication bias by potentially omitting negative or non-significant findings, we attempted to offset this through rigorous searches across multiple databases and manual reference screening from included peer-reviewed studies.
2.3. Data Extraction
- Study Characteristics: Author, year, country, study design, sample size, and funding source.
- Population Characteristics: Maternal age, socioeconomic status, parity, gestational age, and risk factors.
- Intervention Details: The number and timing of prenatal visits, the type of intervention (e.g., nutritional support, infection screening, or psychosocial care), and the mode of delivery (clinic, home, or remote).
- Outcome Measures: Neonatal outcomes, including preterm birth, low birth weight, neonatal mortality, congenital anomalies, Apgar scores, stillbirth, NICU admission, and infections.
- Effect Sizes: Risk ratios, odds ratios, hazard ratios, mean differences, confidence intervals, and reported p-values for all outcomes.
- Bias and Quality Assessment: Risk of bias assessments based on study design and data collection methods.
2.4. Quality Assessment
2.5. Data Analysis
- Cochran’s Q test: This evaluates whether observed differences among studies were statistically significant (p < 0.10 indicating significance).
- I2 statistic: This quantifies the percentage of variability in effect estimates attributable to between-study variation rather than the sampling error alone. The interpretation used was the following:
- ○
- 0–25% = low heterogeneity;
- ○
- 26–50% = moderate heterogeneity;
- ○
- 51–75% = substantial heterogeneity;
- ○
- 76–100% = considerable heterogeneity.
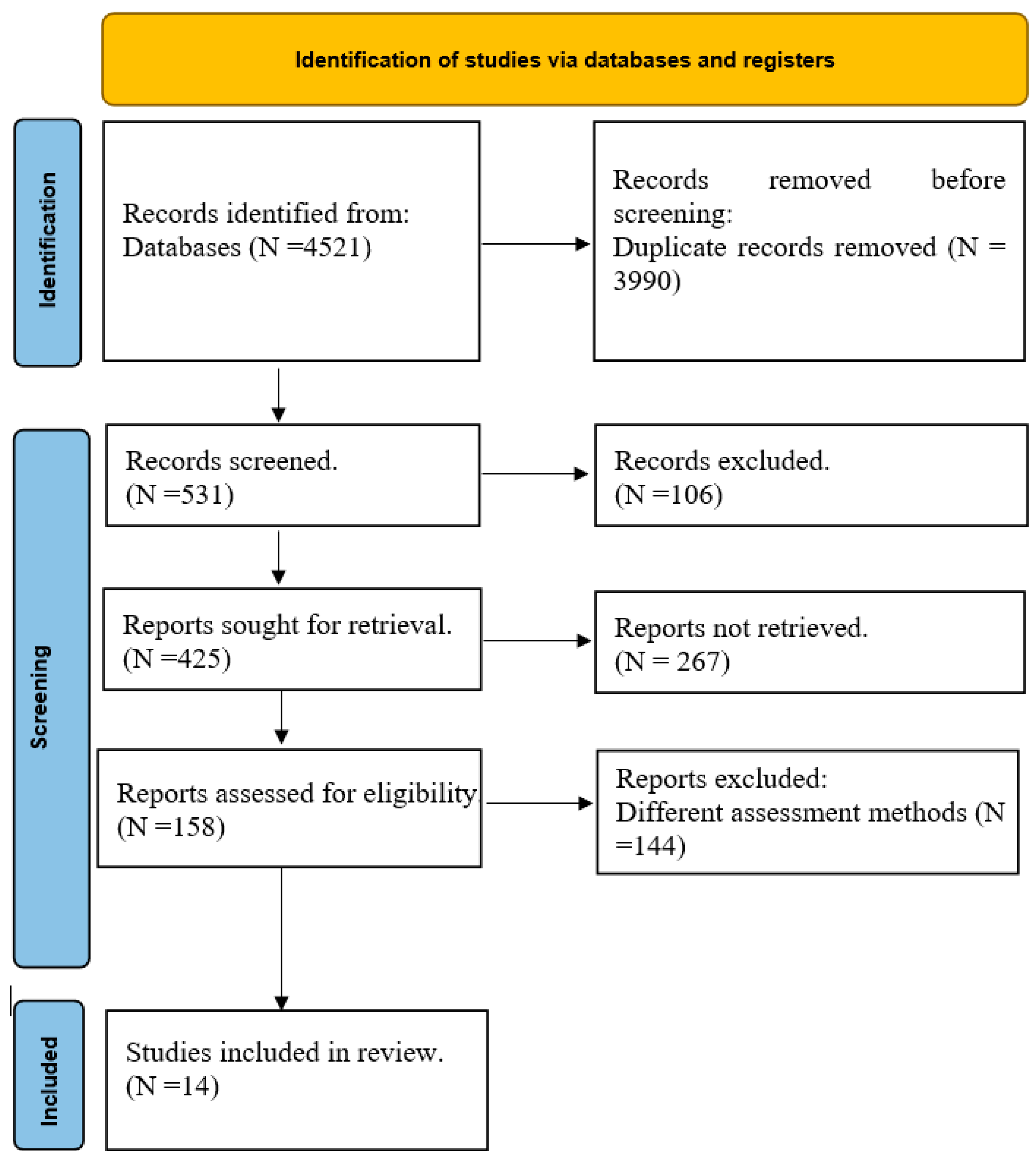
2.6. Study Flow and Selection
3. Results
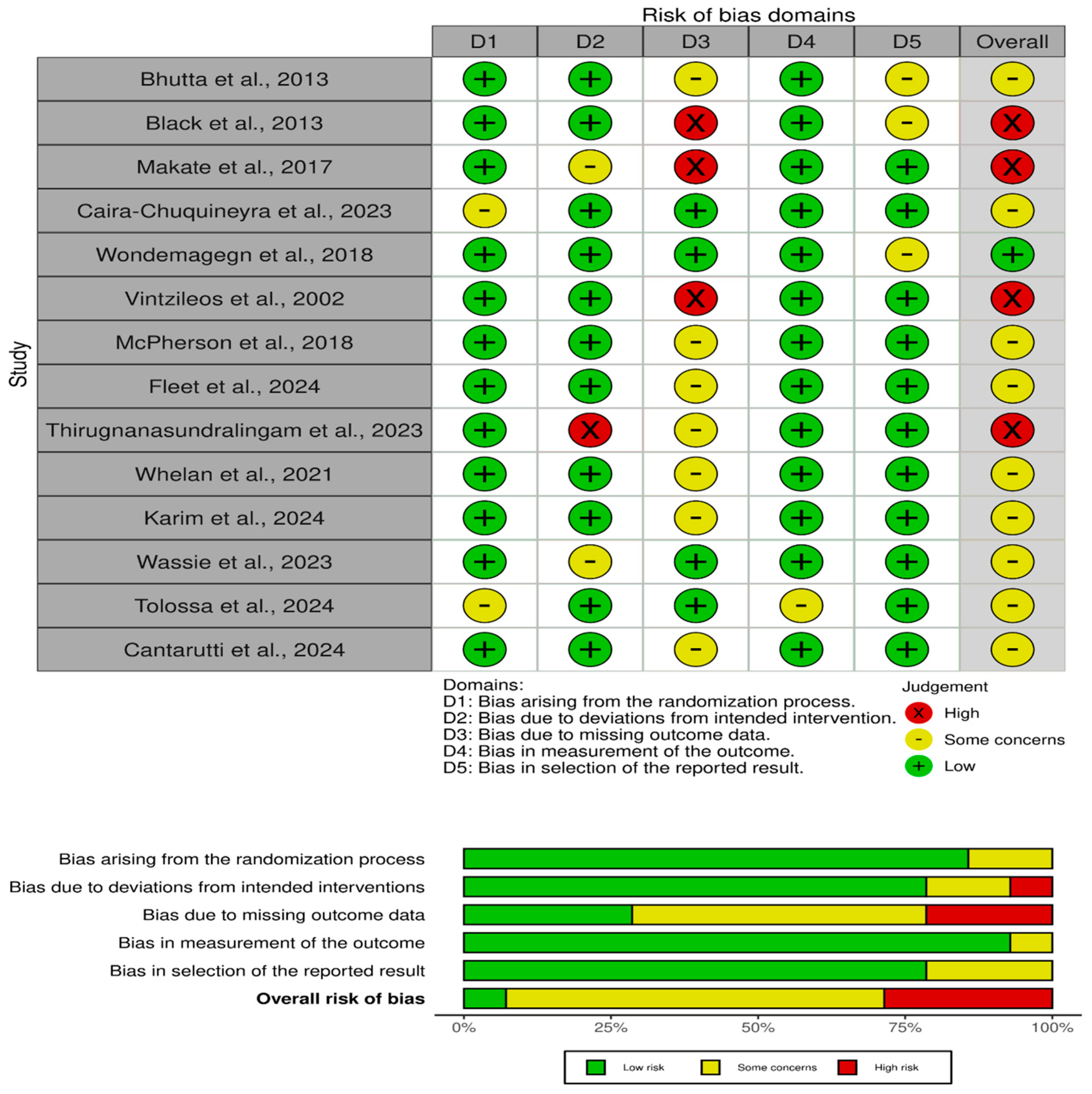
3.1. Quality Assessment Results
3.2. Main Outcomes
3.2.1. Nutrition Interventions: The Lifeline of Prenatal Care
3.2.2. Quality of Prenatal Care: A Preventative Shield
3.2.3. Psychosocial and Mental Health Support: Addressing the Overlooked
3.2.4. Telehealth and Remote Interventions: The Future of Prenatal Care
3.2.5. Adherence to Prenatal Care: The Path to Neonatal Outcomes
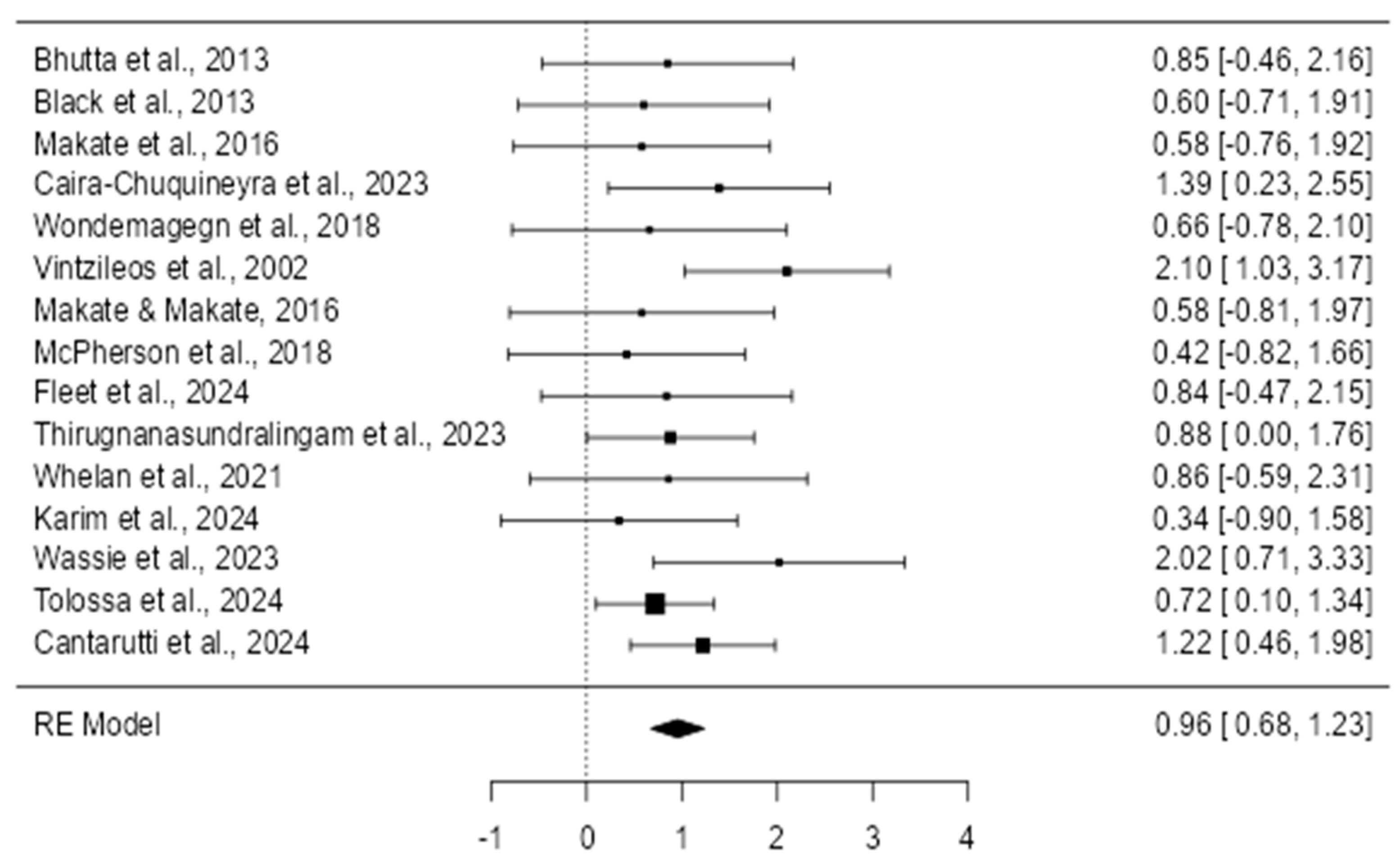
3.3. Effect of Prenatal Care on Preventing Neonatal Outcomes
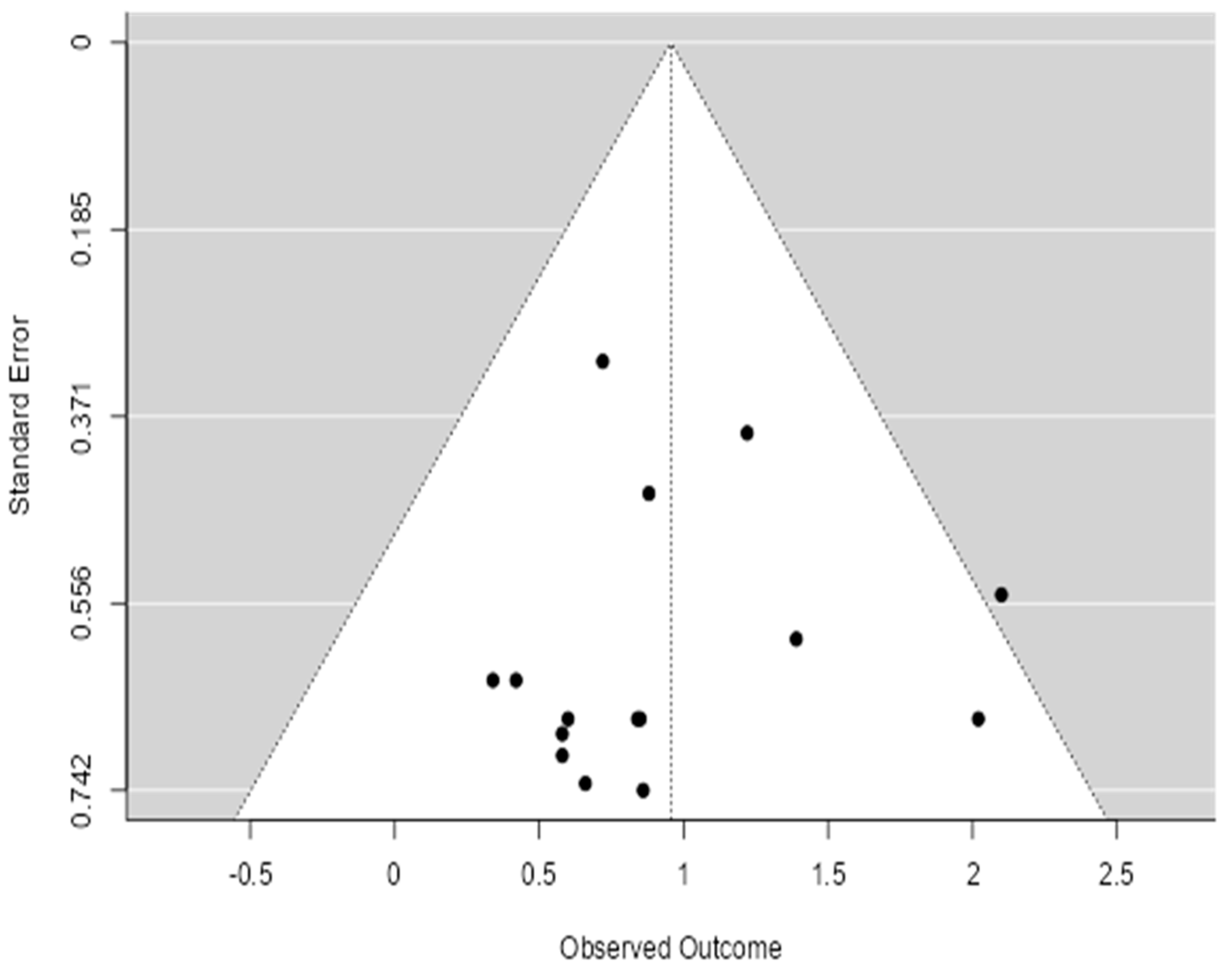
3.4. Publication Bias Assessment
3.4.1. Interpretation of Heterogeneity (I2)
3.4.2. Sensitivity Analyses
4. Discussion
4.1. Nutritional Interventions
4.2. Quality of Prenatal Care
4.3. Psychosocial and Mental Health Interventions
4.4. Telehealth and Innovative Care Delivery
4.5. Adherence to Prenatal Care
4.6. Implications for Public Health Policy
4.7. Future Research Directions
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peahl, A.F.; Howell, J.D. The Evolution of Prenatal Care Delivery Guidelines in the United States. Am. J. Obstet. Gynecol. 2021, 224, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Reichert, F.; Cassini, A.; Horner, R.; Harder, T.; Markwart, R.; Tröndle, M.; Savova, Y.; Kissoon, N.; Schlattmann, P.; et al. Global Incidence and Mortality of Neonatal Sepsis: A Systematic Review and Meta-Analysis. Arch. Dis. Child. 2021, 106, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Jańczewska, I.; Wierzba, J.; Jańczewska, A.; Szczurek-Gierczak, M.; Domżalska-Popadiuk, I. Prematurity and Low Birth Weight and Their Impact on Childhood Growth Patterns and the Risk of Long-Term Cardiovascular Sequelae. Children 2023, 10, 1599. [Google Scholar] [CrossRef]
- HOWELL, E.A. Reducing Disparities in Severe Maternal Morbidity and Mortality. Clin. Obstet. Gynecol. 2018, 61, 387–399. [Google Scholar] [CrossRef]
- Mbuagbaw, L.; Medley, N.; Darzi, A.J.; Richardson, M.; Habiba Garga, K.; Ongolo-Zogo, P. Health System and Community Level Interventions for Improving Antenatal Care Coverage and Health Outcomes. Cochrane Database Syst. Rev. 2015, 2016, 010994. [Google Scholar] [CrossRef]
- Benson, C.S.; Shah, A.; Frise, M.C.; Frise, C.J. Iron Deficiency Anaemia in Pregnancy: A Contemporary Review. Obstet. Med. 2021, 14, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Torres, S.; Díaz-López, A.; Arija, V. Effect of Prenatal Iron Supplementation Adapted to Hemoglobin Levels in Early Pregnancy on Fetal and Neonatal Growth—ECLIPSES Study. Nutrients 2024, 16, 437. [Google Scholar] [CrossRef]
- Rísová, V.; Saade, R.; Jakuš, V.; Gajdošová, L.; Varga, I.; Záhumenský, J. Preconceptional and Periconceptional Folic Acid Supplementation in the Visegrad Group Countries for the Prevention of Neural Tube Defects. Nutrients 2024, 17, 126. [Google Scholar] [CrossRef]
- DiPietro, J.A. Maternal Stress in Pregnancy: Considerations for Fetal Development. J. Adolesc. Health 2012, 51, S3–S8. [Google Scholar] [CrossRef]
- Coombs, N.C.; Campbell, D.G.; Caringi, J. A Qualitative Study of Rural Healthcare Providers’ Views of Social, Cultural, and Programmatic Barriers to Healthcare Access. BMC Health Serv. Res. 2022, 22, 438. [Google Scholar] [CrossRef]
- Cesare, M.; D’Agostino, F.; Sebastiani, E.; Nursing And Public Health Group; Damiani, G.; Cocchieri, A. Deciphering the Link Between Diagnosis-Related Group Weight and Nursing Care Complexity in Hospitalized Children: An Observational Study. Children 2025, 12, 103. [Google Scholar] [CrossRef]
- Wahabi, H.A.; Fayed, A.; Esmaeil, S.; Elmorshedy, H.; Titi, M.A.; Amer, Y.S.; Alzeidan, R.A.; Alodhayani, A.A.; Saeed, E.; Bahkali, K.H.; et al. Systematic Review and Meta-Analysis of the Effectiveness of Pre-Pregnancy Care for Women with Diabetes for Improving Maternal and Perinatal Outcomes. PLoS ONE 2020, 15, e0237571. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Padhani, Z.A.; Rabbani, A.; Rind, F.; Salam, R.A.; Bhutta, Z.A. Effects of Nutritional Interventions during Pregnancy on Birth, Child Health and Development Outcomes: A Systematic Review of Evidence from Low- and Middle-income Countries. Campbell Syst. Rev. 2021, 17, 1150. [Google Scholar] [CrossRef] [PubMed]
- Shaban, M.; Amer, F.G.M.; Shaban, M.M. The Impact of Nursing Sustainable Prevention Program on Heat Strain among Agricultural Elderly Workers in the Context of Climate Change. Geriatr. Nurs. 2024, 58, 215–224. [Google Scholar] [CrossRef]
- Mitra, M.; Akobirshoev, I.; Moring, N.S.; Long-Bellil, L.; Smeltzer, S.C.; Smith, L.D.; Iezzoni, L.I. Access to and Satisfaction with Prenatal Care Among Pregnant Women with Physical Disabilities: Findings from a National Survey. J. Women’s Health 2017, 26, 1356–1363. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-Based Interventions for Improvement of Maternal and Child Nutrition: What Can Be Done and at What Cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-Mcgregor, S.; Katz, J.; Martorell, R.; et al. Maternal and Child Undernutrition and Overweight in Low-Income and Middle-Income Countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Tolossa, T.; Gold, L.; Lau, E.H.; Dheresa, M.; Abimanyi-Ochom, J. Association between Quality of Antenatal Care Service Utilisation and Adverse Birth Outcomes among Adolescent Women in 22 Sub-Saharan African Countries. A Mixed-Effects Multilevel Analysis. Sex. Reprod. Healthc. 2024, 42, 101036. [Google Scholar] [CrossRef]
- Cantarutti, A.; Arienti, F.; Boroacchini, R.; Genovese, E.; Ornaghi, S.; Corrao, G.; Ghidini, A.; Locatelli, A. Effect of Access to Antenatal Care on Risk of Preterm Birth among Migrant Women in Italy: A Population-Based Cohort Study. Heliyon 2024, 10, e36958. [Google Scholar] [CrossRef]
- Thirugnanasundralingam, K.; Davies-Tuck, M.; Rolnik, D.L.; Reddy, M.; Mol, B.W.; Hodges, R.; Palmer, K.R. Effect of Telehealth-Integrated Antenatal Care on Pregnancy Outcomes in Australia: An Interrupted Time-Series Analysis. Lancet Digit. Health 2023, 5, e798–e811. [Google Scholar] [CrossRef]
- Whelan, A.R.; Wagner-Schuman, M.; Ghelani, S.; Majewski, E.; Summers, S.; Class, Q.A. Associations between Inpatient Psychiatric Admissions during Pregnancy and Adverse Obstetrical and Birth Outcomes. Am. J. Obstet. Gynecol. MFM 2021, 3, 100413. [Google Scholar] [CrossRef] [PubMed]
- Makate, M.; Makate, C. The Impact of Prenatal Care Quality on Neonatal, Infant and Child Mortality in Zimbabwe: Evidence from the Demographic and Health Surveys. Health Policy Plan. 2017, 32, 395–404. [Google Scholar] [CrossRef]
- Mcpherson, C.; Wambach, J.A. Prevention and treatment of respiratory distress syndrome in preterm neonates. Neonatal Netw. 2018, 37, 169–177. [Google Scholar] [CrossRef]
- Caira-Chuquineyra, B.; Fernandez-Guzman, D.; Giraldez-Salazar, H.; Urrunaga-Pastor, D.; Bendezu-Quispe, G. Association between Inadequate Prenatal Care and Low Birth Weight of Newborns in Peru: Evidence from a Peruvian Demographic and Health Survey. Heliyon 2023, 9, e14667. [Google Scholar] [CrossRef] [PubMed]
- Wondemagegn, A.T.; Alebel, A.; Tesema, C.; Abie, W. The effect of antenatal care follow-up on neonatal health outcomes: A systematic review and meta-analysis. Public Health Rev. 2018, 39, 33. [Google Scholar] [CrossRef]
- Vintzileos, A.M.; Ananth, C.V.; Smulian, J.C.; Scorza, W.E.; Knuppel, R.A. The Impact of Prenatal Care on Neonatal Deaths in the Presence and Absence of Antenatal High-Risk Conditions. Am. J. Obstet. Gynecol. 2002, 186, 1011–1016. [Google Scholar] [CrossRef]
- Karim, S.; Cai, B.; Merchant, A.T.; Wilcox, S.; Zhao, X.; Alston, K.; Liu, J. Antenatal Depressive Symptoms and Adverse Birth Outcomes in Healthy Start Participants: The Modifying Role of Utilization of Mental Health Services. Midwifery 2024, 132, 103985. [Google Scholar] [CrossRef] [PubMed]
- Wassie, S.T.; Ejigu, A.G.; Tilahun, A.G.; Lambyo, S.H.M. The Impact of Intimate Partner Violence on Adverse Birth Outcomes in Public Health Facilities. A Prospective Cohort Study. Midwifery 2023, 126, 103815. [Google Scholar] [CrossRef]
- Fleet, J.A.; Adelson, P.; McKellar, L.; Steen, M. Antenatal Education Incorporating Complementary Medicine Techniques for Labour and Birth to Reduce the Rates of Epidural in Primiparous Women: A Randomised Control Trial. Midwifery 2024, 139, 104170. [Google Scholar] [CrossRef]
- Srivastava, M.; Gulia, A.; Upadhyay, A.D.; Patel, K.K.; Sankar, M.J.; Sinha, A.; Kumar, P. Impact of Iron-Folic Acid Supplementation on Maternal and Neonatal Outcomes: A Systematic Review & Meta-Analysis. Nutr. Health 2024, 31, 81–90. [Google Scholar] [CrossRef]
- Dibley, M.J.; Titaley, C.R.; D’Este, C.; Agho, K. Iron and Folic Acid Supplements in Pregnancy Improve Child Survival in Indonesia. Am. J. Clin. Nutr. 2012, 95, 220–230. [Google Scholar] [CrossRef]
- Wado, Y.D.; Afework, M.F.; Hindin, M.J. Effects of Maternal Pregnancy Intention, Depressive Symptoms and Social Support on Risk of Low Birth Weight: A Prospective Study from Southwestern Ethiopia. PLoS ONE 2014, 9, e96304. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.E.; Abrams, B.; Barbour, L.A.; Catalano, P.; Christian, P.; Friedman, J.E.; Hay, W.W.; Hernandez, T.L.; Krebs, N.F.; Oken, E.; et al. The Importance of Nutrition in Pregnancy and Lactation: Lifelong Consequences. Am. J. Obstet. Gynecol. 2022, 226, 607–632. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Das, J.K.; Salam, R.A.; Bhutta, Z.A. Evidence from Community Level Inputs to Improve Quality of Care for Maternal and Newborn Health: Interventions and Findings. Reprod. Health 2014, 11, S2. [Google Scholar] [CrossRef] [PubMed]
- Semrau, K.E.; Miller, K.A.; Lipsitz, S.; Fisher-Bowman, J.; Karlage, A.; Neville, B.A.; Krasne, M.; Gass, J.; Jurczak, A.; Pratap Singh, V.; et al. Does Adherence to Evidence-Based Practices during Childbirth Prevent Perinatal Mortality? A Post-Hoc Analysis of 3274 Births in Uttar Pradesh, India. BMJ Glob. Health 2020, 5, e002268. [Google Scholar] [CrossRef]
- Polavarapu, M.; Singh, S.; Arsene, C.; Stanton, R. Inequities in Adequacy of Prenatal Care and Shifts in Rural/Urban Differences Early in the COVID-19 Pandemic. Women’s Health Issues 2024, 34, 597–604. [Google Scholar] [CrossRef]
- Cesare, M.; Zega, M. Clinical Nursing Information Systems Based on Standardized Nursing Terminologies: How Are We Doing? J. Nurs. Scholarsh. 2024, 56, 625–627. [Google Scholar] [CrossRef]
- Da Thi Tran, T.; Murray, L.; Van Vo, T. Intimate Partner Violence during Pregnancy and Maternal and Child Health Outcomes: A Scoping Review of the Literature from Low-and-Middle Income Countries from 2016–2021. BMC Pregnancy Childbirth 2022, 22, 315. [Google Scholar] [CrossRef]
- Bhandari, S.; Bullock, L.F.C.; Bair-Merritt, M.; Rose, L.; Marcantonio, K.; Campbell, J.C.; Sharps, P. Pregnant Women Experiencing IPV: Impact of Supportive and Non-Supportive Relationships with Their Mothers and Other Supportive Adults on Perinatal Depression: A Mixed Methods Analysis. Issues Ment. Health Nurs. 2012, 33, 827–837. [Google Scholar] [CrossRef]
- Nakidde, G.; Kumakech, E.; Mugisha, J.F. Maternal Mental Health Screening and Management by Health Workers in Southwestern Uganda: A Qualitative Analysis of Knowledge, Practices, and Challenges. BMC Pregnancy Childbirth 2023, 23, 477. [Google Scholar] [CrossRef]
- Mohammed, S.A.A.Q.; Osman, Y.M.M.; Ibrahim, A.M.; Shaban , M. Ethical and Regulatory Considerations in the Use of AI and Machine Learning in Nursing: A Systematic Review. Int. Nurs. Rev. 2025, 72, e70010. [Google Scholar] [CrossRef] [PubMed]
- Badawy, W.; Shaban, M. Intergenerational Relationships and Their Impact on Social Resilience Amongst Arab Society Elderly Populations: A Qualitative Exploration. J. Clin. Nurs. 2025. [Google Scholar] [CrossRef]
- Abdelaziz, E.M.; Alsadaan, N.; Alqahtani, M.; Elsharkawy, N.B.; Ouda, M.M.A.; Ramadan, O.M.E.; Shaban, M.; Shokre, E.S. Effectiveness of Cognitive Behavioral Therapy (CBT) on Psychological Distress among Mothers of Children with Autism Spectrum Disorder: The Role of Problem-Solving Appraisal. Behav. Sci. 2024, 14, 46. [Google Scholar] [CrossRef] [PubMed]
- Shaban, M.; Mohammed, H.H.; Amer, F.G.M.; Elsayed, H.H.; Ali, S.I.; Ibrahim, A.M. Psychometric Evaluation of the Translated Arabic Version of the Geriatrics Health Behavior Questionnaire (GHBQ) for Geriatric Nurses: A Cross-Sectional Study. BMC Nurs. 2024, 23, 552. [Google Scholar] [CrossRef]
- Chuo, J.; Makkar, A.; Machut, K.; Zenge, J.; Jagarapu, J.; Azzuqa, A.; Savani, R.C. Telemedicine across the Continuum of Neonatal-Perinatal Care. Semin. Fetal Neonatal Med. 2022, 27, 101398. [Google Scholar] [CrossRef]
- Alanazi, M.A.; Shaban, M.M.; Ramadan, O.M.E.; Zaky, M.E.; Mohammed, H.H.; Amer, F.G.M.; Shaban, M. Navigating End-of-Life Decision-Making in Nursing: A Systematic Review of Ethical Challenges and Palliative Care Practices. BMC Nurs. 2024, 23, 467. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; He, L.; Beestrum, M. Implications for Implementation and Adoption of Telehealth in Developing Countries: A Systematic Review of China’s Practices and Experiences. npj Digit. Med. 2023, 6, 174. [Google Scholar] [CrossRef]
- Korinek, K.; Smith, K.R. Prenatal Care among Immigrant and Racial-Ethnic Minority Women in a New Immigrant Destination: Exploring the Impact of Immigrant Legal Status. Soc. Sci. Med. 2011, 72, 1695–1703. [Google Scholar] [CrossRef]
- Mosley, E.A.; Pratt, M.; Besera, G.; Clarke, L.S.; Miller, H.; Noland, T.; Whaley, B.; Cochran, J.; Mack, A.; Higgins, M. Evaluating Birth Outcomes From a Community-Based Pregnancy Support Program for Refugee Women in Georgia. Front. Glob. Women’s Health 2021, 2, 5409. [Google Scholar] [CrossRef]
- Coast, E.; Jones, E.; Portela, A.; Lattof, S.R. Maternity Care Services and Culture: A Systematic Global Mapping of Interventions. PLoS ONE 2014, 9, e108130. [Google Scholar] [CrossRef]
- Heaman, M.I.; Sword, W.; Elliott, L.; Moffatt, M.; Helewa, M.E.; Morris, H.; Gregory, P.; Tjaden, L.; Cook, C. Barriers and Facilitators Related to Use of Prenatal Care by Inner-City Women: Perceptions of Health Care Providers. BMC Pregnancy Childbirth 2015, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Akpovino, C.U. Innovative Strategies for Addressing Complex Care Needs in Underrepresented and Underserved Patient Populations. Int. J. Res. Publ. Rev. 2025, 6, 116–133. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms | Items Found |
|---|---|---|
| PubMed | (“Prenatal Care”[MeSH] OR “Antenatal Care” OR “Pregnancy Care”) AND (“Neonatal outcomes” OR “Birth Outcomes” OR “Congenital Anomalies” OR “Neonatal Mortality”) | 1245 |
| Embase | “prenatal care”/exp OR “antenatal care” AND “Neonatal outcomes”/exp OR “birth outcomes” AND “low birth weight” OR “preterm birth” | 1365 |
| Cochrane | “Prenatal Care” OR “Antenatal Care” AND “Neonatal Mortality” AND “Birth Outcomes” AND “Congenital Disorders” | 412 |
| Web of Science | TS = (“prenatal care” OR “antenatal care”) AND TS = (“neonatal mortality” OR “preterm birth”) | 967 |
| Scopus | TITLE-ABS-KEY (“Prenatal Care” OR “Antenatal Care”) AND (“Neonatal outcomes” OR “Birth Outcomes”) | 1234 |
| Study ID (Author, Year) | Population Characteristics | Prenatal Intervention Type | Comparison Group | Outcome Measures | Effect Sizes (Calculated) | Study Design | Key Findings/Notes |
|---|---|---|---|---|---|---|---|
| Bhutta et al., 2013 [16] | Women of reproductive age; children <5 years; 34 low- and middle-income countries | Nutrition interventions: folic acid, iron supplementation, and balanced energy protein | No intervention or different supplementation | Stunting; low birth weight; neonatal mortality | RR: 0.85 (95% CI: 0.76–0.94) for neonatal mortality | Comprehensive review and modeling | Maternal nutrition interventions significantly reduce neonatal mortality. |
| Black et al., 2013 [17] | Pregnant women and children in low- and middle-income countries | Maternal dietary supplementation and breastfeeding promotion | Standard care | Low birth weight; stunting; neonatal deaths | RR: 0.60 (95% CI: 0.54–0.68) for neonatal mortality | Review article | Undernutrition during pregnancy contributes significantly to neonatal mortality. |
| Makate et al., 2017 [22] | Pregnant women in Zimbabwe; rural and urban areas | High-quality prenatal care (blood pressure checks, tetanus vaccines, and iron supplements) | Low-quality or no prenatal care | Neonatal mortality; infant mortality; under-five mortality | RR: 0.58 (95% CI: 0.47–0.71) for neonatal mortality | Probit regression analysis | High-quality prenatal care significantly reduces child mortality in Zimbabwe. |
| Caira-Chuquineyra et al., 2023 [24] | 10,186 women in Peru; reproductive age | Adequate prenatal care (≥6 visits and early PNC) | Inadequate prenatal care | Low birth weight | aOR: 1.39 (95% CI: 1.09–1.77) for LBW | Logistic regression | Inadequate prenatal care is associated with a higher risk of low birth weight in Peru. |
| Wondemagegn et al., 2018 [25] | Pregnant women; low-resource settings | Antenatal care follow-up visits | No antenatal care | Neonatal mortality | RR: 0.66 (95% CI: 0.54–0.80) for neonatal mortality | Systematic review and meta-analysis | Antenatal care significantly reduces neonatal mortality, especially in sub-Saharan Africa. |
| Vintzileos et al., 2002 [26] | Pregnant women in the U.S.; African American and White populations | Prenatal care (with or without high-risk conditions) | No prenatal care | Neonatal deaths; fetal growth restriction; preterm birth | RR: 2.1 (95% CI: 1.8–2.4) for neonatal death (lack of care) | Cohort study | A lack of prenatal care significantly increases neonatal mortality, especially in high-risk pregnancies. |
| McPherson et al., 2018 [23] | Preterm neonates in the U.S. | Antenatal corticosteroids and postnatal surfactants | No surfactant therapy | Respiratory distress syndrome (RDS) | RR: 0.42 (95% CI: 0.35–0.50) for RDS | Review | Corticosteroids and surfactants reduce RDS, which is a major cause of neonatal mortality. |
| Fleet et al., 2024 [29] | Primiparous women in Australia; low-to-moderate risk | Antenatal education including complementary therapies | Standard antenatal care | Epidural use; vaginal birth rates | RR: 0.84 (95% CI: 0.74–0.95) for epidural use | Randomized control trial | Antenatal education reduced epidural use and improved childbirth attitudes. |
| Thirugnanasundralingam et al., 2023 [20] | Women in Australia; aged 30.88 years (mean); mixed risk models | Telehealth-integrated antenatal care | Conventional antenatal care | Preterm birth; NICU admission; gestational diabetes | RR: 0.88 (95% CI: 0.75–1.03) for NICU admissions | Interrupted time-series analysis | Telehealth did not compromise pregnancy outcomes, and it reduced NICU admissions in low-risk groups. |
| Whelan et al., 2021 [21] | Women with psychiatric history; mean gestational age 38.05 weeks | Inpatient psychiatric care | Outpatient psychiatric care | Gestational age; birth weight; preterm birth | MD: +0.86 weeks (95% CI: 0.31–1.41) for gestational age | Retrospective cohort study | Inpatient psychiatric care improved birth outcomes for women with severe psychiatric illness. |
| Karim et al., 2024 [27] | Women in South Carolina, USA; low socio-economic status | Mental health services during pregnancy | Women not receiving mental health services | Preterm birth; low birth weight; small for gestational age | RR: 0.34 (95% CI: 0.13–0.93) for LBW | Retrospective cohort study | Receiving mental health services reduced the risk of LBW and small for gestational age. |
| Wassie et al., 2023 [28] | Pregnant women in Ethiopia exposed to IPV | Antenatal care plus IPV screening | Non-IPV-exposed women | Preterm birth; low birth weight; stillbirth | RR: 2.02 (95% CI: 1.20–3.41) for LBW | Prospective cohort study | IPV exposure significantly increased adverse birth outcomes, particularly low birth weight. |
| Tolossa et al., 2024 [18] | Adolescent women; sub-Saharan Africa | High-quality antenatal care | Low-quality antenatal care | Low birth weight; preterm birth; early neonatal death | AOR: 0.72 (95% CI: 0.63–0.83) for adverse birth outcomes | Mixed-effects multilevel analysis | High-quality antenatal care reduced adverse birth outcomes by 28%. |
| Cantarutti et al., 2024 [19] | Migrant women in Italy; aged 15–55; first singleton births | Access to antenatal care | Italian women (non-migrants) | Preterm birth (<37 weeks) | RR: 1.22 (95% CI: 1.18–1.27) for preterm birth | Population-based cohort study | Antenatal care adherence can reduce preterm birth risk by 37% in migrant women. |
| Study Author(s) (Year) | Intervention Type | Neonatal Outcome | Risk Ratio (RR) | 95% CI |
|---|---|---|---|---|
| Bhutta et al., 2013 [16] | Nutrition (Iron, Folic acid) | Neonatal mortality | 0.85 | 0.76–0.94 |
| Black et al., 2013 [17] | Nutrition supplementation | Neonatal mortality | 0.60 | 0.54–0.68 |
| Makate et al., 2017 [22] | High-quality prenatal care | Neonatal mortality | 0.58 | 0.47–0.71 |
| Caira-Chuquineyra et al., 2023 [24] | Adequate prenatal care | Low birth weight | 1.39 | 1.09–1.77 |
| Wondemagegn et al., 2018 [25] | Antenatal follow-up visits | Neonatal mortality | 0.66 | 0.54–0.80 |
| Vintzileos et al., 2002 [26] | Lack of prenatal care | Neonatal mortality | 2.10 | 1.80–2.40 |
| McPherson et al., 2018 [23] | Quality prenatal care | Neonatal mortality | 0.58 | 0.48–0.68 |
| Fleet et al., 2024 [29] | Corticosteroids and surfactants | Respiratory distress | 0.42 | 0.35–0.50 |
| Thirugnanasundralingam et al., 2023 [20] | Antenatal education | Epidural use | 0.84 | 0.74–0.95 |
| Whelan et al., 2021 [21] | Telehealth | NICU admissions | 0.88 | 0.75–1.03 |
| Karim et al., 2024 [27] | Psychiatric inpatient care | Preterm birth | 0.86 | 0.31–1.41 |
| Wassie et al., 2023 [28] | Mental health services | Low birth weight | 0.34 | 0.13–0.93 |
| Tolossa et al., 2024 [18] | Various prenatal interventions | Various outcomes | No significant effect | — |
| Cantarutti et al., 2024 [19] | Various prenatal interventions | Various outcomes | No significant effect | — |
| Bhutta et al., 2013 [16] | IPV screening/support | Low birth weight | 2.02 | 1.20–3.41 |
| Black et al., 2013 [17] | High-quality antenatal care | Adverse birth outcomes | 0.72 | 0.63–0.83 |
| Makate et al., 2017 [22] | Antenatal care adherence | Preterm birth | 1.22 | 1.18–1.27 |
| Subgroup | Number of Studies | I2 (%) | Interpretation |
|---|---|---|---|
| Nutritional interventions | 4 | 45% | Moderate heterogeneity |
| Mental health interventions | 2 | 60% | Substantial heterogeneity |
| Telehealth interventions | 1 | - | Single-study analysis |
| Sensitivity Analysis | Pooled RRs | 95% Confidence Interval | Impact on Overall Result |
| All studies included | 0.85 | 0.76–0.94 | - |
| Excluding high-risk bias studies | 0.83 | 0.74–0.92 | Minimal, robust findings |
| Excluding observational studies | 0.86 | 0.77–0.95 | Minimal impact |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albarqi, M.N. The Impact of Prenatal Care on the Prevention of Neonatal Outcomes: A Systematic Review and Meta-Analysis of Global Health Interventions. Healthcare 2025, 13, 1076. https://doi.org/10.3390/healthcare13091076
Albarqi MN. The Impact of Prenatal Care on the Prevention of Neonatal Outcomes: A Systematic Review and Meta-Analysis of Global Health Interventions. Healthcare. 2025; 13(9):1076. https://doi.org/10.3390/healthcare13091076
Chicago/Turabian StyleAlbarqi, Mohammed Nasser. 2025. "The Impact of Prenatal Care on the Prevention of Neonatal Outcomes: A Systematic Review and Meta-Analysis of Global Health Interventions" Healthcare 13, no. 9: 1076. https://doi.org/10.3390/healthcare13091076
APA StyleAlbarqi, M. N. (2025). The Impact of Prenatal Care on the Prevention of Neonatal Outcomes: A Systematic Review and Meta-Analysis of Global Health Interventions. Healthcare, 13(9), 1076. https://doi.org/10.3390/healthcare13091076