Abstract
Background: The International Association for the Study of Pain (IASP) conceptualizes pain as a subjective experience, influenced by biopsychosocial factors, strongly related to the person’s environment and previous experience. It is necessary to understand painful experiences from birth and their influence on the self-perception of pain later in life. In addition, training competent health professionals to identify and treat pain becomes a priority. The main objective of the protocol is to describe the situations that influence pain perception. These influences are conceived from birth to adulthood, taking into account the gender perspective. Methods: This is a two-year exploratory mixed-methods educational intervention design, incorporating cross-sectional assessments at baseline. The research will be carried out in the academic community, including nursing students from two universities. The following will be carried out: (1) practical seminars (groups of 20–25) to increase future healthcare professionals’ awareness of pain-inducing procedures and critical thinking; (2) a peer-mentoring session, led by senior students, addressing pain research, its clinical impact, and strategies for improved pain management through theoretical and practical components; (3) supervised sessions, where students will learn and perform vital sign measurements (HR, SpO2), algometry, and the Cold Pressor Test (CPT) to assess pain perception, threshold, and tolerance, practicing in pairs; (4) a gender-specific questionnaire to evaluate students’ perceptions of pain, fostering reflection on gender differences in pain experiences. Discussion: The aim is to enhance knowledge about pain in future health professionals to increase their skills in the approach to pain. Conclusions: This study aims to promote formal academic contact between higher education students, promoting comprehensive care in the management of pain at different stages of life.
1. Introduction
The first formal definition of pain, proposed in 1979 by the IASP Subcommittee on Taxonomy and adopted by the IASP Council, conceptualized pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”, or described in such terms. This definition has been globally accepted by healthcare professionals and organizations, including the World Health Organization (WHO). Over the ensuing four decades, the scientific and clinical understanding of pain has expanded considerably [1,2,3]. This prompted the formation of a multinational IASP Presidential Task Force in 2018, composed of 14 experts in clinical and basic pain sciences, tasked with revisiting the original concept. In 2020, the IASP adopted a revised definition: “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” [4]. Pain is recognized as a subjective phenomenon shaped by biological, psychological, and social factors, with nociception and pain defined as distinct processes [4,5]. This perspective underpins the concept of “total pain,” which integrates physical, emotional, social, and spiritual dimensions [6]. Importantly, pain can be experienced and expressed even without verbal communication [5]. Early exposure to painful stimuli can disrupt neurodevelopment and increase vulnerability to long-term behavioral and neurological consequences. In NICUs, neonates often undergo up to 300 painful procedures, leading to cumulative effects on neuropsychosocial development and future pain processing [7,8,9,10,11,12,13].
Adverse Childhood Experiences (ACEs) affect over 50% of children worldwide and are associated with heightened pain sensitivity, stress-related cortisol responses, and poorer treatment outcomes in adulthood [14,15,16,17,18,19,20,21,22]. Women with a history of childhood abuse report greater pain intensity and lower thresholds compared with those without such histories [14,23,24,25,26]. Recognizing pain relief as a fundamental human right, the UN underscores that no individual should suffer avoidable pain when effective treatments exist [27]. For neonates, reliable assessment remains challenging, but validated scales such as NFCS, N-PASS, COMFORTneo, NIPS, and FLACC enable consistent evaluation and guide effective management [7,28,29,30,31]. In the case of adolescence and young people, chronic pain during this stage has been shown to be associated with functional limitations and mental health problems in adulthood, underscoring the importance of addressing it at an early stage [32] Furthermore, in line with more contemporary perspectives, adolescence is increasingly recognized as extending up to the age of 24 years, as it represents a critical biological, psychological, and social transition into adulthood [33].
Once pain is assessed, healthcare professionals must judiciously select appropriate treatments. Pharmacological interventions in neonates must be approached with caution due to metabolic variability and the risk of adverse effects [34]. Opioids, while commonly used in NICUs, are associated with adverse neurodevelopmental outcomes [20,35,36,37,38,39] and organ toxicity—including in the kidneys, liver, and lungs—owing to the functional immaturity of these systems in neonates [7,40,41].
Given the limitations of pharmacological therapies, non-pharmacological interventions are an invaluable adjunct in neonatal pain management. These interventions, which modulate nociceptive transmission or activate descending inhibitory pathways, are associated with minimal side effects. Techniques include sucrose administration, skin-to-skin contact (kangaroo care), breastfeeding, non-nutritive sucking, facilitated tucking, music therapy, massage, environmental modifications, and aromatherapy [7,20]. Combining non-pharmacological methods with pharmacological treatments yields superior analgesic outcomes compared to either approach alone [20,42,43].
Despite advances in pediatric pain management, significant barriers persist in healthcare settings [44,45]. International evidence shows that pain education in nursing curricula remains insufficient, with persistent gaps in students’ knowledge and attitudes despite longstanding initiatives [46,47]. In Europe and Spain, nurses’ competencies in pain assessment and management remain suboptimal, although educational interventions—particularly in pediatrics—have proven effective in improving knowledge and practice [48,49,50]. These gaps highlight the need for innovative projects that incorporate pediatric pain and a gender perspective into nursing education [51]. In line with this, the IASP designated 2024 as the Global Year for Sex and Gender Disparities in Pain, underscoring the role of biological and sociocultural factors, with women showing greater vulnerability and higher prevalence of chronic pain [52,53,54,55,56,57,58,59]. Recent studies in fibromyalgia, a female-predominant condition, reveal this disproportionate burden, where women reported their pain being minimized or attributed to psychological causes. These findings indicate that disparities in pain are not solely biologically mediated but also reinforced by clinical practice, highlighting the urgent need for reforms in research and professional training [60].
The relationship between pain and sport warrants attention, as different sports entail varying risks of injury and pain, which in turn influence athletic participation and performance. The chronification of pain is determined not only by the initial injury but also by psychosocial and neurophysiological factors, the duration of sports practice, and the specific sport type [61]. A recent study in professional and semi-professional football in the United Kingdom further emphasized this interplay, highlighting the emotional impact of injuries and the fear of re-injury, which substantially affected recovery and rehabilitation outcomes. These findings underscore the critical role of psychosocial factors in shaping both the experience and management of sports-related pain [62].
The primary aim of this protocol is to examine the factors that influence pain perception from a gender perspective, while equipping future healthcare professionals with the knowledge to deliver effective and equitable pain management. The specific objectives are: (1) to assess nursing students’ prior knowledge regarding the relationship between gender and pain; (2) to raise awareness of the impact of routine clinical procedures and promote reflection on personal pain perception; (3) to provide theoretical training on pediatric pain within a cultural and gender framework; (4) to train the research team in non-pharmacological pain management using problem-based learning (PBL); and (5) to develop students’ skills in applying non-pharmacological strategies through active learning methodologies.
2. Materials and Methods
The research follows a mixed-methods educational intervention design, incorporating cross-sectional assessments at baseline. It will run across two academic years (2025–2026 and 2026–2027) with the collaboration of two partner institutions: (a) the Faculty of Physiotherapy and Nursing, Toledo Campus, University of Castilla-La Mancha, Spain, and (b) the Faculty of Health Sciences, Francisco de Vitoria University, Madrid, Spain. Both institutions have established a consortium grounded in their mutual commitment to advancing pediatric pain education and embedding a gender perspective within health sciences training.
The analytical plan will include descriptive and inferential statistics to evaluate differences between groups, as well as regression models to explore associations between gender, pain perception, and related variables. This approach will enable a more comprehensive analysis of how developmental, clinical, and psychosocial experiences interact with gender aspects in the perception and management of pain, thereby strengthening the methodological rigor and explanatory power of this study.
To frame the approach according to the needs of the project, the objectives are subdivided taking into account the following stakeholders:
- (1)
- For students: to increase knowledge about total pain and pediatric pain; increase knowledge about non-pharmacological therapies for pediatric pain management and their practical application; to improve critical thinking; open up to sexual, social, gender and cultural diversity, and study how this impacts the perception of pain.
- (2)
- For university lecturers: to increase skills/competences in non-pharmacological treatments; using innovative pedagogical approaches, in different modalities (face-to-face/distance learning).
- (3)
- For universities involved in the project: to facilitate theoretical and practical studies in total pain and non-pharmacological management of pediatric pain; possibility of mobility and cooperation between partners; to develop innovative educational approaches (gamification); to produce face-to-face/distance learning formats; strengthen inter-university networks.
- (4)
- For higher education degrees outside the project: to facilitate free access to distance learning formats on pain. This research will promote education at the international level in different higher education health courses at the member universities of this study.
Participants: participants will be individuals enrolled in higher education nursing programs, where the following inclusion criteria will be taken into account: (a) being enrolled in person in the third academic year; (b) having completed the Anatomy and Physiology course; (c) being over 18 years of age. Exclusion criteria: (a) students under the age of 18; (b) students enrolled in distance learning programs; and (c) students enrolled in the Erasmus program.
Sample: the sample size calculation was based on the main outcome of interest, namely the detection of gender-related differences in pressure pain thresholds assessed with algometry. Assuming a response proportion of 50% (p = 0.5), with a 95% confidence level and a margin of error of ±5%, the required minimum sample size was estimated at 152 participants, using the standard formula for finite populations.
Participants will be recruited from both partner universities (N1 and N2). While balanced recruitment across sites will be sought, the final number of students at each university will depend on actual participation rates.
Data Collection Instruments: the evaluation instruments are detailed in the following sections. It is important to note that the universities participating in the project enroll students from various regions of their respective countries. Consequently, the sociocultural characteristics of the sample are considered representative within each participating institution.
Quantitative Data Collection from Students: quantitative data will be gathered using a variety of instruments. The full questionnaire will be self-administered by students in paper format.
Ethical considerations: this study has received approval from the Ethics Committee of the University of Francisco de Vitoria (registration 46/2024), as well as from the relevant academic authorities of the collaborating universities. Teaching staff and students will receive an oral briefing about this study from the research team (one or two members at each university). Those who choose to participate will then be provided with written information. It is mandatory for both teachers and students to sign an informed consent form prior to taking part in this study.
The project will be carried out with participating students, organized in groups of 20–25 (N = 80 per university), developing the following outcomes:
- Outcome 1.
A peer-mentoring session will be conducted in which participating students will attend a presentation designed and delivered by senior students (undergraduate or postgraduate) who are part of the research team at the participating universities. This session will aim to raise awareness of the importance of pain research as a central theme, in line with Objective 1. In addition, it will include the discussion of painful processes, their effects on both students and patients, their consequences, and the challenges of pain management, thereby addressing Objective 2, as these aspects are essential to improving care through more humane, holistic, and effective approaches.
Within this framework, the subsequent components should be understood as subthemes that expand on the main topic. The session will also explicitly integrate an analysis of the role of sex and gender in pain research, recognizing their critical influence on pain perception, expression, and management from a cultural perspective, in accordance with Objective 3 of this study. To achieve these goals, students will engage with scientific articles on pain and its multiple dimensions, develop infographics that synthesize key concepts, and actively participate in the class session itself, thereby reinforcing both theoretical knowledge and practical skills.
Furthermore, training will be provided to members of the research team at each of the participating universities, based on problem-based learning (PBL), thus fulfilling Objective 4.
Finally, through an activity that combines theoretical principles with practical applications, students will strengthen their understanding of pain from a non-pharmacological perspective and acquire the competencies necessary to act more effectively and safely for the benefit of patients. This training will be evaluated using a checklist to assess specific skills in the application of non-pharmacological techniques, thus achieving objective 5.
- Outcome 2.
Theoretical and practical explanation of the techniques to be performed:
- (1)
- Heart rate (HR) measurement technique and reference values in pediatrics.
- (2)
- Pulse oximetry measurement technique as a non-invasive method for determining blood oxygen levels (O2) by emitting a beam of light through a pulsatile capillary. Students will be informed of the pediatric reference value for pulse oximetry (SpO2 > 93) [63,64].
- (3)
- Algometry technique to determine the minimum pressure perceived by the participant as painful [65,66]. By gradually increasing the applied force on the skin, sensations progress from touch to pressure and finally to pain [67,68]. At specific measurement points (Table 1 and Table 2), students will rate pain intensity using a Visual Analogue Scale (VAS). The device will then be removed, and pain intensity will be recorded again using the VAS.
 Table 1. Sensitive points.
Table 2. Control points.
Table 1. Sensitive points.
Table 2. Control points.
This technique serves as an indirect measure of the effect on sensory fibers at various sensitive points of the human body. A handheld algometer with an incremental scale of 0.1 N (Wagner Instruments, model FDIX), featuring a 1 cm diameter circular applicator, will be used. The applicator will be positioned perpendicularly to the skin, with pressure applied at approximately 1 kg/cm2 per second. Three measurements will be taken at 30 s intervals, and the average will be recorded as the pressure pain threshold. A 2 min rest will be allowed between measurement points to minimize sensitization effects. According to the study by Buskila [67], 9 tender points and 4 control points are identified, which will be used in the protocol as follows [67]:
These measurements will always be marked on the skin by the same investigator to ensure greater accuracy.
- (4)
- Cold Pressor Test (CPT) [69] to assess pain threshold, tolerance, and intensity.
The test will be conducted using water at a temperature of 4–6 °C. Ice cubes will be removed before immersion to prevent direct skin contact. Participants will immerse their non-dominant forearm in the water, ensuring their fingertips touch the bottom of the container. Participants will be asked to verbally indicate when they first perceive discomfort by saying “it bothers me”, which will be recorded as their pain threshold. They will also rate the pain intensity using the VAS. Participants will then be instructed to withdraw their arm when they can no longer tolerate the pain, this point will be recorded as their pain tolerance. The pain intensity will again be rated on the VAS. If the participant does not withdraw their arm after 180 s, the test will be terminated—this is the maximum recommended duration, and participants will not be informed of this time limit in advance [69].
- Outcome 3.
All of these measurements explained in outcome 2 will be performed in groups of six students (Figure 1).
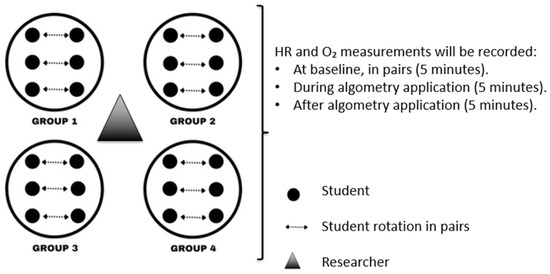
Figure 1.
Six students are assigned to each group to perform the different measurements outlined in the protocol. Tasks are rotated among participants, ensuring that each student alternates roles (examiner and subject). All activities are conducted under the direct supervision of the research team.
Each student will record their individual measurements including algometry and Cold Pressor Test on a designated form (Appendix A).
At the start of the intervention, a training video will be shown to teach students how to measure vital signs and use the algometer. Subsequently, each pair will have 60 min to perform measurements on both partners, followed by a 20 min break during which a gender-specific questionnaire will be completed. The total duration will be 80 min.
- Outcome 4.
A gender-specific questionnaire will be completed to analyze students’ perceptions of painful processes (Appendix B).
3. Discussion
This project aims to create an open resource for use in both higher education and the community to promote a comprehensive and healthy understanding of pain and non-pharmacological pain management in pediatrics, taking into account gender perspectives. It also aims to promote formal academic contact between undergraduate students and the concept of pain and, consequently, to increase discussion on the subject in the training of future health professionals. This is important, given that, to date, many health professionals have only had contact with the concept through an informal curriculum [70,71]. In many places, competence in pain management is not a parameter analyzed in the licensing of health professionals. As a consequence of this slow adoption of the concept in the academic curriculum, professionals are trained who do not feel prepared to identify and treat cases of pain [72]. Thus, the project aims to train future health professionals with better preparation in this area.
The overall objective will be achieved through the achievement of the results presented in the intervention. The objectives will be achieved in a multicenter manner, which will allow for a broad discussion on the topic addressed, favoring the democratization of access to knowledge.
The results of this project will improve the development of knowledge about pain in academic settings, with an emphasis on nursing. In a context where persistent or chronic pain is a growing cause of disability-related morbidity worldwide [73,74], the results of this protocol aim to reduce barriers and challenges in teaching about pain: the slow adoption of pain content in the curriculum of HE courses and the lack of preparation of university professors in teaching the subject [73].
Currently, many health professionals lack adequate training in the concept of pain [71,73], which makes it difficult to pass on this knowledge to students. In this way, teachers participating in the protocol, by teaching classes on the subject and training in Outcomes 1 and 2, will be able to address what happened during the project and also in future occasions, contributing to the maintenance of the concept in academic curricula.
In addition to the general concept of pain, the concept of pediatric pain and pain in women will also be addressed. Although studies on this topic have increased since the 1980s, it is still clear that there are major gaps in the treatment of childhood pain, largely due to the need for holistic studies holistic studies on the subject [75]. In this way, by promoting educational interventions with both students and teachers, the results of the protocol will encourage further discussion of the subject in academia, with an emphasis on the non-pharmacological treatment of pediatric pain.
Another important analysis that will be carried out through the results of the protocol is the relationship between self-perception of health status and cultural differences between the groups involved, through the application of the form presented in outcome 4. In its definition of the concept of health, the World Health Organization (WHO) takes into account the physical, mental and social aspects of the individual [76]. In this sense, pain is an important factor in self-perception of health status, which is modulated by factors common to those present in the WHO definition [6,77,78]. With the data collected from the form, it will be possible to observe how this perception changes according to the student’s environment, even in a multicentric way, since we know that it originates through a cognitive process, which occurs from the acquisition of information, meanings, interpretations and representations, which are acquired from the sociocultural environment to which the individual belongs [78,79]. In this context, it is known that self-perception of health status can influence individuals’ daily practices, being associated with their choices for certain healthcare practices, including self-medication [79]. Thus, the objective is to discover how students define, perceive and alleviate their pain, relating it to: their previous experiences; sports practice, which is related to psychosocial aspects and varies the interpretation of pain; and gender, emphasizing the differences in the assessment of pain and its treatment from a gender perspective, focusing on self-perception and management of menstrual pain in women.
This study has limitations that should be acknowledged. First, as a protocol focused on nursing students, the results will not be generalizable to other populations or health professionals. The findings will reflect the particular context of undergraduate nursing education and may therefore be influenced by cultural, institutional, and curricular factors. Second, data collection relies on self-reported information, which may be subject to recall bias and social desirability bias. Third, a control group was not incorporated into this study, since the objective is not to determine the effectiveness of a single, tightly controlled intervention, but to examine the feasibility, acceptability, and educational impact of introducing innovative teaching approaches across both universities. Consequently, the design emphasizes ecological validity and wide participation rather than strict internal validity.
Despite these limitations, this study will provide novel insights into the role of gender and prior experiences in shaping the perception of pain among nursing students, and it may serve as a basis for future research in broader populations and with more diverse methodological approaches.
4. Conclusions
This protocol seeks to promote the concept of pain in the academic sphere, contributing to the training of future health professionals who are competent in the identification and treatment of pain, with an emphasis on neonatal and pediatric pain, and who analyze the perception of pain through a sociocultural and gender perspective, so that they can provide optimal treatment for different social groups. Finally, it is worth highlighting the project’s work in promoting health among students, so that they can increase their critical awareness of self-perception of pain, how it influences daily routines, and the differences that exist in its expression and approach among different individuals.
Author Contributions
Conceptualization J.M.P.-P., V.L.-V. and S.G.-C.; methodology, S.H.-I. and S.G.-C.; software, N.G.-M.; validation, J.M.P.-P., M.H.-M. and S.G.-C.; formal analysis, Á.L.-G. and N.G.-M.; investigation, J.M.P.-P.; resources, A.C.-C.; data curation, A.C.-C., S.H.-I. and S.G.-C.; writing—original draft preparation, J.M.P.-P.; writing—review and editing, N.G.-M. and A.C.-C.; visualization, V.L.-V.; supervision, M.H.-M.; project administration, Á.L.-G., S.H.-I. and S.G.-C.; funding acquisition, J.M.P.-P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Universidad Francisco de Vitoria (UFV) (protocol code 46/2024 approved on 2 December 2025) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study. Written informed consent has been obtained from the students to publish this paper.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
The research team would like to thank the managers of Higher Education in the Nursing Degree, the possibility of implementing this Protocol.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| IASP | International Association for the Study of Pain |
| WHO | World Health Organization |
| NICUs | Neonatal Intensive Care Unit |
| ACEs | Adverse Childhood Experiences |
| HE | Higher Education |
| HR | Heart Rate |
| VAS | Visual Analogic Scale |
| CPT | Cold Pressor Test |
Appendix A
Table A1.
Measurement of Sensitive Points.
Table A1.
Measurement of Sensitive Points.
| Anatomical Point | Side | Measurement 1 (N) | Pain (VAS1) | Measurement 2 (N) | Pain (VAS2) | Measurement 3 (N) | Pain (VAS3) | Mean (N) |
|---|---|---|---|---|---|---|---|---|
| Upper Trapezius | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Upper Trapezius | Left | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Occipital | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Cervical Spine | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Second Rib | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Knee (Medial side) | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Knee (Medial side) | Left | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Lateral Epicondyle | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Greater Trochanter | Right | |||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Anatomic Point (2) | Measurement 1 (N) | Measurement 2 (N) | Measurement 3 (N) | Mean (N) | ||||
| Glabella | ||||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Right Forearm | ||||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Right Knee (Lateral side) | ||||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
| Right Metatarsus | ||||||||
| HR: | HR: | HR: | ||||||
| O2: | O2: | O2: | ||||||
* Thermal Pain: (1) threshold; (2) tolerance.
Observations:
| Time (s) | Pain (VAS) |
| Time (s) | Pain (VAS) |
| Source: own elaboration based on Buskila research [67]. | |
Appendix B
Appendix B.1. Specific Questionnaire for Women
PAIN MANAGEMENT IN WOMEN.
BLOCK 9. PAIN PERCEPTION AND MENSTRUAL EXPERIENCE.
- 1.
- At what age did you start menstruating?
| <12 years | Between 12 and 14 years | Between 15 and 17 years | >18 years |
- 2.
- Are your menstrual cycles regular?
- YES
 NO
NO
- 3.
- Indicate menstrual cycle frequency:
| <28 days | 28–32 days | ||
| >32 days | Irregular Cycles |
- 4.
- Do you usually experience menstrual pain (dysmenorrhea)?
- YES NO
- (If no, skip to question 10)
- 5.
- Evaluate your menstrual pain on a scale from 1 to 10:
- 6.

- 7.
- Which pattern describes your menstrual pain?
-
- Pain before bleeding, intense, then decreases
-
- Consistently intense pain throughout
-
- Mild but persistent pain
-
- Very mild pain that progressively disappears
-
- 8.
- Do you think your menstrual pain experience influences your perception of other types of pain?
- YES NO
- 9.
- Do you think men tolerate pain better than women?
- YES NO
BLOCK 10. MENSTRUAL PAIN MANAGEMENT.
- 10.
- What methods do you use to alleviate menstrual pain?
-
- Pharmacological analgesia
-
- Walking
-
- Relaxing baths
-
- Heat application
-
- Other: ________
-
- 11.
- Which drugs do you use? (multiple options possible):
|
| Have you ever needed oral contraceptives (OC) for menstrual pain? YES NO Are you currently taking OC? YES NO |
BLOCK 11. SOCIO-HEALTH ENVIRONMENT INFLUENCE.
- 1.
- Do you believe there is sufficient health education on menstrual pain prevention/management in your health/educational environment?
- YES NO
- 2.
- Do you consider healthcare professionals important in managing menstrual pain?
- YES NO
- 3.
- Evaluate on a Likert scale your satisfaction with the socio-health care received during menstruation:

Appendix B.2. Specific Questionnaire for Men
PAIN MANAGEMENT IN MEN.
BLOCK 6. KNOWLEDGE ABOUT MENSTRUAL PAIN
- 1.
- Do you think students should receive more training on menstrual pain to better understand their patients?
- YES NO
- 2.
- Menstrual pain can be disabling and significantly affect women’s daily activities.
| True | |
| False |
- 3.
- Do you think men tolerate pain better than women?
- YES NO
- 4.
- Indicate how important you think each of the following strategies is for managing menstrual pain:
- (a)
- Pharmacological therapy as a method to address menstrual pain and improve women’s quality of life

- (b)
- Non-pharmacological therapy (yoga, acupuncture, and relaxation techniques) as a method to address menstrual pain and improve women’s quality of life.

BLOCK 7. INFLUENCE OF THE SOCIO-HEALTH ENVIRONMENT ON THE PAINFUL MENSTRUAL EXPERIENCE
- 5.
- Do you consider that, in your healthcare and/or educational environment (high schools, universities, health centers, etc.), there is sufficient health education on the prevention and management of menstrual pain?
- YES NO
- 6.
- Do you consider healthcare professionals important in addressing menstrual pain?
- YES NO
BLOCK 8. MALE EXPERIENCE OF PAIN SELF-PERCEPTION
- 7.
- Do you think it is more common for men to ignore pain or delay going to the doctor compared to women?
- YES NO
- 8.
- What do you think is the main reason men tend to avoid going to the doctor for pain?
-
- Fear of receiving bad news
-
- Lack of time
-
- Belief that “the pain will go away on its own without professional help”
-
- Preference for handling pain with home remedies or self-medication
-
- 9.
- What type of pain do you think is most prevalent in the male population?
-
- Back pain, especially lower back pain
-
- Muscle and joint pain
-
- Abdominal or groin pain
-
- Testicular pain
-
- 10.
- Indicate which factor you believe is most relevant in the difference in pain self-perception according to sex (choose only one option):
-
- The different hormones in the body influence the pain threshold and tolerance between men and women.
-
- The attitude toward pain in terms of openly expressing it influences the pain threshold and tolerance between men and women.
-
- Seeking medical help influences the pain threshold and tolerance between men and women.
-
- 11.
- Regarding testicular pain from trauma (blow), do you consider it a medical emergency?
- YES NO
- 12.
- Regarding testicular pain from trauma, do you think there is a risk of serious complications such as a testicular hematoma, testicular torsion, or even rupture of the testicular membrane?
- YES NO
- 13.
- If you have ever suffered testicular trauma, did you go to the doctor to assess the situation to prevent possible complications and/or treat the associated pain?
- YES NO
Appendix B.3. General Questionnaire
SOCIO-DEMOGRAPHIC DATA OF THE PARTICIPANT.
| Nursing Degree | Degree in Physiotherapy | |
| 1st Year | ||
| 2nd Year | ||
| 3rd Year | ||
| 4th Year | ||
| Gender | Female | Male | Others | |||||
| Age | 18–25 | 26–33 | 33–40 | >40 | ||||
| University | UCLM (Toledo) | UCLM (Albacete) | UFV |
- Do you work while studying?: YES /NO

- Do you have family responsibilities?: YES /NO
PAINFUL EXPERIENCES AND PERSONAL PAIN MANAGEMENT TECHNIQUES.
BLOCK 1. PAIN AND PERINATAL EXPERIENCE.
- 1.
- In which week or month of gestation (WG) were you born?
| Less than 37 WG | Between 37–40 WG | More than 40 WG |
- 2.
- If you were born before 37 weeks of gestation, how many weeks exactly were you born?
- ____________________________________________________
- 3.
- How much did you weigh at birth?
- ____________________________________________________
- 4.
- If you know your APGAR score at birth, indicate it numerically:________________________________________________________
- 5.
- Were you born via vaginal delivery (natural/eutocic)?
- YES NO
- 6.
- If not, which method was used?
-
- Instrume-Forceps-assisted
-
- Spatula-assisted
-
- Vacuum-assisted
-
- Cesarean
-
- Other: ________
-
BLOCK 2. PREVIOUS PATHOLOGICAL EXPERIENCE.
- 7.
- Have you ever been admitted to the Neonatal or Pediatric Intensive Care Unit (NICU or PICU)?
- YES NO
- 8.
- Have you ever been hospitalized?
- YES NO
- 9.
- If yes, complete the following
- Age of admission: ________
- Length of stay (days): ________
- Reason for admission: ________
- Did you experience pain during hospitalization
- YES NO
- 10.
- Do you have any disease that causes pain?
- YES NO
- ____________________________________________________
- ____________________________________________________
- ____________________________________________________
- 11.
- If yes, which one?
BLOCK 3. HEALTHCARE ACCESS.
- 12.
- What type of healthcare center do you usually attend?
- Private Public
BLOCK 4. PAIN MANAGEMENT.
- 13.
- If you experience pain
- a.
- Do you seek healthcare assistance?
- b.
- Do you try to manage it at home by yourself?
- 14.
- Do you try to manage it at home by yourself?
- Rate your self-management capability from 1 to 10:

- 15.
- What measures do you usually take to relieve pain?
-
- Pharmacological analgesia
-
- Walking
-
- Relaxing baths
-
- Applying heat to the painful area (seed bags, hot water bottles)
-
- Other methods: ________
-
- 16.
- If using pharmacological measures, which drugs do you usually take? (select all that apply):
|
| Have you taken any of these drugs in the last 24 h? YES NO If yes, indicate which: ________________________ |
|
BLOCK 5. SPORTS AND PAIN.
- 17.
- What type of physical activity do you regularly do?
| Grade 0: Hiking only, walking to university/work, household chores | |
| Grade 1: Minimum WHO activity guidelines (2.5–5 h/week moderate or 1.5–2 h/week intense activity, group sports) | |
| Grade 2: Local competitive level | |
| Grade 3: National competitive level | |
| Grade 4: International competitive level |
- Indicate which sport: ________________________________________________________
References
- Anand, K.J.; Craig, K.D. New perspectives on the definition of pain. Pain 1996, 67, 3–6. [Google Scholar] [CrossRef]
- Aydede, M. Does the IASP definition of pain need updating? PAIN Rep. 2019, 4, e777. [Google Scholar] [CrossRef]
- Iglesias, S.B.O.; de Macedo Barbosa, S.M.; Carneiro Neves, C.; Luiz Ferreira, E.A.; de Araujo Torreao, L.; Michalowski, M.B.; de Oliveira, N.F.; Molinari, P.C.C.; Moraes, C.V.B. Dores Comuns em Pediatria: Avaliação e Abordagem; Sociedade Brasileira de Pediatria: São Paulo, Brazil, 2024; Volume 111. [Google Scholar]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- DeSantana, J.M.; Perissinotti, D.M.N.; Oliveira Junior, J.O.; Correia, L.M.F.; Oliveira, C.M.; Fonseca, P.R.B. Revised definition of pain after four decades. BrJP 2020, 3, 197–198. [Google Scholar] [CrossRef]
- Wood, J. Cicely Saunders, ‘Total Pain’ and emotional evidence at the end of life. Med. Humanit. 2022, 48, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.; Tan, Z.; Chen, J.; Weidig, T.; Xu, W.; Cong, X.S. Neonatal pain: Perceptions and current practice. Crit. Care Nurs. Clin. N. Am. 2018, 30, 549–561. [Google Scholar] [CrossRef]
- Dittz, E.; Malloy-Diniz, L.F. Dor neonatal e desenvolvimento neuropsicológico. Rev. Min. Enferm. 2006, 10, 266–270. [Google Scholar]
- Anand, K.J.; Hickey, P.R. Pain and its effects in the human neonate and fetus. N. Engl. J. Med. 1987, 317, 1321–1329. [Google Scholar] [CrossRef]
- Hatfield, L.A. Neonatal pain: What’s age got to do with it? Surg. Neurol. Int. 2014, 5 (Suppl. S13), S479–S489. [Google Scholar] [CrossRef] [PubMed]
- Kostovic, I.; Rakic, P. Developmental history of the transient subplate zone in the visual and somatosensory cortex of the macaque monkey and human brain. J. Comp. Neurol. 1990, 297, 441–470. [Google Scholar] [CrossRef]
- Hasegawa, M.; Houdou, S.; Mito, T.; Takashima, S.; Asanuma, K.; Ohno, T. Development of myelination in the human fetal and infant cerebrum: A myelin basic protein immunohistochemical study. Brain Dev. 1992, 14, 1–6. [Google Scholar] [CrossRef]
- Slater, R.; Fabrizi, L.; Worley, A.; Meek, J.; Boyd, S.; Fitzgerald, M. Premature infants display increased noxious-evoked neuronal activity in the brain compared to healthy age-matched term-born infants. Neuroimage 2010, 52, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Pace, C.S.; Muzi, S.; Rogier, G.; Meinero, L.L.; Marcenaro, S. The adverse childhood experiences—International Questionnaire (ACE-IQ) in community samples around the world: A systematic review (part I). Child Abuse Negl. 2022, 129, 105640. [Google Scholar] [CrossRef]
- Levy Gigi, E.; Rachmani, M.; Defrin, R. The relationship between traumatic exposure and pain perception in children: The moderating role of posttraumatic symptoms. Pain 2024, 165, 2274–2281. [Google Scholar] [CrossRef] [PubMed]
- Cabanis, M.; Outadi, A.; Choi, F. Early childhood trauma, substance use and complex concurrent disorders among adolescents. Curr. Opin. Psychiatry 2021, 34, 393–399. [Google Scholar] [CrossRef]
- Dempster, K.S.; O’Leary, D.D.; MacNeil, A.J.; Hodges, G.J.; Wade, T.J. Linking the hemodynamic consequences of adverse childhood experiences to an altered HPA axis and acute stress response. Brain Behav. Immun. 2021, 93, 254–263. [Google Scholar] [CrossRef]
- Soee, A.-B.L.; Skov, L.; Kreiner, S.; Tornoe, B.; Thomsen, L.L. Pain sensitivity and pericranial tenderness in children with tension-type headache: A controlled study. J. Pain Res. 2013, 6, 425–434. [Google Scholar] [CrossRef]
- Zohsel, K.; Hohmeister, J.; Oelkers-Ax, R.; Flor, H.; Hermann, C. Quantitative sensory testing in children with migraine: Preliminary evidence for enhanced sensitivity to painful stimuli especially in girls. Pain 2006, 123, 10–18. [Google Scholar] [CrossRef]
- van Dijk, M.; Roofthooft, D.W.; Anand, K.J.; Guldemond, F.; de Graaf, J.; Simons, S.; de Jager, Y.; van Goudoever, J.; Tibboel, D. Taking up the challenge of measuring prolonged pain in (premature) neonates: The COMFORTneo scale seems promising. Clin. J. Pain 2009, 25, 607–616. [Google Scholar] [CrossRef]
- Beveridge, J.K.; Dobson, K.S.; Madigan, S.; Yeates, K.O.; Stone, A.L.; Wilson, A.C.; Salberg, S.; Mychasiuk, R.; Noel, M. Adverse childhood experiences in parents of youth with chronic pain: Prevalence and comparison with a community-based sample. PAIN Rep. 2020, 5, e866. [Google Scholar] [CrossRef] [PubMed]
- Craner, J.R.; Lake, E.S.; Barr, A.C.; Kirby, K.E.; O’Neill, M. Childhood adversity among adults with chronic pain: Prevalence and association with pain-related outcomes. Clin. J. Pain 2022, 38, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Beal, S.J.; Kashikar-Zuck, S.; King, C.; Black, W.; Barnes, J.; Noll, J.G. Heightened risk of pain in young adult women with a history of childhood maltreatment: A prospective longitudinal study. Pain 2020, 161, 156–165. [Google Scholar] [CrossRef]
- Raphael, K.G.; Widom, C.S. Post-traumatic stress disorder moderates the relation between documented childhood victimization and pain 30 years later. Pain 2011, 152, 163–169. [Google Scholar] [CrossRef]
- Tesarz, J.; Eich, W.; Treede, R.-D.; Gerhardt, A. Altered pressure pain thresholds and increased wind-up in adult patients with chronic back pain with a history of childhood maltreatment: A quantitative sensory testing study. Pain 2016, 157, 1799–1809. [Google Scholar] [CrossRef]
- Scarinci, I.C.; McDonald-Haile, J.; Bradley, L.A.; Richter, J.E. Altered pain perception and psychosocial features among women with gastrointestinal disorders and history of abuse: A preliminary model. Am. J. Med. 1994, 97, 108–118. [Google Scholar] [CrossRef]
- Office of the High Commissioner for Human Rights (OHCHR). Advice of the Subcommittee on Prevention of Torture to States Parties and National Preventive Mechanisms Relating to the Coronavirus Pandemic (Adopted on 25 March 2020). Available online: https://www.ohchr.org/Documents/HRBodies/OPCAT/AdviceStatePartiesCoronavirusPandemic2020.pdf (accessed on 10 February 2025).
- Committee on Fetus and Newborn; Section on Anesthesiology and Pain Medicine. Prevention and management of procedural pain in the neonate: An update. Pediatrics 2016, 137, e20154271. [Google Scholar] [CrossRef]
- Grunau, R.E.; Craig, K.D. Pain expression in neonates: Facial action and cry. Pain 1987, 28, 395–410. [Google Scholar] [CrossRef]
- Hummel, P.; Puchalski, M.; Creech, S.D.; Weiss, M.G. Clinical reliability and validity of the N-PASS: Neonatal pain, agitation and sedation scale with prolonged pain. J. Perinatol. 2008, 28, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, J.; Alcock, D.; McGrath, P.; Kay, J.; MacMurray, S.B.; Dulberg, C. The development of a tool to assess neonatal pain. Neonatal Netw. 1993, 12, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Pud, D.; Aamar, S.; Schiff-Keren, B.; Sheinfeld, R.; Brill, S.; Robinson, D.; Fogelman, Y.; Habib, G.; Sharon, H.; Amital, H.; et al. Chronic pain in adolescence: Prevalence, impact, and clinical implications. PAIN Rep. 2024, 9, e1143. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Ancora, G.; Lago, P.; Garetti, E.; Pirelli, A.; Merazzi, D.; Pierantoni, L.; Ferrari, F.; Faldella, G. Follow-up at the corrected age of 24 months of preterm newborns receiving continuous infusion of fentanyl for pain control during mechanical ventilation. Pain 2017, 158, 840–845. [Google Scholar] [CrossRef]
- de Graaf, J.; van Lingen, R.A.; Simons, S.H.; Anand, K.J.; Duivenvoorden, H.J.; Weisglas-Kuperus, N.; Roofthooft, D.W.; Groot Jebbink, L.J.; Veenstra, R.R.; Tibboel, D.; et al. Long-term effects of routine morphine infusion in mechanically ventilated neonates on children’s functioning: Five-year follow-up of a randomized controlled trial. Pain 2011, 152, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, S.A.; Ward, W.L.; Paule, M.G.; Hall, R.W.; Anand, K.J. A pilot study of preemptive morphine analgesia in preterm neonates: Effects on head circumference, social behavior, and response latencies in early childhood. Neurotoxicol. Teratol. 2012, 34, 47–55. [Google Scholar] [CrossRef]
- Kocek, M.; Wilcox, R.; Crank, C.; Patra, K. Evaluation of the relationship between opioid exposure in extremely low birth weight infants in the neonatal intensive care unit and neurodevelopmental outcome at 2 years. Early Hum. Dev. 2016, 92, 29–32. [Google Scholar] [CrossRef]
- Ranger, M.; Synnes, A.R.; Vinall, J.; Grunau, R.E. Internalizing behaviours in school-age children born very preterm are predicted by neonatal pain and morphine exposure. Eur. J. Pain 2014, 18, 844–852. [Google Scholar] [CrossRef]
- Bhalla, T.; Shepherd, E.; Tobias, J.D. Neonatal pain management. Saudi J. Anaesth. 2014, 8 (Suppl. S1), S89–S97. [Google Scholar] [CrossRef]
- Hall, R.W.; Shbarou, R.M. Drugs of choice for sedation and analgesia in the neonatal ICU. Clin. Perinatol. 2009, 36, 215–226. [Google Scholar] [CrossRef]
- Gao, H.; Gao, H.; Xu, G.; Li, M.; Du, S.; Li, F.; Zhang, H.; Wang, D. Efficacy and safety of repeated oral sucrose for repeated procedural pain in neonates: A systematic review. Int. J. Nurs. Stud. 2016, 62, 118–125. [Google Scholar] [CrossRef]
- Qiu, J.; Jiang, Y.F.; Li, F.; Tong, Q.H.; Rong, H.; Cheng, R. Effect of combined music and touch intervention on pain response and β-endorphin and cortisol concentrations in late preterm infants. BMC Pediatr. 2017, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.C.; Caminha, M.F.; Coutinho, A.C.; Ventura, C.M. Pain in the neonatal unit: The knowledge, attitude and practice of the nursing team. Cogitare Enferm. 2016, 21, 1–10. [Google Scholar]
- Sposito, N.P.B.; Rossato, L.M.; Bueno, M.; Kimura, A.F.; Costa, T.; Guedes, D.M.B. Assessment and management of pain in newborns hospitalized in a neonatal intensive care unit: A cross-sectional study. Rev. Lat.-Am. Enferm. 2017, 25, e2931. [Google Scholar] [CrossRef]
- Cong, X.; Delaney, C.; Vazquez, V. Neonatal nurses’ perceptions of pain assessment and management in NICUs: A national survey. Adv. Neonatal Care 2013, 13, 353–360. [Google Scholar] [CrossRef]
- Cousins, M.; Lane-Krebs, K.; Matthews, J.; Johnston-Devin, C. Student nurses’ pain knowledge and attitudes towards pain management over the last 20 years: A systematic review. Nurse Educ. Today 2022, 108, 105169. [Google Scholar] [CrossRef]
- Grommi, S.; Vaajoki, A.; Voutilainen, A.; Kankkunen, P. Effect of pain education interventions on registered nurses’ pain management: A systematic review and meta-analysis. Pain Manag. Nurs. 2023, 24, 456–468. [Google Scholar] [CrossRef]
- McCabe, C.; Feeney, A.; Basa, M.; Eustace-Cook, J.; McCann, M. Nurses knowledge, attitudes and education needs towards acute pain management in hospital settings: A meta-analysis. J. Clin. Nurs. 2023, 32, 4325–4336. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L. Effect of educational interventions for improving the nurses’ knowledge, attitudes, and practice of paediatric pain management: A aystematic review and meta-analysis. Pain Manag. Nurs. 2024, 25, e271–e278. [Google Scholar] [CrossRef]
- Innab, A.; Alammar, K.; Alqahtani, N.; Aldawood, F.; Kerari, A.; Alenezi, A. The impact of a 12-hour educational program on nurses’ knowledge and attitudes regarding pain management: A quasi-experimental study. BMC Nurs. 2022, 21, 250. [Google Scholar] [CrossRef] [PubMed]
- Samulowitz, A.; Gremyr, I.; Eriksson, E.; Hensing, G. “Brave Men” and “Emotional Women”: A theory-guided literature review on gender bias in healthcare and gendered norms towards patients with chronic pain. Pain Res. Manag. 2018, 2018, 6358624. [Google Scholar] [CrossRef] [PubMed]
- International Association for the Study of Pain (IASP). IASP 2023 Global Year for Integrative Pain Care. 2024. Available online: https://www.iasp-pain.org/advocacy/global-year/integrative-pain-care/ (accessed on 23 May 2024).
- Osborne, N.R.; Davis, K.D. Sex and gender differences in pain. Int. Rev. Neurobiol. 2022, 164, 277–307. [Google Scholar] [CrossRef]
- Templeton, K.J. Sex and gender issues in pain management. J. Bone Jt. Surg. Am. 2020, 102 (Suppl. S1), 32–35. [Google Scholar] [CrossRef]
- Paller, C.J.; Campbell, C.M.; Edwards, R.R.; Dobs, A.S. Sex-based differences in pain perception and treatment. Pain Med. 2009, 10, 289–299. [Google Scholar] [CrossRef]
- Abraham, A.; Barnett, C.; Katzberg, H.D.; Lovblom, L.E.; Perkins, B.A.; Bril, V. Sex differences in neuropathic pain intensity in diabetes. J. Neurol. Sci. 2018, 388, 103–106. [Google Scholar] [CrossRef]
- Taves, S.; Berta, T.; Liu, D.L.; Gan, S.; Chen, G.; Kim, Y.H.; Ji, R.R. Spinal inhibition of p38 MAP kinase reduces inflammatory and neuropathic pain in male but not female mice: Sex-dependent microglial signaling in the spinal cord. Brain Behav. Immun. 2016, 55, 70–81. [Google Scholar] [CrossRef]
- Sorge, R.E.; Mapplebeck, J.C.; Rosen, S.; Beggs, S.; Taves, S.; Alexander, J.K.; Mogil, J.S. Different immune cells mediate mechanical pain hypersensitivity in male and female mice. Nat. Neurosci. 2015, 18, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- The Lancet. Managing pain effectively. Lancet 2011, 377, 2151. [Google Scholar] [CrossRef]
- Maher, C.; Gaffiero, D. Exploring the lived experiences of patients with fibromyalgia in the United Kingdom: A study of patient-general practitioner communication. Psychol. Health 2025, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Volpin, M.C.; Ferreira, E.L.; Eduardo, A.A.; Bombarda, T.B. Ensino sobre cuidados paliativos nos cursos da área de saúde: Apontamentos sobre lacunas e caminhos. Diálogos Interdisc. 2022, 11, 140–153. [Google Scholar]
- Powell, A.; Gaffiero, D. Between the Lines: An Interpretative Phenomenological Analysis Exploring Injury, Mental Health and Support in Professional and Semi-Professional Football in the United Kingdom. Cogent Psychol. 2025, 12, 2537216. [Google Scholar] [CrossRef]
- Organización Panamericana de la Salud (OPS). Aspectos Técnicos y Regulatorios Sobre el uso de Oxímetros de Pulso en el Monitoreo de Pacientes con COVID-19; OPS/HSS/MT/COVID-19/20-0029; 7 de Agosto de 2020. Available online: https://iris.paho.org/handle/10665.2/52551 (accessed on 15 January 2025).
- Evans, D.W.; De Nunzio, A.M. Controlled manual loading of body tissues: Towards the next generation of pressure algometer. Chiropract. Man. Ther. 2020, 28, 51. [Google Scholar] [CrossRef]
- Bedenik, G.; Graça, G.; Carvalho, E.; de Santana, J. Desenvolvimento de sistema de algometria de pressão. Oncology 2011, 23, 381–386. [Google Scholar]
- Jones, D.H.; Kilgour, R.D.; Comtois, A.S. Test–retest reliability of pressure pain threshold measurements of the upper limb and torso in young healthy women. J. Pain 2007, 8, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Buskila, D.; Neumann, L.; Zmora, E.; Feldman, M.; Bolotin, A.; Press, J. Pain sensitivity in prematurely born adolescents. Arch. Pediatr. Adolesc. Med. 2003, 157, 1079–1082. [Google Scholar] [CrossRef]
- Pardo, C.; Muñoz, T.; Chamorro, C. Monitorización del dolor: Recomendaciones del grupo de trabajo de analgesia y sedación de la SEMICYUC. Med. Intensiv. 2006, 30, 379–385. [Google Scholar] [CrossRef]
- van Ganzewinkel, C.-j.J.L.M.; Been, J.V.; Verbeek, I.; van der Loo, T.B.; van der Pal, S.M.; Kramer, B.W.; Andriessen, P. Pain threshold, tolerance and intensity in adolescents born very preterm or with low birth weight. Early Hum. Dev. 2017, 110, 31–38. [Google Scholar] [CrossRef]
- Watt-Watson, J.; Hogans, B. Current Status of Pain Education and Implementation Challenges. IASP. 2021. Available online: https://www.iasp-pain.org/resources/fact-sheets/current-status-of-pain-education-and-implementation-challenges/ (accessed on 18 December 2024).
- Watt-Watson, J.; Peter, E.; Clark, A.J.; Dewar, A.; Hadjistavropoulos, T.; Morley-Forster, P.; O’Leary, C.; Raman-Wilms, L.; Unruh, A.; Webber, K.; et al. The ethics of Canadian entry-to-practice pain competencies: How are we doing? Pain Res. Manag. 2013, 18, 25–33. [Google Scholar] [CrossRef]
- Watt-Watson, J.; Murinson, B. Current challenges in pain education. Pain Manag. 2013, 3, 351–357. [Google Scholar] [CrossRef]
- Rice, A.; Smith, B.; Blyth, F. Pain and the global burden of disease. Pain 2016, 157, 791–796. [Google Scholar] [CrossRef]
- Sedrez, E.S.; Monteiro, J.K. Pain assessment in pediatrics. Rev. Bras. Enferm. 2020, 73, e20190109. [Google Scholar] [CrossRef]
- Faccioli, S.C.; Tacla, M.T.G.M.; Rossetto, E.G.; Collet, N. The management of pediatric pain and the perception of the nursing team in light of the Social Communication Model of Pain. BrJP 2020, 3, 37–41. [Google Scholar] [CrossRef]
- World Health Organization. Basic Documents, 48th ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Olsson, M.; Currow, D.C.; Ekström, M.P. Exploring the most important factors related to self-perceived health among older men in Sweden: A cross-sectional study using machine learning. BMJ Open 2022, 12, e061242. [Google Scholar] [CrossRef] [PubMed]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Coelho, M.T.Á.D.; dos Santos, V.P.; do Carmo, M.B.B.; de Souza, A.C.; França, C.P.X. Relação entre a autopercepção do estado de saúde e a automedicação entre estudantes universitários. Rev. Psicol. Divers. Saúde 2017, 6, 5–13. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).