Abstract
Background/Objectives: Babywearing is a carrying system that ensures consistent contact and proper posture between the baby and carrying adult, in which there is no age or weight limit, and it is rarely inadvisable. Although babywearing has been growing in popularity and acclaim due to the comfort and emotional closeness between the carrier and baby, there are a number of physical and physiological consequences for the adult carrier when using an ergonomic babywearing device, such as muscular, postural, cardiorespiratory, and energy expenditure, and the perception of effort and pain. The objective is to explore the physical implications affecting the carrier, as well as the subjective perception of strain and pain. Methods: A systematic review was carried out including articles up to December 2023 in the Web of Science (WOS), Medline, and SportDiscus databases. Studies dealing with ergonomic babywearing and the physical implications of babywearing were included; systematic reviews or case studies were excluded. Results: After applying the inclusion and exclusion criteria, a total of 14 original articles were obtained for analysis. Methodological quality was rated using the Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies with scores between 3 and 8 points. All articles included valid and reliable information on exposure, outcome measures, and results. Conclusions: The studies reviewed cover different aspects, such as muscle activation and postural stability, as well as specific ergonomic design for particular groups. In general terms, it seems that the use of certain babywearing devices, especially back or front carry, seems to be the one that generates fewer physiological alterations in the carriers compared to carrying babies in arms or other positions.
1. Introduction
The use of babywearing devices is spreading in the population, so much so that it has gained popularity and has experienced a remarkable increase in recent years, being a beneficial practice due to the constant contact between the baby and carrying adult [1]. Furthermore, appropriate babywearing has the potential to consistently support infants’ spines [2]. This carrying practice involves carrying the baby in an ergonomically designed baby carrier, in which the baby’s weight is evenly distributed. Although babywearing has been growing in popularity and praise due to the comfort and emotional closeness between the carrier and baby, there are still some precise questions and doubts about the physical and physiological implications for both the baby and adult. Furthermore, there are certain aspects that pediatricians and health professionals should inform in a correct manner and encourage good practice, as it is often not known what the appropriate devices are, whether it is conducted safely or not, and what the benefits are [3].
Babywearing can also involve differentiated strain between different types and methods of carrying. In the study by Fista et al. [4], subjective strain perception was measured using the BORG scale, in which the babywearer used three different types of baby carriers (a soft structured carrier, a ring sling, and a traditional shawl). The data indicated that the mechanism that caused the most strain was the baby carrier with a ring on the left shoulder because the sling rings made of metal put pressure on the left shoulder. In addition, they found that it also affected other areas such as the neck, back, and trunk.
The physical load is an important consideration to take into account, as it generates different muscle activations in the babywearer. Certain baby carriers generate less activation in the spinal muscles compared to other situations and therefore generate less injurious strains [5]. Yuk et al. [6], using electromyography (EMG), observed that different muscle patterns are activated depending on the method of carrying.
Just as there are muscle specificities of different physical activities, the practice of babywearing affects the adult’s posture and gait. According to Azaman et al. [7], the pelvis, head, and shoulder are affected by carrying. In addition, carrying in the arms increases the load-bearing knee abduction moment by 8.7% and the load-bearing knee extension moment by 16.7% [8].
Also, the technique and duration of carrying and the physical characteristics of the carrying adult can alter cardiorespiratory aspects, and the energy expenditure related to ergonomic carrying can affect endurance and the ability to perform other physical tasks during the day. There are differences in energy costs [9] and perceived effort [10] between carrying a baby in the arms versus carrying a baby in a carry system.
Furthermore, the occurrence of pain is an important issue to consider when deciding whether to babywear or not. In the study by Mannen et al. [11], pain perception was analyzed using the Visual Analogue Scale. The results indicated that carrying adults experience more pain when carrying babies than when babywearing devices are used. This seemed to be due to the fact that when babies are carried, the body is in an asymmetrical position, and there are more areas of swaying.
It is important to assess the impact of babywearing in order to take appropriate measures to improve physical fitness. The design of baby carriers and their technique of use should be studied to minimize the risk of injury due to poor posture or increased muscle fatigue from prolonged carrying.
From the above, it appears that babywearing offers numerous benefits to ensure a comfortable and safe experience for the adult and baby, but it also has physical implications that affect the babywearer, and knowing the alterations produced by this practice of carrying and care, it will be possible to design exercise programs adapted to these populations, focused on preventing injuries or improving the experience.
It is important to better understand the physical implications for the adult using babywearing devices in order to generate exercise programs that prevent possible alterations or injuries. In addition, it seems relevant to provide information to parents, carrying adults, health professionals, and product designers in order to promote safe and healthy babywearing practices that benefit both the baby and the carrying adult.
Therefore, the aim of this paper is to explore the physical implications affecting the babywearer, focusing on physical and physiological aspects such as muscle activity, posture, and gait, and cardiorespiratory and energetic factors, as well as subjective perception of effort and pain.
2. Materials and Methods
2.1. Databases and Searches
This systematic review aimed to answer the following: What are the effects of different babywearing methods on (a) muscle activation, (b) postural stability, (c) energy expenditure, and (d) subjective pain and fatigue in healthy adults?
The PRISMA 2020 statement (Preferred Reporting Items for Systematic reviews and MetaAnalyses) [12] was followed for the search of the articles included in this review. This review protocol was developed prior to data extraction and is publicly available at OSF: https://osf.io/qjp4r/ (accessed on 29 December 2023). The search was conducted in the following databases: Web of Science (WOS), Medline, and SportDiscus, including results up to December 2023.
The following PICO(S) strategy was followed: Patient (babywearers); intervention (physical and physiological implications); comparison (other carrying methods); outcome (effects of babywearing).
The search strategy was applied independently in each database following the particularities of each one. The Medical Subject Heading (MESH) terms used in the search were “Physical fitness” [Mesh], “Postural Balance” [Mesh] and “Biomechanical phenomena” [Mesh]. In addition, the keywords used to identify articles on the subject of this review were ‘baby carrier’, ‘ergonomic carrier’, ‘babywearing’, ‘baby carrying’, combined with ‘electromyography’, ‘muscle activity’, ‘postural stability’, ‘body balance’, ‘ergonomic’, ‘center of pressure’, ‘physical condition’, and ‘posture’. The Boolean operators OR and AND were used to link the terms and establish the search equations (Table 1).

Table 1.
Search equations from different databases.
All studies were assessed independently by two reviewers. Each reviewer screened titles and abstracts to obtain relevant full articles which were assessed against the inclusion and exclusion criteria described. In case of a lack of consensus, the judgment of a third reviewer prevailed.
2.2. Selection of Studies and Selection Criteria
For the selection of articles, studies dealing with babywearing and the physical implications of babywearing were set as inclusion criteria. Exclusion criteria were systematic reviews or case studies (Table 2).
Table 2.
Inclusion and exclusion criteria.
The search identified 223 articles in the three databases, of which 9 were eliminated as duplicates. Of the 17 full-text articles assessed, 10 were excluded due to the fact that they were case studies, reviews, or articles that did not address the topic, resulting in 7 studies from the database search. Notably, 7 additional studies were identified through citation searching, yielding a total of 14 studies for inclusion. The entire process detailing the study selection steps can be found in the PRISMA flowchart (Figure 1).
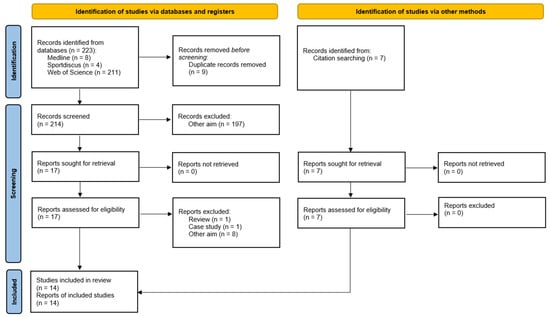
Figure 1.
PRISMA flowchart of the item selection process.
2.3. Variables
This research includes data on the effects of babywearing on the babywearer’s body, including variables such as muscle activation, load distribution and pressure, skin temperature, heart rate, stability, posture, balance, pain, gait kinematics, volumes, and respiratory rate, among others. For the interpretation of the results, results with statistical significance were compared. When studies use different units of measurement, results shall be standardized as far as possible. In addition, if the results provided are by subgroups, these shall be taken into account in the analysis.
2.4. Assessment of Methodological Quality and Risk of Bias of Individual Studies
The Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies (JBI) scale for analytical cross-sectional studies was used for the analysis of methodological quality [13].
The JBI scale uses eight criteria to assess the overall methodological quality of a study. Criteria for inclusion: sample inclusion criteria; description of subjects and settings; valid and reliable exposure measure; objective and standard measure of condition; identification of confounders; strategies to address confounders; valid and reliable outcome measure; and adequate statistical analysis. The final score ranges from 0 to 8 points. There is no ranking criterion for study quality. For ease of interpretation, we classified the methodological quality score, regardless of the scale used, as low (0–3 points), medium (4–6 points), and high (>6 points), as was conducted in a previous study [14].
3. Results
Methodological quality analysis yielded scores ranging from 3 to 8 points. One article scored low [15], nine scored medium [4,5,6,7,8,9,16,17,18], and four scored high [11,19,20,21] (Table 3). All studies met criteria 3 (exposure was measured in a valid and reliable manner), 4 (objective and standardized criteria were used to measure the condition), and 7 (outcomes were measured in a valid and reliable manner).
Table 3.
Methodological quality scores of the “Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies”.
Table 4 showed the different types of carrying evaluated in each of the studies, while Table 5 summarized the main results and research characteristics of the studies included in this review, grouped by the different variables studied. We found that variables such as muscle activation have been evaluated in four studies [5,6,18,21]. Posture or stability has been investigated in six of the studies [4,7,8,9,15,17], while foot pressure or center of pressure has been investigated in five [6,7,11,18,19]. Physiological variables such as heart rate, skin temperature, or respiratory values have been evaluated in four of the studies [4,16,20,21].
Table 4.
Types of carrying evaluated in each of the included studies.
Table 5.
Summary of studies included in the review.
4. Discussion
This paper has analyzed the physical and physiological consequences of babywearing on the babywearer. To the authors’ knowledge, this is the first systematic review on this topic. The results analyzed in this review come from articles with acceptable methodological quality, with only one article rated with a low score on the JBI scale.
When interpreting the different results obtained in the studies, methodological differences have been observed, such as the use of dummies versus babies, the different walking or standing protocols used, as well as the different designs of carrying systems used, among others. Such heterogeneity in the studies has made direct comparability between them difficult.
4.1. Muscle Activity
Different types of baby carriers affect the muscle activation of the babywearer and in this case, EMG is a widely used tool. In the study by Fagundes et al. [5], an electromyographic analysis of the spinal muscles was performed during walking and with different baby carriers. In terms of the results, baby carriers that do not distribute the weight evenly generate more activation of the spinal muscles. In contrast, the kangaroo method activates these muscles the least compared to other situations. In the study by Yuk et al. [6], they also used EMG to study the activation of trunk and lower limb muscles such as the biceps femoris. Their results show that front babywearing (LBC-F) generates greater activation in all the muscles analyzed than back babywearing (LBC-B), which could result in greater muscle fatigue and injury with prolonged use. On the other hand, in a high-quality study [21], the activation of the upper trapezius was greater when carrying a two-part front-facing backpack than with a front-facing backpack with shoulder straps. In addition, upper trapezius and erector spinae activation was statistically significantly higher in males and also in heavier babies, while rectus abdominis activation was higher in females. Based on this, an ergonomic design that minimizes muscle loading and favors adequate weight distribution of the baby is important.
4.2. Posture and Gait
The use of baby carriers has a significant impact on the babywearer’s posture and gait. Azaman et al. [7] found that baby carriers can alter the wearer’s posture, increasing postural sway. Thus, according to the results analyzed, the pelvis, head, and trunk are affected by the load. Another curious fact is that carrying a baby carrier in the front produces less anteroposterior deviation of the joints than back or side baby carriers.
Along the same lines, Havens et al. [17] analyze how different methods of carrying the baby affect the carrier’s posture during walking and picking up objects. Thus, carrying the baby with unequal weight and asymmetrical posture results in back extension, which affects the efficiency of movement. In terms of retrieval, most individuals performed the squat technique to retrieve the object from the floor, both while carrying it and with it in their arms.
And for its relationship with lower and upper limbs, the study by Williams et al. [8] also examines the babywearer’s posture using different infant carrier methods, and the resulting data are similar to the previous study in that carrying in arms increases the carrying knee abduction moment by 8.7% and the carrying knee extension moment by 16.7%. Hyun and Ryew [19] studied the effects of carrying an infant using a rear carrier during high-heeled walking in high-quality research. After analyzing the 1st and 2nd peak vertical force (PVF), there are statistically significant differences according to the use of high heels and walking conditions. On the other hand, medial-lateral center of pressure (COP) and leg stiffness showed statistically significant differences according to heel height and walking conditions. This finding is particularly relevant for babywearers performing activities where posture and stability are crucial, such as walking on inclined or uneven surfaces.
4.3. Load
Another factor to consider is the weight of the baby. Chen et al. [16] investigated the maximum acceptable load during babywearing, finding that men carried more weight than women, that more weight could be carried in 1 h than in 4 h, that when back babywearing, the acceptable weight was greater than when front carrying, and that backpacks with shoulder straps carried more weight than two-part backpacks. These data will be important for babywearers to consider, as depending on the weight of the baby, the choice of both baby carrier and carrying position may vary. In addition, the length of use should also be considered, as excessive use can be harmful even with regard to the recommended weight for each device.
4.4. Cardiorespiratory Effects
The impact of baby carrier use on cardiorespiratory response and energy expenditure is another important determinant to consider. When assessing heart rate (HR), Wu et al. [21] found, in their high-quality study, that HR was statistically higher in women, and that the weight of the baby also affected exercise intensity, as it was higher when carrying a 10 kg baby than a 7 kg baby. Chen et al. [16] also assessed HR, finding that the percentage of maximum heart rate (%HR) was higher when carrying for 1 h than for 4 h. A study evaluating the relationship between the HR of babywearers and babies during babywearing also found that babywearing increases the babywearer’s HR, but the baby’s HR decreases, especially when the mother is carrying the baby [22].
In the high-quality study by Ohashi et al. [20], the respiratory response during downhill walking was analyzed by front and back carrying with baby carriers, and in both situations, the respiratory effort increased significantly. This effort is accompanied by higher energy expenditure, which leads to lower locomotion efficiency and greater fatigue during prolonged use. From a different perspective, the study by Wall-Scheffler et al. [9] analyzed the effects on the musculoskeletal system of carrying a baby using different carrying mechanisms. The results indicated that there is an average increase in the perceived physical effort when carrying a baby in arms compared to carrying a baby in a sling (16%, ranging from a 13% to a 25% increase). In addition, standardized stride lengths are shorter during carriage in arms than when using a front carrier. Following these explorations, it is of vital importance to design babywearing devices that promote ergonomic posture, reduce energy expenditure, and improve movement efficiency.
4.5. Fatigue and Pain
To assess comfort and fatigue during babywearing, perceived exertion can help us, even though it is a subjective measure. In the study by Chen et al. [16], front carrying had a higher value in perceived exertion compared to back carrying, both in the lower back and abdomen, as measured by the Borg CR-10 scale. Fista et al. [4] used a physiological and biomechanical approach to evaluate different methods of use (Soft Structured Carrier (SSC) harness, Jarik, and ring sling) of baby carriers. The data indicated that the mechanism that caused the most strain was the ring sling and the Jarik, especially on the left shoulder. The SSC-type harness provided the best change of posture and the highest level of confidence. Similarly, Lee and Hong [18] measured muscle fatigue and COP in different types of baby carriers. They found that designs that allow a more natural posture and distribute weight evenly reduce muscle fatigue. This reduction in muscle fatigue translates into less perceived strain on the part of the carrier, which is crucial for carrier acceptance and prolonged use, since the time spent carrying babies is considerable [23].
As with the previous variable, pain perception is also important to take into account when carrying and is a good indicator of whether the ergonomic design is adequate or not. To this end, the study by Mannen et al. [11], considered to be of good quality, investigated how different methods of carrying the baby (unloaded, carrying a dummy in arms, carrying a dummy) affect postural sway and pain during prolonged standing. The results indicated that 30% of the participants reported pain during unloading and carrying, while 50% reported pain during carrying. Participants shifted their weight more frequently as they spent more time in an asymmetrical position and had greater areas of swinging in weight bearing and therefore increased the perception of pain, especially in the lumbar region. In relation to the previous article and the pain that can be suffered in the back while carrying, one study [15], which had moderate methodological quality, suggested the need to design baby carriers that provide good lumbar support and distribute the weight in a balanced way, especially for older people, as this can reduce pain in the back and joints. Another factor pointed out by these authors is the posture of the shoulders and hips while using the baby carrier by the users.
4.6. Limitations, Future Lines of Research, and Practical Implications
In terms of limitations, while the chosen databases are major sources, a broader search might have captured additional relevant literature. The review includes studies with different experimental designs and measurement methods, which may limit the comparability of results. On the other hand, most of the studies focus on young and middle-aged adults, and most of them are conducted only on women, which makes it difficult to extrapolate results to the male or older population; however, the profile found in the studies corresponds to the population that tends to use these parenting aids the most. Furthermore, the interpretation of some of the variables studied, such as heart rate or muscle activation, may imply a difference in results depending on the characteristics of the wearer, including age, sex, and anthropometry. A number of studies are conducted in controlled settings and with dummies simulating babies rather than real children, which may not reflect the conditions of real, everyday use.
In terms of future lines of research, the long-term effects of baby carrier use on the health of the carriers in real, everyday conditions could be investigated, as well as extending studies to broader groups such as older people, individuals with disabilities, or different ethnicities. In addition, research can be conducted on the incorporation of new smart technologies in baby carrier design.
Furthermore, this information can serve as a basis for designers to improve the design of baby carriers, making them more ergonomic and adaptable to different carriers. As for health professionals, they should use this information to educate users about the best types of baby carriers and the importance of good posture. In addition, these experts should apply the knowledge to develop specific exercise and stretching programs for babywearers. As for parents, understanding the effects of different types of baby carriers helps them choose which one to use, given the wide variety available on the market.
5. Conclusions
The analysis carried out on the existing literature on the use of baby carriers and their relationship to carrier ergonomics reveals a number of important findings that should be considered by both health professionals and baby carrier designers. The studies under analysis cover different aspects, such as muscle activation and postural stability, as well as specific ergonomic design for particular groups. The synthesized evidence suggests that back carriers seem to be the least likely to cause physiological alterations in babywearers compared to babywearing babies in arms or other positions.
On the one hand, it has been shown that different ways of carrying the baby (front, back, or in arms) affect the electromyographic activity of the spinal muscles, and, in terms of muscle fatigue, it is essential that baby carriers minimize excessive activation of the trunk and lower limb muscles to reduce muscle fatigue and the risk of injury, as this can have a considerable impact on the user’s musculoskeletal health in the long term, with kangaroo or back carry mode being found to generate the least activation.
On the other hand, depending on the type of baby carrier, these can influence the wearer’s posture and gait, so a design that favors even weight distribution and supports a natural posture is crucial to maintain stability and gait efficiency.
Infant carrying methods also affect breathing and energy expenditure compared to carrying the baby in your arms, so the design should be optimized to reduce respiratory and energy expenditure, which can significantly improve the comfort and prolonged wearability of the baby carrier. Therefore, in addition to design factors and carrying modalities that minimize injury and improve the posture and stability of the carrier, intervention through physical exercise is important to reduce and prevent physical problems that may affect the carriers. It is also important to take into account the duration of use due to the load being carried, trying not to exceed the time limit, and taking breaks whenever possible to avoid injuries due to overexertion.
Author Contributions
Conceptualization, Y.T.-I.; methodology, Y.T.-I. and A.D.-E.; investigation, C.R.-G. and Á.G.-S.; resources, A.D.-E.; writing—original draft preparation, Y.T.-I. and A.D.-E.; writing—review and editing, Y.T.-I., C.R.-G., and Á.G.-S.; visualization, C.R.-G. and Á.G.-S.; supervision, Y.T.-I.; project administration, Y.T.-I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| EMG | Electromyography |
| PRISMA | Preferred Reporting Items for Systematic reviews and MetaAnalyses |
| WOS | Web of Science |
| PICO | Patient, Intervention, Comparison, Outcome |
| MESH | Medical Subject Heading |
| JBI | Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies |
| LBC-B | Loaded with baby carrier on the back |
| LBC-F | Loaded with baby carrier in front |
| PVF | Peak Vertical Force |
| COP | Center of pressure |
| HR | Heart Rate |
| SSC | Soft Structured Carrier |
References
- Williams, L.R.; Grisham, L.M.; Gebler-Wolfe, M.; Kelsch, K.; Bedrick, A.; Bader, M.Y. Nurse Perceptions of Babywearing for Neonates with Neonatal Abstinence Syndrome in the Neonatal Intensive Care Unit. Adv. Neonatal. Care. 2021, 21, 23–31. [Google Scholar] [CrossRef]
- Siddicky, S.F.; Bumpass, D.B.; Krishnan, A.; Tackett, S.A.; McCarthy, R.E.; Mannen, E.M. Positioning and baby devices impact infant spinal muscle activity. J. Biomech. 2020, 104, 109741. [Google Scholar] [CrossRef]
- López Acuña, E.S.; Salmerón Ruiz, M.A. El porteo ergonómico; Ergonomic babywearing. Pediatr. Integral. 2014, XVIII, 774–780. (In Spanish) [Google Scholar]
- Fista, B.; Widyanti, A.; Muslim, K.; Salma, S.A. Evaluation of Baby Carriers in Indonesia: Physiological and Biomechanical Approach. IOP Conf. Ser. Mater. Sci. Eng. 2019, 598, 012113. [Google Scholar] [CrossRef]
- Fagundes, F.; Teixeira, F.; Camargo, L.; Mochizuki, L.; Amorim, C.; Soares, R. Análise eletromiográfica de músculos da coluna vertebral durante a marcha em diferentes formas de carregar o bebê; Electromyographic analysis of the spinal muscles during the gait in different ways to carry a baby. Conscientiae Saúde 2016, 15, 210–216. Available online: http://www.redalyc.org/articulo.oa?id=92949791005 (accessed on 29 December 2023). [CrossRef][Green Version]
- Yuk, G.C.; Park, R.J.; Lee, H.Y.; Lee, M.H.; Lee, J.H.; Kuk, J.S.; Jang, J.-S. The Effects of Baby Carrier and Sling in Muscle Activation of Trunk, Low Extremity and Foot Pressure. J. Korean Soc. Phys. Med. 2010, 5, 223–317. [Google Scholar][Green Version]
- Azaman, A.; Isa, N.M.; Dzahir, M.; Xiang, K.K. Effects of baby carrier on wearer’s posture stability. J. Mech. Eng. 2017, SI 4, 107–118. Available online: https://ir.uitm.edu.my/id/eprint/39240 (accessed on 29 December 2023).[Green Version]
- Williams, L.; Standifird, T.; Madsen, M. Effects of infant transportation on lower extremity joint moments: Baby carrier versus carrying in-arms. Gait Posture 2019, 70, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Wall-Scheffler, C.; Geiger, K.; Steudel-Numbers, K. Infant carrying: The role of increased locomotory costs in early tool development. Am. J. Phys. Anthropol. 2007, 133, 841–846. [Google Scholar] [CrossRef]
- Ojukwu, C.P.; Okafor, C.J.; Chukwu, S.C.; Anekwu, E.M.; Okemuo, A.J. Evaluation of selected cardiopulmonary and perceived exertion responses to four infant carrying methods utilised by African Mothers. J. Obstet Gynaecol. 2019, 39, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Mannen, E.; Havens, K.; Kahney, A.; Nelson-Wong, E. Baby-Carrying Method Impacts Caregiver Postural Sway and Pain During Prolonged Standing. J. Womens Health 2020, 44, 47–53. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Checklist for Analytical Cross Sectional Studies Critical Appraisal. 2020. Available online: https://jbi.global/sites/default/files/2020-08/Checklist_for_Analytical_Cross_Sectional_Studies.pdf (accessed on 27 July 2022).
- Leno-Durán, E.; Micha-Mabale, M.; García-Pérez, M.; Bueno-Cavanillas, A.; Barrios-Rodríguez, R.; Requena, P. Influencia de la dieta en el riesgo de infección y de gravedad de la COVID-19: Una revisión sistemática; Influence of diet in COVID-19 infection and severity risk: A systematic review. Nutr. Hosp. 2023, 40, 444–456. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Atthawuttikul, A.; Khongkharat, S. Factors in Ergonomic Design of 6-to-18-month Baby Carriers for Elderly People. Pertanika J. Sci. 2021, 29, 1097–1108. [Google Scholar] [CrossRef]
- Chen, T.H.; Kao, Y.Y.; Wang, M.J.J. The Psychophysical Evaluations of Baby Carriers. In Advances in Physical Ergonomics & Human Factors; Goonetilleke, R.S., Karwowski, W., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 234–241. [Google Scholar]
- Havens, K.L.; Severin, A.C.; Bumpass, D.B.; Mannen, E.M. Infant carrying method impacts caregiver posture and loading during gait and item retrieval. Gait Posture 2020, 80, 117–123. [Google Scholar] [CrossRef]
- Lee, H.; Hong, K. Type and wearing method-dependent COP and muscle fatigue measurement of baby carriers for the development of smart baby carriers. Int. J. Cloth. Sci. Technol. 2018, 30, 610–627. [Google Scholar] [CrossRef]
- Hyun, S.H.; Ryew, C.C. Effect of lower limb kinetic on carrying infant by hip seat carrier during high heel gait. J. Exerc. Rehabil. 2018, 14, 1092–1095. [Google Scholar] [CrossRef]
- Ohashi, K.; Ono, K.; Kawate, Y.; Watase, R.; Ishikawa, A. Respiratory response during upslope walking with different ways to carry a baby using baby carrier. Jpn. J. Phys. Fit. Sports Med. 2018, 67, 303–309. (In Japanese) [Google Scholar] [CrossRef]
- Wu, C.Y.; Huang, H.R.; Wang, M.J. Baby carriers: A comparison of traditional sling and front-worn, rear-facing harness carriers. Ergonomics 2017, 60, 111–117. [Google Scholar] [CrossRef]
- Han, J.H.; Rankin, L.; Lee, H.; Feng, D.; Grisham, L.M.; Benfield, R. Infant and parent heart rates during a babywearing procedure: Evidence for autonomic coregulation. Infant Behav. Dev. 2024, 77, 101996. [Google Scholar] [CrossRef]
- Nadeem, A.; Faisal, S.; Waqas, S. Association Between Infant Carrying Methods, Duration, And Trunk Position Among Nursing Mothers of Lahore. J. Riphah. Coll. Rehabili. Sci. 2024, 12, 213–218. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).