
Public Awareness and Perceptions of Longevity Determinants in Saudi Arabia: A Cross-Sectional Study (2024–2025)
 ,
, 
Abstract
1. Introduction
2. Method
2.1. Study Design
2.2. Sample Size
2.3. Questionnaire and Data Collection
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Passarino, G.; De Rango, F.; Montesanto, A. Human longevity: Genetics or Lifestyle? It takes two to tango. Immun. Ageing 2016, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Govindaraju, D.; Atzmon, G.; Barzilai, N. Genetics, lifestyle and longevity: Lessons from centenarians. Appl. Transl. Genom. 2015, 4, 23. [Google Scholar] [CrossRef]
- Fries, J.F. Frailty, heart disease, and stroke: The compression of morbidity paradigm. Am. J. Prev. Med. 2005, 29 (Suppl. S1), 164–168. [Google Scholar] [CrossRef]
- Wang, H.; Abbas, K.M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; Abolhassani, H.; Abreu, L.G.; Abrigo, M.R.; et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: A comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1160–1203. [Google Scholar] [CrossRef]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The Hallmarks of Aging. Cell 2013, 153, 1194. [Google Scholar] [CrossRef]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Li, Y.; Pan, A.; Wang, D.D.; Liu, X.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; et al. Impact of healthy lifestyle factors on life expectancies in the us population. Circulation 2018, 138, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-analytic Review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef] [PubMed]
- Apte, J.S.; Brauer, M.; Cohen, A.J.; Ezzati, M.; Pope, C.A. Ambient PM2.5 Reduces Global and Regional Life Expectancy. Environ. Sci. Technol. Lett. 2018, 5, 546–551. [Google Scholar] [CrossRef]
- WHO. Saudi Arabia. 2025. Available online: https://data.who.int/countries/682 (accessed on 21 April 2025).
- Khan, M.; Al Saud, H.; Sierra, F.; Perez, V.; Greene, W.; Al Asiry, S.; Pathai, S.; Torres, M. Global Healthspan Summit 2023: Closing the gap between healthspan and lifespan. Nat. Aging 2024, 4, 445–448. [Google Scholar] [CrossRef]
- Suarez-Lledo, V.; Alvarez-Galvez, J. Prevalence of Health Misinformation on Social Media: Systematic Review. J. Med. Internet. Res. 2021, 23, e17187. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Rimer, B.K.; Viswanath, K. (Eds.) Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass/Wiley: San Francisco, CA, USA, 2008. [Google Scholar]
- General Authority for Statistics. Available online: https://www.stats.gov.sa/en/home (accessed on 21 April 2025).
- Chesser, A.K.; Keene Woods, N.; Smothers, K.; Rogers, N. Health Literacy and Older Adults: A Systematic Review. Gerontol. Geriatr. Med. 2016, 2, 2333721416630492. [Google Scholar] [CrossRef]
- Rippe, J.M. Lifestyle Medicine: The Health Promoting Power of Daily Habits and Practices. Am. J. Lifestyle Med. 2018, 12, 499. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Niechcial, M.A.; Vaportzis, E.; Gow, A.J. Genes Versus Lifestyles: Exploring Beliefs About the Determinants of Cognitive Ageing. Front. Psychol. 2022, 13, 838323. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Barbagallo, M. The link between spirituality and longevity. Aging Clin. Exp. Res. 2024, 36, 32. [Google Scholar] [CrossRef]
- Goodyear, V.A.; Armour, K.M.; Wood, H. Young people and their engagement with health-related social media: New perspectives. Sport Educ. Soc. 2018, 24, 673. [Google Scholar] [CrossRef]
- Wen, M.; Gu, D. Air Pollution Shortens Life Expectancy and Health Expectancy for Older Adults: The Case of China. J. Gerontol. Ser A 2012, 67, 1219–1229. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.C.; Boen, C.; Gerken, K.; Li, T.; Schorpp, K.; Harris, K.M. Social relationships and physiological determinants of longevity across the human life span. Proc. Natl. Acad. Sci. USA 2016, 113, 578–583. [Google Scholar] [CrossRef]
- Abu-Ras, W.; Aboul-Enein, B.H.; Almoayad, F.; Benajiba, N.; Dodge, E. Mosques and Public Health Promotion: A Scoping Review of Faith-Driven Health Interventions. Health Educ. Behav. 2024, 51, 677–690. [Google Scholar] [CrossRef]
- Khubchandani, J.; Batra, K. Diet fads and supplements: Navigating the allure, risks, and reality. J. Med. Surg. Public Health 2024, 4, 100168. [Google Scholar] [CrossRef]
- Diekman, C.; Ryan, C.D.; Oliver, T.L. Misinformation and Disinformation in Food Science and Nutrition: Impact on Practice. J. Nutr. 2023, 153, 3–9. [Google Scholar] [CrossRef] [PubMed]
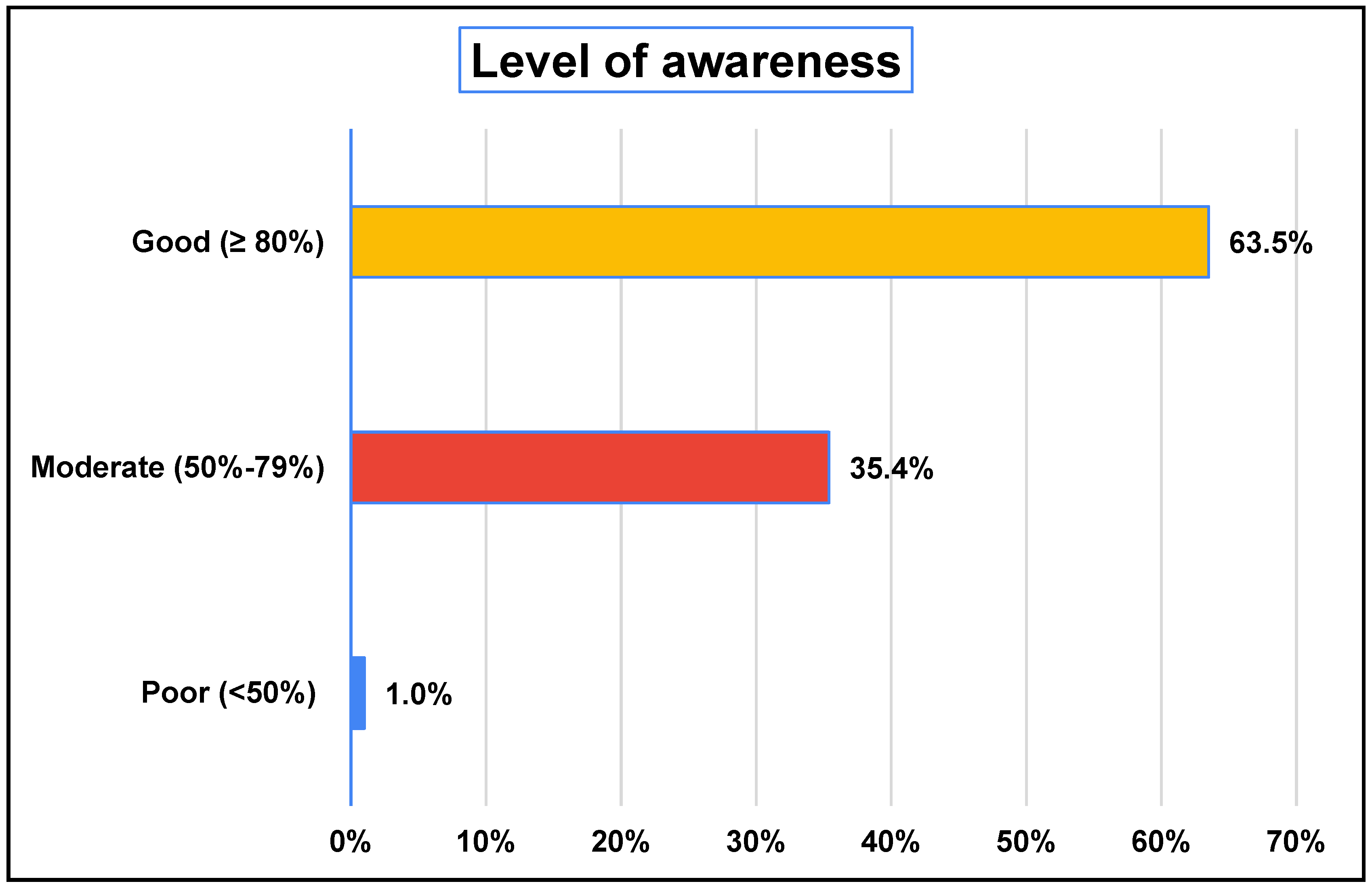

{kind=link}
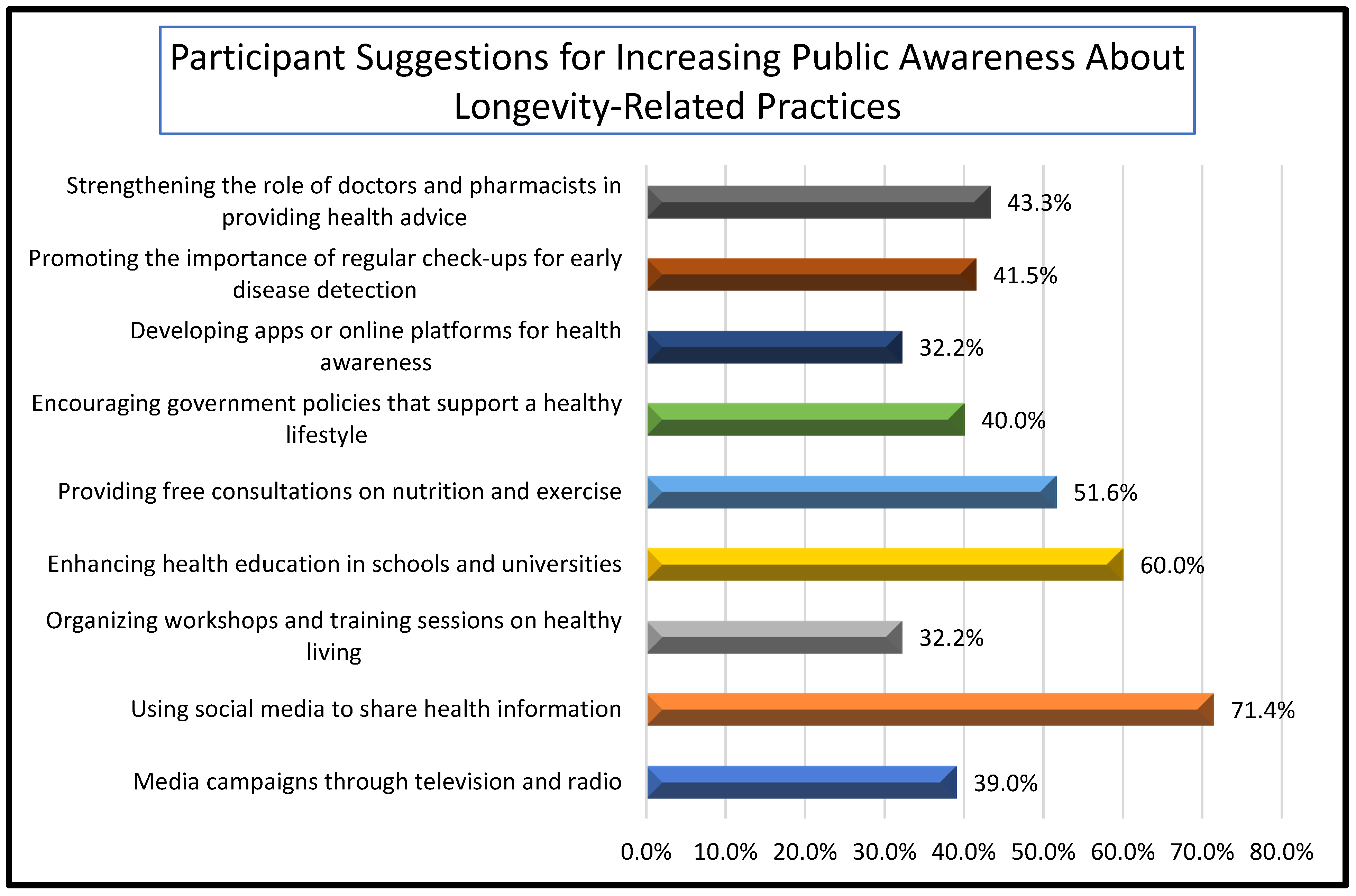
{kind=link}
| Survey Items | Studied Participants (N = 395) | ||
|---|---|---|---|
| n | % | ||
| Age | 18–25 years | 203 | 51.4% |
| 26–35 years | 57 | 14.4% | |
| 36–45 years | 56 | 14.2% | |
| 46–55 years | 52 | 13.2% | |
| >56 years | 27 | 6.8% | |
| Gender | Female | 268 | 67.8% |
| Male | 127 | 32.2% | |
| Nationality | Saudi | 382 | 96.7% |
| Non-Saudi | 13 | 3.3% | |
| Region | Central Province | 45 | 11.4% |
| Eastern Province | 25 | 6.3% | |
| Northern Province | 18 | 4.6% | |
| Southern Province | 38 | 9.6% | |
| Western Province | 267 | 67.6% | |
| Makkah Province | 2 | 0.5% | |
| Marital Status | Divorced | 13 | 3.3% |
| Married | 152 | 38.5% | |
| Single | 227 | 57.5% | |
| Widowed | 3 | 0.8% | |
| Educational Level | Primary | 3 | 0.8% |
| Intermediate | 7 | 1.8% | |
| Secondary | 69 | 17.5% | |
| Bachelor’s | 279 | 70.6% | |
| Diploma | 10 | 2.5% | |
| Master’s | 22 | 5.6% | |
| Doctorate | 5 | 1.3% | |
| Employment Status | Employed | 138 | 34.9% |
| Unemployed | 54 | 13.7% | |
| Business Owner | 15 | 3.8% | |
| Student | 163 | 41.3% | |
| Retired | 25 | 6.3% | |
| Monthly Household Income | USD 4000–8000 | 81 | 20.5% |
| USD 8000–13,300 | 19 | 4.8% | |
| USD 1600–4000 | 161 | 40.8% | |
| Less than ~USD 1600 | 126 | 31.9% | |
| More than USD 13,300 | 8 | 2.0% | |
| Perceived Urban Classification of Current Residence | Yes | 334 | 84.6% |
| Survey Items | Study Participants (N = 395) | ||
|---|---|---|---|
| n | % | ||
| Awareness of medical advancements related to longevity | No | 190 | 48.1% |
| Yes | 205 | 51.9% | |
| Primary source of information on longevity-related medical advancements * | Healthcare practitioners | 79 | 20.0% |
| Traditional media (TV, newspapers) | 83 | 21.0% | |
| Social media | 152 | 38.5% | |
| Family or friends | 50 | 12.7% | |
| Other: University | 5 | 1.3% | |
| Not previously aware of longevity-related medical advancements. | 174 | 44.1% | |
| Awareness of the impact of environmental factors (e.g., pollution, climate change) on longevity | No | 110 | 27.8% |
| Yes | 285 | 72.2% | |
| Level of understanding of how social factors (e.g., support networks) influence longevity | Moderate understanding | 182 | 46.1% |
| High understanding | 159 | 40.3% | |
| Unaware | 54 | 13.7% | |
| Perception of the role of regular physical activity in promoting longevity | Strongly agree | 237 | 60.0% |
| Agree | 127 | 32.2% | |
| Neutral | 24 | 6.1% | |
| Disagree | 6 | 1.5% | |
| Strongly disagree | 1 | 0.3% | |
| Level of interest in learning about longevity-promoting practices | Not interested | 85 | 21.5% |
| Interested | 182 | 46.1% | |
| Very interested | 128 | 32.4% | |
| Awareness of the role of adequate sleep in promoting health and longevity | No | 45 | 11.4% |
| Yes | 350 | 88.6% | |
| Perception of technology (e.g., health apps) in supporting longevity and health | Strongly agree | 92 | 23.3% |
| Agree | 145 | 36.7% | |
| Neutral | 121 | 30.6% | |
| Disagree | 29 | 7.3% | |
| Strongly disagree | 8 | 2.0% | |
| Survey Items | Study Participants (N = 395) | |
|---|---|---|
| n | % | |
| Perception that religious practices (e.g., prayer, fasting) contribute to health and longevity | ||
| Strongly agree | 297 | 75.2% |
| Agree | 68 | 17.2% |
| Neutral | 22 | 5.6% |
| Disagree | 7 | 1.8% |
| Strongly disagree | 1 | 0.3% |
| Frequency of engagement in religious practices that support mental and physical health | ||
| Daily | 332 | 84.1% |
| Weekly | 22 | 5.6% |
| Sometimes | 30 | 7.6% |
| Rarely | 6 | 1.5% |
| Never | 5 | 1.3% |
| Belief that local culture promotes healthy lifestyles linked to longevity | ||
| No | 187 | 47.3% |
| Yes | 208 | 52.7% |
| Perception that incorporating religious elements into public health campaigns enhances effectiveness | ||
| Strongly agree | 225 | 57.0% |
| Agree | 122 | 30.9% |
| Neutral | 38 | 9.6% |
| Disagree | 6 | 1.5% |
| Strongly disagree | 4 | 1.0% |
| Survey Item | Study Participants (N = 395) | |
|---|---|---|
| n | % | |
| Willingness to change lifestyle (e.g., diet, exercise) to improve health and longevity | ||
| Not willing | 18 | 4.6% |
| Somewhat willing | 162 | 41.0% |
| Very willing | 215 | 54.4% |
| Use of dietary supplements or herbs believed to improve overall health | ||
| No | 161 | 40.8% |
| Yes | 234 | 59.2% |
| Types of supplements/herbs used (multiple responses allowed) | ||
| Vitamin supplements (such as vitamin C or D) | 195 | 49.4% |
| Mineral supplements (such as calcium or magnesium) | 76 | 19.2% |
| Protein supplements (such as whey protein) | 22 | 5.6% |
| Fish oil or omega-3 supplements | 79 | 20.0% |
| Medicinal herbs (such as fenugreek, ginger, or turmeric) | 85 | 21.5% |
| Commercial herbal products (such as black seed or honey-based products) | 93 | 23.5% |
| Energy or endurance supplements (such as caffeine or sports supplements) | 62 | 15.7% |
| Regular engagement in physical exercise | ||
| No | 248 | 62.8% |
| Yes | 147 | 37.2% |
| Types of physical activity practiced (among those who exercise) | ||
| Walking or running | 213 | 53.9% |
| Strength training (weightlifting) | 75 | 19.0% |
| Yoga or meditation exercises | 39 | 9.9% |
| Aerobic exercises (such as Zumba or cardio) | 52 | 13.2% |
| Team sports (such as football or basketball) | 26 | 6.6% |
| Swimming | 27 | 6.8% |
| Cycling | 18 | 4.6% |
| Perception that inadequate sleep negatively affects health and longevity | ||
| No | 16 | 4.1% |
| Yes | 379 | 95.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allehaibi, L.; Abuhaimed, L.; Hakami, B.; Alotaibi, A.; Alabbasi, S.; Alsharif, Z.; Alayyafi, T.; Alamri, A.; Althaqil, R.; Alnuhait, M. Public Awareness and Perceptions of Longevity Determinants in Saudi Arabia: A Cross-Sectional Study (2024–2025). Healthcare 2025, 13, 1229. https://doi.org/10.3390/healthcare13111229
Allehaibi L, Abuhaimed L, Hakami B, Alotaibi A, Alabbasi S, Alsharif Z, Alayyafi T, Alamri A, Althaqil R, Alnuhait M. Public Awareness and Perceptions of Longevity Determinants in Saudi Arabia: A Cross-Sectional Study (2024–2025). Healthcare. 2025; 13(11):1229. https://doi.org/10.3390/healthcare13111229
Chicago/Turabian StyleAllehaibi, Lamah, Lamia Abuhaimed, Bashaer Hakami, Ayman Alotaibi, Sarah Alabbasi, Zain Alsharif, Taif Alayyafi, Asayel Alamri, Rawan Althaqil, and Mohammed Alnuhait. 2025. "Public Awareness and Perceptions of Longevity Determinants in Saudi Arabia: A Cross-Sectional Study (2024–2025)" Healthcare 13, no. 11: 1229. https://doi.org/10.3390/healthcare13111229
APA StyleAllehaibi, L., Abuhaimed, L., Hakami, B., Alotaibi, A., Alabbasi, S., Alsharif, Z., Alayyafi, T., Alamri, A., Althaqil, R., & Alnuhait, M. (2025). Public Awareness and Perceptions of Longevity Determinants in Saudi Arabia: A Cross-Sectional Study (2024–2025). Healthcare, 13(11), 1229. https://doi.org/10.3390/healthcare13111229