Translation, Cross-Cultural Adaptation, and Feasibility of the NHPT-E of Manual Dexterity for the Spanish Population

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
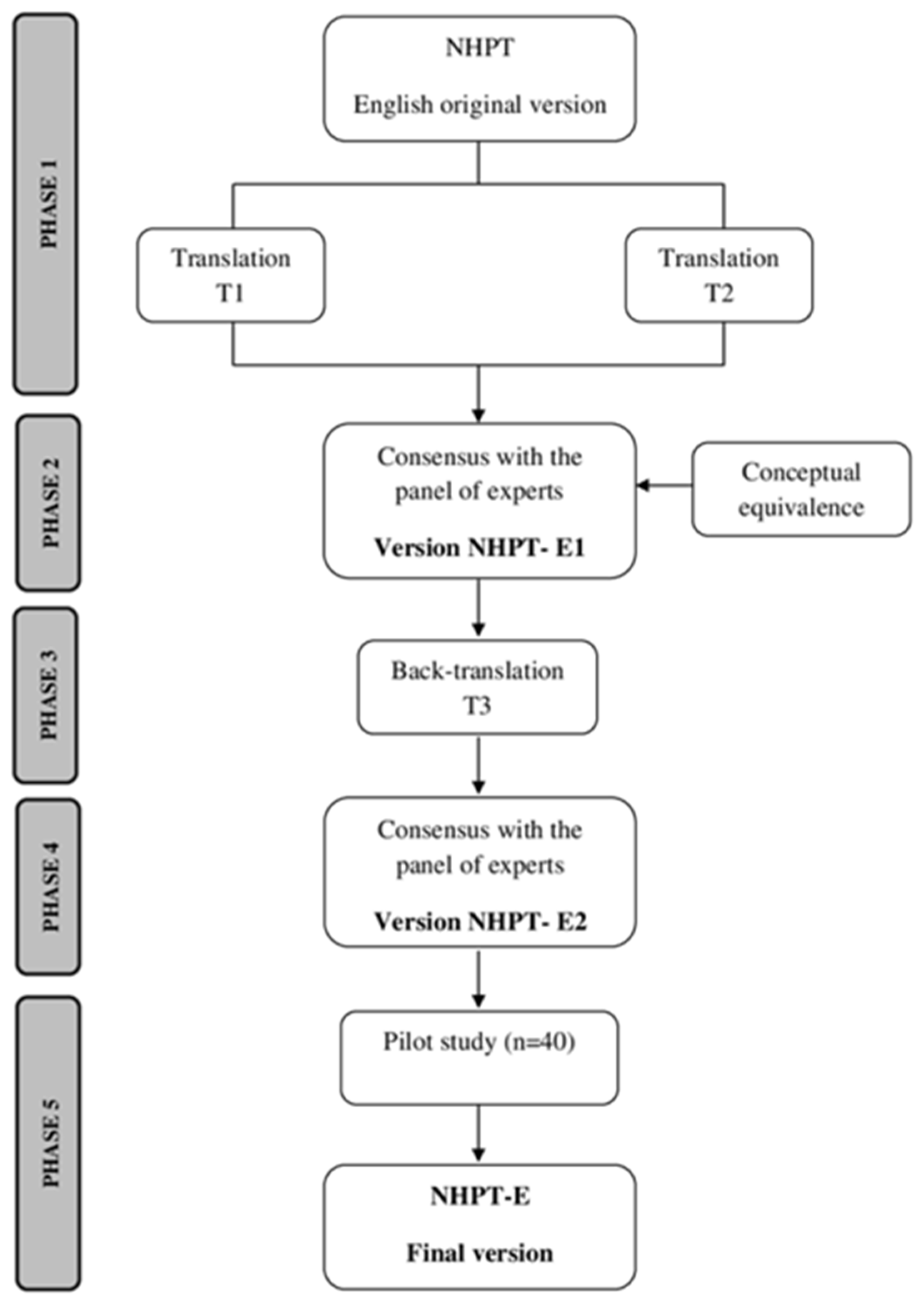
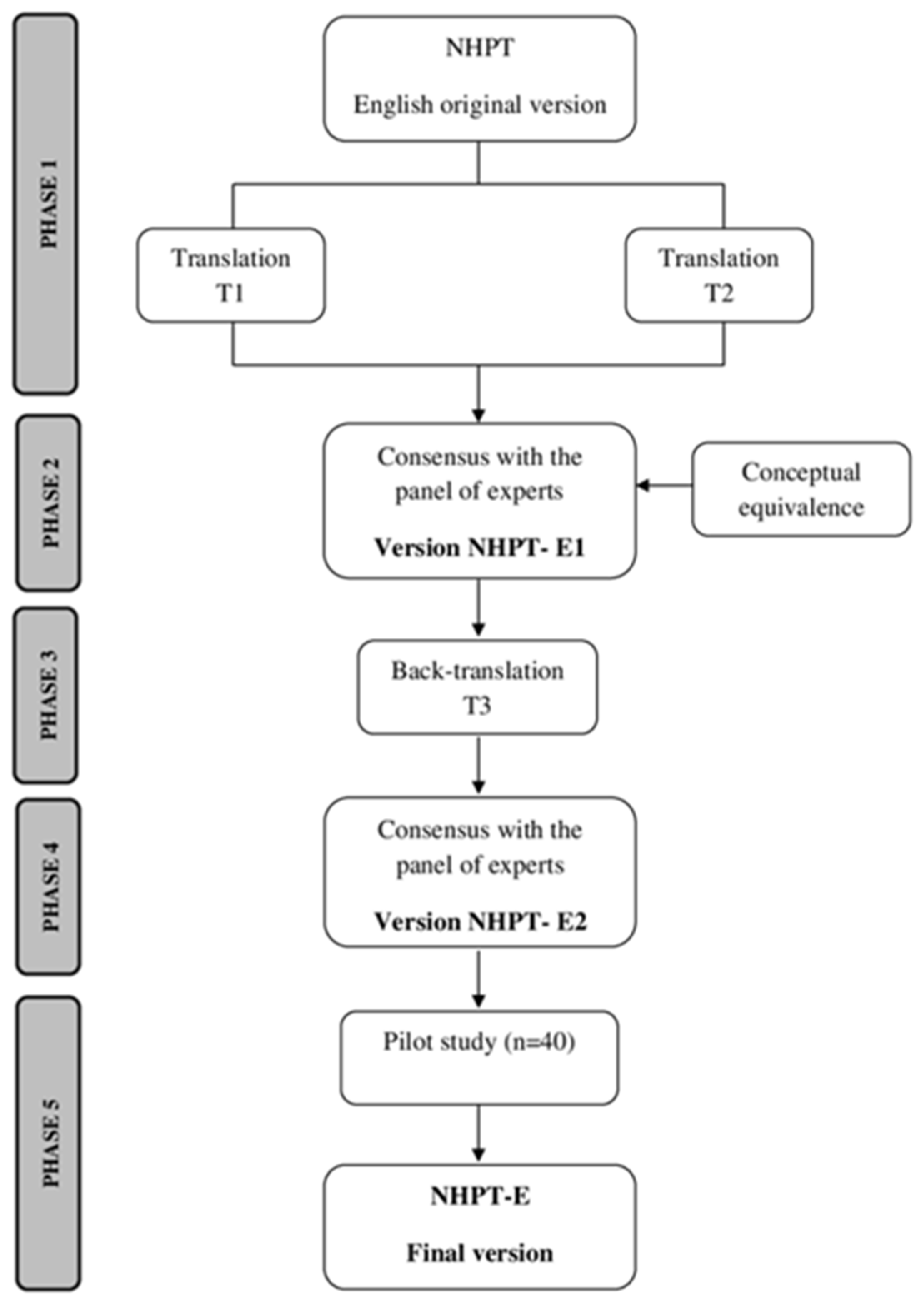
2.1. Process of Transcultural Adaptation of the NHPT to Spanish (NHPT-E)
2.2. Pilot Testing of the NHPT-E2
2.2.1. Participants
2.2.2. Instrument
- -
- NHPT-E2: It consists, like the original version (NHPT), of a rectangular base composed of a small container with nine holes (10 mm diameter and 15 mm deep) and nine pins (7 mm diameter and 32 mm long). The recommended commercial plastic version of the NHPT [28] was used after finding that there is no significant difference in the time to complete the task between this version and the wooden version [14]. To perform the test, the person being tested must insert the nine pegs, one at a time, into the holes as quickly as possible. Subsequently, the pegs must be removed, one at a time, and placed back into the container. This process must be completed with both hands independently, and the test is always started with the dominant hand, recording the time (in seconds) it takes the person being tested to complete the task with each hand.
- -
- Feasibility: an evaluation questionnaire developed from Iraossi’s pilot test process checklist was used [29]. It included 5 questions for participants focusing on (1) the purpose of the test, (2) comfort in taking the test, and (3) clarity of the prompts. Another 14 questions were intended for the evaluators (n = 4), related to the aforementioned information (1,2,3), and also to the ease or difficulty in its application, recording, and interpretation of results. The answers for the total of the 19 questions were Likert-type (not at all; I don’t think so; I am not sure; I think so; and yes totally).
2.2.3. Statistical Analysis
3. Results
3.1. NHPT-E2 Adaptation
3.2. NHPT-E2 Pilot Study
3.3. Feasibility of NHPT-E2
4. Discussion
Limitations
5. Conclusions
Clinical Applicability and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Prueba Del Tablero de Nueve Agujeros |
| Mathiowetz V, Weber K, Kashman N, Volland G. Adult Norms for the Nine Hole Peg Test of Finger Dexterity. The Occupational Therapy Journal of Research. 1985; 5:24–33 [14] |
 |
| Información general: |
|
| Medidas de construcción (Mathiowetz et al., 1985 [14]): |
|
| Instrucciones (Mathiowetz et al., 1985 [14]): |
|
| Registro de respuesta |
| Prueba del Tablero de Nueve Agujeros (NHPT-E) |
| Adaptado por Moreno-Morente G, Hurtado-Pomares M, Sánchez-Pérez A, Terol Cantero MC |
| Nombre: _______________________________________________________ |
| Mano Dominante (marque una opción): Derecha Izquierda |
| Tiempo para completar la prueba en segundos: |
| Fecha:_______Mano Dominante:___________Mano No Dominante:_________ |
| Fecha:_______Mano Dominante:___________Mano No Dominante:_________ |
| Fecha:_______Mano Dominante:___________Mano No Dominante:_________ |
| Fecha:_______Mano Dominante:___________Mano No Dominante:_________ |
References
- Oliveira, C.S.; Almeida, C.S.; Freitas, L.C.; Santana, R.; Fernandes, G.; Junior, P.R.F.; Moura, R.C.F. Use of the Box and Block Test for the evaluation of manual dexterity in individuals with central nervous system disorders: A systematic review. Man. Ther. Posturol. Rehabil. J. 2020, 14, 436. [Google Scholar] [CrossRef]
- Andersen, K.W.; Siebner, H.R. Mapping dexterity and handedness: Recent insights and future challenges. Curr. Opin. Behav. Sci. 2018, 20, 123–129. Available online: https://www.sciencedirect.com/science/article/pii/S2352154617300918 (accessed on 16 November 2023). [CrossRef]
- Pérez-Mármol, J.M.; Ortega-Valdivieso, M.A.; Cano-Deltell, E.E.; Peralta-Ramírez, M.I.; García-Ríos, M.C.; Aguilar-Ferrándiz, M.E. Influence of upper limb disability, manual dexterity and fine motor skill on general self-efficacy in institutionalized elderly with osteoarthritis. J. Hand Ther. 2016, 29, 58–65. [Google Scholar] [CrossRef]
- Lotze, M.; Lindberg, P.G. Editorial: Promoting Manual Dexterity Recovery after Stroke. Front. Neurol. 2019, 10, 815. [Google Scholar] [CrossRef] [PubMed]
- De-Bernardi-Ojuel, L.; Torres-Collado, L.; García-De-La-Hera, M. Occupational Therapy Interventions in Adults with Multiple Sclerosis or Amyotrophic Lateral Sclerosis: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 1432. [Google Scholar] [CrossRef] [PubMed]
- Månsson, E.; Lexell, J. Performance of activities of daily living in multiple sclerosis. Disabil. Rehabil. 2004, 26, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Jaric, S. Hand function in multiple sclerosis: Force coordination in manipulation tasks. Clin. Neurophysiol. 2008, 119, 2274–2281. [Google Scholar] [CrossRef]
- Abbas, D.; Gehanno, J.F.; Caillard, J.F.; Beuret-Blanquart, F. Characteristics of patients sufferingfrom multiple sclerosis according to profesional situation. Ann. Readapt. Med. Phys. 2008, 51, 386–393. [Google Scholar] [CrossRef] [PubMed]
- García, C.C.; Vicente, L.S.; Niño, M.G.C.; Muñoz, E.M.N. Evaluación de la funcionalidad del miembro superior en personas adultas con daño cerebral adquirido realizada por los/as profesionales de la terapia ocupacional en España, estudio transversal. J. Move Ther. Sci. 2021, 3, 309–318. [Google Scholar]
- Li, K.-Y.; Lin, L.-J.; Chan, A.-T.; Chen, C.-H.; Chang, W.-M.; Cho, Y.-J. Population based norms for the box and blocks test in healthy right-handed Taiwanese adults. Biomed. J. 2020, 43, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Jebsen, R.H.; Taylor, N.; Trieschmann, R.B.; Trotter, M.J.; A Howard, L. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar]
- Tiffin, J.; Asher, E.J. The Purdue pegboard: Norms and studies of reliability and validity. J. Appl. Psychol. 1948, 32, 234–247. [Google Scholar] [CrossRef]
- Kellor, M.; Frost, J.; Silberberg, N.; Iversen, I.; Cummings, R. Hand strength and dexterity. Am. J. Occup. Ther. 1971, 25, 77–83. [Google Scholar]
- Mathiowetz, V.; Weber, K.; Kashman, N.; Volland, G. Adult norms for the Nine Hole Peg Test of finger dexterity: Occupation, Participation and Health. Occup. Ther. J. Res. 1985, 5, 24–38. [Google Scholar] [CrossRef]
- Grice, K.O.; Vogel, K.A.; Le, V.; Mitchell, A.; Muniz, S.; Vollmer, M.A. Adult norms for a commercially available nine hole peg test for finger dexterity. Am. J. Occup. Ther. 2003, 57, 570–573. [Google Scholar] [CrossRef]
- Hashemi, Y.; Taghizadeh, G.; Azad, A.; Behzadipour, S. The effects of supervised and non-supervised upper limb virtual reality exercises on upper limb sensory-motor functions in patients with idiopathic Parkinson’s disease. Hum. Mov. Sci. 2022, 85, 102977. [Google Scholar] [CrossRef]
- Testud, B.; Delacour, C.; El Ahmadi, A.A.; Brun, G.; Girard, N.; Duhamel, G.; Heesen, C.; Häußler, V.; Thaler, C.; Silemek, A.C.H.; et al. Brain grey matter perfusion in primary progressive multiple sclerosis: Mild decrease over years and regional associations with cognition and hand function. Eur. J. Neurol. 2022, 29, 1741–1752. [Google Scholar] [CrossRef]
- Almhdawi, K.A.; Alazrai, A.; Kanaan, S.; Shyyab, A.A.; Oteir, A.O.; Mansour, Z.M.; Jaber, H. Post-stroke depression, anxiety, and stress symptoms and their associated factors: A cross-sectional study. Neuropsychol. Rehabil. 2020, 31, 1091–1104. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Sánchez, S.; Molina-Rueda, F.; Florencio, L.L.; Carratalá-Tejada, M.; Cuesta-Gómez, A. Reliability and agreement of the Nine Hole Peg Test in patients with unilateral spastic cerebral palsy. Eur. J. Pediatr. 2022, 181, 2283–2290. [Google Scholar] [CrossRef] [PubMed]
- Temporiti, F.; Mandaresu, S.; Calcagno, A.; Coelli, S.; Bianchi, A.M.; Gatti, R.; Galli, M. Kinematic evaluation and reliability assessment of the Nine Hole Peg Test for manual dexterity. J. Hand Ther. 2022, 36, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Wesley, A.; Bray, P.; Pacey, V.; Chan, C.; Nicholson, L.L. Hand Impairment and Function in Children and Adolescents with Heritable Disorders of Connective Tissue. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 2022, 76, 7606205030. [Google Scholar] [CrossRef]
- Poole, J.L.; Burtner, P.A.; Torres, T.A.; McMullen, C.K.; Markham, A.; Marcum, M.L.; Anderson, J.B.; Qualls, C. Measuring dexterity in children using the Nine-hole Peg Test. J. Hand Ther. 2005, 18, 348–351. [Google Scholar] [CrossRef]
- Hervault, M.; Balto, J.M.; Hubbard, E.A.; Motl, R.W. Reliability, precision, and clinically important change of the Nine-Hole Peg Test in individuals with multiple sclerosis. Int. J. Rehabil. Res. 2017, 40, 91–93. [Google Scholar] [CrossRef]
- Serrano-López Terradas, P.A.; Criado Ferrer, T.; Jakob, I.; Calvo-Arenillas, J.I. Quo Vadis, Amadeo Hand Robot? A Randomized Study with a Hand Recovery Predictive Model in Subacute Stroke. Int. J. Environ. Res. Public Health 2022, 20, 690. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Herrera-Baeza, P.; García-Bravo, C.; Huertas-Hoyas, E.; Florencio, L.-L.; Martínez-Piédrola, R.M.; Pérez-Corrales, J.; Sánchez-Camarero, C.; Pérez-De-Heredia-Torres, M. Mental Practice and Manipulative Skills Training Among People with Multiple Sclerosis: A Pilot Study. Am. J. Occup. Ther. 2022, 76, 7602205040. [Google Scholar] [CrossRef] [PubMed]
- International Test Commission. The ITC Guidelines for Translating and Adapting Tests, 2nd ed.; International Test Commission: Hemel Hempstead, UK, 2017; Available online: www.InTestCom.org (accessed on 17 April 2021).
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Feys, P.; Lamers, I.; Francis, G.; Benedict, R.; Phillips, G.; Larocca, N.; Hudson, L.D.; Rudick, R.; Multiple Sclerosis Outcome Assessments Consortium. The Nine-Hole Peg Test as a manual dexterity performance measure for multiple sclerosis. Mult. Scler. 2017, 23, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Iarossi, G. The Power of Survey Design: A User’s Guide for Managing Surveys, Interpreting Results, and Influencing Respondents; World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Sommerfeld, D.K.; Eek, E.U.; Svensson, A.K.; Holmqvist, L.W.; von Arbin, M.H. Spasticity after stroke: Its occurrence and association with motor impairments and activity limitations. Stroke 2004, 35, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Heller, A.; Wade, D.T.; Wood, V.A.; Sunderland, A.; Hewer, R.L.; Ward, E. Arm function after stroke: Measurement and recovery over the first three months. J. Neurol. Neurosurg. Psychiatry 1987, 50, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Alberto, A.; Unidad, B.; Blanca, B. Adaptación Transcultural de Instrumentos. Guía para el Proceso de Validación de Instrumentos Tipo Encuestas. Rev. Científica AMBB 2006, 16, 74–82. [Google Scholar]
- Vasylenko, O.; Gorecka, M.M.; Rodríguez-Aranda, C. Manual dexterity in young and healthy older adults. Age- and gender-related differences in unimanual and bimanual performance. Dev. Psychobiol. 2018, 60, 407–427. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Luján, J.A.; Cardona, J.A. Construcción y validación de escalas de medición en salud: Revisión de propiedades psicométricas. Arch. Med. 2015, 11, 1–10. [Google Scholar]

{kind=link}
| Age, Mean (IR) | 39 (21;59) |
|---|---|
| Gender, n (%) | |
| Female | 24 (60) |
| Male | 16 (40) |
| Educational level, n (%) | |
| No or primary education | 13 (32.5) |
| Secondary | 11 (27.5) |
| Superiors | 16 (40) |
| Employment status, n (%) | |
| Active | 35 (87.5) |
| Unemployed | 5 (12.5) |
| Dominance, n (%) | |
| Right-handed | 37 (92.5) |
| Lefty | 3 (7.5) |
| Mathiowetz et al., 1985 [14] | Committee of Experts | |
|---|---|---|
| Información Ormación General |
|
|
|
| |
|
| |
|
| |
|
| |
| Instalación (Mathiowetz et al., 1985 [14]) |
|
|
|
| |
|
| |
|
| |
| Instrucciones (Mathiowtz et al., 1985 [14]) |
|
|
|
| |
|
| |
|
| |
|
| |
|
|
| Sociodemographic Variables (n) | NHPT-E SCORE | ||||
|---|---|---|---|---|---|
| Hand | Mean (SD) | Median (IR) | Minimum | Maximum | |
| Total (40) | D | 16.55 (2.52) | 16.32 (14.83–17.58) | 12.35 | 23.50 |
| ND | 17.43 (2.56) | 16.62 (15.74–18.78) | 13.86 | 23.54 | |
| Age | |||||
| 20–39 (20) | D | 16.08 (2.5) | 15.40 (14.71–17.27) | 12.35 | 23.50 |
| ND | 16.72 (2.08) | 16.01 (15.63–17.39) | 14.13 | 22.67 | |
| 40–59 (20) | D | 17.01 (2.52) | 16.84 (15.53–18.08) | 13.43 | 22.35 |
| ND | 18.15 (2.84) | 17.14 (16.20–20.37) | 13.86 | 23.54 | |
| Sex | |||||
| Women (24) | D | 16.57 (2.19) | 16.42 (15.48–17.62) | 12.35 | 21.83 |
| ND | 17.57 (2.30) | 16.75 (15.89–18.78) | 15.14 | 22.67 | |
| Men (16) | D | 16.52 (3.03) | 15.05 (14.48–17.36) | 13.43 | 23.50 |
| ND | 17.22 (2.98) | 16.27 (15.14–18.91) | 13.86 | 23.54 | |
| Educational level | |||||
| Primary Education (23) | D | 17.06 (2.09) | 16.97 (16.06–17.67) | 13.90 | 21.83 |
| ND | 18.35 (2.38) | 17.39 (16.70–20.35) | 13.86 | 21.66 | |
| Secondary Education (11) | D | 17.17 (2.30) | 16.42 (15.08–18.98) | 13.43 | 23.50 |
| ND | 18.35 (2.39) | 15.75 (15.43–16.14) | 13.95 | 22.67 | |
| Higher Education (16) | D | 15.70 (2.40) | 15.12 (13.98–17.01) | 12.35 | 22.35 |
| ND | 17.28 (2.549 | 16.59 (15.82–17.70) | 14.13 | 23.54 | |
| Employment status | |||||
| Active (35) | D | 16.08 (2.04) | 16.09 (14.65–17.27) | 12.35 | 21.83 |
| ND | 17.54 (2.38) | 16.80 (15.88–19.16) | 13.86 | 22.67 | |
| Unemployed (5) | D | 19.77 (3.42) | 19.96 (18.12–22.35) | 14.92 | 23.50 |
| ND | 16.70 (3.90) | 15.46 (14.39–15.94) | 14.13 | 23.54 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Morente, G.; Hurtado-Pomares, M.; Sánchez-Pérez, A.; Terol-Cantero, M.C. Translation, Cross-Cultural Adaptation, and Feasibility of the NHPT-E of Manual Dexterity for the Spanish Population. Healthcare 2024, 12, 550. https://doi.org/10.3390/healthcare12050550
Moreno-Morente G, Hurtado-Pomares M, Sánchez-Pérez A, Terol-Cantero MC. Translation, Cross-Cultural Adaptation, and Feasibility of the NHPT-E of Manual Dexterity for the Spanish Population. Healthcare. 2024; 12(5):550. https://doi.org/10.3390/healthcare12050550
Chicago/Turabian StyleMoreno-Morente, Gema, Miriam Hurtado-Pomares, Alicia Sánchez-Pérez, and M. Carmen Terol-Cantero. 2024. "Translation, Cross-Cultural Adaptation, and Feasibility of the NHPT-E of Manual Dexterity for the Spanish Population" Healthcare 12, no. 5: 550. https://doi.org/10.3390/healthcare12050550
APA StyleMoreno-Morente, G., Hurtado-Pomares, M., Sánchez-Pérez, A., & Terol-Cantero, M. C. (2024). Translation, Cross-Cultural Adaptation, and Feasibility of the NHPT-E of Manual Dexterity for the Spanish Population. Healthcare, 12(5), 550. https://doi.org/10.3390/healthcare12050550