
Cross-Cultural Adaptation and Validation of the Arabic Version of the Prolapse Quality of Life Questionnaire in the United Arab Emirates


Abstract
1. Introduction
2. Materials and Methods
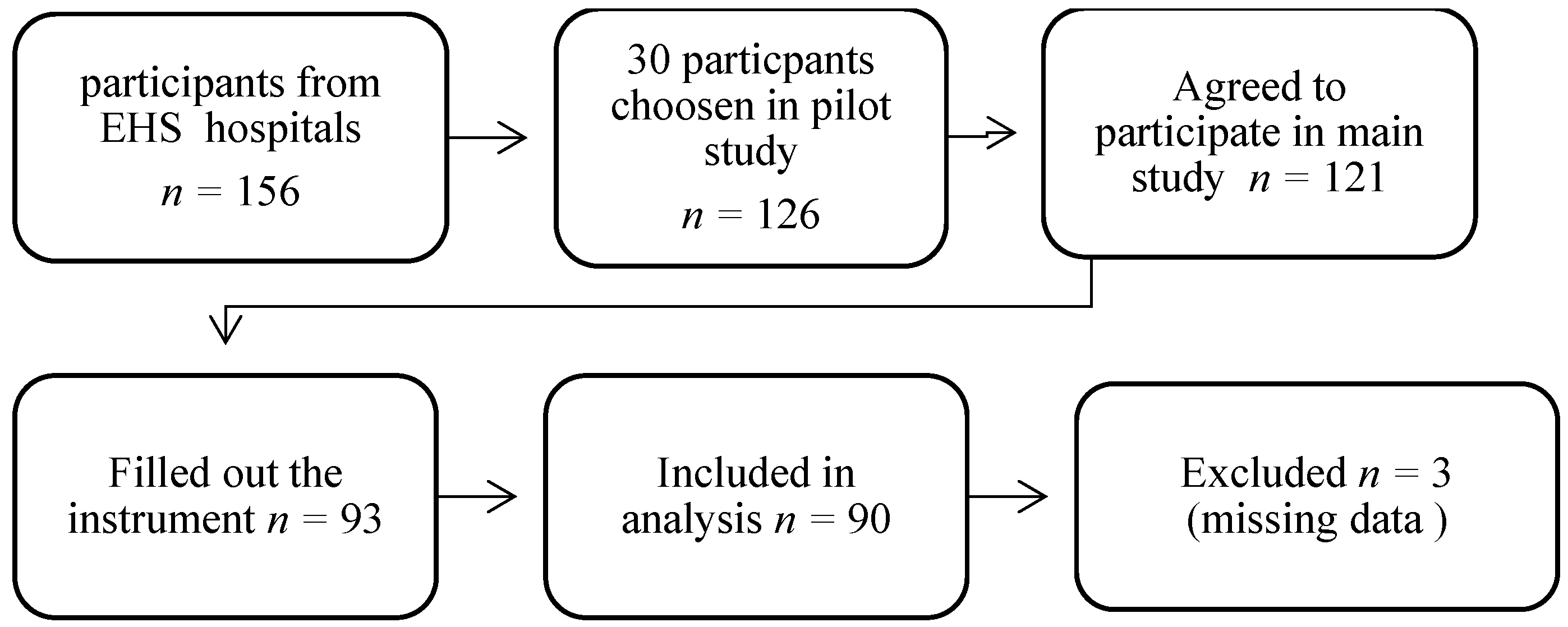
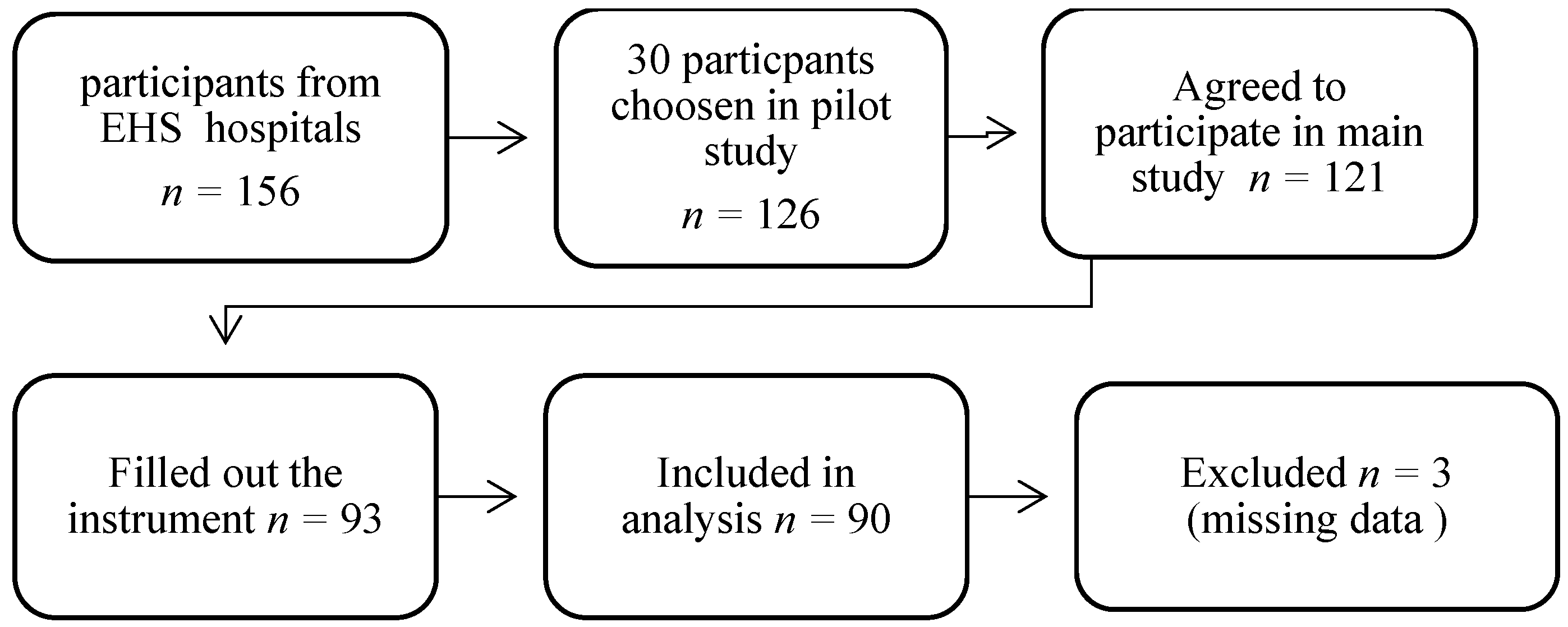
2.1. Participants
2.2. Prolapse Quality of Life Questionnaire (Study Tool)
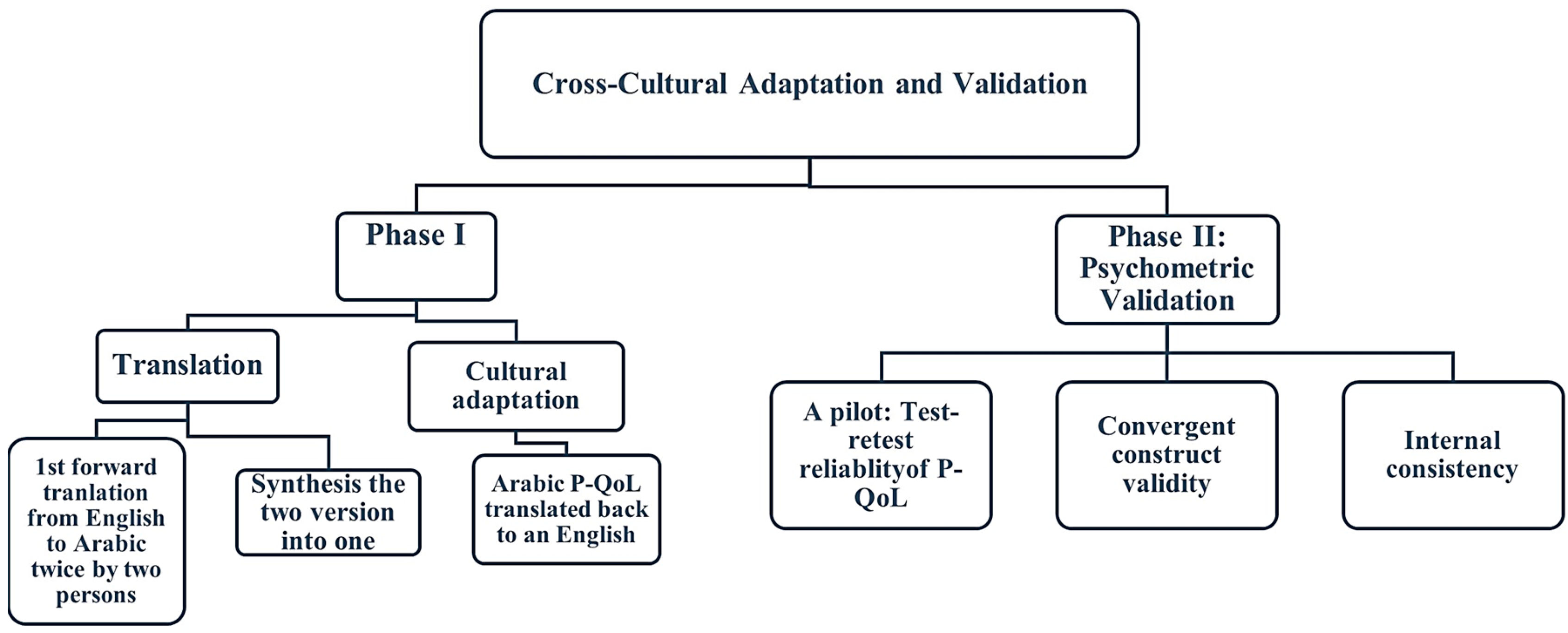
2.3. Phase I: Translation and Cultural Adaptation
2.4. Phase II: Psychometric Validation
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
6. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyer, I.; Morgan, S.L.; Markland, A.D.; Szychowski, J.M.; Richter, H.E. Pelvic Floor Disorder Symptoms and Bone Strength in Postmenopausal Women. Int. Urogynecol. J. 2020, 31, 1777–1784. [Google Scholar] [CrossRef] [PubMed]
- Zuchelo, L.T.; Bezerra, I.M.; Da Silva, A.T.; Gomes, J.; Soares Junior, J.M.; Chada Baracat, E.; de Abreu, L.C.; Sorpreso, I.C. Questionnaires to Evaluate Pelvic Floor Dysfunction in the Postpartum Period: A Systematic Review. Int. J. Womens Health 2018, 10, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Malaekah, H.; Al Medbel, H.S.; Al Mowallad, S.; Al Asiri, Z.; Albadrani, A.; Abdullah, H. Arabic Translation, Cultural Adaptation, and Validation of Australian Pelvic Floor Questionnaire in a Saudi Population. BMC Womens Health 2021, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- Belayneh, T.; Gebeyehu, A.; Adefris, M.; Rortveit, G.; Genet, T. Translation, Transcultural Adaptation, Reliability and Validation of the Pelvic Organ Prolapse Quality of Life (P-QoL) in Amharic. Health Qual. Life Outcomes 2019, 17, 12. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, N.K.; Nieminen, K.; Heikkinen, A.-M.; Jalkanen, J.; Koivurova, S.; Eloranta, M.-L.; Suvitie, P.; Tolppanen, A.-M. Validation of the Short Forms of the Pelvic Floor Distress Inventory (PFDI-20), Pelvic Floor Impact Questionnaire (PFIQ-7), and Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12) in Finnish. Health Qual. Life Outcomes 2017, 15, 88. [Google Scholar] [CrossRef]
- Digesu, G.A.; Khullar, V.; Cardozo, L.; Robinson, D.; Salvatore, S. P-QOL: A Validated Questionnaire to Assess the Symptoms and Quality of Life of Women with Urogenital Prolapse. Int. Urogynecol. J. 2005, 16, 176–181. [Google Scholar] [CrossRef]
- Digesu, G.A.; Santamato, S.; Khullar, V.; Santillo, V.; Digesu, A.; Cormio, G.; Loverro, G.; Selvaggi, L. Validation of an Italian Version of the Prolapse Quality of Life Questionnaire. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 106, 184–192. [Google Scholar] [CrossRef]
- Lenz, F.; Stammer, H.; Brocker, K.; Rak, M.; Scherg, H.; Sohn, C. Validation of a German Version of the P-QOL Questionnaire. Int. Urogynecol. J. 2009, 20, 641–649. [Google Scholar] [CrossRef]
- Svihrova, V.; Digesu, G.A.; Svihra, J.; Hudeckova, H.; Kliment, J.; Swift, S. Validation of the Slovakian Version of the P-QOL Questionnaire. Int. Urogynecol. J. 2010, 21, 53–61. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, M.S.; Tamanini, J.T.N.; de Aguiar Cavalcanti, G. Validation of the Prolapse Quality-of-Life Questionnaire (P-QoL) in Portuguese Version in Brazilian Women. Int. Urogynecol. J. 2009, 20, 1191–1202. [Google Scholar] [CrossRef] [PubMed]
- Manchana, T.; Bunyavejchevin, S. Validation of the Prolapse Quality of Life (P-QOL) Questionnaire in Thai Version. Int. Urogynecol. J. 2010, 21, 985–993. [Google Scholar] [CrossRef]
- Fukumoto, Y.; Uesaka, Y.; Yamamoto, K.; Ito, S.; Yamanaka, M.; Takeyama, M.; Noma, M. Assessment of Quality of Life in Women with Pelvic Organ Prolapse: Conditional Translation and Trial of p-Qol for Use in Japan. Nihon Hinyokika Gakkai Zasshi 2008, 99, 531–542. [Google Scholar] [CrossRef]
- Claerhout, F.; Moons, P.; Ghesquiere, S.; Verguts, J.; De Ridder, D.; Deprest, J. Validity, Reliability and Responsiveness of a Dutch Version of the Prolapse Quality-of-Life (P-QoL) Questionnaire. Int. Urogynecol. J. 2010, 21, 569–578. [Google Scholar] [CrossRef]
- Brandt, C.; Van Rooyen, C.; Cronje, H. Validation of the Prolapse Quality of Life Questionnaire (P-QOL): An Afrikaans Version in a South African Population. S. Afr. J. Obstet. Gynaecol. 2016, 22, 38. [Google Scholar] [CrossRef]
- Nojomi, M.; Digesu, G.A.; Khullar, V.; Morovatdar, N.; Haghighi, L.; Alirezaei, M.; Swift, S. Validation of Persian Version of the Prolapse Quality-of-Life Questionnaire (P-QOL). Int. Urogynecol. J. 2012, 23, 229–233. [Google Scholar] [CrossRef]
- Bazi, T.; Kabakian-Khasholian, T.; Ezzeddine, D.; Ayoub, H. Validation of an Arabic Version of the Global Pelvic Floor Bother Questionnaire. Int. J. Gynaecol. Obstet. 2013, 121, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Elbiss, H.M.; Osman, N.; Hammad, F.T. Prevalence, Risk Factors and Severity of Symptoms of Pelvic Organ Prolapse among Emirati Women. BMC Urol. 2015, 15, 66. [Google Scholar] [CrossRef] [PubMed]
- De Figueiredo, V.B.; Ferreira, C.H.J.; da Silva, J.B.; de Oliveira Esmeraldo, G.N.D.; Brito, L.G.O.; do Nascimento, S.L.; Driusso, P. Responsiveness of Pelvic Floor Distress Inventory (PFDI-20) and Pelvic Floor Impact Questionnaire (PFIQ-7) after Pelvic Floor Muscle Training in Women with Stress and Mixed Urinary Incontinence. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 255, 129–133. [Google Scholar] [CrossRef]
- Bump, R.C.; Mattiasson, A.; Bø, K.; Brubaker, L.P.; DeLancey, J.O.L.; Klarskov, P.; Shull, B.L.; Smith, A.R.B. The Standardization of Terminology of Female Pelvic Organ Prolapse and Pelvic Floor Dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Cam, C.; Sakalli, M.; Ay, P.; Aran, T.; Cam, M.; Karateke, A. Validation of the Prolapse Quality of Life Questionnaire (P-QOL) in a Turkish Population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 135, 132–135. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A General Power Analysis Program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Lim, C.R.; Harris, K.; Dawson, J.; Beard, D.J.; Fitzpatrick, R.; Price, A.J. Floor and Ceiling Effects in the OHS: An Analysis of the NHS PROMs Data Set. BMJ Open 2015, 5, e007765. [Google Scholar] [CrossRef]
- Van Kampen, D.A.; Willems, W.; van Beers, L.W.A.H.; Castelein, R.M.; Scholtes, V.A.B.; Terwee, C.B. Determination and Comparison of the Smallest Detectable Change (SDC) and the Minimal Important Change (MIC) of Four-Shoulder Patient-Reported Outcome Measures (PROMs). J. Orthop. Surg. Res. 2013, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Dontje, M.L.; Dall, P.M.; Skelton, D.A.; Gill, J.M.R.; Chastin, S.F.M.; on behalf of the Seniors USP Team. Reliability, Minimal Detectable Change and Responsiveness to Change: Indicators to Select the Best Method to Measure Sedentary Behaviour in Older Adults in Different Study Designs. PLoS ONE 2018, 13, e0195424. [Google Scholar] [CrossRef] [PubMed]
- Billis, E.; Kritikou, S.; Konstantinidou, E.; Fousekis, K.; Deltsidou, A.; Sergaki, C.; Giannitsas, K. The Greek Version of the Australian Pelvic Floor Questionnaire: Cross-Cultural Adaptation and Validation amongst Women with Urinary Incontinence. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 279, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Sánchez, B.; Yuste-Sánchez, M.J.; Arranz-Martín, B.; Navarro-Brazález, B.; Romay-Barrero, H.; Torres-Lacomba, M. Quality of Life in POP: Validity, Reliability and Responsiveness of the Prolapse Quality of Life Questionnaire (P-QoL) in Spanish Women. Int. J. Environ. Res. Public Health 2020, 17, 1690. [Google Scholar] [CrossRef] [PubMed]
- Rzepka, J.; Zalewski, K.; Stefanowicz, A.; Khullar, V.; Swift, S.; Digesu, G.A. Validation of the Polish Version of P-QoL Questionnaire. Ginekol. Pol. 2016, 87, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Seamon, B.A.; Kautz, S.A.; Bowden, M.G.; Velozo, C.A. Revisiting the Concept of Minimal Detectable Change for Patient-Reported Outcome Measures. Phys. Ther. 2022, 102, 68. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Pilot Study | Main Study | |||
|---|---|---|---|---|
| n = 30 | Symptomatic n = 55 | Asymptomatic n = 35 | p-Value | |
| Age, n (%) | 0.001 ** | |||
| Mean (±SD) | 35.9 (±11.7) | 42.53 (±7.64) | 33.54 (±7.12) | |
| 18–24 | 3 (10.0) | 0 | 4 (4.4) | |
| 25–34 | 11 (36.6) | 15 (16.7) | 15 (16.7) | |
| 35–44 | 10 (33.3) | 14 (15.6) | 14 (15.6) | |
| 45–54 | 3 (10.0) | 23 (25.6) | 2 (2.2) | |
| 55–64 | 3 (10.0) | 3 (3.3) | 0 | |
| Parity, n (%) | ||||
| None | 0 (0.0) | 4 (4.4) | 16 (17.8) | 0.001 ** |
| 1–3 | 12 (40.0) | 17 (18.9) | 13 (14.4) | |
| 4 | 4 (13.3) | 30 (33.3) | 2 (2.2) | |
| More than 4 | 14 (46.6) | 4 (4.4) | 4 (4.4) | |
| Number of Deliveries, Mean (±SD) | ||||
| Vaginal delivery | 4.18 (±2.76) | 1.40 (±1.77) | ||
| Cesarean delivery | 0.91 (±1.46) | 0.60 (±1.01) | ||
| POP—Q stage, n (%) | 0.001 ** | |||
| Mean (±SD) | 1.82 (±0.77) | 0.54 (±0.51) | ||
| Stage 0 | 0 | 16 (17.7) | ||
| Stage 1 | 21 (23.3) | 19 (21.1) | ||
| Stage 2 | 24 (26.6) | 0 | ||
| Stage 3 | 9 (10.0) | 0 | ||
| Stage 4 | 1 (1.1) | 0 | ||
| Education Status Level, n (%) | ||||
| Preparatory school | 3 (10.0) | 1 (1.1) | 0 | 0.001 ** |
| High school graduate | 15 (50.0) | 52 (57.8) | 5 (5.6) | |
| Undergraduate (university level) | 12 (40.0) | 2 (2.2) | 30 (33.3) | |
| BMI (kg/m2), n (%) | ||||
| Normal (18.5–25) | 18 (60.0) | 16 (17.7) | 11 (12.2) | 0.971 |
| Overweight (25–30) | 10 (33.3) | 18 (20.0) | 10 (11.1) | |
| Obese class I (30–35) | 2 (6.6) | 19 (21.1) | 13 (14.4) | |
| Obese class II (35–40) | 2 (2.2) | 2 (2.2) | 1 (1.1) | |
| Test–Retest Reliability (N = 30) | Internal Consistency (N = 90) | ||
|---|---|---|---|
| ICC | p-Value for ICC | Cronbach’s Alpha | |
| P-QoL | 0.987 | <0.001 | 0.971 |
| General Health Perceptions | 0.974 | <0.001 | |
| Prolapse Impact | 0.969 | <0.001 | |
| Role Limitations | 0.989 | <0.001 | 0.936 |
| Physical Limitations | 0.980 | <0.001 | 0.836 |
| Social Limitations | 0.947 | <0.001 | 0.860 |
| Personal Relationships | 0.985 | <0.001 | 0.896 |
| Emotions | 0.967 | <0.001 | 0.918 |
| Sleep/Energy | 0.935 | <0.001 | 0.682 |
| Severity Measures | 0.711 | <0.001 | 0.885 |
| ICC | SDdiff | SEM | MDC | |
|---|---|---|---|---|
| P-QoL | 0.987 (0.972–0.994) | 5.33 | 0.61 | 1.19 |
| General Health Perceptions | 0.954 (0.903–0.978) | 0.26 | 0.06 | 0.11 |
| Prolapse Impact | 0.954 (0.904–0.978) | 0.37 | 0.08 | 0.16 |
| Role Limitations | 0.982 (0.962–0.991) | 2.89 | 0.39 | 0.76 |
| Physical Limitations | 0.989 (0.976–0.995) | 0.37 | 0.04 | 0.08 |
| Social Limitations | 0.980 (0.958–0.992) | 0.78 | 0.11 | 0.22 |
| Personal Relationships | 0.934 (0.861–0.969) | 1.00 | 0.26 | 0.50 |
| Emotions | 0.985 (0.968–0.993) | 0.63 | 0.08 | 0.15 |
| Sleep/Energy | 0.967 (0.930–0.984) | 0.57 | 0.10 | 0.20 |
| Severity Measures | 0.973 (0.944–0.987) | 0.68 | 0.11 | 0.22 |
| P-QoL | APFD | SF-12 | VAS | |||
|---|---|---|---|---|---|---|
| Spearman’s rho | P-QoL | Correlation Coefficient | 1.000 | 0.676 ** | 0.020 | 0.471 ** |
| Sig. (2-tailed) | - | 0.000 | 0.855 | 0.000 | ||
| N | 90 | 90 | 90 | 89 | ||
| APFD | Correlation Coefficient | 0.676 ** | 1.000 | 0.002 | 0.463 ** | |
| Sig. (2-tailed) | 0.000 | - | 0.988 | 0.000 | ||
| N | 90 | 90 | 90 | 89 | ||
| SF-12 | Correlation Coefficient | 0.020 | 0.002 | 1.000 | −0.148 | |
| Sig. (2-tailed) | 0.855 | 0.988 | - | 0.166 | ||
| N | 90 | 90 | 90 | 89 | ||
| VAS | Correlation Coefficient | 0.471 ** | 0.463 ** | −0.148 | 1.000 | |
| Sig. (2-tailed) | 0.000 | 0.000 | 0.166 | - | ||
| N | 89 | 89 | 89 | 89 | ||
| P-QoL (GH) | P-QoL (PI) | P-QoL (RL) | P-QoL (PL) | P-QoL (SL) | P-QoL (PR) | P-QoL (Emotions) | P-QoL (Sleep/Energy) | P-QoL (SM) | P-QoL | |
|---|---|---|---|---|---|---|---|---|---|---|
| P-QoL | 0.638 ** | 0.830 ** | 0.978 ** | 0.865 ** | 0.841 ** | 0.688 ** | 0.843 ** | 0.776 ** | 0.797 ** | - |
| APFD1 | 0.595 ** | 0.695 ** | 0.853 ** | 0.790 ** | 0.793 ** | 0.637 ** | 0.723 ** | 0.680 ** | 0.713 ** | 0.873 ** |
| APFD2 | 0.414 ** | 0.499 ** | 0.754 ** | 0.583 ** | 0.585 ** | 0.427 ** | 0.515 ** | 0.543 ** | 0.569 ** | 0.728 ** |
| APFD3 | 0.211 * | 0.232 * | 0.288 ** | 0.288 ** | 0.312 ** | 0.047 | 0.342 ** | 0.218 * | 0.327 ** | 0.297 ** |
| APFD | 0.443 ** | 0.492 ** | 0.674 ** | 0.595 ** | 0.613 ** | 0.371 ** | 0.585 ** | 0.494 ** | 0.594 ** | 0.677 ** |
| SF-12 | 0.017 | −0.091 | 0.049 | 0.075 | −0.050 | −0.049 | 0.041 | −0.040 | 0.032 | 0.024 |
| VAS | 0.333 ** | 0.363 ** | 0.493 ** | 0.432 ** | 0.447 ** | 0.445 ** | 0.439 ** | 0.378 ** | 0.308 ** | 0.471 ** |
| Mean of Rank | Symptomatic (n = 55) (Mean%) | Asymptomatic (n = 35) (Mean%) | p-Value |
|---|---|---|---|
| P-QoL | 60.46 | 21.99 | 0.001 * |
| APFD | 54.93 | 30.69 | 0.001 * |
| SF-12 | 44.64 | 46.86 | 0.693 |
| VAS | 52.78 | 33 | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzarooni, A.A.; Shousha, T.M.; Kim, M. Cross-Cultural Adaptation and Validation of the Arabic Version of the Prolapse Quality of Life Questionnaire in the United Arab Emirates. Healthcare 2024, 12, 444. https://doi.org/10.3390/healthcare12040444
Alzarooni AA, Shousha TM, Kim M. Cross-Cultural Adaptation and Validation of the Arabic Version of the Prolapse Quality of Life Questionnaire in the United Arab Emirates. Healthcare. 2024; 12(4):444. https://doi.org/10.3390/healthcare12040444
Chicago/Turabian StyleAlzarooni, Asma Abdelrahman, Tamer Mohamed Shousha, and Meeyoung Kim. 2024. "Cross-Cultural Adaptation and Validation of the Arabic Version of the Prolapse Quality of Life Questionnaire in the United Arab Emirates" Healthcare 12, no. 4: 444. https://doi.org/10.3390/healthcare12040444
APA StyleAlzarooni, A. A., Shousha, T. M., & Kim, M. (2024). Cross-Cultural Adaptation and Validation of the Arabic Version of the Prolapse Quality of Life Questionnaire in the United Arab Emirates. Healthcare, 12(4), 444. https://doi.org/10.3390/healthcare12040444