Abstract
Objective: This scoping review aims to map the available literature and provide an overview of the published articles discussing the impact of electronic prescribing on medication errors and pharmacy workflow. Methods: The literature search was conducted using PubMed®, Web of Science®, and the Cochrane Database of Systematic Reviews®, as well as grey literature reports, using the search terms and related components of “pharmacists”, “electronic prescribing”, “medication errors”, and “efficiency”. The search included all articles that were published from January 2011 to September 2023. Twenty-two relevant articles were identified and fully reviewed, ten of which were included in this review. Results: Electronic prescribing (e-prescribing) provides a solution for some of the challenges that are associated with handwritten and paper prescriptions. However, the implementation of e-prescribing systems has been recognized as a source of new unforeseen medication errors in all the reviewed articles. Productivity in community pharmacies has been affected with receiving electronic prescriptions (e-prescriptions) and having to deal with the issues that arise from them. The pharmacists’ interventions were not eliminated with e-prescriptions compared to other prescription formats. The most frequently reported reason for intervention was related to incomplete instructions in the field of directions of use. Other common challenges with e-prescriptions were related to missing information, quantity, inappropriate dose, dosage form, and drug. Discussion: This review demonstrates the scarcity of research about the impact of electronic prescribing on medication error and efficiency in community pharmacies. In the literature, most of the studies had mainly focused on hospital pharmacies. The literature search demonstrated that there are still some barriers to overcome with e-prescribing systems and that medication errors were not fully eliminated with e-prescriptions. New errors have been identified with e-prescriptions, all of which caused delays in processing, which affected the productivity of the pharmacy staff, and could have negatively impacted patients’ safety if not properly resolved. Conclusion: e-Prescribing solved some of the challenges associated with illegibility of handwritten prescriptions. However, more time is required to allow e-prescribing systems to mature. Further training for prescribers and pharmacists is also recommended before and after the implementation.
1. Introduction
Electronic prescribing (e-prescribing) systems are intended to establish a direct communication between the prescriber and pharmacy computer systems [1,2]. One of the major benefits of e-prescribing is the elimination of medication errors due to illegible handwriting [3]. There has been a growing interest in adopting and implementing e-prescribing systems around the world to improve patient safety and enhance the provision of healthcare. e-Prescribing is described as a solution that improves the quality of care, helps with reducing physician and pharmacist errors, and helps to decrease malpractice claims [4].
Several studies suggest that e-prescribing can reduce prescribing errors, and increase efficiency [5,6,7]. The definition of prescribing errors has been largely debated. Aronson defined a prescription error as ‘a failure in the prescription writing process that results in a wrong instruction about one or more of the normal features of a prescription’ [8]. The ‘normal features’ include the identity of the recipient, the identity of the drug, the formulation, dose, route, timing, frequency, and duration of administration [8].
e-Prescribing can be defined as the creation of a digital prescription and securely transmitting it from the prescriber’s electronic medical record (EMR) system directly to the pharmacy management system (PMS) through a secure, direct communication [6]. Electronic prescriptions aim to replace all other formats of prescriptions, including handwritten and EMR-generated prescriptions. Eliminating the need to manually enter and transcribe prescriptions into the PMS will reduce the chance pharmacy-induced errors, including transcribing errors [9].
According to a systematic review of e-prescribing practices in the ambulatory care setting published about a decade ago, e-prescribing reduces prescribing errors, increases efficiency, and helps to save on healthcare costs [10]. The focus of this review has been directed to community pharmacies since they represent the majority of pharmacy practice in Canada [11]. The main difference between a community and a hospital pharmacy is the type of patients they both serve. A community pharmacy’s main services are directed to the general public, while a hospital pharmacy is responsible for overseeing the medication management process for inpatients and outpatients in a hospital setting.
2. Study Rationale
Innovative health information technologies have been widely embraced by pharmacists to assist in their patient care duties. However, we need to acknowledge that changes in technology can also have an influence on the nature of a pharmacy’s workflow and the pace of pharmacist work, whether in hospital or in community practice.
For that reason, awareness needs to be raised about the impact of technology on a pharmacy working environment in terms of efficiency and productivity in the workplace [12]. Most importantly, there is a need to assess the impact of introducing these new technologies on patients’ safety and health outcomes. To address this gap in the literature, a scoping review was conducted to accumulate knowledge and learn about the current state of the literature.
3. Study Objective
This scoping review aims to map the available literature and provide an overview of the published articles discussing the impact of electronic prescribing on medication errors and pharmacy workflow. The objective is to provide an overview of the community pharmacists’ perception of the impact of electronic prescribing on pharmacist work, workflow, medication errors, productivity, and patient outcomes in community pharmacies.
4. Methods
This scoping review followed an enhanced Arksey and O’Malley methodological framework as described by Daudt et al. [13]. This enhanced framework describes the five steps of a scoping review as follows: identifying the research question; identifying relevant studies; study selection; charting the data; and collating, summarizing, and reporting the results.
4.1. Identifying the Research Questions
Based on the initial search conducted before writing this review, limited research was found addressing community pharmacies in general. Therefore, the research questions for this scoping review have been determined to focus on the following:
- What are the community pharmacists’ perceptions of the impact of electronic prescribing on medication errors and patient outcomes in community pharmacies?
- What are the community pharmacists’ perceptions of the impact of electronic prescribing on the pharmacist work and productivity in their pharmacy?
4.2. Identifying Relevant Studies
Identification of the relevant literature, whether qualitative or quantitative studies, was performed by conducting an initial search using two electronic databases (i.e., PubMed® and Web of Science®). The Cochrane Database of Systematic Reviews® was also reviewed in a second search to identify any systematic or scoping reviews pertinent to the research questions. To ensure that all relevant information was captured, the Grey Literature Report, an online grey literature database repository of reports, working publications, and conference proceedings, was also searched.
The search for this review was performed for published literature from January 2011 to September 2023 and was limited to English language articles only. A preliminary search of the literature was completed before conducting this review, and most of the articles relevant to our review questions started to be published in 2011. For that reason, it was decided that the search dates will include articles published between 2011 and 2023. The limitation of English only articles was imposed due to the inability to secure a reliable source of translation from other languages into English.
An experienced research librarian was consulted before starting the search to ensure that the selection of databases, search terms, and search strategy was thorough. Searches were performed using the search terms in Table 1.

Table 1.
Key word search terms.
5. Study Selection
The inclusion criteria of this scoping review are listed in Table 2. These criteria were tested on a few of the identified articles to ensure that they are capturing all articles related to the research questions. The first search was performed using PubMed® and Web of Science® databases and included two queries. The date limitation was set from January 2011 to September 2023, during the study selection process. Firstly, we used all fields to search for all articles about e-prescribing, pharmacists, and medication errors. Then the second query was used to search for articles about e-prescribing, pharmacists, and efficiency. This step was added to ensure we captured all relevant articles that might be related to our second research question. The Cochrane Database of Systematic Reviews and the Grey Literature Report were also searched for relevant articles.
Table 2.
Inclusion and exclusion criteria.
During the first stage of screening, a review of titles and abstracts was conducted by two researchers to select all relevant articles (AF and EB). A full-text examination was performed at the second stage of screening. Relevant studies were included only if they were found to fit the inclusion criteria (see Table 2).
5.1. Charting the Data
An iterative process was used to classify the general themes extracted from the selected articles in the review. This process was initially started by reading each article individually to identify the category of evidence presented in each article. Then the charting of the data was completed using Microsoft Excel. The charting form was used to collect some descriptive characteristics of the selected articles, such as the main author, year of publication, and country of origin. A data summary of the characteristics of the articles is provided in Table 3.
Table 3.
Data summary of articles included in the review.
5.2. Collating, Summarizing, and Reporting the Results
Scoping reviews are intended to provide an overview of the characteristics or factors related to a particular concept regardless of the quality of evidence [23]. For that reason, no critical appraisal was conducted to evaluate the quality of evidence in the selected articles. The variables sought in the articles were divided into two main categories: e-prescribing-related variables influencing medication errors (Table 4), and e-prescribing-related variables affecting productivity in the pharmacy (Table 5). Synthesis of the results and the data were collated and summarized across all the articles following these two categories and findings presented accordingly.
Table 4.
Summary of e-prescriptions related variables impacting medication errors across the articles.
Table 5.
Summary of e-prescriptions related variables impacting productivity in pharmacy across the articles.
6. Results
6.1. Study Selection
The searches in PubMed® and Web of Science® databases were performed in September 2023. The first query resulted in 158 articles and the second one resulted in 82 articles. On searching the other databases, 30 additional articles were found on Cochrane Database of Systematic Reviews® and no results were found in the Grey Literature Report®. After removal of duplicates, a total of 199 articles were included. The first screening process was performed by screening the titles and abstracts of all the identified articles by two researchers (EB and AF). Only 24 articles met the inclusion criteria. These articles were screened further by conducting a full text reading. The second screening yielded 10 relevant articles. Figure 1 illustrates the study selection process.
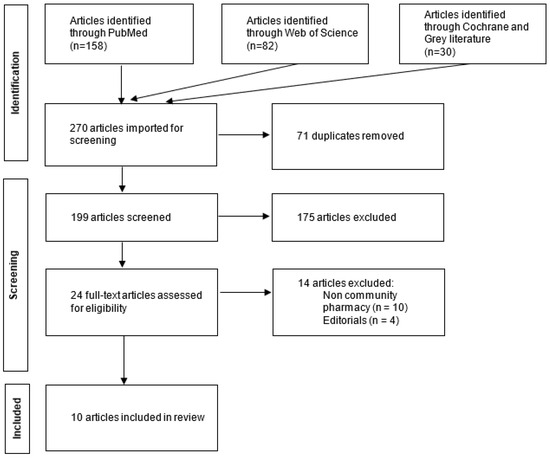
Figure 1.
Flow diagram for the study selection process.
6.2. Study Characteristics
Most of the articles in this review, around 60% (n = 6) originated from the United States, while the others were from Finland (n = 2), Canada (n = 1), and Sweden (n = 1). The oldest article identified was published in 2011 [22], which indicates that less research has been conducted on community pharmacies while the focus of most of the literature remains on hospital pharmacies.
6.3. Characteristics of the Subjects in the Studies
All subjects in this review were healthcare professionals practicing in a community pharmacy setting; whether as pharmacists, pharmacy students or pharmacy technicians and using e-prescribing systems. However, one study examined community pharmacies that did not accept e-prescriptions [18]. This study aimed to explore the barriers to adopting systems from a pharmacist’ perspective as they impact the pharmacist’s decision to adopt e-prescribing systems (i.e., whether the pharmacists were planning on using the e-prescribing systems in the future or not).
6.4. Country and Pharmacy Characteristics
The definition of e-prescribing varied between different countries. Most of the e-prescribing systems used in this review included prescriptions that were electronically generated by a prescribers’ office and securely transmitted electronically (i.e., directly) to the pharmacy’s computer system. Pharmacies that printed e-prescriptions and dealt with them as paper prescriptions were excluded [21].
6.5. Data Collection Technique
Many of the articles in this review applied observational study designs and used direct observation of the dispensing process in the participating pharmacies [14,15,19,21]. Postal questionnaires were used to survey pharmacists’ perceptions of e-prescribing systems and their thoughts about their systems’ strengths and pitfalls [17,22]. Two studies involved a secondary analysis of pre-existing datasets. One was on the National Survey of Community-Based Pharmacists [6], and the other one was on the Dyke Anderson Patient Safety Database (DAPSD) [16]. The National Survey of Community-Based Pharmacists data was collected using a web-based survey sent to community pharmacists in Canada by email [6]. The DAPSD dataset was collected using surveys of pharmacists working in different pharmacy settings in the state of Nebraska [24]. Telephone interviews were also employed, and the interviews employed both structured and semi-structured interview formats [18,20].
6.6. e-Prescribing Impact on Medication Errors
To assess the impact of e-prescribing on medication errors, some variables (for example, inaccurate dose, inappropriate quantity, wrong drug) were captured and compared between the studies included in this review (Table 4). These variables were, for the most part, consistently collected across the differing articles. Once recognized in an e-prescription, all these variables might have led to a medication error, a potential risk to patients’ safety, and/or led to the disruption of the dispensing process. A pharmacist intervention was required to resolve the problem and to complete the medication dispensing process.
The most common e-prescribing errors that required a pharmacist’s intervention had as a root cause an inaccuracy in the instructions field in the e-prescribing system regarding how to use the medication. The lack of clarity regarding the directions of medication use could lead to medication errors. Here, pharmacy staff or patients could potentially misunderstand the directions for taking the medication [16,17,20,21]. Another potential risk involving e-prescriptions was the use of abbreviation terms by prescribers in the instructions field instead of the full term(s), which can easily get misinterpreted or missed during transcription [17,19,20].
A potential source for medication errors was the use of additional field notes for extending the directions of use for a prescription. Those notes might not match the directions in the instructions field of the e-prescription which could lead to misinterpretation by the pharmacist or to the information being easily missed by pharmacy personnel [20].
Another challenge identified with e-prescriptions was the inability to accurately specify the quantity of the drug to be dispensed when the prescription is received by the pharmacy. Wrong drug quantity, duration, or day supply were reported as a regular occurrence in e-prescriptions which could also occur due to discrepancies between the directions of use and the requested quantity [17,19,21]. Other problems with e-prescriptions that increased the risk of medication errors included inappropriate drug choice, medication name, drug strength, or drug–drug interactions that were detected before the dispensing of medications [15,16,19,20]. Wrong drug selection has been reported in most of the articles, which could lead to serious clinical problems or drug–drug interactions.
The design of e-prescribing systems had an impact on medication safety as well. Some design challenges affected the proper selection of the appropriate medication (for example the drop-down menus), or the medication name was too long so the prescriber could not verify their proper selection because of it [17,21]. Other design issues were caused by inconsistencies between the size of the text fields between the prescriber’s and the pharmacy systems that could lead to data entry errors or missing some parts of the instructions of medication use [16,20,21]. Prescribing compounded medications using e-prescribing systems is a challenge due to the inconsistencies in drug names and interoperability issues between both computer systems [17].
Incorrect dose selection is another commonly occurring problem which could have a direct impact on patients’ safety if left undetected by the pharmacist [17,19]. Medication errors could occur due to the inaccurate selection of the medication dosage form which is a common challenge with e-prescriptions [17].
6.7. e-Prescribing Impact on Productivity
e-Prescribing systems have a direct impact on the workflow of all the pharmacies according to all the articles in this review (Table 5). The pharmacists described e-prescribing systems as more efficient for handling and processing prescriptions than the traditional paper format [6]. The average time for dispensing medications has decreased as less time was needed to spend on clarifying ambiguities of paper prescriptions due to illegible handwriting [14,22]. The process of retrieving, filing, and archiving the original prescription was also more efficient and faster for e-prescriptions. Another relevant feature of e-prescriptions was the ability to control medication hoarding that occurred during the COVID-19 pandemic [14].
However, there are still some of barriers to overcome with e-prescribing systems impacting the productivity of pharmacy staff while dispensing e-prescriptions [18]. When received in the pharmacy system, the pharmacy staff was often required to verify and manually change the instructions field of e-prescriptions before processing them and printing the pharmacy labels [17,20]. The manual selection of the prescribed medication was also necessary due to discrepancies between the prescriber and the pharmacy database systems [15,21]. A design challenge in e-prescribing systems was related to the excessive amount of information on e-prescriptions, which increased the time needed by the pharmacy staff to process them [21].
One study reported missing some legally required information related to the dispensing of controlled substances [19]. Missing information on the e-prescriptions led to delays, patients’ dissatisfaction, and pharmacists spending more time on solving the problem [17]. One of the important features of e-prescribing systems is the electronic refill option for renewing prescriptions, which allows for direct, prompt communication between the pharmacist and the prescriber [6]. However, the electronic renewal process was not optimally used by some pharmacies to avoid the associated service charges, or due to missing this function in the e-prescribing system [20].
Incidents of missing prescriptions occurred when patients were not able to receive their medications because of delays in sending the e-prescription or sending it to an incorrect pharmacy [20]. Missing prescriptions led to interruptions of the pharmacy workflow and more time spent by pharmacy staff to resolve the issue, which added to patients’ dissatisfaction. Pharmacy staff workload increased when duplicate orders were received, for example sending the same e-prescription by fax as well [16]. Delays with e-prescriptions also happened when the patient’s or prescriber’s information was not properly identified in the pharmacy system [15,21]. The pharmacy staff had to spend more time during the verification process to match the e-prescription with the right patient’s profile or create a new record for the prescriber if not found in the system.
Other barriers that affected productivity in the pharmacy, while dispensing e-prescriptions, were the insufficient staff training, computer and network connectivity problems, and inadequate support or maintenance [18,20,22]. Some pharmacies took a business decision and decided not to use e-prescribing systems due to the initial setup cost, or to avoid the transaction fees of e-prescriptions [18,20]. Some pharmacists thought that their intervention rates did not change with e-prescriptions compared to a handwritten or paper format [19].
7. Discussion
Research on the impact of technology on the workflow and medication safety in community pharmacies is scarce. The number of publications in hospital pharmacies and primary care settings continues to outnumber those in community pharmacy practice, even though the number of community pharmacies exceeds by far the number in any other pharmacy setting. Improving patients’ safety and reducing medication errors are two of the major attributes of e-prescribing systems that are being used to advocate for their widespread use in many countries [4,10]. The results of this review suggest that there are still some barriers to overcome with the adoption and full use of e-prescribing systems in retail pharmacies.
The literature suggests that e-prescribing helps reduce the risk of medication errors that contribute to the poor legibility of handwritten prescriptions, decreases the turnaround time for refill requests, and reduces call-backs for unsigned prescriptions [17,20,25]. However, the findings of this review demonstrated that e-prescriptions might inadvertently introduce some unforeseen challenges that could lead to medication errors and impact the productivity in community pharmacies. And for that reason, adoption and implementation rates of e-prescribing in retail pharmacies are still not meeting expectations in many countries, for example in Canada [6,26].
New Challenges with e-Prescribing
All the articles in this review demonstrated that there are some problems to overcome with e-prescriptions. The pharmacists’ interventions for medication errors were not fully eliminated with e-prescribing systems as it has been reported that there was no change in the intervention rates compared to the traditional paper prescriptions [19]. Most of the studies reported that the directions and quantity fields of the e-prescriptions were either incomplete or inappropriate. This finding is consistent with the evidence found in similar studies [27,28].
Medication errors occurred when prescribers used some Latin abbreviations in the instructions field that would not be understood by patients, for example, ‘b.i.d.’, which has to be manually changed to ‘take one tablet orally twice a day’ [17,20]. Some limitations in the e-prescription design forced the prescribers to choose unintended structured directions from a drop-down menu. As a result, the prescriber would use the additional notes field that allowed for free-text input to expand or elaborate on the directions provided in the structured field. However, using the additional notes field often did not match the provided directions in the instructions field in the e-prescription. This led to pharmacist confusion and required additional pharmacist time to clarify the e-prescriptions [20]. Sometimes these notes were just missed by the pharmacy staff, which could impose a potential risk for preventable medication errors.
This scoping review provided evidence that pharmacy staff were required to spend more time verifying and manually changing various fields of the e-prescription before dispensing a medication. Other studies reported similar findings indicating that e-prescriptions required more clarifications and time to resolve problems compared to other types of prescriptions [25,29,30,31]. The articles in this review indicated that more time was spent on resolving issues with e-prescriptions due to missing information, such as legal notation, quantity, or dose [17,19]. Manual drug selection was still required to be performed by the pharmacy staff due to discrepancies between the PMS and the EMR databases [15,20]. Depending on the training and experience of the staff, who were tasked e-prescriptions data entry, having to manually select the medication might lead to potential errors that could affect a patients’ safety.
Several researchers found patients were frustrated with e-prescriptions. Researchers identified that patients expect to pick up their medications when they arrive at the pharmacy. However, in many cases, the e-prescription had not been sent by the prescriber. Other studies had similar findings [25,32,33]. Delays in sending e-prescriptions arose from technical difficulties associated with the service, inadequate training on the prescriber or pharmacist side, or unintentionally sending of the e-prescription to the wrong pharmacy [20,25,29]. To resolve this problem, the researchers noted that pharmacists had to stop the task they were doing and had to contact the prescriber’s office to obtain a confirmation of the missing prescription, verbally or by fax. This activity caused interruptions in the pharmacy workflow and increased wait times for medications. Delays also happened when controlled substances (e.g., benzodiazepines, amphetamines, cannabinoids) were prescribed electronically. In some cases, the researchers found that the e-prescription was not compliant with the legal regulations in certain country jurisdictions [19,29].
Interoperability challenges between the EMR and the PMS created additional work for pharmacy staff. Mismatches happened due to differences in pack sizes or unit doses between the two systems that had to be corrected before processing an e-prescription. For example, when the prescribed medication is commercially available in a prepackaged form, such as an inhaler of 200 doses, or prefilled syringe of 3 mL, prescribers usually indicate in the quantity field the number of packs (e.g., three inhalers instead of 600 doses, or three syringes instead of 9 mL) [19,20]. These discrepancies cause additional processing time of e-prescriptions, leading to delays for the patients.
Wrong dose, strength, quantity, duration, and dosage form were common occurrences with e-prescriptions that could lead to significant medication errors, if not caught and addressed by a pharmacist. Pharmacists have also reported duplicate orders. Duplicate orders arise, when an e-prescription is sent, and the same prescription is also sent by other means (such as a fax or over the phone) by a prescriber. This negatively impacts the workflow in the pharmacies (i.e., pharmacists need to check for duplicate orders, and, in some cases, they need to contact the prescriber to confirm the order).
Other new challenges with e-prescribing systems included resistance from staff and the need for ongoing technical support [34]. Alert fatigue and a need for continuous updates to the database system to include new drugs, drug interactions, and contraindications has been reported [35]. Some pharmacies have decided to delay the implementation of e-prescribing systems due to business concerns. Pharmacies have identified e-prescribing start-up costs and the cost of paying transaction fees for e-prescriptions as reasons for delaying the implementation of this technology [18,20].
8. Limitations
This scoping review is first attempt to provide evidence of and highlight the impact of e-prescribing systems upon community pharmacies. To the best of our knowledge, no other reviews focused on community pharmacy workflow and error in the context of e-prescribing systems. One of the strengths in this review is the inclusion of articles from differing countries. This helped to identify common e-prescribing challenges experienced by varying nations globally, allowing for learning across healthcare systems. The review of differing country studies highlights the generalizability of the findings described in this review.
The review has a few limitations that must be acknowledged. Scoping reviews do not assess the quality of the evidence. Some of the articles in our review relied on self-reported tools to identify pharmacists’ perceptions about issues related to e-prescribing. The small sample size and limited duration of data collection period for the studies has also been identified as a limitation in some of the articles. A critical appraisal of the evidence presented in the articles was not performed as the intention of this review was to present available research regardless of the quality of evidence.
The articles included in this review were published between 2011 and 2023, and the search was limited to two main databases PubMed® and Web of Science®, along with the Grey literature. The Cochrane Database of Systematic Reviews® was also reviewed for any other systematic or scoping reviews on our topic. The articles included in the review were also limited to English language only. More articles dated before 2011, after 2023, and other literature sources might have led to more articles that would fit the inclusion criteria and might have had valuable insights. Lastly, in reviewing articles from varying countries, it was noted that the implementations of e-prescribing services varied, and this may have had an impact on the pharmacy workflow and medical error outcomes.
9. Conclusions
This scoping review provided evidence about some of the inadvertent challenges created due to the introduction of e-prescribing in primary care and community pharmacies. Medications errors and workflow interruptions are still occurring when prescriptions are received electronically. No decline was noticed in the rate of pharmacist’s interventions dealing with ambiguities related to e-prescriptions. The time spent by pharmacy staff resolving issues related to e-prescriptions was not significantly different than other formats of prescriptions (i.e., paper-based prescriptions, faxed prescriptions).
The findings of this review indicate that there are potential benefits for implementing e-prescribing systems in primary care and community pharmacies. However, system design improvements and interoperability issues need to be addressed to ensure efficiency and seamless transmission of prescriptions between the prescriber and the pharmacy before reaching the patient. More research is needed to understand the effects of introducing e-prescribing on pharmacist work. This could include more investigation into solutions that would help to address the challenges identified in this review.
Author Contributions
Conceptualization, A.A.F. and E.M.B.; methodology, A.A.F. and E.M.B.; validation, A.A.F. and E.M.B.; formal analysis, A.A.F.; investigation, A.A.F.; resources, A.A.F. and E.M.B.; data curation, A.A.F. and E.M.B.; writing—original draft preparation, A.A.F.; writing—review and editing, A.A.F. and E.M.B.; visualization, A.A.F.; supervision, E.M.B.; project administration, E.M.B.; funding acquisition, E.M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Michael Smith Health Research BC, grant number: 17589, and the University of Victoria, Canada.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Campbell, C.; Morris, C.; McBain, L. Electronic transmission of prescriptions in primary care: Transformation, timing and teamwork. J. Prim. Health Care 2021, 13, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Motulsky, A.; Liang, M.; Moreault, M.P.; Borycki, E.; Kushniruk, A.; Sicotte, C. Evaluation of a Nationwide e-Prescribing System. Stud. Health Technol. Inform. 2019, 264, 714–718. [Google Scholar] [PubMed]
- Phillips, J.L.; Shea, J.M.; Leung, V.; MacDonald, D. Impact of Early Electronic Prescribing on Pharmacists’ Clarification Calls in Four Community Pharmacies Located in St John’s, Newfoundland. JMIR Med. Inform. 2015, 3, e2. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.W.; Jiang, R. E-Prescribing: History, Issues, Potential. Online J. Public Health Inform. 2012, 4, e61049. Available online: https://journals.uic.edu/ojs/index.php/ojphi/article/view/4304 (accessed on 1 December 2018). [CrossRef] [PubMed]
- Elliott, R.; Lee, C.; Hussainy, S. Electronic prescribing and medication management at a residential aged care facility Uptake by general practitioners and qualitative evaluation of the benefits and barriers. Appl. Clin. Inform. 2016, 7, 116–127. [Google Scholar] [PubMed]
- Farghali, A.; Borycki, E.M.; Macdonald, S. Pharmacist’s perception of the impact of electronic prescribing on medication errors and productivity in community pharmacies. Knowl. Manag. E-Learn. Int. J. 2021, 13, 536–558. [Google Scholar]
- Au, Y.; Baker, L.; Hindmarsh, J. The Impact of an Electronic Prescribing Template with Decision Support upon the Prescribing of Subcutaneous Infusions at the End of Life in a Community Setting: A Future Vision for Community Palliative Care. Pharmacy 2022, 10, 112. [Google Scholar] [CrossRef] [PubMed]
- Aronson, J.K. Medication errors: Definitions and classification. Br. J. Clin. Pharmacol. 2009, 67, 599–604. [Google Scholar] [CrossRef]
- Garfield, S.; Hibberd, R.; Barber, N. English community pharmacists’ experiences of using electronic transmission of prescriptions: A qualitative study. BMC Health Serv. Res. 2013, 13, 435. [Google Scholar] [CrossRef]
- Porterfield, A.; Engelbert, K.; Coustasse, A. Electronic Prescribing: Improving the Efficiency and Accuracy of Prescribing in the Ambulatory Care Setting. Perspect. Health Inf. Manag. 2014, 11, 1g. [Google Scholar]
- National Statistics|NAPRA. 2018. Available online: https://napra.ca/national-statistics (accessed on 7 October 2018).
- MacLure, K.; Stewart, D. Digital literacy knowledge and needs of pharmacy staff: A systematic review. J. Innov. Health Inform. 2016, 23, 560–571. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Daudt, H.M.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [PubMed]
- Peltoniemi, T.; Suomi, R.; Peura, S.; Lähteenoja, M.N.Y. Electronic prescription as a driver for digitalization in Finnish pharmacies. BMC Health Serv. Res. 2021, 21, 1017. [Google Scholar] [CrossRef] [PubMed]
- Panich, J.; Larson, N.; Sojka, L.; Wallace, Z.; Lokken, J. Assessing automated product selection success rates in transmissions between electronic prescribing and community pharmacy platforms. J. Am. Med. Inf. Assoc. 2021, 28, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.R.; Galt, K.A.; Fuji, K.T. Error types with use of medication-related technology: A mixed methods research study. Res. Soc. Adm. Pharm. 2019, 15, 1480–1483. [Google Scholar] [CrossRef] [PubMed]
- Kauppinen, H.; Ahonen, R.; Timonen, J. The impact of electronic prescriptions on medication safety in Finnish community pharmacies: A survey of pharmacists. Int. J. Med. Inform. 2017, 100, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Lander, L.; Klepser, D.G.; Cochran, G.L.; Lomelin, D.E.; Morien, M. Barriers to electronic prescribing: Nebraska pharmacists’ perspective. J. Rural Health 2013, 29, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, A.M.; Miller, K.; Mohney, A.; Montenegro, C.; Schwarz, J.; Warholak, T.L. Analysis of pharmacists’ interventions on electronic versus traditional prescriptions in 2 community pharmacies. Res. Soc. Adm. Pharm. RSAP 2012, 8, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Grossman, J.M.; Cross, D.A.; Boukus, E.R.; Cohen, G.R. Transmitting and processing electronic prescriptions: Experiences of physician practices and pharmacies. J. Am. Med. Inform. Assoc. JAMIA 2012, 19, 353–359. [Google Scholar] [CrossRef]
- Odukoya, O.K.; Chui, M.A. Relationship between e-prescriptions and community pharmacy workflow. J. Am. Pharm. Assoc. Japha 2012, 52, e168–e174. [Google Scholar] [CrossRef]
- Rahimi, B.; Timpka, T. Pharmacists’ views on integrated electronic prescribing systems: Associations between usefulness, pharmacological safety, and barriers to technology use. Eur. J. Clin. Pharmacol. 2011, 67, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Galt, K.A.; Fuji, K.T.; Kaufman, T.K.; Shah, S.R. Health Information Technology Use and Patient Safety: Study of Pharmacists in Nebraska. Pharmacy 2019, 7, 7. [Google Scholar] [CrossRef]
- Franklin, B.D.; Reynolds, M.J.; Hibberd, R.; Sadler, S.; Barber, N. Community pharmacists’ interventions with electronic prescriptions in England: An exploratory study. Int. J. Clin. Pharm. 2013, 35, 1030–1035. [Google Scholar] [CrossRef]
- Canadian Medical Association (CMA); Canadian Pharmacists Association (CPhA). Vision for e-Prescribing: A Joint Statement by the Canadian Medical Association and the Canadian Pharmacists Association. 2012. Available online: http://policybase.cma.ca/dbtw-wpd/Policypdf/PD13-02.pdf (accessed on 30 April 2020).
- Ekedahl, A. Problem prescriptions in Sweden necessitating contact with the prescriber before dispensing. Res. Soc. Adm. Pharm. 2010, 6, 174–184. [Google Scholar] [CrossRef]
- Warholak, T.L.; Rupp, M.T.; Leal, S.; Kurniawan, G.; Patel, N. Assessing the effect of providing a pharmacist with patient diagnosis on electronic prescription orders: A pilot study. Res. Soc. Adm. Pharm. 2014, 10, 246–251. [Google Scholar] [CrossRef]
- Hincapie, A.L.; Warholak, T.; Altyar, A.; Snead, R.; Modisett, T. Electronic prescribing problems reported to the Pharmacy and Provider ePrescribing Experience Reporting (PEER) portal. Res. Soc. Adm. Pharm. 2014, 10, 647–655. [Google Scholar] [CrossRef]
- McLeod, M.; Karampatakis, G.D.; Heyligen, L.; McGinley, A.; Franklin, B.D. The impact of implementing a hospital electronic prescribing and administration system on clinical pharmacists’ activities—A mixed methods study. BMC Health Serv. Res. 2019, 19, 156. [Google Scholar] [CrossRef]
- Smith, M.; Sprecher, B. Pharmacy communications with physician offices to clarify prescriptions. J. Am. Pharm. Assoc. Japha 2017, 57, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Klepser, D.; Lanham, A.; Cochran, G. Electronic prescriptions: Opportunities and challenges for the patient and pharmacist. AHCT 2016, 2, 1–11. [Google Scholar] [CrossRef]
- Odukoya, O.K.; Stone, J.A.; Chui, M.A. How do community pharmacies recover from e-prescription errors? Res. Soc. Adm. Pharm. 2014, 10, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Altamura, G.; Zedda, M.; Nurchis, M.C.; Aulino, G.; Alizadeh, A.H.; Cazzato, F.; Della Morte, G.; Caputo, M.; Grassi, S.; et al. Potentiality of algorithms and artificial intelligence adoption to improve medication management in primary care: A systematic review. BMJ Open 2023, 13, e065301. [Google Scholar] [CrossRef] [PubMed]
- Rieckert, A.; Reeves, D.; Altiner, A.; Drewelow, E.; Esmail, A.; Flamm, M.; Hann, M.; Johansson, T.; Klaassen-Mielke, R.; Kunnamo, I.; et al. Use of an electronic decision support tool to reduce polypharmacy in elderly people with chronic diseases: Cluster randomised controlled trial. BMJ 2020, 369, m1822. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).