
Secondary Prevention via Case Managers in Stroke Patients: A Cost-Effectiveness Analysis of Claims Data from German Statutory Health Insurance Providers


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Intervention Costs
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Descriptive Analysis
3.3. Regression Analysis
3.4. Cost-Effectiveness Analysis
3.4.1. Deterministic Analysis
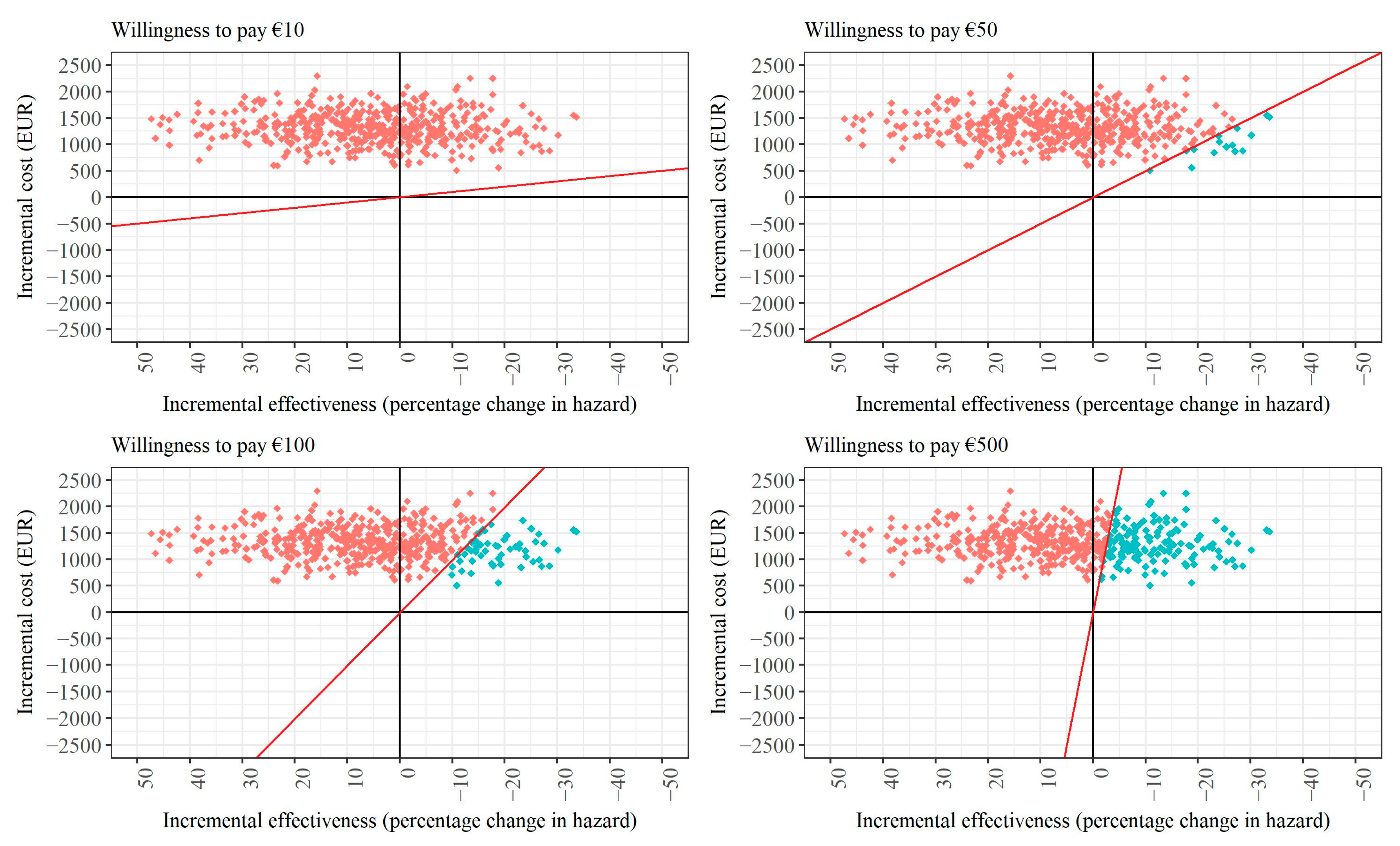
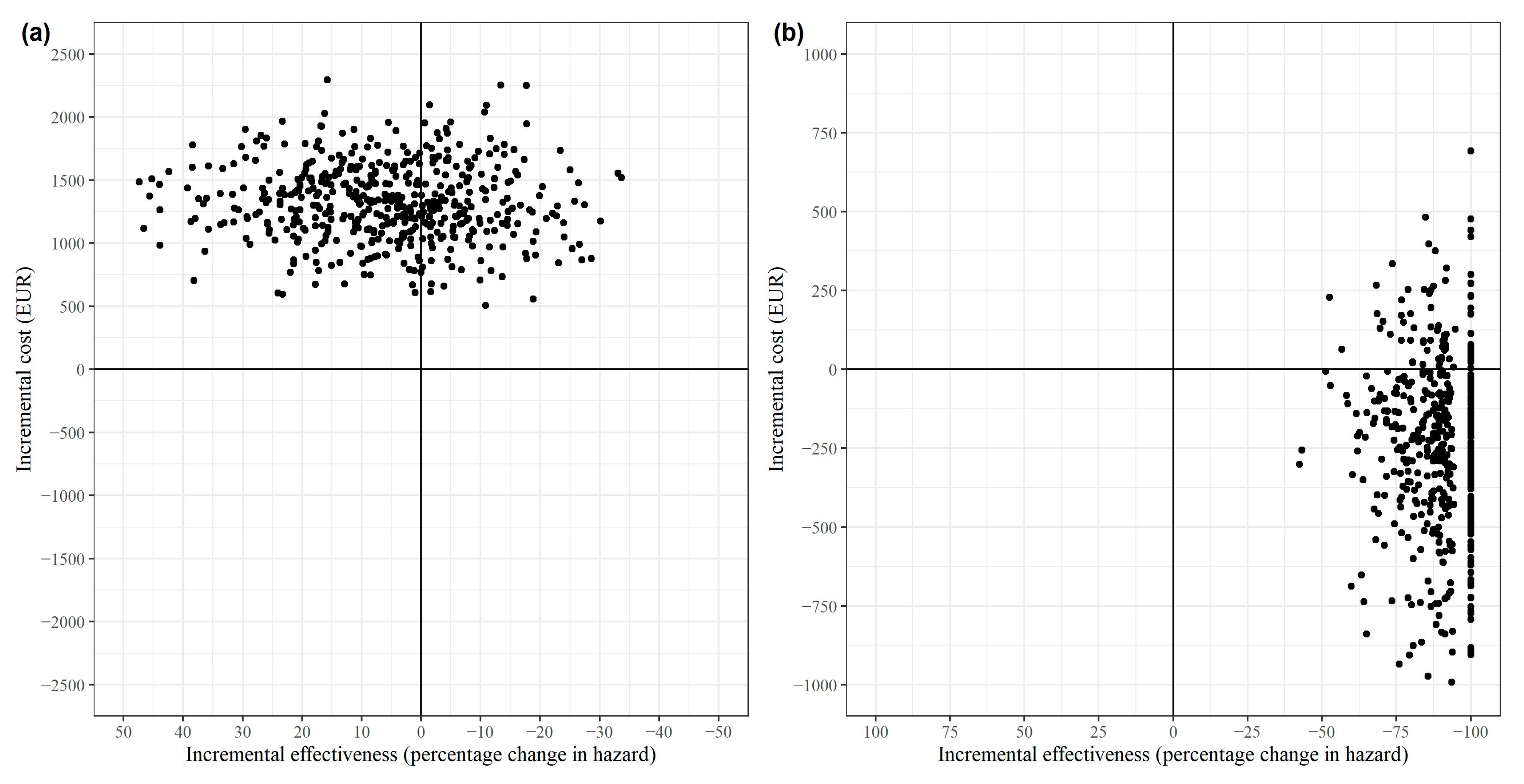
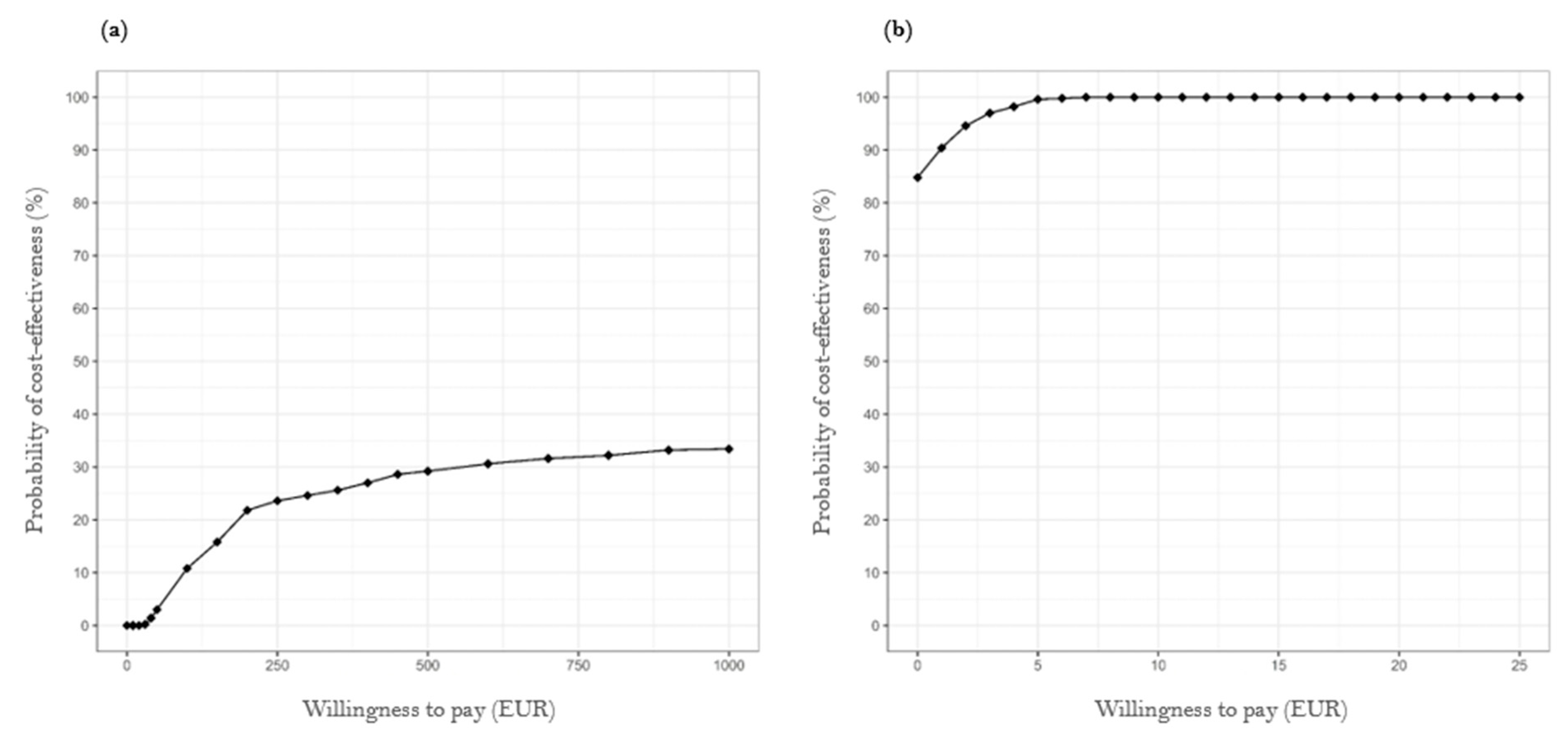
3.4.2. Probabilistic Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Regression Coefficient (ß) | SE | 95% CI | p-Value | |||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| All stroke patients 2 | Intercept | 8.3634 | 0.1117 | 8.1446 | 8.5822 | <0.0001 |
| Age | −0.013 | 0.0015 | −0.0159 | −0.0101 | <0.0001 | |
| Type of stroke 1: | ||||||
| I60 | −0.1702 | 0.574 | −1.2952 | 0.9548 | 0.7668 | |
| I61 | 0.2827 | 0.1114 | 0.0644 | 0.501 | 0.0112 | |
| I63 | 0.4195 | 0.05 | 0.3215 | 0.5175 | <0.0001 | |
| Direct costs in the previous year | <0.001 | <0.001 | <0.001 | <0.001 | <0.0001 | |
| Physician contacts in the previous year (outpatient) | 0.0137 | 0.0017 | 0.0105 | 0.0169 | <0.0001 | |
| Diabetes mellitus | 0.152 | 0.041 | 0.0716 | 0.2324 | 0.0002 | |
| Index LOS | 0.03 | 0.0025 | 0.025 | 0.035 | <0.0001 | |
| Intervention | 0.2802 | 0.0339 | 0.2138 | 0.3466 | <0.0001 | |
| Subgroup of TIA patients 3 | Intercept | 6.7568 | 0.2576 | 6.252 | 7.2617 | <0.0001 |
| Age | 0.0089 | 0.0037 | 0.0017 | 0.0162 | 0.0158 | |
| Direct costs in the previous year | 0.0001 | <0.0001 | 0.0001 | 0.0001 | <0.0001 | |
| Hospital days in the previous year | −12.4399 | 3.9124 | −20.1081 | −4.7716 | 0.0015 | |
| Physicians contacts in the previous year (outpatient) | 0.0165 | 0.004 | 0.0087 | 0.0243 | <0.0001 | |
| Myocardial infarction | 0.7811 | 0.3969 | 0.0031 | 1.5591 | 0.0495 | |
| Diabetes mellitus | 0.1896 | 0.1023 | −0.011 | 0.3902 | 0.0644 | |
| COPD | 0.2156 | 0.1359 | −0.0508 | 0.4819 | 0.1132 | |
| Intervention | 0.2381 | 0.0824 | 0.0766 | 0.3996 | 0.004 | |
Appendix B
Appendix C

References
- Peng, S.; Liu, X.; Cao, W.; Liu, Y.; Liu, Y.; Wang, W.; Zhang, T.; Guan, X.; Tang, J.; Zhang, Q. Global, regional, and national time trends in mortality for stroke, 1990–2019: An age-period-cohort analysis for the global burden of disease 2019 study and implications for stroke prevention. Int. J. Cardiol. 2023, 383, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J. Stroke. Lancet 2017, 389, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Carod-Artal, F.J.; Egido, J.A. Quality of life after stroke: The importance of a good recovery. Cerebrovasc. Dis. 2009, 27 (Suppl. S1), 204–214. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, J.H.; Bohmann, F.O.; Lieschke, F.; Misselwitz, B.; Foerch, C. Divergence and Convergence of Sex-Specific Time Trends in Ischemic Stroke: 10-Year Analysis of a State-Wide Registry in Germany. J. Am. Heart Assoc. 2022, 11, e027130. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, C.; Schmidt, H.L.; Kranaster, L.; Alonso, A. Impact of psychiatric comorbidity on the severity, short-term functional outcome, and psychiatric complications after acute stroke. Neuropsychiatr. Dis. Treat. 2019, 15, 1823–1831. [Google Scholar] [CrossRef]
- Schwarzbach, C.J.; Grau, A.J. Komplikationen nach Schlaganfall: Klinische Herausforderungen in der Schlaganfallnachsorge. Nervenarzt 2020, 91, 920–925. [Google Scholar] [CrossRef]
- Khanevski, A.N.; Bjerkreim, A.T.; Novotny, V.; Naess, H.; Thomassen, L.; Logallo, N.; Kvistad, C.E. Recurrent ischemic stroke: Incidence, predictors, and impact on mortality. Acta Neurol. Scand. 2019, 140, 3–8. [Google Scholar] [CrossRef]
- Schmid, T. Costs of treating cardiovascular events in Germany: A systematic literature review. Health Econ. Rev. 2015, 5, 27. [Google Scholar] [CrossRef] [PubMed]
- Düvel, J.A.; Damm, O.; Greiner, W. Die Kosten des Schlaganfalls in Deutschland: Eine systematische Übersichtsarbeit. Gesundheitsökonomie Qual. 2021, 26, 40–50. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Violato, M.; Candio, P.; Leal, J. Economic burden of stroke across Europe: A population-based cost analysis. Eur. Stroke J. 2020, 5, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut. Wie Steht es um Unsere Gesundheit? Robert Koch-Institut: Berlin, Germany, 2015. [CrossRef]
- Leal, J.; Luengo-Fernández, R.; Gray, A.; Petersen, S.; Rayner, M. Economic burden of cardiovascular diseases in the enlarged European Union. Eur. Heart J. 2006, 27, 1610–1619. [Google Scholar] [CrossRef] [PubMed]
- Stevens, E.; Emmett, E.; Wang, Y.; McKevitt, C.; Wolfe, C. The Burden of Stroke in Europe. Available online: http://strokeeurope.eu/ (accessed on 6 October 2023).
- Ritter, M.; Dittrich, R.; Busse, O.; Nabavi, D.; Ringelstein, E. Zukünftige Versorgungskonzepte des Schlaganfalls. Aktuelle Neurol. 2012, 39, 27–32. [Google Scholar] [CrossRef]
- Carot-sans, G.; Vela, E.; Plaza, A.; Contel, J.C.; Salvat-Plana, M.; Fabà, M.; Giralt, A.; Ribera, A.; Santaeugènia, S.; Piera-Jiménez, J. Effectiveness of an integrated care program for intensive home care services after discharge of stroke patients. Int. J. Integr. Care 2022, 22, 280. [Google Scholar] [CrossRef]
- Bodechtel, U.; Barlinn, K.; Helbig, U.; Arnold, K.; Siepmann, T.; Pallesen, L.-P.; Puetz, V.; Reichmann, H.; Schmitt, J.; Kepplinger, J. The stroke east Saxony pilot project for organized post-stroke care: A case-control study. Brain Behav. 2016, 6, e00455. [Google Scholar] [CrossRef]
- Ogunlana, M.O.; Oyewole, O.O.; Fafolahan, A.; Govender, P. Exploring community reintegration among Nigerian stroke survivors. S. Afr. J. Physiother. 2023, 79, 1857. [Google Scholar] [CrossRef]
- Abdul Aziz, A.F.; Mohd Nordin, N.A.; Muhd Nur, A.; Sulong, S.; Aljunid, S.M. The integrated care pathway for managing post stroke patients (iCaPPS©) in public primary care Healthcentres in Malaysia: Impact on quality adjusted life years (QALYs) and cost effectiveness analysis. BMC Geriatr. 2020, 20, 70. [Google Scholar] [CrossRef]
- Phillips-Harris, C. The Integration of Primary Care and Case Management in Chronic Disease. Qual. Manag. Health Care 1996, 5, 1–6. [Google Scholar] [CrossRef]
- Holloway, F.; Carson, J. Case management: An update. Int. J. Soc. Psychiatry 2001, 47, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Lukersmith, S.; Millington, M.; Salvador-Carulla, L. What Is Case Management? A Scoping and Mapping Review. Int. J. Integr. Care 2016, 16, 2. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Care und Case Management. Standards und Richtlinien für die Weiterbildung Case Management im Sozial- und Gesundheitswesen und in der Beschäftigungsförderung. 2019. Available online: https://www.dgcc.de/wp-content/uploads/2020/09/Standards-und-Richtlinien-fuer-die-Weiterbildung.pdf (accessed on 6 October 2023).
- German Stroke Foundation. Report on the Results STROKE OWL. 2023. Available online: https://innovationsfonds.g-ba.de/downloads/beschluss-dokumente/371/2023-02-23_STROKE%20OWL_Ergebnisbericht.pdf (accessed on 25 April 2023).
- King, G.; Nielsen, R. Why Propensity Scores Should Not Be Used for Matching. Political Anal. 2019, 27, 435–454. [Google Scholar] [CrossRef]
- Rubin, D.B. The Use of Matched Sampling and Regression Adjustment to Remove Bias in Observational Studies. Biometrics 1973, 29, 185. [Google Scholar] [CrossRef]
- Stuart, E.A.; Green, K.M. Using full matching to estimate causal effects in nonexperimental studies: Examining the relationship between adolescent marijuana use and adult outcomes. Dev. Psychol. 2008, 44, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Ripollone, J.E.; Huybrechts, K.F.; Rothman, K.J.; Ferguson, R.E.; Franklin, J.M. Evaluating the Utility of Coarsened Exact Matching for Pharmacoepidemiology Using Real and Simulated Claims Data. Am. J. Epidemiol. 2020, 189, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Link, S. Long-term care reform in Germany—At long last. Br. Actuar. J. 2019, 24, e17. [Google Scholar] [CrossRef]
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: Updated reporting guidance for health economic evaluations. BMC Med. 2022, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Greiner, W.; Damm, O. 3 Die Berechnung von Kosten und Nutzen. In Gesundheitsökonomische Evaluationen; Schöffski, O., von der Schulenburg, J.-M.G., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 23–42. ISBN 978-3-642-21700-5. [Google Scholar]
- Statistisches Bundesamt. Volkswirtschaftliche Gesamtrechnungen: Wichtige Zusammenhänge im Überblick 2021; Statistisches Bundesamt: Wiesbaden, Germany, 2022. Available online: https://www.destatis.de/DE/Themen/Wirtschaft/Volkswirtschaftliche-Gesamtrechnungen-Inlandsprodukt/Publikationen/Downloads-Inlandsprodukt/zusammenhaenge-pdf-0310100.html (accessed on 6 July 2022).
- Schwahn, F.; Mai, C.-M.; Braig, M. Arbeitsmarkt im Wandel—Wirtschaftsstrukturen, Erwerbsformen und Digitalisierung. In WISTA 3/2018: Wirtschaft und Statistik; Statistisches Bundesamt: Wiesbaden, Germany, 2018; pp. 24–39. ISBN 978-3-8246-1070-9. [Google Scholar]
- Hoyer, C.; Ebert, A.; Huttner, H.B.; Puetz, V.; Kallmünzer, B.; Barlinn, K.; Haverkamp, C.; Harloff, A.; Brich, J.; Platten, M.; et al. Acute Stroke in Times of the COVID-19 Pandemic: A Multicenter Study. Stroke 2020, 51, 2224–2227. [Google Scholar] [CrossRef]
- Kim, Y.; Gordon, A.; Rowerdink, K.; Herrera Scott, L.; Chi, W. The Impact of the COVID-19 Pandemic on Health Care Utilization Among Insured Individuals with Common Chronic Conditions. Med. Care 2022, 60, 673–679. [Google Scholar] [CrossRef]
- Bambha, K.; Kim, W.R. Cost-effectiveness analysis and incremental cost-effectiveness ratios: Uses and pitfalls. Eur. J. Gastroenterol. Hepatol. 2004, 16, 519–526. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes, 4th ed.; Oxford University Press: Oxford, UK; New York, NY, USA, 2015; ISBN 9780199665884. [Google Scholar]
- Paulden, M. Calculating and Interpreting ICERs and Net Benefit. Pharmacoeconomics 2020, 38, 785–807. [Google Scholar] [CrossRef] [PubMed]
- Glick, H.A.; Briggs, A.H.; Polsky, D. Quantifying stochastic uncertainty and presenting results of cost-effectiveness analyses. Expert Rev. Pharmacoecon. Outcomes Res. 2001, 1, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Schöffski, O.; Schumann, A.; Kuhlmann, A.; Schwarzbach, C. 6 Das Schwellenwertkonzept: Theorie sowie Umsetzung beim IQWiG und anderen Institutionen. In Gesundheitsökonomische Evaluationen; Schöffski, O., von der Schulenburg, J.-M.G., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 111–153. ISBN 978-3-642-21699-2. [Google Scholar]
- Duevel, J.A.; Elkenkamp, S.; Gensorowsky, D.; Brinkmeier, M.; Galle, G.; Miethe, J.; Greiner, W. A case management intervention in stroke care: Evaluation of a quasi-experimental study. Z. Evidenz Fortbild. Qual. Gesundheitswesen 2024, in press. [Google Scholar] [CrossRef]
- Stokes, J.; Panagioti, M.; Alam, R.; Checkland, K.; Cheraghi-Sohi, S.; Bower, P. Effectiveness of Case Management for ‘At Risk’ Patients in Primary Care: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0132340. [Google Scholar] [CrossRef] [PubMed]
- Schwarzbach, C.J.; Eichner, F.A.; Rücker, V.; Hofmann, A.-L.; Keller, M.; Audebert, H.J.; von Bandemer, S.; Engelter, S.T.; Geis, D.; Gröschel, K.; et al. The structured ambulatory post-stroke care program for outpatient aftercare in patients with ischaemic stroke in Germany (SANO): An open-label, cluster-randomised controlled trial. Lancet Neurol. 2023, 22, 787–799. [Google Scholar] [CrossRef] [PubMed]
- Guzauskas, G.F.; Boudreau, D.M.; Villa, K.F.; Levine, S.R.; Veenstra, D.L. The cost-effectiveness of primary stroke centers for acute stroke care. Stroke 2012, 43, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Earnshaw, S.R.; Wilson, M.; Mauskopf, J.; Joshi, A.V. Model-based cost-effectiveness analyses for the treatment of acute stroke events: A review and summary of challenges. Value Health 2009, 12, 507–520. [Google Scholar] [CrossRef]
- Briggs, A.H. Handling uncertainty in cost-effectiveness models. Pharmacoeconomics 2000, 17, 479–500. [Google Scholar] [CrossRef]
- Gray, A.M.; Clarke, P.M.; Wolstenholme, J.; Wordsworth, S. Applied Methods of Cost-Effectiveness Analysis in Health Care; Oxford Univ. Press: Oxford, UK, 2011; ISBN 978-0199227280. [Google Scholar]
- Lawrence, D.B. The Economic Value of Information; Springer: New York, NY, USA, 1999; ISBN 9781461214601. [Google Scholar]
- Claxton, K.P.; Sculpher, M.J. Using value of information analysis to prioritise health research: Some lessons from recent UK experience. Pharmacoeconomics 2006, 24, 1055–1068. [Google Scholar] [CrossRef]
| Criteria | Inclusion | Exclusion |
|---|---|---|
| CVD history | Initial stroke or TIA | Previous stroke |
| Age at study enrollment | ≥18 years | <18 years |
| Initial mRS | 0–4 | >4 |
| Long-term-care grade 1 | 0–3 | >3 |
| Previous living conditions | Previous residential care in a nursing home | |
| Residence | Within the selected regions | Outside the selected regions |
| Insurance | Ongoing membership in one of the participating 2 SHI companies | Membership of another SHI or private health insurance |
| Serious comorbidities (ICD-10 code) | C00-C97 (malignant neoplasms) G30 (Alzheimer disease) G31 (other degenerative diseases of the nervous system, not elsewhere classified) F00-F09 (organic, including symptomatic, mental disorders) F10-F19 3 (mental and behavioral disorders due to psychoactive substance use) F20-F29 (schizophrenia, schizotypal, and delusional disorders) F30 (manic episode) F31 (bipolar affective disorder) |
| Cost Component | Unit |
|---|---|
| Inpatient care | Number of hospital stays |
| Rehabilitation | Number of outpatient and/or inpatient rehabilitation stays |
| Outpatient medical care | Number of physician consultations |
| Pharmaceuticals | Number of daily defined doses |
| Therapeutic services and medical devices | Number of items |
| Sick leave | Number of sick leave days |
| Inpatient long-term care and home nursing | Number of prescribed services |
| Intervention costs | Average number of invoiced modules |
| Modules | Services Provided per Patient 1 Mean (SD) | Costs per Service in EUR Mean (SD) |
|---|---|---|
| Basic service package (invoiced quarterly) | 3.84 (0.59) | 126.71 (19.38) |
| Enrollment and assessment | 1 (0) | 99.00 (0) |
| Rehabilitation visit | 0.63 (0.48) | 73.06 (55.71) |
| Reassessment/monitoring (face-to-face) | 0.98 (0.60) | 103.00 (62.72) |
| Additional contact (by phone) | 2.30 (1.18) | 113.87 (58.51) |
| Completion of contact | 1 (0) | 33.00 (33.00) |
| Determination of need for neuropsychological treatment | 0.07 (0.25) | 3.41 (12.53) |
| Full intervention | 552.05 (117.78) |
| Type of Healthcare | Control Group Mean (SD) | Intervention Group Mean (SD) |
|---|---|---|
| Inpatient care | 1.01 (0.99) | 0.88 (1.14) |
| Outpatient medical care | 12.24 (12.59) | 14.05 (6.44) |
| Pharmaceuticals | 2348.27 (2469.47) | 2434.22 (1243.01) |
| Therapeutic services | 16.46 (31.65) | 22.15 (41.65) |
| Medical devices | 4.36 (6.84) | 3.94 (6.45) |
| Sick leave | 0.46 (1.61) | 0.53 (2.20) |
| Intervention modules | n.a. | 9.83 (1.81) |
| Rehabilitation 1 | 0.51 (0.58) | 0.76 (0.66) |
| Residential nursing care 1 | 6.63 (8.04) | 5.73 (10.88) |
| Home nursing care 1 | 2.86 (18.22) | 1.93 (20.00) |
| Cost Components | Control Group Mean (SD) | Intervention Group Mean (SD) | SE | p-Value |
|---|---|---|---|---|
| Total direct costs | 9554.56 (12,107.10) | 10,600.62 (11,024.82) | 405.27 | <0.0001 |
| Inpatient care | 4351.08 (9100.98) | 3929.56 (7759.13) | 219.78 | 0.0511 |
| Outpatient care | 967.98 (1182.78) | 1030.52 (1207.91) | 42.87 | 0.0003 |
| Pharmaceuticals | 1231.56 (1907.69) | 1210.93 (2285.85) | 77.94 | 0.9948 |
| Therapeutic services | 779.75 (1482.07) | 1153.47 (1741.06) | 59.63 | <0.0001 |
| Medical devices | 488.54 (1282.11) | 442.85 (1049.18) | 40.06 | 0.5715 |
| Sick leave | 1735.65 (5595.85) | 2281.24 (6103.04) | 212.83 | <0.0001 |
| Intervention | n.a. | 552.05 (117.78) | n.a. | n.a. |
| Rehabilitation 1 | 2028.64 (4018.98) | 2713.15 (3836.87) | 138.92 | <0.0001 |
| Residential nursing care 1 | 3039.56 (45,157.71) | 1826.04 (4069.23) | 877.27 | 0.3208 |
| Home nursing care 1 | 458.30 (3043.10) | 313.13 (1277.40) | 70.03 | 0.0874 |
| Productivity losses | 1389.07 (3776.01) | 1741.09 (4244.00) | 146.89 | 0.0548 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duevel, J.A.; Gruhn, S.; Grosser, J.; Elkenkamp, S.; Greiner, W. Secondary Prevention via Case Managers in Stroke Patients: A Cost-Effectiveness Analysis of Claims Data from German Statutory Health Insurance Providers. Healthcare 2024, 12, 1157. https://doi.org/10.3390/healthcare12111157
Duevel JA, Gruhn S, Grosser J, Elkenkamp S, Greiner W. Secondary Prevention via Case Managers in Stroke Patients: A Cost-Effectiveness Analysis of Claims Data from German Statutory Health Insurance Providers. Healthcare. 2024; 12(11):1157. https://doi.org/10.3390/healthcare12111157
Chicago/Turabian StyleDuevel, Juliane A., Sebastian Gruhn, John Grosser, Svenja Elkenkamp, and Wolfgang Greiner. 2024. "Secondary Prevention via Case Managers in Stroke Patients: A Cost-Effectiveness Analysis of Claims Data from German Statutory Health Insurance Providers" Healthcare 12, no. 11: 1157. https://doi.org/10.3390/healthcare12111157
APA StyleDuevel, J. A., Gruhn, S., Grosser, J., Elkenkamp, S., & Greiner, W. (2024). Secondary Prevention via Case Managers in Stroke Patients: A Cost-Effectiveness Analysis of Claims Data from German Statutory Health Insurance Providers. Healthcare, 12(11), 1157. https://doi.org/10.3390/healthcare12111157