
Primary Healthcare Case Management Nurses and Assistance Provided to Chronic Patients: A Narrative Review



Abstract
1. Introduction
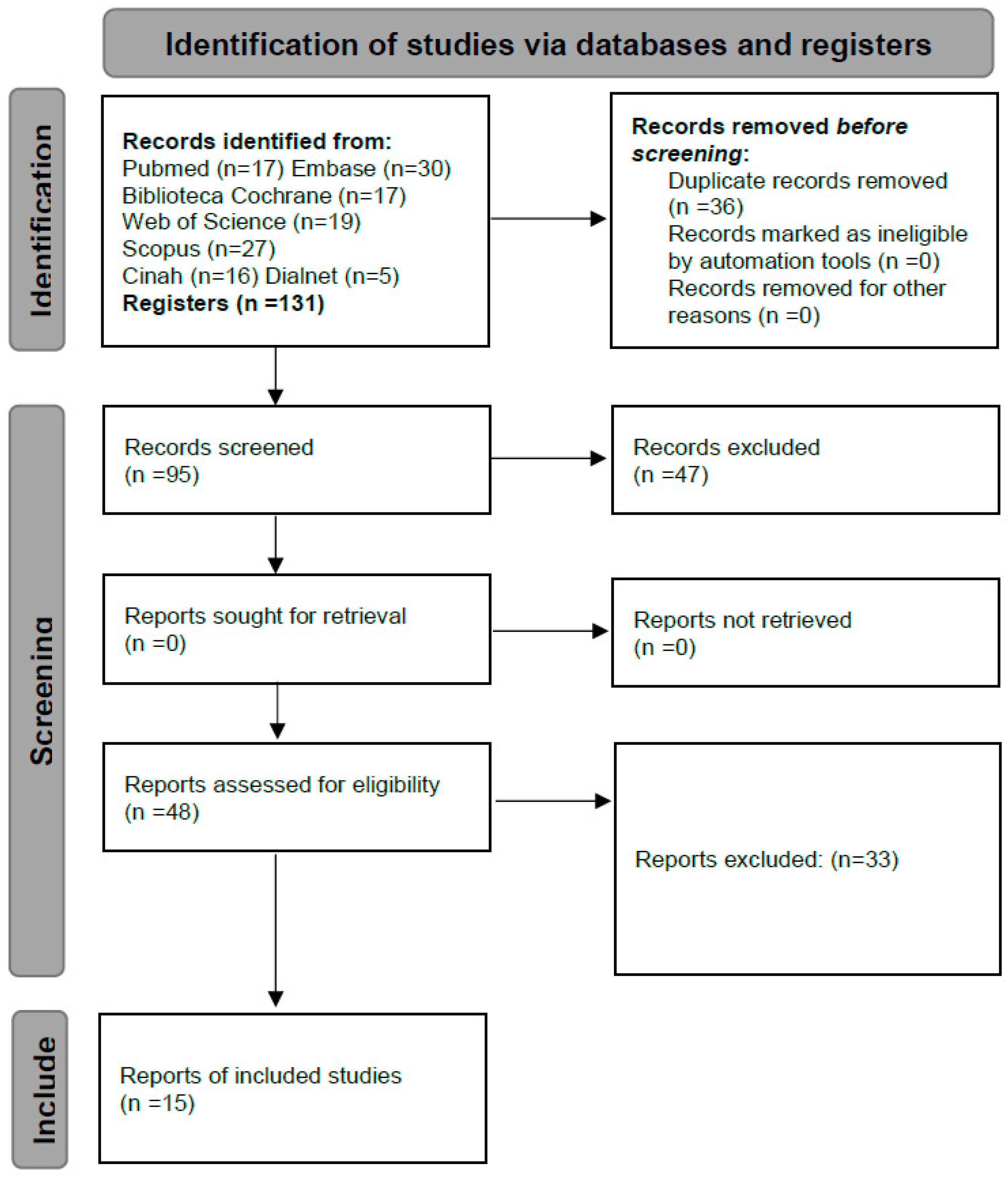
2. Materials and Methods
3. Results
3.1. Characteristics of the Studies
3.2. Assistance Provided by CMNs to Chronic Patients and Caregivers in PHC
3.3. CMNs’ Competencies and Effectiveness
4. Discussion
4.1. Assistance Provided by CMNs to Chronic Patients and Caregivers in PHC
4.2. CMNs’ Competencies and Effectiveness
4.3. Opportunities and Barriers
4.4. Added Value of this Study
4.5. Areas for Research Expansion and Suggestions for Future Developments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arjona, C.R.; Criado, J.; Sánchez, L. Enfermedades crónicas y consumo de fármacos en mayores de 65 años. Med. Gen. 2002, 47, 684–695. Available online: https://semg.info/mgyf/medicinageneral/revista_47/pdf/684-695.pdf (accessed on 20 February 2022).
- Abades, M.; Rayón, E. Aging in Spain: A challenge or social problem? Gerokomos 2012, 23, 151–155. [Google Scholar] [CrossRef]
- Morales, A.; Aguilar, J.M.; Padilla, D.; Rocamora, P.; López, R. Consumo farmacológico y salud en personas mayors. Int. J. Dev. Educ. Psychol. 2018, 4, 235. Available online: https://www.redalyc.org/journal/3498/349857603023/349857603023.pdf (accessed on 1 March 2022).
- World Health Organization. ICD-11 2022 Release. 2022. Available online: https://www.who.int/es/news/item/11-02-2022-icd-11-2022-release (accessed on 22 February 2022).
- Robledo, R.; Escobar, F.A. Las Enfermedades Crónicas no Transmisibles en Colombia. Universidad Nacional de Colombia, Facultad de Medicina. 2010. Available online: https://repositorio.unal.edu.co/handle/unal/31438 (accessed on 2 March 2022).
- Riera, L. El etiquetado de pacientes en atención primaria. El caso de la cronicidad. Aten. Prim. 2017, 49, 508–509. [Google Scholar] [CrossRef] [PubMed]
- Miguélez, A.; Casado, M.I.; Company, M.C.; Balboa, E.; Font, M.A.; Román, I. Advanced practice in case management: An essential element in the new complex chronicity care model. Enferm. Clín. 2019, 29, 99–106. [Google Scholar] [CrossRef]
- Viña, M.; Román, I. The role of the geriatric nurse specialist as a key response in the care of the elderly, chronicity, complex chronicity and its consequences on dependence. Enferm. Clín. 2019, 29, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Contel, J.C.; Muntané, B.; Camp, L. La atención al paciente crónico en situación de complejidad: El reto de construir un escenario de atención integrada. Aten. Prim. 2012, 44, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Flores, B.; Aceituno, J. Planes de prevención de enfermedades crónicas no transmisibles en niños y adolescentes. Rev. Pediatr. Aten. Prim. 2021, 23, 143–153. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1139-76322021000200006 (accessed on 15 June 2022).
- Bruins, M.J.; Van Dael, P.; Eggersdorfer, M. The Role of Nutrients in Reducing the Risk for Noncommunicable Diseases During Aging. Nutrients 2019, 11, 85. [Google Scholar] [CrossRef]
- Capodaglio, E.M. Physical activity, tool for the prevention and management of chronic diseases. G. Ital. Med. Lav. Ergon. 2018, 40, 106–119. Available online: https://pubmed.ncbi.nlm.nih.gov/30480395/ (accessed on 10 April 2022).
- Del Brutto, O.H.; Mera, R.M.; Zambrano, M.; Del Brutto, V.J. El Proyecto de Atahualpa: Protocolo, definiciones operacionales y diseño inicial. Rev. Ecuat. Neurol. 2017, 26, 95–100. Available online: http://scielo.senescyt.gob.ec/scielo.php?script=sci_arttext&pid=S2631-25812017000100095 (accessed on 25 April 2022).
- Morales-Asencio, J.M.; Martin-Santos, F.J.; Morilla-Herrera, J.C.; Fernández-Gallego, M.C.; Celdrán-Mañas, M.; Navarro-Moya, F.J.; Rodríguez-Salvador, M.M.; Muñoz-Ronda, F.J.; Gonzalo-Jiménez, E.; Carrasco, A.M. Design of a case management model for people with chronic disease (Heart Failure and COPD). Phase I: Modeling and identification of the main components of the intervention through their actors: Patients and professionals (DELTA-icE-PRO Study). BMC Health Serv. Res. 2010, 10, 324. [Google Scholar] [CrossRef] [PubMed]
- Caldararo, A.M.; Graña, M.E.; López, M.; Maestre, L.; Martín, P.; Morales, I.; Nebot Fernández, C.; Pérez Casado, S.; Rico Merino, M.; Ríos Gómez, M.T. Guía de Recomendaciones Prácticas en Enfermería: Terapias Respiratorias en el Ámbito Domiciliario. Fontán G y Rico M. (Coordinadores); IM&C: Madrid, Spain, 2023; Available online: https://www.consejogeneralenfermeria.org/profesion/guias-clinicas/send/160-guias-clinicas/2579-terapias-respiratorias (accessed on 28 September 2023).
- Lafuente, N.; Fernández, S.; Rodríguez, S.; Casado, M.I.; Morales, J.M.; Ramos, A.J. Competency development of nurses in the public health system of Andalusia. Clin. Enferm. 2019, 29, 83–89. [Google Scholar] [CrossRef] [PubMed]
- López, M.; Puente, J. Institutionalization of the case management nurse in Spain. Comparative analysis of health systems of the Spanish autonomous communities. Enferm. Clín. Engl. Ed. 2019, 29, 107–118. [Google Scholar] [CrossRef]
- Prácticas Avanzadas. Servicio Andaluz de Salud. Consejería de Salud y Consumo. Junta de Andalucía. 2019. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/el-sas/planes-marco-y-estrategias/estrategia-de-cuidados-de-andalucia/practicas-avanzadas (accessed on 20 December 2022).
- Decreto 137/2002, de 30 de Abril, de Apoyo a las Familias Andaluzas. Boletín Oficial de la Junta de Andalucía, Número 52 de 04/05/2002. Available online: https://www.juntadeandalucia.es/boja/2002/52/1 (accessed on 22 October 2022).
- Casado, M.I.; Cuevas, M.; González, F.; Martín, F.J.; Morillas, J.C.; Perteguer, I.; Toral, I.; Modelo de Gestión de Casos del Servicio Andaluz de Salud. Guía de Reorientación de las Prácticas Profesionales de la Gestión de Casos en el Servicio Andaluz de Salud. 2017. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/sites/default/files/sincfiles/wsas-media-pdf_publicacion/2021/mgc_modelo_gestion_casos.pdf (accessed on 10 March 2023).
- Schober, M.; Lehwaldt, D.; Rogers, M.; Steinke, M.; Turale, S.; Pulcini, J.; Rousse, J.; Stewart, D. Directrices de Enfermería de Práctica Avanzada 2020. Consejo Internacional de Enfermeras. 2020. Available online: https://www.icn.ch/system/files/documents/2020-04/ICN_APN%20Report_ES_WEB.pdf (accessed on 30 November 2022).
- Feyereisen, S.; Puro, N.; Thomas, C.; McConnell, W. A new kind of gatekeeper: The increasing prevalence of Advanced Practice Nurses as case managers in US hospitals. Health 2021, 25, 596–612. [Google Scholar] [CrossRef] [PubMed]
- Sastre, P.; Morales, J.M.; Sesé, A.; Bennasar, M.; Fernández, J.C.; De Pedro, J. Advanced Practice Nursing Competency Assessment Instrument (APNCAI): Clinimetric validation. BMJ Open 2017, 7, e013659. [Google Scholar] [CrossRef] [PubMed]
- Estrategia Atención Primaria. Plan Estratégico 2020–2022.Servicio Andaluz de Salud. Consejería de Salud y Consumo. 2020. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/el-sas/planes-marco-y-estrategias/estrategia-atencion-primaria-plan-estrategico-2020-2022 (accessed on 10 June 2023).
- Higgins, J.; Thomas, J.; Cochrane Handbook for Systematic Reviews of Interventions. 22 August 2023. Available online: https://training.cochrane.org/handbook (accessed on 11 October 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Del Pino, R.; Frías, A.; Palomino, P.A. La revisión sistemática cuantitativa en enfermería. Rev. Iberoam. Enferm. Comunitaria 2014, 7, 24–40. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=6336945 (accessed on 5 September 2022).
- Hudon, C.; Chouinard, M.C.; Dubois, M.F.; Roberge, P.; Loignon, C.; Tchouaket, É.; Lambert, M.; Hudon, É.; Diadiou, F.; Bouliane, D. Case Management in Primary Care for Frequent Users of Health Care Services: A Mixed Methods Study. Ann. Fam. Med. 2018, 16, 232–239. [Google Scholar] [CrossRef]
- Askerud, A.; Conder, J. Patients’ experiences of nurse case management in primary care: A meta-synthesis. Aust. J. Prim. Health 2017, 23, 420–428. [Google Scholar] [CrossRef]
- Kahn, L.S.; Fox, C.H.; Carrington, J.; Desai, U.; Bartlett, D.P.; Lyle, H.; Kowalski, M. Telephonic nurse case management for patients with diabetes and mental illnesses: A qualitative perspective. Chronic Illn. 2009, 5, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Doménech-Briz, V.; Romero, R.G.; de Miguel-Montoya, I.; Juárez-Vela, R.; Martínez-Riera, J.R.; Mármol-López, M.I.; Verdeguer-Gómez, M.V.; Sánchez-Rodríguez, Á.; Gea-Caballero, V. Results of Nurse Case Management in Primary Heath Care: Bibliographic Review. Int. J. Environ. Res. Public Health 2020, 17, 9541. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, D.; Hayter, M. Structured review: Evaluating the effectiveness of nurse case managers in improving health outcomes in three major chronic diseases. J. Clin. Nurs. 2009, 18, 2978–2992. [Google Scholar] [CrossRef]
- Watts, S.A.; Lucatorto, M. A review of recent literature—Nurse case managers in diabetes care: Equivalent or better outcomes compared to primary care providers. Curr. Diab. Rep. 2014, 14, 504. [Google Scholar] [CrossRef]
- Casas, A.; Troosters, T.; Garcia-Aymerich, J.; Roca, J.; Hernández, C.; Alonso, A.; del Pozo, F.; de Toledo, P.; Antó, J.M.; Rodríguez-Roisín, R.; et al. Integrated care prevents hospitalisations for exacerbations in COPD patients. Eur. Respir. J. 2006, 28, 123–130. [Google Scholar] [CrossRef]
- Cook, C.L.; Hall, A.G.; Garvan, C.S.; Kneipp, S.M. A Public Health Nursing Model Assists Women Receiving Temporary Assistance for Needy Families Benefits to Identify a Usual Source of Primary Care. Care Manag. J. 2015, 16, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Crane, S.; Collins, L.; Hall, J.; Rochester, D.; Patch, S. Reducing utilization by uninsured frequent users of the emergency department: Combining case management and drop-in group medical appointments. J. Am. Board Fam. Med. 2012, 25, 184–191. [Google Scholar] [CrossRef]
- Gabbay, R.A.; Añel-Tiangco, R.M.; Dellasega, C.; Mauger, D.T.; Adelman, A.; Van Horn, D.H.A. Diabetes Nurse Case Management and Motivational Interviewing for Change (DYNAMIC): Results of a 2-year Randomized Controlled Pragmatic Trial. J. Diabetes 2013, 5, 349–357. [Google Scholar] [CrossRef]
- Gordon, J.B.; Colby, H.H.; Bartelt, T.; Jablonski, D.; Krauthoefer, M.L.; Havens, P. A tertiary care-primary care partnership model for medically complex and fragile children and youth with special health care needs. Arch. Pediatr. Adolesc. Med. 2007, 161, 937–944. [Google Scholar] [CrossRef]
- Lanzeta, I.; Mar, J.; Arrospide, A. Cost-utility analysis of an integrated care model for multimorbid patients based on a clinical trial. Gac. Sanit. 2016, 30, 352–358. [Google Scholar] [CrossRef]
- Mallitt, K.A.; Mcnab, J.; Hughes, R.; Fernyhough, J.; Paterson, J.; O’Halloran, D. Reducing emergency department presentations among chronically ill patients in Western Sydney: A key role for coordinated primary care. Aust. J. Prim. Health 2017, 23, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Mattei, A.T.; de Fátima, M.; Castanho, R.; Perez, J.; Molina, R. Nursing case management for people with hypertension in primary health care: A randomized controlled trial. Res. Nurs. Health 2020, 43, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Watts, S.A.; Sood, A. Diabetes nurse case management: Improving glucose control: 10 years of quality improvement follow-up data. Appl. Nurs. Res. 2016, 29, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Peña, R.; Ortego-Maté, C.; Amo-Setién, F.J.; Silió-García, T.; Casasempere-Satorres, A.; Sarabia-Cobo, C. Implementing a Care Pathway for Complex Chronic Patients from a Nursing Perspective: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 6324. [Google Scholar] [CrossRef]
- Reig-Garcia, G.; Suñer-Soler, R.; Mantas-Jiménez, S.; Bonmatí-Tomas, A.; Malagón-Aguilera, M.C.; Bosch-Farré, C.; Gelabert-Viella, S.; Juvinyà-Canal, D. Assessing Nurses Satisfaction with Continuity of Care and the Case management Model as an Indicator of Quality of Care in Spain. Int. J. Environ. Res. Public Health 2021, 18, 6609. [Google Scholar] [CrossRef]
- Gisele, K.A.; Bernardino, E.; Lapierre, J.; Dallaire, C. Activities of liaison nurses at hospital discharge: A strategy for continuity of care. Rev. Lat. Am. Enfermagem. 2019, 27, e3162. [Google Scholar] [CrossRef]

{kind=link}
| Author, Year, and Locus | Study: Type, Methodology, and Objective | Sample (N), Gender, Age, and Period | Main Findings |
|---|---|---|---|
| Hudon et al., 2018 [28] Canada | Mixed methods. Randomised controlled trial. First and second phase: qualitative and descriptive design. To assess the effects of a case management intervention for users with chronic diseases and complex needs, in relation to psychological distress. | N = 247 patients (126 in the Intervention Group and 121 in the Control Group). Age: patients aged from 18 to 80 years old and 69 key informants. From February 2013 to January 2014. | The case management intervention reduces psychological distress, enhancing patient safety. Many patients and family caregivers stated improvements in self-control ability; however, this did not translate into greater patient activation in the controlled trial. Future studies should assess the effect of a longer intervention (1 year), as this would improve self-care. |
| Askerud and Condel, 2017 [29] New Zealand | Qualitative meta-synthesis. To know the patients’ experience in relation to the assistance provided by CMNs. | N = 1052 individuals sampled. Age: 55–90 years old. | Case management in charge of nurses generated high safety and confidence levels and helped the individuals to self-manage their conditions in the long term. CMNs provided professional coordination and a long-term personal relationship, easing care continuity and preventing hospital readmissions. During the last 20 years, case management has been developed as a care model for people with long-term complex chronic conditions; it is a holistic model based on strengths. The experiences of the people treated through case management were almost universally positive and helped them improve their quality of life, fostering self-management and personal accountability. |
| Kahn et al., 2009 [30] USA | Qualitative. To identify the problems faced by patients with behavioural health and diabetes diagnoses documented by case management nurses via telephone calls. | N = 853. Majority of women. May 2008 and January 2009. | Case management nurses address countless challenges, solving behavioural health problems and other general medical conditions. They also intervene in social and health services, coordinating patients with PHC services. This study shows how, after multiple telephone calls and email messages, the patients took the initiative of calling a case-management nurse. This nurse served as a trainer, educator, counsellor, and case manager. |
| Domenech-Briz et al., 2020 [31] Spain | Bibliographic review. To know the effectiveness and efficiency of CMNs in PHC. | N = 16 related articles. January and April 2020. | The assistance provided by CMNs is more effective and efficient in relation to the traditional model. The patients assisted by CMNs improved the self-management of their disease based on knowledge, and this gave rise to improvements in quality of life. Through the CMNs, the caregivers were provided emotional and instrumental support, as well as better accessibility, whether in person, via telephone calls, or in the home environment. Only one meta-analysis reflected that there was no significant evidence in relation to mortality regarding the patients assisted by CMNs. Fewer care appointments, admissions, and readmissions. Cost reductions. Greater activation of social services. Comprehensive care, easing continuity and coordination. Increased satisfaction in patients and caregivers. CMNs are APNs: they improve chronic patients’ health. |
| Sutherland and Hayter, 2009 [32] United Kingdom | Literature review. To assess nursing case management with one or all three main long-term chronic diseases (diabetes, COPD, and coronary diseases). | N = 108 articles (18 were included). | Significantly positive results, excellent evidence in terms of effectiveness for the impact of nursing case management in five health results: objective clinical measures; quality of life and functionality; patients’ satisfaction; adherence to the treatment; self-care; and use of the services. More research studies are required to support role development and propose a more specific intervention approach. The interventions should be maintained in time for the long-term benefits to be appreciated. |
| Watts and Lucatorto, 2014 [33] Boston | Literature review. | 2000–2013. | Abundant scientific literature states improved assistance for patients with diabetes. No studies suggesting that a reduction in quality of life or safety problems were found. Several studies indicate cost analyses, but they fail to specify a comprehensive calculation of the ROI. Mandatory and continuous training is required to offer effective assistance as a CMN, as well as methods to evaluate competencies and measures for ongoing control in terms of safety and quality. CMNs are a cost-efficient resource for facing the medical care challenges inherent to the assistance currently provided for chronic diabetes. Adequate training for nurses about the management of chronic diseases is required. Skill and experience levels are also important. |
| Casas et al., 2006 [34] Spain | Quantitative. To know the efficacy of a simple, well-standardised, and integrated care intervention to prevent hospitalisations. | N = 155 patients with exacerbated COPD; 17% women. | The intervention consisted of a customised care plan shared with the PHC team, as well as access to a specialised nursing case manager through a web-based call centre. The trial shows that this intervention effectively prevents hospitalisations due to exacerbation in patients with chronic pulmonary disease. |
| Cook et al., 2015 [35] Florida | Quantitative. Controlled trial. To determine if a nursing case management intervention affected acquisition of a habitual care source. | N = 432. Women aged 18–60 years old. 2007–2009. | The nursing case management intervention was an efficient way to help women find a habitual care source, improving knowledge about health and the benefits and easing good-quality, cost-efficient, coordinated, and integrated assistance. Nurses employ a holistic approach, focusing their practice on health promotion; they helped the patients book appointments, learn how to handle chronic health conditions, and communicate medical care needs to health providers, social workers, and new employees. |
| Crane et al., 2012 [36] North Carolina | Quantitative. Randomised controlled trial with 12-month follow-up in a PHC clinic from Brazil. To examine the effectiveness of nursing case management for blood pressure control in Brazilian adults. | N = 94 (47 in the Intervention Group and 47 in the Control Group). Adults with arterial hypertension. From December 2016 to December 2017 | Nursing case management can improve the effects of the arterial hypertension management strategy used in PHC. The results showed reductions in blood pressure, waist circumference, and BMI, in addition to an improvement in adherence to the treatment. The individuals from the Intervention Group had fewer hospital admissions and lower schooling levels. This model should be tested and expanded to other chronic diseases. |
| Gabbay R., 2013 [37] USA | Quantitative. Randomised controlled trial conducted over 2 years in 12 PHC clinics. To determine if duly training CMNs in motivational interviews would provide better results in high-risk patients with type 2 diabetes. | N = 545 patients (313 in the Control Group and 232 in the Intervention Group). From August 2006 to March 2008. | The CMNs improved blood pressure and the detection of complications. Improvements were observed in HbA1C, low-density lipoproteins, and systolic blood pressure in both groups. The scores for the depressive symptoms were better in the Intervention Group. Diabetes is better controlled with an integrated and multidisciplinary approach. Care management is considered as a core characteristic and key component of quality assurance. |
| Gordon et al., 2007 [38] Wisconsin | Quantitative. Up to 3 years of data before and after the patients’ enrolment in the Special Needs program were compared. To assess the impact of a Special Needs program at a tertiary-level care centre that partners with families and PHC physicians to ensure uninterrupted in-hospital and outpatient care and help provide medical homes. | N = 227. Medically complex and frail children and young individuals, with a broad range of chronic disorders. From 1 July 2002, to June 2005. | This new association model between tertiary-level assistance and PHC was effective in improving the care provided to the patients, their health, and the cost reductions achieved. The key interventions were as follows: collaboration with the family; familiarity with the child’s pathology; close participation during the hospitalisation periods; and proactive outpatient care. The patients and families indicated an increase in their satisfaction level. |
| Lanzeta et al., 2016 [39] Spain | Quantitative. Clustered randomised clinical trial. To perform a cost–benefit analysis of an integrated care model comprising a designated Internist and a hospital Liaison Nurse for patients with multiple morbidities, when compared to a conventional reactive health system. | N = 140 patients. 70 patients in each group. It lasted 1 year: from April 2011 to February 2012. | The intervention was not efficient. The subgroup comprising patients aged less than 80 years old with at least 3 clinical categories saved 89% of the costs in the simulations. The intervention was not suitable for all patients; the subgroup analysis allowed for identifying a more specific target population that should be analysed in future studies. |
| Mallitt et al., 2016 [40] Australia | Quantitative (before and after comparison). To determine the results of the HealthOne Mount Druitt (HOMD) coordinated care program, with coordination provided by liaison nurses. | N = 125 participants. Majority of women (58.4%). 68.4 years old (from 17 to 93). | The HOMD was certainly positive: more comprehensive planning for the clients (82%); closer work links with other organisations (76%); better relationships with health workers (73%); and enhanced coordination of services for patients with multiple needs (75%). Showed qualitative evidence that a coordinated care intervention (HealthOne) improves patients’ health results. Greater integration of services, coordination, flexibility, and care continuity. Lesser use of hospital emergency services and greater access to a combination of allied health services in the community. |
| Mattei et al., 2019 [41] Brazil | Quantitative. Randomised controlled trial with 12-month follow-up in a PHC clinic from Brazil. To examine the effectiveness of nursing case management for blood pressure control in Brazilian adults. | N = 94 (47 in the Intervention Group and 47 in the Control Group). Adults with arterial hypertension. From December 2016 to December 2017. | Nursing case management can improve the effects of the arterial hypertension management strategy used in PHC. The results showed reductions in blood pressure, waist circumference, and BMI, in addition to an improvement in adherence to the treatment. The individuals from the Intervention Group had fewer hospital admissions and lower schooling levels. This model should be tested and expanded to other chronic diseases. |
| Watts and Sood, 2016 [42] USA | Quantitative. To determine the efficacy of a case management program to improve the qualifications of diabetes educators certified in case management nursing. | N = 15,636 patients during a 10-year period. From 1 July 2004, to 7 July 2014. | The intervention led by case management nurses showed a significant reduction in glycated haemoglobin. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Gil, M.J.; Guerra-Martín, M.D.; Diego-Cordero, R.D. Primary Healthcare Case Management Nurses and Assistance Provided to Chronic Patients: A Narrative Review. Healthcare 2024, 12, 1054. https://doi.org/10.3390/healthcare12111054
Molina-Gil MJ, Guerra-Martín MD, Diego-Cordero RD. Primary Healthcare Case Management Nurses and Assistance Provided to Chronic Patients: A Narrative Review. Healthcare. 2024; 12(11):1054. https://doi.org/10.3390/healthcare12111054
Chicago/Turabian StyleMolina-Gil, María José, María Dolores Guerra-Martín, and Rocío De Diego-Cordero. 2024. "Primary Healthcare Case Management Nurses and Assistance Provided to Chronic Patients: A Narrative Review" Healthcare 12, no. 11: 1054. https://doi.org/10.3390/healthcare12111054
APA StyleMolina-Gil, M. J., Guerra-Martín, M. D., & Diego-Cordero, R. D. (2024). Primary Healthcare Case Management Nurses and Assistance Provided to Chronic Patients: A Narrative Review. Healthcare, 12(11), 1054. https://doi.org/10.3390/healthcare12111054