
Neuropsychology of Generalized Anxiety Disorder in Clinical Setting: A Systematic Evaluation



Abstract
:1. Introduction
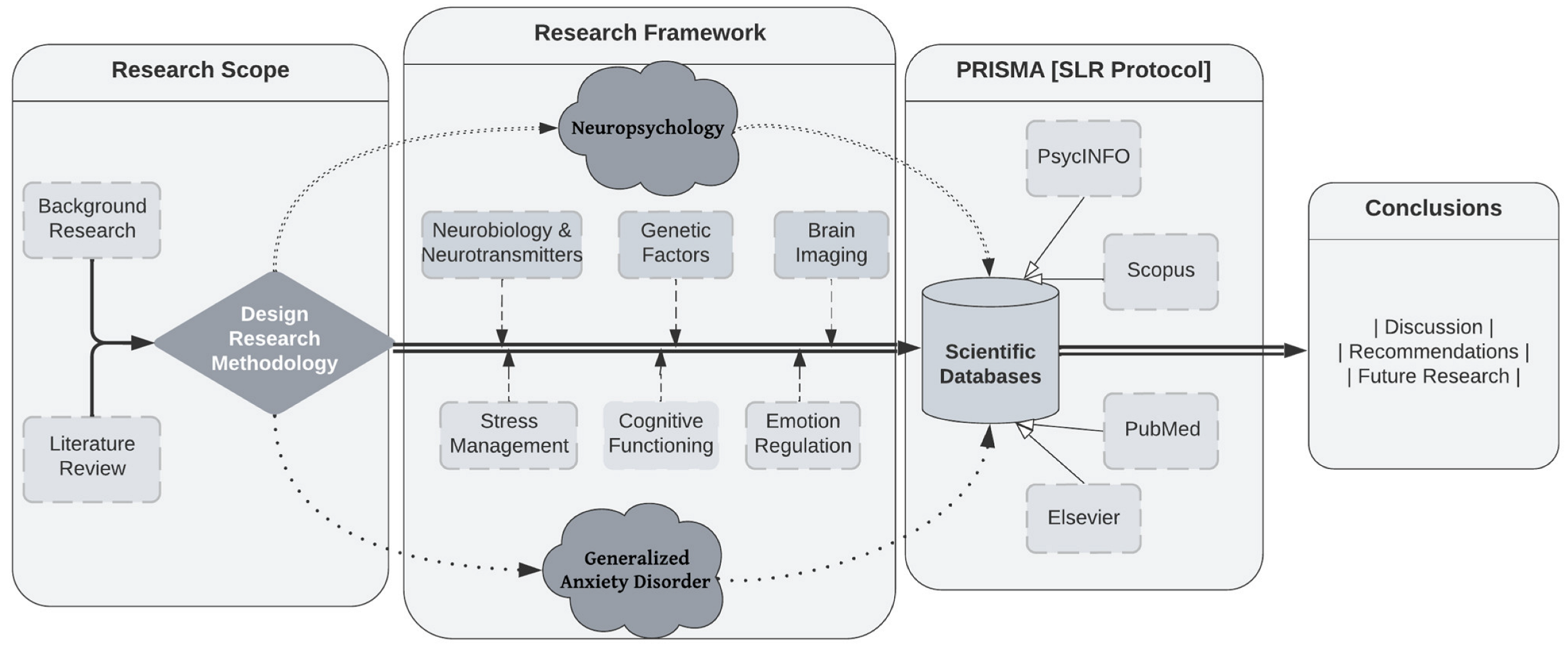
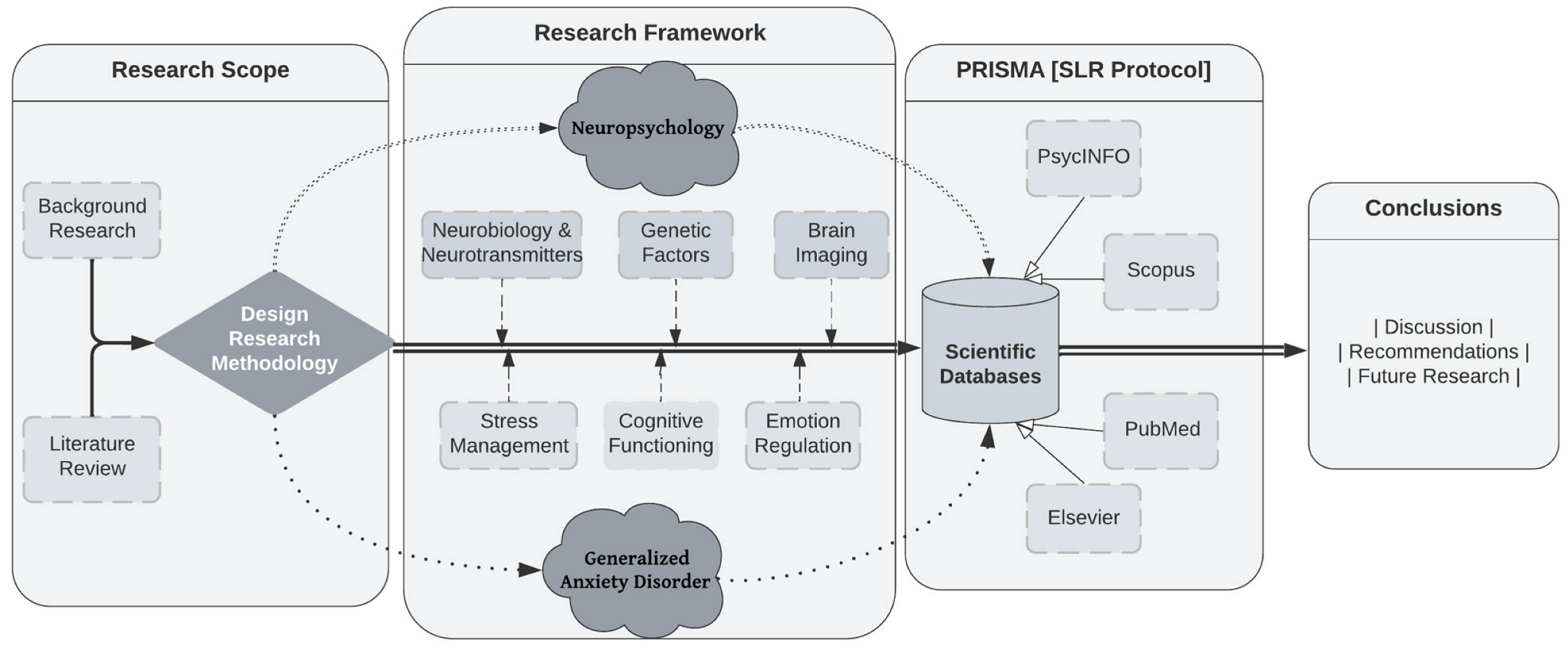
Theoretical Framework
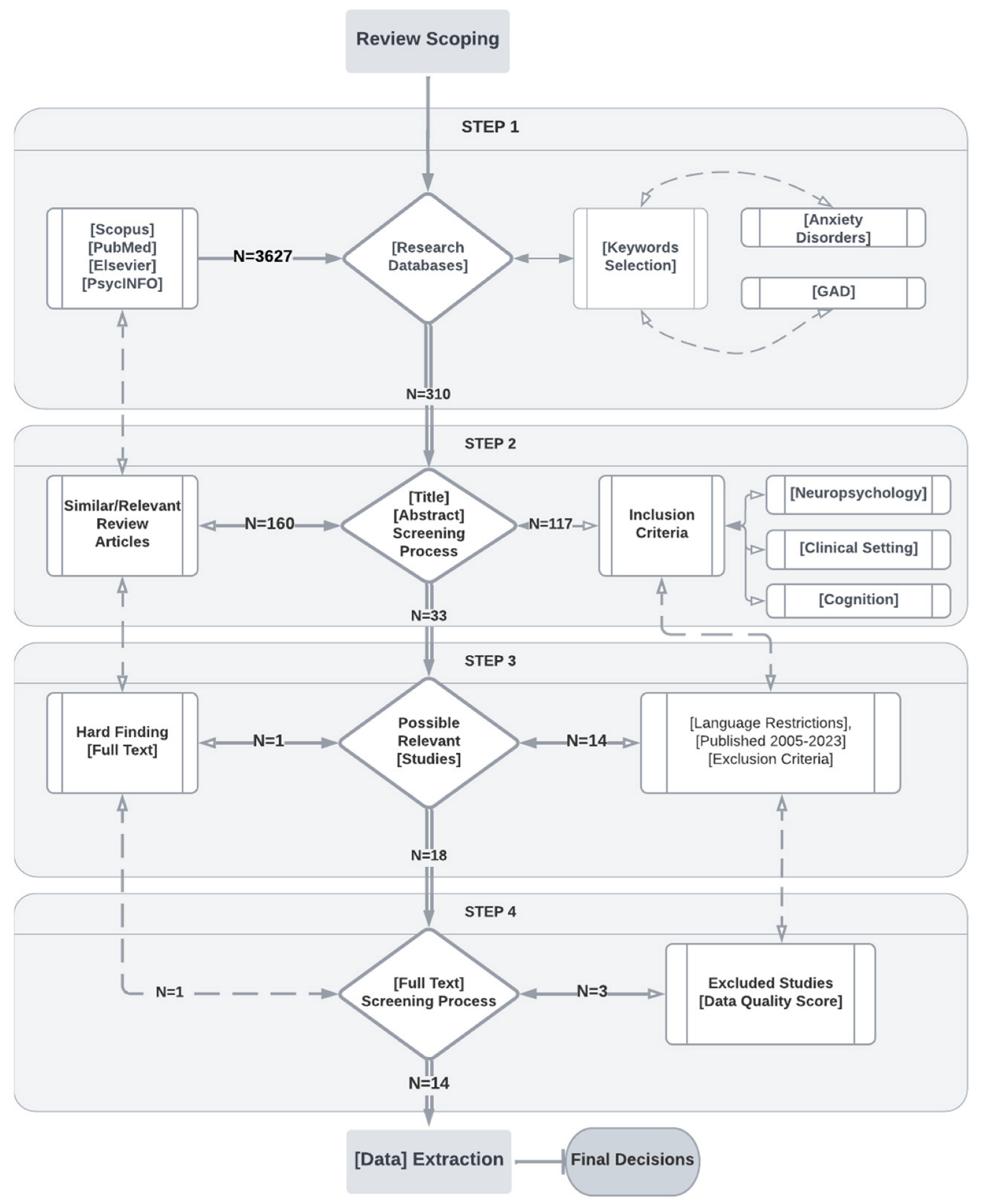
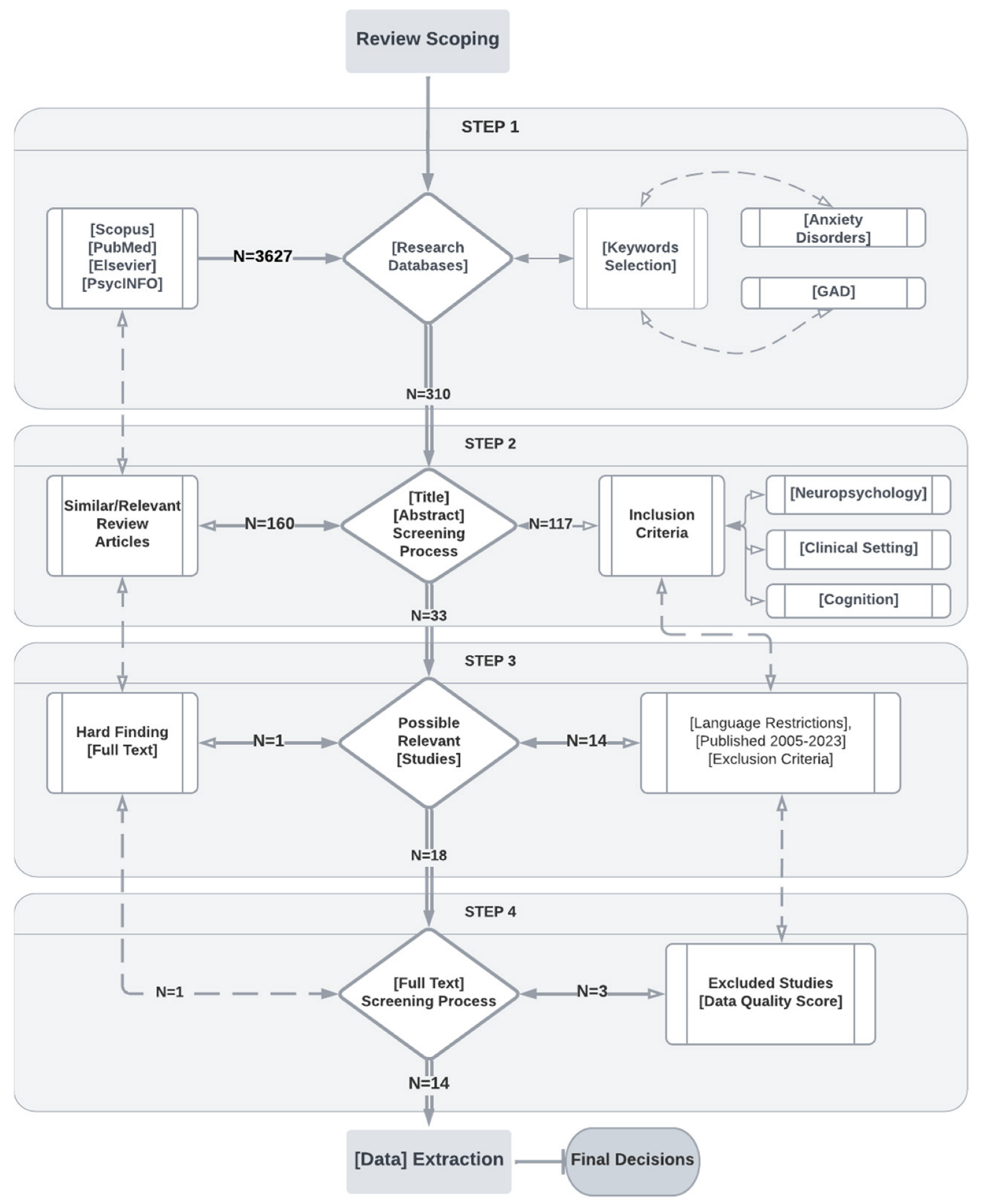
2. Materials and Methods
3. Results
3.1. Information Sources and Search Strategies
3.2. Empirical Studies
4. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Leonard, K.; Abramovitch, A. Cognitive Functions in Young Adults with Generalized Anxiety Disorder. Eur. Psychiatry 2018, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Butters, M.A.; Bhalla, R.K.; Andreescu, C.; Wetherell, J.L.; Mantella, R.C.; Begley, A.E.; Lenze, E.J. Changes in Neuropsychological Functioning Following Treatment for Late-life Generalised Anxiety Disorder. Br. J. Psychiatry 2011, 3, 211–218. [Google Scholar] [CrossRef]
- Robinson, O.J.; Vytal, K.; Cornwell, B.R.; Grillon, C. The Impact of Anxiety Upon Cognition: Perspectives from Human Threat of Shock Studies. Front. Hum. Neurosci. 2013, 7, 203. [Google Scholar] [CrossRef] [PubMed]
- Etkin, A.; Wager, T.D. Functional Neuroimaging of Anxiety: A Meta-analysis Of Emotional Processing in Ptsd, Social Anxiety Disorder, And Specific Phobia. Am. J. Psychiatry 2007, 10, 1476–1488. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Guzmán, I.; Gudayol-Ferré, E.; Jarne-Esparcia, A.; Herrera-Abarca, J.E.; Herrera-Guzmán, D.; Peró, M.; Guàrdia-Olmos, J. Comorbidity of Anxiety Disorders in Major Depressive Disorder: A Clinical Trial to Evaluate Neuropsychological Deficit. Eur. J. Psychiatry 2009, 1, 5–18. [Google Scholar] [CrossRef]
- Del Giudice, M. Generalized Anxiety Disorder. In Evolutionary Psychopathology; Oxford University Press: Oxford, UK, 2018; pp. 319–322. [Google Scholar] [CrossRef]
- Gkintoni, E.; Pallis, E.; Bitsios, P.; Giakoumaki, S. Neurocognitive performance, psychopathology and social functioning in individuals at high-genetic risk for schizophrenia and psychotic bipolar disorder. Int. J. Affect. Disord. 2017, 208, 512–520. [Google Scholar] [CrossRef] [PubMed]
- De la Peña-Arteaga, V.; Fernández-Rodríguez, M.; Silva Moreira, P.; Abreu, T.; Portugal-Nunes, C.; Soriano-Mas, C.; Picó-Pérez, M.; Sousa, N.; Ferreira, S.; Morgado, P. An fMRI study of cognitive regulation of reward processing in generalized anxiety disorder (GAD). Psychiatry Res. Neuroimaging 2022, 324, 111493. [Google Scholar] [CrossRef]
- Newman, M.G.; Zainal, N.H.; Hoyer, J. Cognitive-Behavioral Therapy (CBT) for Generalized Anxiety Disorder (GAD). In Generalized Anxiety Disorder and Worrying; Portico: Murfreesboro, TN, USA, 2020; pp. 203–230. [Google Scholar] [CrossRef]
- Gordeev, S.A.; Posokhov, S.I.; Kovrov, G.V.; Katenko, S.V. Psychophysiological characteristics of panic disorder and generalized anxiety disorder. Zhurnal Nevrol. I Psikhiatrii Im. SS Korsakova 2013, 113, 11–14. [Google Scholar]
- Hallion, L.S.; Tolin, D.F.; Assaf, M.; Goethe, J.; Diefenbach, G.J. Cognitive Control in Generalized Anxiety Disorder: Relation of Inhibition Impairments to Worry and Anxiety Severity. Cogn. Ther. Res. 2017, 41, 610–618. [Google Scholar] [CrossRef]
- Khdour, H.Y.; Abushalbaq, O.M.; Mughrabi, I.T.; Imam, A.F.; Gluck, M.A.; Herzallah, M.M.; Moustafa, A.A. Generalized Anxiety Disorder and Social Anxiety Disorder, but Not Panic Anxiety Disorder, Are Associated with Higher Sensitivity to Learning from Negative Feedback: Behavioral and Computational Investigation. Front. Integr. Neurosci. 2016, 10, 20. [Google Scholar] [CrossRef]
- Moon, C.-M.; Jeong, G.-W. Functional neuroanatomy on the working memory under emotional distraction in patients with generalized anxiety disorder. Psychiatry Clin. Neurosci. 2015, 69, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Stefanopoulou, E.; Hirsch, C.R.; Hayes, S.; Adlam, A.; Coker, S. Are attentional control resources reduced by worry in generalized anxiety disorder? J. Abnorm. Psychol. 2014, 123, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Sbicigo, J.B.; Toazza, R.; Becker, N.; Ecker, K.K.; Manfro, G.G.; Salles, J.F.D. Memory and Language Impairments Are Associated with Anxiety Disorder Severity in Childhood. Trends Psychiatry Psychother. 2020, 2, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Mogg, K.; Bradley, B.P. Attentional Bias in Generalized Anxiety Disorder Versus Depressive Disorder. Cogn. Ther. Res. 2005, 1, 29–45. [Google Scholar] [CrossRef]
- Fuglset, T.S. Is Set-shifting and Central Coherence in Anorexia Nervosa Influenced by Body Mass Index, Anxiety or Depression? A Systematic Review. BMC Psychiatry 2021, 1, 137. [Google Scholar] [CrossRef]
- Rippe, J.M. Promoting Regular Physical Activity. Increasing Phys. Act. 2020, 173–188. [Google Scholar]
- Wenzel, A. Substance/Medication-Induced Anxiety Disorder. In The SAGE Encyclopedia of Abnormal and Clinical Psychology; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar] [CrossRef]
- Chapman, A.L.; Owens, L. Mechanisms of Change in Dialectical Behavior Therapy. In The Handbook of Dialectical Behavior Therapy; Elsevier Academic Press: Amsterdam, The Netherlands, 2020; pp. 51–69. [Google Scholar] [CrossRef]
- Whittingham, K.; Coyne, L.W. Integrating Acceptance and Commitment Therapy with other interventions. In Acceptance and Commitment Therapy; Academic Press: Cambridge, MA, USA, 2019; pp. 377–402. [Google Scholar] [CrossRef]
- Portman, M.E. Pharmacotherapy for Generalized Anxiety Disorder. In Generalized Anxiety Disorder Across the Lifespan; Springer: Berlin/Heidelberg, Germany, 2009; pp. 65–84. [Google Scholar] [CrossRef]
- Aasvik, J.K.; Woodhouse, A.; Jacobsen, H.B.; Borchgrevink, P.C.; Stiles, T.C.; Landrø, N.I. Subjective memory complaints among patients on sick leave are associated with symptoms of fatigue and anxiety. Front. Psychol. 2015, 6, 1338. [Google Scholar] [CrossRef]
- Timulak, L. Generalized anxiety disorder. In Transforming Generalized Anxiety; Routledge: Abingdon, UK, 2017; pp. 8–28. [Google Scholar] [CrossRef]
- Diamanduros, T.; Tysinger, P.D.; Tysinger, J.A.; Fenning, P.A. Child and Adolescent Psychopathology for School Psychology. In Generalized Anxiety Disorder; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar] [CrossRef]
- Balderston, N.L.; Vytal, K.E.; O’Connell, K.; Torrisi, S.; Letkiewicz, A.; Ernst, M.; Grillon, C. Anxiety Patients Show Reduced Working Memory Related dlPFC Activation During Safety and Threat. Depress. Anxiety 2016, 34, 25–36. [Google Scholar] [CrossRef]
- Fitzgerald, J.M.; Phan, K.L.; Kennedy, A.E.; Shankman, S.A.; Langenecker, S.A.; Klumpp, H. Prefrontal and amygdala engagement during emotional reactivity and regulation in generalized anxiety disorder. J. Affect. Disord. 2017, 218, 398–406. [Google Scholar] [CrossRef]
- Fonzo, G.A.; Ramsawh, H.J.; Flagan, T.M.; Sullivan, S.G.; Simmons, A.N.; Paulus, M.P.; Stein, M.B. Cognitive-behavioral therapy for generalized anxiety disorder is associated with attenuation of limbic activation to threat-related facial emotions. J. Affect. Disord. 2014, 169, 76–85. [Google Scholar] [CrossRef]
- Plana, I.; Lavoie, M.-A.; Battaglia, M.; Achim, A.M. A meta-analysis and scoping review of social cognition performance in social phobia, posttraumatic stress disorder and other anxiety disorders. J. Anxiety Disord. 2014, 28, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Renna, M.E.; Seeley, S.H.; Heimberg, R.G.; Etkin, A.; Fresco, D.M.; Mennin, D.S. Increased Attention Regulation from Emotion Regulation Therapy for Generalized Anxiety Disorder. Cogn. Ther. Res. 2017, 42, 121–134. [Google Scholar] [CrossRef]
- Tempesta, D.; Mazza, M.; Serroni, N.; Moschetta, F.S.; Di Giannantonio, M.; Ferrara, M.; De Berardis, D. Neuropsychological functioning in young subjects with generalized anxiety disorder with and without pharmacotherapy. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 45, 236–241. [Google Scholar] [CrossRef] [PubMed]
- White, S.F.; Geraci, M.; Lewis, E.; Leshin, J.; Teng, C.; Averbeck, B.; Meffert, H.; Ernst, M.; Blair, J.R.; Grillon, C.; et al. Prediction Error Representation in Individuals with Generalized Anxiety Disorder During Passive Avoidance. Am. J. Psychiatry 2017, 174, 110–117. [Google Scholar] [CrossRef]
- Patel, N.; Stoodley, C.; Pine, D.S.; Grillon, C.; Ernst, M. Interaction of induced anxiety and verbal working memory: Influence of trait anxiety. Learn. Mem. 2017, 24, 407–413. [Google Scholar] [CrossRef]
- Gorka, S.M.; Lieberman, L.; Shankman, S.A.; Phan, K.L. Association between neural reactivity and startle reactivity to uncertain threat in two independent samples. Psychophysiology 2017, 54, 652–662. [Google Scholar] [CrossRef]
- Cunningham, W.A.; Kirkland, T. The joyful, yet balanced, amygdala: Moderated responses to positive but not negative stimuli in trait happiness. Soc. Cogn. Affect. Neurosci. 2013, 9, 760–766. [Google Scholar] [CrossRef]
- Ward, T.; Delrue, N.; Plagnol, A. Neuropsychotherapy as an integrative framework in counselling psychology:The example of trauma. Couns. Psychol. Rev. 2017, 32, 18–28. [Google Scholar] [CrossRef]
- Gkintoni, E.; Boutsinas, B.; Kourkoutas, E. Developmental Trauma and Neurocognition in Young Adults. In Proceedings of the 14th Annual International Conference on Education and New Learning Technologies, Mallorca, Spain, 4–6 July 2022. [Google Scholar] [CrossRef]
- Carruthers, S.; Gurvich, C.; Sumner, P.; Tan, E.; Thomas, E.; Rossell, S. T75. General and executive cognitive profiles: General cognitions influence on WCST performance. Schizophr. Bull. 2018, 44 (Suppl. S1), S143. [Google Scholar] [CrossRef]
- Wells, A. The Metacognitive Model of Worry and Generalised Anxiety Disorder. In Worry and Its Psychological Disorders: Theory, Assessment and Treatment; John Wiley & Sons: Hoboken, NJ, USA, 2006; pp. 177–199. [Google Scholar] [CrossRef]
- Anderson, I.M.; Palm, M.E. Pharmacological Treatments for Worry: Focus on Generalised Anxiety Disorder. In Worry and Its Psychological Disorders: Theory, Assessment and Treatment; John Wiley & Sons: Hoboken, NJ, USA, 2006; pp. 305–334. [Google Scholar] [CrossRef]
- Berg, C. The Fundamental Nature of Anxiety. In Fear, Punishment Anxiety and the Wolfenden Report; Routledge: New York, NY, USA, 2021; pp. 83–100. [Google Scholar] [CrossRef]
- Bashford-Largo, J.; Aloi, J.; Zhang, R.; Bajaj, S.; Carollo, E.; Elowsky, J.; Schwartz, A.; Dobbertin, M.; Blair, R.J.R.; Blair, K.S. Reduced neural differentiation of rewards and punishment during passive avoidance learning in adolescents with generalized anxiety disorder. Depress. Anxiety 2021, 38, 794–803. [Google Scholar] [CrossRef]
- Taylor, S. Treating anxiety sensitivity in adults with anxiety and related disorders. In The Clinician’s Guide to Anxiety Sensitivity Treatment and Assessment; Academic Press: Cambridge, MA, USA, 2019; pp. 55–75. [Google Scholar] [CrossRef]
- McHugh, R.K. Assessing anxiety sensitivity. In The Clinician’s Guide to Anxiety Sensitivity Treatment and Assessment; Academic Press: Cambridge, MA, USA, 2019; pp. 9–29. [Google Scholar] [CrossRef]
- Halkiopoulos, C.; Antonopoulou, H.; Gkintoni, E.; Aroutzidis, A. Neuromarketing as an Indicator of Cognitive Consumer Behavior in Decision-Making Process of Tourism Destination—An Overview; Springer Proceedings in Business and Economics: Berlin/Heidelberg, Germany, 2022; pp. 679–697. [Google Scholar] [CrossRef]
- Fung, K.; Alden, L.E.; Sernasie, C. Social anxiety and the acquisition of anxiety towards self-attributes. Cogn. Emot. 2021, 35, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Norton, P.J.; Price, E.C. A Meta-analytic Review of Adult Cognitive-behavioral Treatment Outcome Across the anxiety disorders. J. Nerv. Ment. Dis. 2007, 6, 521–531. [Google Scholar] [CrossRef]
- Michael, S.; Blakey, S.M.; Sherrill, A.M.; Aosved, A.C. Exposure Therapy Training and Supervision: Research-informed Strategies for Addressing Barriers to Adoption and Dissemination. Train. Educ. Prof. Psychol. 2021, 2, 97–105. [Google Scholar] [CrossRef]
- Balsamo, M.; Cataldi, F.; Carlucci, L.; Fairfield, B. Assessment Of Anxiety in Older Adults: A Review of Self-report Measures. In Clinical Interventions in Aging; Taylor & Francis: Abingdon, UK, 2018; Volume 13, pp. 573–593. [Google Scholar] [CrossRef]
- Borkovec, T.D.; Newman, M.G.; Castonguay, L.G. Cognitive-behavioral Therapy for Generalized Anxiety Disorder with Integrations from Interpersonal and Experiential Therapies. CNS Spectrums 2003, 5, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Nakamae, T. Neuromodulation for Obsessive-Compulsive Disorder. Anxiety Disord. Res. 2017, 9, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.-X.; LI, L. Virtual Reality Exposure Therapy of Anxiety Disorders. Adv. Psychol. Sci. 2013, 20, 1277–1286. [Google Scholar] [CrossRef]
- Antonopoulou, H.; Halkiopoulos, C.; Gkintoni, E.; Katsibelis, A. Application of Gamification Tools for Identification of Neurocognitive and Social Function in Distance Learning Education. Int. J. Learn. Teach. Educ. Res. 2022, 21, 367–400. [Google Scholar] [CrossRef]
- Gkintoni, E.; Halkiopoulos, C.; Antonopoulou, H. Neuroleadership an Asset in Educational Settings: An Overview. Emerg. Sci. J. 2022, 6, 893–904. [Google Scholar] [CrossRef]
- Gorman, J.M. Comorbid Depression and Anxiety Spectrum Disorders. Depress. Anxiety 1996, 4, 160–168. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Authors | Sample | Measures | Results |
|---|---|---|---|
| Aasvik et al. (2015) [23] | 167 | EMQ-R, SF-8, HADS, CFQ, ISI |
|
| Balderston et al. (2017) [26] | 69 | BAI, STAI, BDI, WASI |
|
| Fitzgerald et al. (2017) [27] | 69 | ERT |
|
| Fonzo et al. (2014) [28] | 32 | PSWQ, 10 sessions of weekly CBT, Emotion Face Assessment Task |
|
| Gordeev et al. (2013) [10] | 95 | Clinical–neurological, neuropsychological methods |
|
| Hallion et al. (2017) [11] | 56 | MINI, CSR, CGI, SIGH-A, PSWQ, SIGH-D |
|
| Khdour et al. (2016) [12] | 73 | NAART, WAIS-R, Digit Span test, HAM-A |
|
| Leonard and Abramovitch (2018) [1] | 1563 | MINI, PSWQ, DASS-21, STAI, NeuroTrax Computerized Neuropsychological Battery |
|
| Moon et al. (2015) [13] | 36 | HAMD 17, GAD-7, STAI-I, STAIII, ASI-R |
|
| Plana et al. (2014) [29] | 2738 | 40 studies evaluating mentalization, emotion, social perception/knowledge, or attributional style in anxiety disorders |
|
| Renna et al. (2018) [30] | 17 | Structured clinical interview Anxiety disorders interview schedule |
|
| Stefanopoulou et al. (2014) [14] | 17 | Penn State Worry Questionnaire, BDI-II, N-Back Task, Random Generation Key-Pressing Task, mood ratings, WTAR |
|
| Tempesta et al. (2013) [31] | 40 | STAI, BDI, PSQI, TAS-20 |
|
| White et al. (2017) [32] | 78 | A passive avoidance task |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkintoni, E.; Ortiz, P.S. Neuropsychology of Generalized Anxiety Disorder in Clinical Setting: A Systematic Evaluation. Healthcare 2023, 11, 2446. https://doi.org/10.3390/healthcare11172446
Gkintoni E, Ortiz PS. Neuropsychology of Generalized Anxiety Disorder in Clinical Setting: A Systematic Evaluation. Healthcare. 2023; 11(17):2446. https://doi.org/10.3390/healthcare11172446
Chicago/Turabian StyleGkintoni, Evgenia, and Paula Suárez Ortiz. 2023. "Neuropsychology of Generalized Anxiety Disorder in Clinical Setting: A Systematic Evaluation" Healthcare 11, no. 17: 2446. https://doi.org/10.3390/healthcare11172446
APA StyleGkintoni, E., & Ortiz, P. S. (2023). Neuropsychology of Generalized Anxiety Disorder in Clinical Setting: A Systematic Evaluation. Healthcare, 11(17), 2446. https://doi.org/10.3390/healthcare11172446