
Design, Development, and Validation of the Self-Perceived Health Scale (SPHS)
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Phase I: Development of the Self-Perceived Health Scale
2.1.1. Elaboration of the Scale
2.1.2. Content Validity
2.1.3. Answer Options
2.1.4. Pilot Study
2.2. Phase II: Validation of the Self-Perceived Health Scale
2.2.1. Design
2.2.2. Participants
2.2.3. Instruments
2.3. Ethical Considerations
2.4. Data Analysis
3. Results
3.1. Item Discrimination Analysis
3.2. Exploratory Factor Analysis
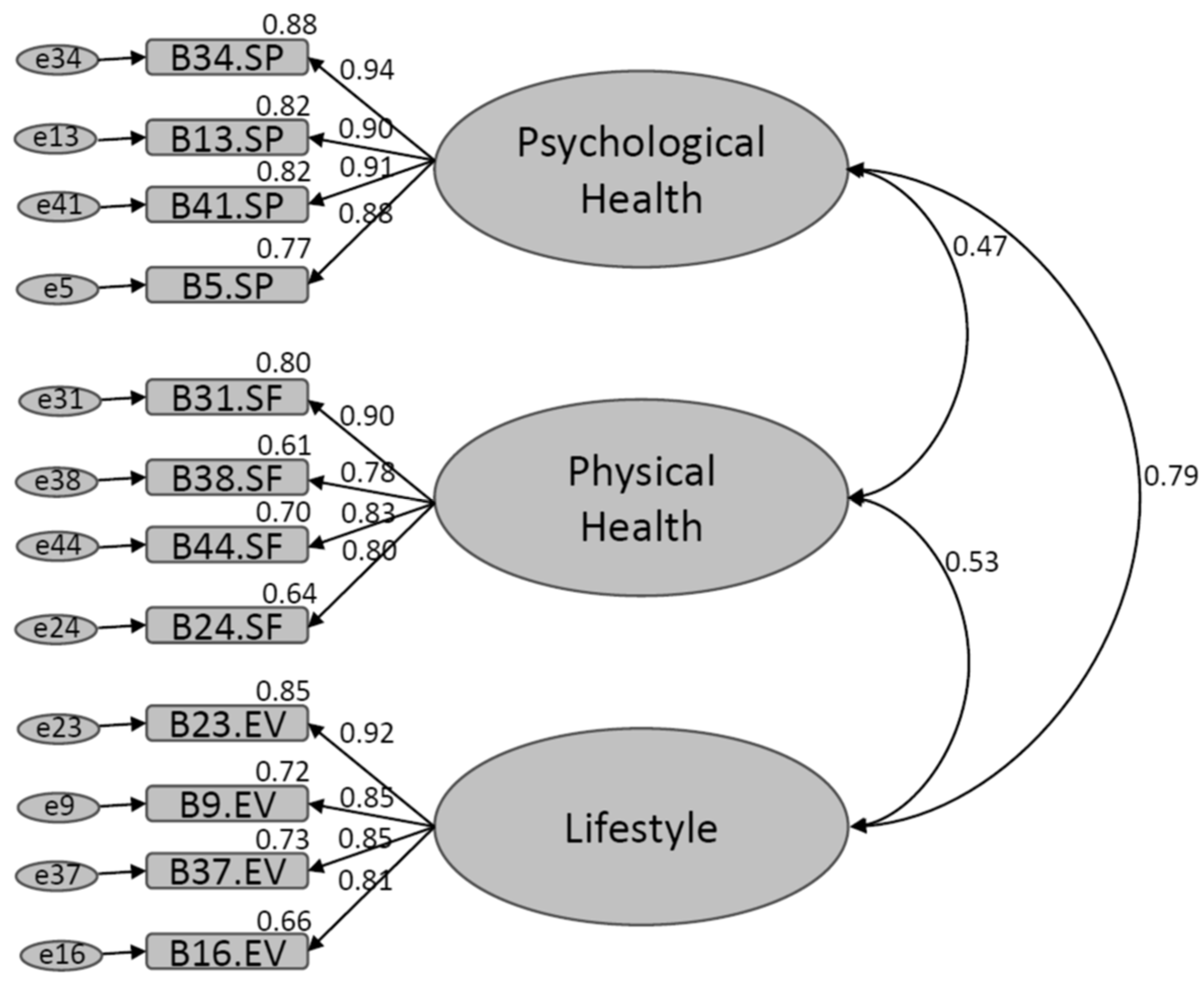
3.3. Confirmatory Factor Analysis
3.4. Measurement Invariance
3.5. Construct Validity
3.6. Convergent Validity
4. Discussion
5. Suggestions for Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gómez-Mármol, A.; Moya-Nicolás, M. Estudio de las dimensiones de la salud autopercibida en mujeres adultas. Rev. Esp. Comun. Salud 2012, 4, 93–103. [Google Scholar]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Palladino, R.; Tayu Lee, J.; Ashworth, M.; Triassi, M.; Millett, C. Associations between multimorbidity, healthcare utilisation and health status: Evidence from 16 European countries. Age Ageing 2016, 45, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Vie, T.L.; Hufthammer, K.O.; Holmen, T.L.; Meland, E.; Breidablik, H.J. Is self-rated health a stable and predictive factor for allostatic load in early adulthood? Findings from the Nord Trøndelag Health Study (HUNT). Soc. Sci. Med. 2014, 117, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Belsky, D.W.; Caspi, A.; Corcoran, D.L.; Sugden, K.; Poulton, R.; Arseneault, L.; Baccarelli, A.; Chamarti, K.; Gao, X.; Moffitt, T.E.; et al. DunedinPACE, a DNA methylation biomarker of the pace of aging. eLife 2022, 11, e73420. [Google Scholar] [CrossRef] [PubMed]
- Gumà, J.; Cámara, A. ¿Informa la salud autopercibida sobre las condiciones objetivas de salud? Algunas conclusiones a partir del análisis demográfico de microdatos de la Encuesta Nacional de Salud. Estad. Esp. 2014, 56, 61–76. [Google Scholar]
- Soto, Á.J. Implicación de la investigación de resultados en salud en la mejora continua de la calidad asistencial del Sistema Nacional de Salud. An. Med. Interna 2007, 24, 517–519. [Google Scholar] [CrossRef][Green Version]
- Ramkumar, A.; Quah, J.L.S.; Wong, T.; Yeo, L.S.H.; Nieh, C.C.; Shankar, A.; Wong, T.Y. Self-rated health, associated factors and diseases: A community-based cross-sectional study of singaporean adults aged 40 years and above. Ann. Acad. Med. Singap. 2009, 38, 606–607. [Google Scholar] [CrossRef]
- McEwen, B.S. Neurobiological and systemic effects of chronic stress. Chronic Stress 2017, 1, 2470547017692328. [Google Scholar] [CrossRef]
- Lazarevič, P. Was Misst Self-Rated Health? Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2019. [Google Scholar]
- Heiestad, H.; Gjestvang, C.; Haakstad, L.A.H. Investigating self-perceived health and quality of life: A longitudinal prospective study among beginner recreational exercisers in a fitness club setting. BMJ Open 2020, 10, e036250. [Google Scholar] [CrossRef]
- Benyamini, Y.; Leventhal, E.A.; Leventhal, H. Gender Differences in Processing Information for Making Self-Assessments of Health. Psychosom. Med. 2000, 62, 354–364. [Google Scholar] [CrossRef]
- Shields, M.; Shooshtari, S. Determinants of self-perceived health. Health Rep. 2001, 13, 35–52. [Google Scholar] [PubMed]
- El Ansari, W.; Suominen, S.; Berg-Beckhoff, G. Is healthier nutrition behaviour associated with better self-reported health and less health complaints? Evidence from Turku, Finland. Nutrients 2015, 7, 8478–8490. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Antó, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Lizán, L.; Reig, A. Adaptación transcultural de un instrumento para la valoración de la calidad de vida en atención primaria: La versión española de las viñetas COOP/WONCA. Aten. Primaria 1999, 24, 75–82. [Google Scholar]
- Alonso, J.; Anto, J.M.; Moreno, C. Spanish version of the Nottingham health profile: Translation and preliminary validity. Am. J. Public Health 1990, 80, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Nord, E. EuroQol: Health-related quality of life measurement. Valuations of health states by the general public in Norway. Health Policy 1991, 18, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Moons, P. Why call it health-related quality of life when you mean perceived health status? Eur. J. Cardiovasc. Nurs. 2004, 3, 275–277. [Google Scholar] [CrossRef]
- Sousa, K.H.; West, S.G.; Moser, S.E.; Harris, J.A.; Cook, S.W. Establishing measurement invariance: English and spanish paediatric asthma quality of life questionnaire. Nurs. Res. 2012, 61, 171–180. [Google Scholar] [CrossRef]
- Organization for Economic Cooperation and Development. Health at a Glance 2021: OECD Indicators; OECD Publishing: Paris, France, 2021. [Google Scholar]
- Lucas, R.E.; Donnellan, M.B. Estimating the reliability of single-item life satisfaction measures: Results from four national panel studies. Soc. Indic. Res. 2012, 105, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Furr, R.M. Psychometrics: An Introduction; SAGE Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Escobar, J.; Bonilla-Jimenez, F.I. Grupos focales: Una guía conceptual y metodológica. Cuad. Hispanoam. Psicol. 2017, 9, 51–67. Available online: http://sacopsi.com/articulos/Grupo%20focal%20.pdf (accessed on 19 June 2023).
- Willis, G. Cognitive Interviewing: A Tool for Improving Questionnaire Design; Sage Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications; Sage Publications: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- Kleinheksel, A.J.; Rockich-Winston, N.; Tawfik, H.; Wyatt, T.R. Demystifying Content Analysis. Am. J. Pharm. Educ. 2020, 84, 7113. [Google Scholar] [CrossRef]
- Aiken, L.R. Content validity and reliability of single items or questionnaires. Educ. Psychol. Meas. 1980, 40, 955–959. [Google Scholar] [CrossRef]
- Ventura-León, J. De regreso a la validez basada en el contenido. Adicciones 2019, 34, 323–326. [Google Scholar] [CrossRef]
- Moret, L.; Nguyen, J.-M.; Pillet, N.; Falissard, B.; Lombrail, P.; Gasquet, I. Improvement of psychometric properties of a scale measuring inpatient satisfaction with care: A better response rate and a reduction of the ceiling effect. BMC Health Serv. Res. 2007, 7, 197. [Google Scholar] [CrossRef] [PubMed]
- Chyung, S.Y.Y.; Roberts, K.; Swanson, I.; Hankinson, A. Evidence-based survey design: The use of a midpoint on the likert scale. Perform. Improv. 2017, 56, 15–23. [Google Scholar] [CrossRef]
- Sánchez-Sosa, J.J.; Rangel, A.L.G.C. Evaluación de la calidad de vida desde la perspectiva psicológica. In Manual Para la Evaluación Clínica de Los Trastornos Psicológicos: Trastornos de la Edad Adulta e Informes Psicológicos; Ediciones Pirámide: Madrid, Spain, 2006; pp. 473–492. [Google Scholar]
- Ato, M.; López-García, J.J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. An. Psicol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández-Baeza, A.; Tomás-Marco, I. El análisis factorial exploratorio de los ítems: Una guía práctica, revisada y actualizada. An. Psicol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Rodriguez-Rey, R.; Moral de la Rubia, J.; Luna, D. A Sociodemographic variables questionnaire (Q-SV) for research on family caregivers of children with chronic disease. BMC Psychol. 2019, 7, 85. [Google Scholar] [CrossRef]
- Calleja, N.; Mason, T. Escala de bienestar subjetivo (EBS-20 y EBS-8): Construcción y validación. Rev. Iberoam. Diagn. Eval. Aval. Psicol. 2020, 55, 185–201. [Google Scholar] [CrossRef]
- Morán, A.C.; Landero, H.R.; González Ramírez, M.T. COPE-28: Un análisis psicométrico de la versión en español del brief COPE. Univ. Psychol. 2009, 9, 543–552. [Google Scholar] [CrossRef]
- Ávila, M.M.; De la Rubia, J.M. Validación del inventario breve de síntomas (BSI-18) en mujeres mexicanas diagnosticadas con cáncer de mamaValidación del inventario breve de síntomas (BSI-18) en mujeres mexicanas diagnosticadas con cáncer de mama. Psicooncología 2017, 14, 307–324. [Google Scholar] [CrossRef]
- Sociedad Mexicana de Psicología. Código Ético Del Psicólogo; Trillas: Ciudad de los Deportes, México, 2010. [Google Scholar]
- American Psychological Association. Ethical Principles of Psychologists and Code of Conduct. With the 2016 Amendment to Standard 3.04; American Psychological Association Press: Washington, DC, USA, 2017. [Google Scholar]
- World Medical Association. World medical association declaration of helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Bollen, K.A. Structural Equations with Latent Variables; John Wiley & Sons: New York, NY, USA, 1989. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Taylor & Francis Group: New York, NY, USA, 2010. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Timmerman, M.E.; Lorenzo-Seva, U. Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol. Methods 2011, 16, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M. EQS 6: Structural Equation Program Manual; Multivariate Software: Encino, CA, USA, 2006. [Google Scholar]
- Putnick, D.L.; Bornstein, M.H. Measurement invariance conventions and reporting: The state of the art and future directions for psychological research. Dev. Rev. DR 2016, 41, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation coefficients: Appropriate use and interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Nielsen, S.S.; Krasnik, A. Poorer self-perceived health among migrants and ethnic minorities versus the majority population in Europe: A systematic review. Int. J. Public Health 2010, 55, 357–371. [Google Scholar] [CrossRef]
- Fielding, R.; Li, J. A validation of the concept of current perceived health and the Current Perceived Health-42 (CPH-42) questionnaire. Qual. Life Res. 1997, 6, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Miilunpalo, S.; Vuori, I.; Oja, P.; Pasanen, M.; Urponen, H. Self-rated health status as a health measure: The predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. J. Clin. Epidemiol. 1997, 50, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Kleber, M.E.; Koenig, J.; Loerbroks, A.; Herr, R.M.; Hoffmann, K.; Fischer, J.E.; Benyamini, Y.; Thayer, J.F. Investigating the associations of self-rated health: Heart rate variability is more strongly associated than inflammatory and other frequently used biomarkers in a cross sectional occupational sample. PLoS ONE 2015, 10, e0117196. [Google Scholar] [CrossRef] [PubMed]
- Eddy, P.; Wertheim, E.H.; Hale, M.W.; Wright, B.J. Trait Mindfulness Helps Explain the Relationships Between Job Stress, Physiological Reactivity, and Self-Perceived. Health J. Occup. Environ. Med. 2019, 61, e12–e18. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Toledano, F.; Jiménez, S.; Moral de la Rubia, J.; Merino-Soto, C.; Rivera-Rivera, L. Positive Mental Health Scale (PMHS) in Parents of Children with Cancer: A Psychometric Evaluation Using Item Response Theory. Cancers 2023, 15, 2744. [Google Scholar] [CrossRef]


{kind=link}
| 50 Items SPHS | ||||
|---|---|---|---|---|
| Items | Psychological Health | Physical Health | Healthy Lifestyle | Communalities (H2) |
| 13. I am emotionally healthy. | 0.899 | −0.131 | 0.105 | 0.808 |
| 34. I feel emotionally healthy. | 0.891 | −0.172 | 0.165 | 0.828 |
| 41. I consider myself a person with emotional well-being. | 0.886 | −0.131 | 0.142 | 0.827 |
| 5. I have an adequate level of mental health. | 0.816 | −0.121 | 0.143 | 0.711 |
| 45. I believe I am able to regulate my emotions. | 0.809 | 0.055 | 0.005 | 0.707 |
| 6. I feel I am open about my feelings and emotions. | 0.773 | −0.043 | −0.015 | 0.555 |
| 20. I accept my emotions and feelings. | 0.770 | −0.054 | 0.036 | 0.583 |
| 27. I am able to solve my problems appropriately. | 0.763 | 0.086 | 0.064 | 0.719 |
| 33. I have the skills necessary to promote my own mental health. | 0.760 | 0.037 | 0.090 | 0.694 |
| 50. I am aware of my emotions and feelings. | 0.721 | 0.082 | −0.071 | 0.529 |
| 40. My mental health makes it easier for me to do my daily activities. | 0.709 | 0.119 | 0.094 | 0.694 |
| 7. I consider myself mentally agile. | 0.700 | 0.111 | −0.015 | 0.568 |
| 28. My mental capacity is adequate. | 0.676 | 0.246 | −0.027 | 0.657 |
| 12. I am able to cope with stressful situations in my life. | 0.667 | 0.073 | 0.110 | 0.599 |
| 21. I consider my brain to be functioning properly. | 0.642 | 0.287 | −0.071 | 0.614 |
| 42. I can learn new things easily. | 0.635 | 0.347 | −0.198 | 0.575 |
| 49. I am able to finish my duties without a problem. | 0.600 | 0.104 | 0.165 | 0.585 |
| 14. I have a good memory. | 0.587 | 0.224 | −0.147 | 0.420 |
| 48. I consider myself able to seek professional psychological help when I need it. | 0.586 | 0.025 | −0.071 | 0.316 |
| 46. I am able to remember details from the previous day. | 0.578 | 0.289 | −0.122 | 0.487 |
| 35. I am able to remember my daily commitments. | 0.576 | 0.294 | −0.071 | 0.526 |
| 26. Talking about my problems gives me peace of mind. | 0.510 | 0.095 | −0.029 | 0.299 |
| 22. I have enough energy to face the day. | 0.391 | 0.276 | 0.258 | 0.587 |
| 29. I feel energetic enough for the rest of the day. | 0.366 | 0.274 | 0.314 | 0.623 |
| 47. The time I sleep allows me to recover to start a new day. | 0.303 | 0.123 | 0.276 | 0.347 |
| 38. I can move my limbs (arms, legs, and/or head) without effort. | 0.114 | 0.839 | −0.114 | 0.712 |
| 31. I am able to walk with ease. | 0.122 | 0.817 | −0.038 | 0.747 |
| 24. I am able to go up and down stairs with ease. | −0.017 | 0.729 | 0.233 | 0.743 |
| 44. I am able to maintain my body balance, e.g., standing on one foot. | 0.247 | 0.706 | −0.079 | 0.661 |
| 32. I feel able to do sport or physical exercise regularly. | −0.146 | 0.684 | 0.344 | 0.694 |
| 10. I am able to move easily. | 0.161 | 0.669 | 0.145 | 0.727 |
| 4. I can make coordinated movements (e.g., stand on one foot, walk on tiptoe, etc.). | 0.214 | 0.646 | −0.041 | 0.567 |
| 39. I consider myself capable of physical exercise for at least 30 min. | −0.092 | 0.633 | 0.326 | 0.636 |
| 3. My ability to move around and walk is adequate. | 0.094 | 0.588 | 0.173 | 0.562 |
| 17. I can perform my daily activities with ease. | 0.190 | 0.567 | 0.160 | 0.618 |
| 11. I am able to perform intense physical activity. | −0.162 | 0.565 | 0.436 | 0.619 |
| 18. I have physical strength. | −0.011 | 0.564 | 0.337 | 0.616 |
| 25. I consider myself physically agile. | −0.004 | 0.512 | 0.441 | 0.685 |
| 15. I am free of pain. | 0.297 | 0.298 | 0.207 | 0.439 |
| 9. My habits allow me to maintain my health. | 0.055 | 0.006 | 0.856 | 0.793 |
| 2. I feel my lifestyle is healthy. | 0.133 | −0.087 | 0.794 | 0.688 |
| 23. My habits help me maintain my health. | 0.144 | 0.028 | 0.779 | 0.778 |
| 16. I feel that my daily activities improve my health. | 0.054 | 0.072 | 0.751 | 0.675 |
| 37. My diet helps me maintain good health. | 0.142 | 0.035 | 0.749 | 0.731 |
| 30. I do activities that help me improve my health. | 0.053 | 0.087 | 0.740 | 0.672 |
| 8. Physically I feel healthy. | 0.186 | 0.154 | 0.609 | 0.676 |
| 43. The exercise and/or physical activity I do helps me maintain my health. | −0.049 | 0.293 | 0.594 | 0.573 |
| 19. My daily activities make me feel good. | 0.205 | 0.114 | 0.593 | 0.632 |
| 36. I consider my physical health to be adequate. | 0.151 | 0.100 | 0.556 | 0.505 |
| 36. I feel healthy. | 0.348 | 0.190 | 0.480 | 0.730 |
| Number of items: 50 | 25 | 14 | 11 | |
| Total explained variance: 62.68% | 28.17% | 17.56% | 16.95% | |
| 38 items SPHS | ||||
| Items | Psychological Health | Physical Health | Healthy Lifestyle | Communalities (H2) |
| 13. I am emotionally healthy. | 0.938 | −0.094 | 0.038 | 0.835 |
| 34. I feel emotionally healthy. | 0.919 | −0.143 | 0.112 | 0.844 |
| 41. I consider myself an emotionally healthy person. | 0.909 | −0.096 | 0.093 | 0.843 |
| 5. I have adequate mental health. | 0.841 | −0.089 | 0.089 | 0.724 |
| 45. I believe I am able to regulate my emotions. | 0.821 | 0.084 | −0.035 | 0.719 |
| 20. I accept my emotions and feelings. | 0.772 | −0.022 | 0.006 | 0.584 |
| 6. I feel I am open to my feelings and emotions. | 0.761 | −0.018 | −0.027 | 0.543 |
| 33. I have the necessary skills to promote my own mental health. | 0.760 | 0.063 | 0.067 | 0.700 |
| 27. I am able to solve my problems adequately. | 0.753 | 0.122 | 0.038 | 0.718 |
| 40. My mental health makes it easier for me to do my daily activities. | 0.701 | 0.141 | 0.075 | 0.694 |
| 12. I am able to cope with stressful situations in my life. | 0.692 | 0.092 | 0.058 | 0.610 |
| 50. I am aware of my emotions and feelings. | 0.691 | 0.098 | −0.063 | 0.504 |
| 7. I consider myself mentally agile. | 0.669 | 0.131 | −0.008 | 0.549 |
| 28. My mental capacity is adequate. | 0.647 | 0.276 | −0.033 | 0.647 |
| 21. I consider my brain to function adequately. | 0.607 | 0.316 | −0.070 | 0.599 |
| 42. I can learn new things easily. | 0.575 | 0.362 | −0.163 | 0.530 |
| 49. I can finish my duties without a problem. | 0.554 | 0.117 | 0.183 | 0.564 |
| 38. I can move my limbs (arms, legs, and/or head) without effort. | 0.054 | 0.878 | −0.109 | 0.725 |
| 31. I can walk with ease. | 0.071 | 0.867 | −0.047 | 0.775 |
| 24. I am able to go up and down stairs with ease. 24. | −0.055 | 0.739 | 0.238 | 0.741 |
| 44. I am able to maintain my body balance, e.g., by standing on one foot. | 0.190 | 0.729 | −0.060 | 0.655 |
| 10. I can move with ease. | 0.115 | 0.702 | 0.140 | 0.737 |
| 4. I can make coordinated movements (e.g., standing on one foot, walking on tiptoe, etc.). | 0.178 | 0.684 | −0.048 | 0.583 |
| 32. I feel able to do sports or physical exercise on a regular basis. | −0.148 | 0.674 | 0.325 | 0.661 |
| 39. I consider myself able to exercise for at least 30 min. | −0.093 | 0.628 | 0.304 | 0.611 |
| 3. My ability to move around and walk is adequate. | 0.054 | 0.625 | 0.166 | 0.582 |
| 17. I can perform my daily activities with ease. | 0.134 | 0.573 | 0.183 | 0.604 |
| 18. I have physical strength. | −0.017 | 0.550 | 0.325 | 0.587 |
| 9. My habits help me maintain my health. | 0.020 | −0.012 | 0.890 | 0.802 |
| 23. My habits help me maintain my health. | 0.092 | 0.007 | 0.837 | 0.806 |
| 16. I feel that my daily activities improve my health. | 0.004 | 0.047 | 0.806 | 0.699 |
| 2. I feel that my lifestyle is healthy. | 0.122 | −0.090 | 0.791 | 0.672 |
| 30. I engage in activities that help me improve my health. | 0.015 | 0.063 | 0.787 | 0.692 |
| 37. My diet allows me to maintain good health. | 0.101 | 0.026 | 0.784 | 0.744 |
| 19. My daily activities make me feel good. | 0.161 | 0.107 | 0.631 | 0.647 |
| 43. The exercise and/or physical activity I do helps me to maintain my health. | −0.079 | 0.280 | 0.624 | 0.584 |
| 8. I feel physically healthy. | 0.188 | 0.157 | 0.577 | 0.650 |
| 36. I feel healthy. | 0.341 | 0.197 | 0.454 | 0.712 |
| Number of items: 38 | 17 | 11 | 10 | |
| Total explained variance: 67.03% | 29.09% | 19.33% | 18.61% | |
| 30 Items SPHS | ||||
| Items | Psychological Health | Healthy Lifestyle | Physical Health | Communalities (H2) |
| 13. I am emotionally healthy. | 0.945 | −0.009 | −0.033 | 0.852 |
| 34. I feel emotionally healthy. | 0.930 | 0.071 | −0.092 | 0.864 |
| 41. I consider myself an emotionally healthy person. | 0.912 | 0.58 | −0.045 | 0.856 |
| 5. I have adequate mental health. | 0.850 | 0.049 | −0.042 | 0.738 |
| 45. I believe I am able to regulate my emotions. | 0.801 | −0.056 | 0.135 | 0.711 |
| 20. I accept my emotions and feelings. | 0.751 | −0.007 | 0.022 | 0.575 |
| 33. I have the skills necessary to foster my own mental health. | 0.740 | 0.053 | 0.14 | 0.694 |
| 6. I feel that I am open to my feelings and emotions. | 0.738 | −0.039 | 0.028 | 0.532 |
| 27. I am able to solve my problems adequately. | 0.711 | 0.037 | 0.163 | 0.692 |
| 40. My mental health makes it easier for me to do my daily activities. | 0.683 | 0.056 | 0.181 | 0.687 |
| 9. My habits allow me to maintain my health. | 0.007 | 0.905 | −0.025 | 0.800 |
| 23. My habits help me to maintain my health. | 0.061 | 0.873 | −0.013 | 0.816 |
| 16. I feel that my daily activities improve my health. | −0.011 | 0.831 | 0.023 | 0.703 |
| 30. I engage in activities that help me improve my health. | −0.007 | 0.815 | 0.041 | 0.698 |
| 37. My diet helps me maintain good health. | 0.077 | 0.805 | 0.015 | 0.745 |
| 2. I feel that my lifestyle is healthy. | 0.116 | 0.797 | −0.096 | 0.667 |
| 19. My daily activities make me feel good. | 0.138 | 0.652 | 0.094 | 0.649 |
| 43. The exercise and/or physical activity I do helps me to maintain my health. | −0.092 | 634 | 0.265 | 0.583 |
| 8. I feel physically healthy. | 0.182 | 0.568 | 0.162 | 0.647 |
| 36. I feel healthy. | 0.334 | 0.440 | 0.213 | 0.712 |
| 31. I can walk easily. | 0.052 | −0.085 | 0.914 | 0.797 |
| 38. I can move my limbs (arms, legs, and/or head) without effort. | 0.026 | −0.132 | 0.911 | 0.727 |
| 44. I am able to maintain my body balance, for example, when standing on one foot. | 0.149 | −0.059 | 0.750 | 0.639 |
| 24. I am able to go up and down stairs with ease. | −0.079 | 0.232 | 0.746 | 0.737 |
| 10. I am able to move easily. | 0.095 | 0.113 | 0.737 | 0.748 |
| 4. I can make coordinated movements (e.g., standing on one foot, walking on tiptoe, etc.). | 0.160 | −0.072 | 0.716 | 0.587 |
| 32. I feel able to do sports or physical exercise on a regular basis. | −0.142 | 0.299 | 0.670 | 0.647 |
| 3. My ability to move around and walk is adequate. | 0.049 | 0.131 | 0.655 | 0.592 |
| 39. I consider myself capable of exercising for at least 30 min. | −0.086 | 0.272 | 0.635 | 0.605 |
| 17. I can do my daily activities with ease. | 0.103 | 0.184 | 0.578 | 0.590 |
| Number of items: 30 | 10 | 10 | 10 | |
| Total explained variance: 69.63% | 25.15% | 22.61% | 21.87% | |
| 24 Items SPHS | ||||
| Items | Psychological Health | Healthy Lifestyle | Physical Health | Communalities (H2) |
| 13. I am emotionally healthy. | 0.943 | −0.023 | −0.002 | 0.861 |
| 34. I feel emotionally healthy. | 0.931 | 0.058 | −0.066 | 0.874 |
| 41. I consider myself a person with emotional well-being. | 0.891 | 0.062 | −0.022 | 0.843 |
| 5. I have adequate mental health. | 0.843 | 0.039 | −0.016 | 0.739 |
| 45. I believe I am able to regulate my emotions. | 0.775 | −0.035 | 0.0149 | 0.701 |
| 20. I accept my emotions and feelings. | 0.732 | 0.006 | 0.040 | 0.571 |
| 6. I feel I am open about my feelings and emotions. | 0.730 | −0.037 | 0.052 | 0.540 |
| 33. I have the skills necessary to promote my own mental health. | 0.724 | 0.064 | 0.122 | 0.696 |
| 23. My habits help me maintain my health. | 0.49 | 0.889 | −0.017 | 0.827 |
| 9. My habits allow me to maintain my health. | 0.019 | 0.876 | −0.014 | 0.772 |
| 16. I feel that my daily activities improve my health. | −0.014 | 0.851 | 0.013 | 0.722 |
| 30. I do activities that help me improve my health. | −0.014 | 0.849 | 0.023 | 0.730 |
| 37. My eating habits allow me to maintain good health. | 0.074 | 0.798 | 0.018 | 0.731 |
| 2. I feel that my lifestyle is healthy. | 0.133 | 0.764 | −0.084 | 0.645 |
| 19. My daily activities give me well-being. | 0.114 | 0.689 | 0.087 | 0.670 |
| 43. The exercise and/or physical activity I do helps me maintain my health. | −0.087 | 0.658 | 0.237 | 0.592 |
| 31. I can walk with ease. | 0.032 | −0.062 | 0.920 | 0.811 |
| 38. I can move my limbs (arms, legs and/or head) without effort. | 0.007 | −0.104 | 0.903 | 0.723 |
| 44. I can maintain my body balance, for example, by standing on one foot. | 0.126 | −0.030 | 0.746 | 0.636 |
| 10. I can move easily. | 0.086 | 0.122 | 0.742 | 0.754 |
| 24. I am able to go up and down stairs with ease. | −0.090 | 0.248 | 0.737 | 0.733 |
| 4. I can make coordinated movements (e.g., standing on one foot, walking on tiptoe, etc.). | 0.146 | −0.053 | 0.724 | 0.599 |
| 3. My ability to move around and walk is adequate. | 0.052 | 0.133 | 0.656 | 0.594 |
| 32. I feel able to engage in sport or physical exercise on a regular basis. | −0.130 | 0.316 | 0.630 | 0.614 |
| Number of items: 24 | 8 | 8 | 8 | |
| Total explained variance: 70.74% | 24.61% | 24.25% | 21.87% | |
| 18 Items SPHS | ||||
| Items | Psychological Health | Healthy Lifestyle | Physical Health | Communalities (H2) |
| 34. I feel emotionally healthy. | 0.938 | 0.041 | −0.057 | 0.877 |
| 13. I have adequate emotional health. | 0.938 | −0.018 | 0.004 | 0.863 |
| 41. I consider myself a person with emotional well-being. | 0.890 | 0.052 | −0.005 | 0.846 |
| 5. I have adequate mental health. | 0.843 | 0.040 | −0.013 | 0.743 |
| 45. I believe I am able to regulate my emotions. | 0.774 | −0.053 | 0.167 | 0.698 |
| 20. I accept my emotions and feelings. | 0.711 | 0.005 | 0.054 | 0.551 |
| 9. My habits allow me to maintain my health. | −0.016 | 0.914 | −0.007 | 0.811 |
| 23. My habits help me maintain my health. | 0.032 | 0.869 | 0.022 | 0.812 |
| 37. My eating allows me to maintain good health. | 0.333 | 0.836 | 0.033 | 0.770 |
| 16. I feel that my daily activities improve my health. | −0.010 | 0.802 | 0.047 | 0.678 |
| 2. I feel that my lifestyle is healthy. | 0.106 | 0.801 | −0.082 | 0.682 |
| 30. I do activities that help me improve my health. | −0.004 | 0.798 | 0.047 | 0.677 |
| 31. I can walk with ease. | 0.009 | −0.035 | 0.922 | 0.824 |
| 38. I can move my limbs (arms, legs, and/or head) without effort. | −0.013 | −0.073 | 0.901 | 0.733 |
| 44. I am able to maintain my body balance, for example, by standing on one foot. | 0.108 | −0.020 | 0.760 | 0.652 |
| 24. I am able to go up and down stairs with ease. | −0.124 | 0.290 | 0.733 | 0.738 |
| 10. I can move easily. | 0.064 | 0.168 | 0.713 | 0.731 |
| 4. I can make coordinated movements (e.g., standing on one foot, walking on tiptoe, etc.). | 0.138 | −0.033 | 0.710 | 0.590 |
| Number of items: 18 | 8 | 8 | 8 | |
| Total explained variance: 73.75% | 25.75% | 25.35% | 22.66% | |
| Factors (λ) | ||||||
|---|---|---|---|---|---|---|
| Items | Psychological Health | Physical Health | Healthy Lifestyle | Communalities (H2) | Alpha If the Item is Removed | |
| 34. I feel emotionally healthy. [34. Me siento emocionalmente saludable.] | 0.944 | 0.012 | −0.023 | 0.885 | 0.926 | |
| 13. I am in adequate emotional health. [13. Tengo una salud emocional adecuada.] | 0.940 | −0.036 | 0.027 | 0.686 | 0.926 | |
| 41. I consider myself to be a person with emotional well-being. [41. Me considero una persona con bienestar emocional.] | 0.864 | 0.060 | 0.019 | 0.829 | 0.925 | |
| 5. I have adequate mental health. [5. Tengo una adecuada salud mental.] | 0.856 | 0.020 | 0.001 | 0.755 | 0.927 | |
| 31. I can walk easily. [31. Puedo caminar con facilidad.] | 0.020 | 0.904 | −0.002 | 0.838 | 0.929 | |
| 38. I can move my limbs (arms, legs, and/or head) without effort. [38. Puedo mover mis extremidades (brazos, piernas y/o cabeza) sin esfuerzo.] | 0.010 | 0.899 | −0.026 | 0.794 | 0.931 | |
| 44. I can keep my balance, for example, by standing on one foot. [44. Puedo mantener el equilibrio de mi cuerpo, por ejemplo, al pararme en un pie.] | 0.051 | 0.825 | 0.025 | 0.759 | 0.930 | |
| 24. I can go up and down stairs with ease. [24. Soy capaz de subir y bajar escaleras con facilidad.] | 0.014 | 0.784 | 0.036 | 0.661 | 0.928 | |
| 23. My lifestyle helps me take care of my health. [23. Mi estilo de vida me ayuda a cuidar mi salud.] | 0.036 | −0.047 | 0.928 | 0.845 | 0.925 | |
| 9. My habits allow me to improve my health. [9. Mis hábitos me permiten mejorar mi salud.] | 0.003 | −0.057 | 0.886 | 0.734 | 0.926 | |
| 37. My diet allows me to maintain good health. [37. Mi alimentación me permite mantener una buena salud.] | 0.110 | 0.010 | 0.734 | 0.635 | 0.925 | |
| 16. I feel that my daily activities improve my health. [16. Siento que mis actividades diarias mejoran mi salud.] | −0.105 | 0.309 | 0.705 | 0.736 | 0.928 | |
| Number of items | Total 12 | 4 | 4 | 4 | ||
| Total explained variance (%) | 77.82% | 28.07% | 26.41% | 23.34% | ||
| Total | Factors | |||
|---|---|---|---|---|
| Psychological Health | Physical Health | Healthy Lifestyle | ||
| Reliability | α = 0.933 ω = 0.925 | α = 0.951 ω = 0.952 | α = 0.907 ω = 0.908 | α = 0.926 ω = 0.927 |
| Interfactor correlations | Psychological health | 1 | ||
| Physical health | 0.463 | 1 | ||
| Healthy lifestyle | 0.605 | 0.558 | 1 | |
| Mean (SD) | 3.98 (1.07) | 3.60 (1.35) | 3.49 (1.32) | 4.87 (1.18) |
| Models | χ2/gl = CMIN <3 | CFI >0.95 | GFI >0.95 | TLI >0.95 | RMSEA (CI 90%) |
|---|---|---|---|---|---|
| SPHS-38 (n = 303) | 2448.693/703 = 3.69 | 0.849 | 0.668 | 0.839 | 0.094 (0.090, 0.098) |
| SPHS-30 (n = 303) | 1535.364/402 = 3.81 | 0.879 | 0.731 | 0.869 | 0.096 (0.091, 0.102) |
| SPHS-24 (n = 303) | 903.262/249 = 3.62 | 0.909 | 0.786 | 0.900 | 0.093 (0.087, 0.100) |
| SPHS-18 (n = 303) | 411.926/132 = 3.12 | 0.947 | 0.865 | 0.939 | 0.084 (0.075, 0.093) |
| SPHS-12 (n = 303) | 126.407/51 = 2.479 | 0.978 | 0.936 | 0.971 | 0.070 (0.055, 0.085) |
| SPHS-12 (n = 297) | 137.132/51 = 2.689 | 0.973 | 0.926 | 0.965 | 0.076 (0.060, 0.091) |
| Model | X2(gl) | X2/gl | CFI | RMSEA (CI 90%) | ΔX2 | ΔCFI | ΔRMSEA | |
| M1. Configuration invariance | 219.253(102) | 2.149 | 0.963 | 0.088 (0.072, 0.104) | ||||
| M2. Measurement or weak invariance (constrained λ) | 230.996(111) | 2.081 | 0.962 | 0.085 (0.070, 0.101) | M2 Vs M1 | 11.743 (9), p = 0.228 | −0.001 | −0.003 |
| M3. Scalar invariance (constrained λ and τ) | 240.864(120) | 2.007 | 0.962 | 0.082 (0.067, 0.097) | M3 Vs M2 | 9.868 (9), p = 0.361 | 0.000 | −0.003 |
| M4. Strict invariance (constrained λ, τ and θ) | 277.416(132) | 2.101 | 0.954 | 0.086 (0.072, 0.100) | M4 Vs M3 | 36.553 (12), p = 0.0002 | −0.008 | 0.004 |
| Criteria | p > 0.05 | ≤0.01 | ≤0.015 |
| Psychological Health | Physical Health | Lifestyle | SPHS-12 | |
|---|---|---|---|---|
| SWBS-8 | 0.688 ** | 0.510 ** | 0.325 ** | 0.617 ** |
| BSI-18 | −0.595 ** | −0.369 ** | −0.130 * | −0.449 ** |
| COPE-28 | 0.334 ** | 0.300 ** | 0.252 ** | 0.356 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tinajero-Chávez, L.I.; Mora-Romo, J.F.; Bravo-Doddoli, A.; Cruz-Narciso, B.V.; Calleja, N.; Toledano-Toledano, F. Design, Development, and Validation of the Self-Perceived Health Scale (SPHS). Healthcare 2023, 11, 2007. https://doi.org/10.3390/healthcare11142007
Tinajero-Chávez LI, Mora-Romo JF, Bravo-Doddoli A, Cruz-Narciso BV, Calleja N, Toledano-Toledano F. Design, Development, and Validation of the Self-Perceived Health Scale (SPHS). Healthcare. 2023; 11(14):2007. https://doi.org/10.3390/healthcare11142007
Chicago/Turabian StyleTinajero-Chávez, Lorena Ishel, José Fernando Mora-Romo, Andrea Bravo-Doddoli, Beatríz Viridiana Cruz-Narciso, Nazira Calleja, and Filiberto Toledano-Toledano. 2023. "Design, Development, and Validation of the Self-Perceived Health Scale (SPHS)" Healthcare 11, no. 14: 2007. https://doi.org/10.3390/healthcare11142007
APA StyleTinajero-Chávez, L. I., Mora-Romo, J. F., Bravo-Doddoli, A., Cruz-Narciso, B. V., Calleja, N., & Toledano-Toledano, F. (2023). Design, Development, and Validation of the Self-Perceived Health Scale (SPHS). Healthcare, 11(14), 2007. https://doi.org/10.3390/healthcare11142007