
White Blood Cells, Platelets, Red Blood Cells and Gas Bubbles in SCUBA Diving: Is There a Relationship?

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Diving Procedures
2.2. Material and Protocol
2.3. Echocardiography Protocol
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doubt, T.J. Cardiovascular and thermal responses to SCUBA diving. Med. Sci. Sports Exerc. 1996, 28, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Perovic, A.; Unic, A.; Dumic, J. Recreational scuba diving: Negative or positive effects of oxidative and cardiovascular stress? Biochem. Med. 2014, 24, 235–247. [Google Scholar] [CrossRef]
- Morabito, C.; Bosco, G.; Pilla, R.; Corona, C.; Mancinelli, R.; Yang, Z.; Camporesi, E.M.; Fano, G.; Mariggio, M.A. Effect of pre-breathing oxygen at different depth on oxidative status and calcium concentration in lymphocytes of scuba divers. Acta Physiol. 2011, 202, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Theunissen, S.; Guerrero, F.; Sponsiello, N.; Cialoni, D.; Pieri, M.; Germonpre, P.; Obeid, G.; Tillmans, F.; Papadopoulou, V.; Hemelryck, W.; et al. Nitric oxide-related endothelial changes in breath-hold and scuba divers. Undersea Hyperb. Med. 2013, 40, 135–144. [Google Scholar] [PubMed]
- Perovic, A.; Nikolac, N.; Braticevic, M.N.; Milcic, A.; Sobocanec, S.; Balog, T.; Dabelic, S.; Dumic, J. Does recreational scuba diving have clinically significant effect on routine haematological parameters? Biochem. Med. 2017, 27, 325–331. [Google Scholar] [CrossRef]
- Anegg, U.; Dietmaier, G.; Maier, A.; Tomaselli, F.; Gabor, S.; Kallus, K.W.; Smolle-Juttner, F.M. Stress-induced hormonal and mood responses in scuba divers: A field study. Life Sci. 2002, 70, 2721–2734. [Google Scholar] [CrossRef]
- Suzuki, K.; Totsuka, M.; Nakaji, S.; Yamada, M.; Kudoh, S.; Liu, Q.; Sugawara, K.; Yamaya, K.; Sato, K. Endurance exercise causes interaction among stress hormones, cytokines, neutrophil dynamics, and muscle damage. J. Appl. Physiol. 1999, 87, 1360–1367. [Google Scholar] [CrossRef]
- Chmura, J.; Kawczynski, A.; Medras, M.; Jozkow, P.; Morawiec, B. The impact of freediving on psychomotor performance and blood catecholamine concentration. Undersea Hyperb. Med. 2014, 41, 111–117. [Google Scholar]
- Walsh, N.P.; Gleeson, M.; Shephard, R.J.; Gleeson, M.; Woods, J.A.; Bishop, N.C.; Fleshner, M.; Green, C.; Pedersen, B.K.; Hoffman-Goetz, L.; et al. Position statement. Part one: Immune function and exercise. Exerc. Immunol. Rev. 2011, 17, 6–63. [Google Scholar]
- Peake, J.; Suzuki, K. Neutrophil activation, antioxidant supplements and exercise-induced oxidative stress. Exerc. Immunol. Rev. 2004, 10, 129–141. [Google Scholar] [PubMed]
- Sugama, K.; Suzuki, K.; Yoshitani, K.; Shiraishi, K.; Kometani, T. IL-17, neutrophil activation and muscle damage following endurance exercise. Exerc. Immunol. Rev. 2012, 18, 116–127. [Google Scholar] [PubMed]
- Rocco, M.; Antonelli, M.; Letizia, V.; Alampi, D.; Spadetta, G.; Passariello, M.; Conti, G.; Serio, P.; Gasparetto, A. Lipid peroxidation, circulating cytokine and endothelin 1 levels in healthy volunteers undergoing hyperbaric oxygenation. Minerva Anestesiol. 2001, 67, 393–400. [Google Scholar] [PubMed]
- Galkina, S.I.; Golenkina, E.A.; Viryasova, G.M.; Romanova, Y.M.; Sud’ina, G.F. Nitric Oxide in Life and Death of Neutrophils. Curr. Med. Chem. 2019, 26, 5764–5780. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; Ricci, C.; Banfi, G. Effect of winter swimming on haematological parameters. Biochem. Med. 2011, 21, 71–78. [Google Scholar] [CrossRef]
- Ferrer, M.D.; Sureda, A.; Batle, J.M.; Tauler, P.; Tur, J.A.; Pons, A. Scuba diving enhances endogenous antioxidant defenses in lymphocytes and neutrophils. Free Radic. Res. 2007, 41, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Rothfuss, A.; Dennog, C.; Speit, G. Adaptive protection against the induction of oxidative DNA damage after hyperbaric oxygen treatment. Carcinogenesis 1998, 19, 1913–1917. [Google Scholar] [CrossRef]
- Vangala, R.R.; Kritzler, K.; Schoch, G.; Topp, H. Induction of single-strand breaks in lymphocyte DNA of rats exposed to hyperoxia. Arch. Toxicol. 1998, 72, 247–248. [Google Scholar] [CrossRef]
- Natale, V.M.; Brenner, I.K.; Moldoveanu, A.I.; Vasiliou, P.; Shek, P.; Shephard, R.J. Effects of three different types of exercise on blood leukocyte count during and following exercise. Sao Paulo Med. J. 2003, 121, 9–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obad, A.; Marinovic, J.; Ljubkovic, M.; Breskovic, T.; Modun, D.; Boban, M.; Dujic, Z. Successive deep dives impair endothelial function and enhance oxidative stress in man. Clin. Physiol. Funct. Imaging 2010, 30, 432–438. [Google Scholar] [CrossRef]
- Marinovic, J.; Ljubkovic, M.; Breskovic, T.; Gunjaca, G.; Obad, A.; Modun, D.; Bilopavlovic, N.; Tsikas, D.; Dujic, Z. Effects of successive air and nitrox dives on human vascular function. Eur. J. Appl. Physiol. 2012, 112, 2131–2137. [Google Scholar] [CrossRef]
- Clemens, M.R.; Waller, H.D. Lipid peroxidation in erythrocytes. Chem. Phys. Lipids 1987, 45, 251–268. [Google Scholar] [CrossRef]
- Sureda, A.; Tauler, P.; Aguilo, A.; Cases, N.; Fuentespina, E.; Cordova, A.; Tur, J.A.; Pons, A. Relation between oxidative stress markers and antioxidant endogenous defences during exhaustive exercise. Free Radic. Res. 2005, 39, 1317–1324. [Google Scholar] [CrossRef]
- Sureda, A.; Batle, J.M.; Capo, X.; Martorell, M.; Cordova, A.; Tur, J.A.; Pons, A. Scuba diving induces nitric oxide synthesis and the expression of inflammatory and regulatory genes of the immune response in neutrophils. Physiol. Genom. 2014, 46, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Nossum, V.; Hjelde, A.; Brubakk, A.O. Small amounts of venous gas embolism cause delayed impairment of endothelial function and increase polymorphonuclear neutrophil infiltration. Eur. J. Appl. Physiol. 2002, 86, 209–214. [Google Scholar] [CrossRef]
- Cialoni, D.; Pieri, M.; Balestra, C.; Marroni, A. Dive Risk Factors, Gas Bubble Formation, and Decompression Illness in Recreational SCUBA Diving: Analysis of DAN Europe DSL Data Base. Front. Psychol. 2017, 8, 1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valic, Z.; Duplancic, D.; Bakovic, D.; Ivancev, V.; Eterovic, D.; Wisloff, U.; Brubakk, A.O.; Dujic, Z. Diving-induced venous gas emboli do not increase pulmonary artery pressure. Int. J. Sports Med. 2005, 26, 626–631. [Google Scholar] [CrossRef]
- Weathersby, P.K.; Hart, B.L.; Flynn, E.T.; Walker, W.F. Role of oxygen in the production of human decompression sickness. J. Appl. Physiol. 1987, 63, 2380–2387. [Google Scholar] [CrossRef]
- Eftedal, O.S.; Lydersen, S.; Brubakk, A.O. The relationship between venous gas bubbles and adverse effects of decompression after air dives. Undersea Hyperb. Med. 2007, 34, 99–105. [Google Scholar]
- Francis, T.; Mitchell, S. Pathophysiology of decompression sickness. In The Bennett and Elliot’s Physiology and Medicine of Diving, 5th ed.; Brubakk, A.O., Neuman, T.S., Eds.; Saunders: London, UK, 2003; pp. 530–556. [Google Scholar]
- Eckmann, D.M.; Armstead, S.C. Influence of endothelial glycocalyx degradation and surfactants on air embolism adhesion. Anesthesiology 2006, 105, 1220–1227. [Google Scholar] [CrossRef]
- Piccin, A.; Murphy, W.G.; Smith, O.P. Circulating microparticles: Pathophysiology and clinical implications. Blood Rev. 2007, 21, 157–171. [Google Scholar] [CrossRef]
- Pontier, J.M.; Gempp, E.; Ignatescu, M. Blood platelet-derived microparticles release and bubble formation after an open-sea air dive. Appl. Physiol. Nutr. Metab. 2012, 37, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Eftedal, O.; Brubakk, A.O. Detecting intravascular gas bubbles in ultrasonic images. Med. Biol. Eng. Comput. 1993, 31, 627–633. [Google Scholar] [CrossRef]
- Ersson, A.; Linder, C.; Ohlsson, K.; Ekholm, A. Cytokine response after acute hyperbaric exposure in the rat. Undersea Hyperb. Med. 1998, 25, 217–221. [Google Scholar]
- Sureda, A.; Batle, J.M.; Ferrer, M.D.; Mestre-Alfaro, A.; Tur, J.A.; Pons, A. Scuba diving activates vascular antioxidant system. Int. J. Sports Med. 2012, 33, 531–536. [Google Scholar] [CrossRef]
- Zarezadeh, R.; Azarbayjani, M.A. The effect of air scuba dives up to a depth of 30 metres on serum cortisol in male divers. Diving Hyperb. Med. 2014, 44, 158–160. [Google Scholar]
- Zbinden-Foncea, H.; Raymackers, J.M.; Deldicque, L.; Renard, P.; Francaux, M. TLR2 and TLR4 activate p38 MAPK and JNK during endurance exercise in skeletal muscle. Med. Sci. Sports Exerc. 2012, 44, 1463–1472. [Google Scholar] [CrossRef]
- Nimmo, M.A.; Leggate, M.; Viana, J.L.; King, J.A. The effect of physical activity on mediators of inflammation. Diabetes Obes. Metab. 2013, 15, 51–60. [Google Scholar] [CrossRef]
- Spisni, E.; Marabotti, C.; De Fazio, L.; Valerii, M.C.; Cavazza, E.; Brambilla, S.; Hoxha, K.; L’Abbate, A.; Longobardi, P. A comparative evaluation of two decompression procedures for technical diving using inflammatory responses: Compartmental versus ratio deco. Diving Hyperb. Med. 2017, 47, 9–16. [Google Scholar] [CrossRef]
- von Hundelshausen, P.; Weber, K.S.; Huo, Y.; Proudfoot, A.E.; Nelson, P.J.; Ley, K.; Weber, C. RANTES deposition by platelets triggers monocyte arrest on inflamed and atherosclerotic endothelium. Circulation 2001, 103, 1772–1777. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Dong, J.; Lobe, C.G.; Gong, P.; Liu, J.; Liao, L. CCR5 facilitates endothelial progenitor cell recruitment and promotes the stabilization of atherosclerotic plaques in ApoE−/− mice. Stem Cell Res. Ther. 2015, 6, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Febbraio, M.A.; Pedersen, B.K. Muscle-derived interleukin-6: Mechanisms for activation and possible biological roles. FASEB J. 2002, 16, 1335–1347. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscle as an endocrine organ: Focus on muscle-derived interleukin-6. Physiol. Rev. 2008, 88, 1379–1406. [Google Scholar] [CrossRef] [Green Version]
- Tauler, P.; Gimeno, I.; Aguilo, A.; Guix, M.P.; Pons, A. Regulation of erythrocyte antioxidant enzyme activities in athletes during competition and short-term recovery. Pflug. Arch. 1999, 438, 782–787. [Google Scholar] [CrossRef]
- Wood, J.G. Oxygen Toxicity. In The Physiology and Medicine of Diving and Compressed Air Work, 2nd ed.; Bennett, P.D., Elliott, D.H., Eds.; Bailliere Tindall: London, UK, 1975. [Google Scholar]
- Fadhil, A.G.; Al-Asadi, J.N.; Ajee, N.A.H. Haematological Changes Among Divers. MJBU 2006, 24, 60–65. [Google Scholar] [CrossRef]
- Barak, M.; Katz, Y. Microbubbles: Pathophysiology and clinical implications. Chest 2005, 128, 2918–2932. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Ten Cate, H. Disseminated intravascular coagulation. N. Engl. J. Med. 1999, 341, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.R.; Ma, A.C.; Tavener, S.A.; McDonald, B.; Goodarzi, Z.; Kelly, M.M.; Patel, K.D.; Chakrabarti, S.; McAvoy, E.; Sinclair, G.D.; et al. Platelet TLR4 activates neutrophil extracellular traps to ensnare bacteria in septic blood. Nat. Med. 2007, 13, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Jacey, M.J.; Madden, R.O.; Tappan, D.V. Hemostatic alterations following severe dysbaric stress. Aerosp. Med. 1974, 45, 1062–1066. [Google Scholar]
- Tanoue, K.; Mano, Y.; Kuroiwa, K.; Suzuki, H.; Shibayama, M.; Yamazaki, H. Consumption of platelets in decompression sickness of rabbits. J. Appl. Physiol. 1987, 62, 1772–1779. [Google Scholar] [CrossRef]
- Philp, R.B. A review of blood changes associated with compression-decompression: Relationship to decompression sickness. Undersea Biomed. Res. 1974, 1, 117–150. [Google Scholar]
- Pontier, J.M.; Jimenez, C.; Blatteau, J.E. Blood platelet count and bubble formation after a dive to 30 msw for 30 min. Aviat. Space Environ. Med. 2008, 79, 1096–1099. [Google Scholar] [CrossRef] [PubMed]
- Gempp, E.; Blatteau, J.E. Risk factors and treatment outcome in scuba divers with spinal cord decompression sickness. J. Crit. Care 2010, 25, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Bosco, G.; Yang, Z.J.; Di Tano, G.; Camporesi, E.M.; Faralli, F.; Savini, F.; Landolfi, A.; Doria, C.; Fano, G. Effect of in-water oxygen prebreathing at different depths on decompression-induced bubble formation and platelet activation. J. Appl. Physiol. 2010, 108, 1077–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baj, Z.; Olszanski, R.; Majewska, E.; Konarski, M. The effect of air and nitrox divings on platelet activation tested by flow cytometry. Aviat. Space Environ. Med. 2000, 71, 925–928. [Google Scholar]

{kind=link}
{kind=link}
| Anthropometric Data | Means ± Ds | B vs. NB |
|---|---|---|
| Age | 45.0 ± 11.8 | N.S. 1 |
| Height | 173.4 ± 7.9 | N.S. |
| Weight | 79.7 ± 14.6 | N.S. |
| BMI | 26.4 ± 4.1 | N.S. |
| Dive Parameters | ||
| Maximum depth | 41.5 ± 0.5 | N.S. |
| Diving time | 50.4 ± 7.7 | N.S. |
| Temperature | 32.7 ± 1.2 | N.S. |
| Maximum GF at the end | 0.83 ± 0.03 | N.S. |
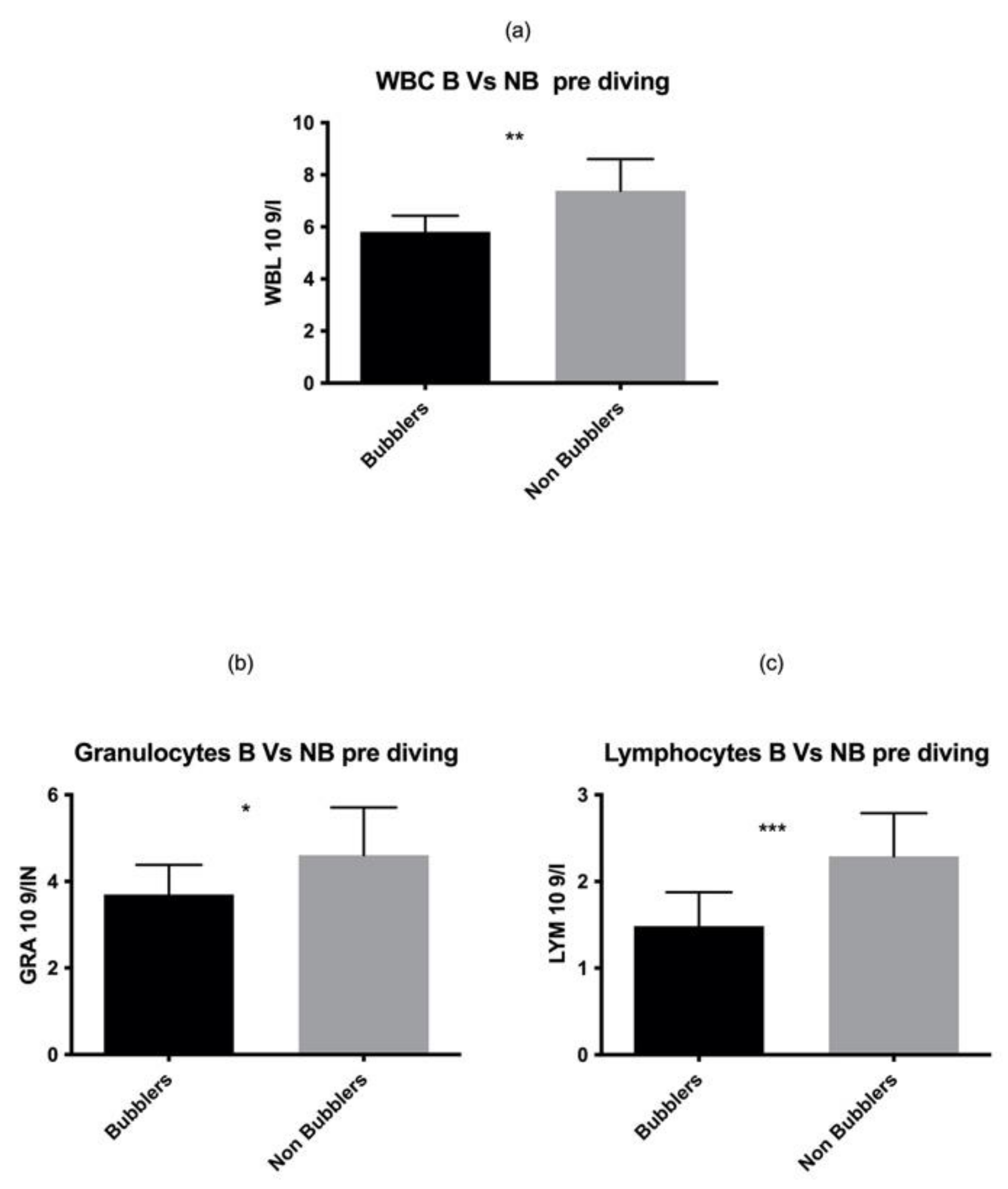
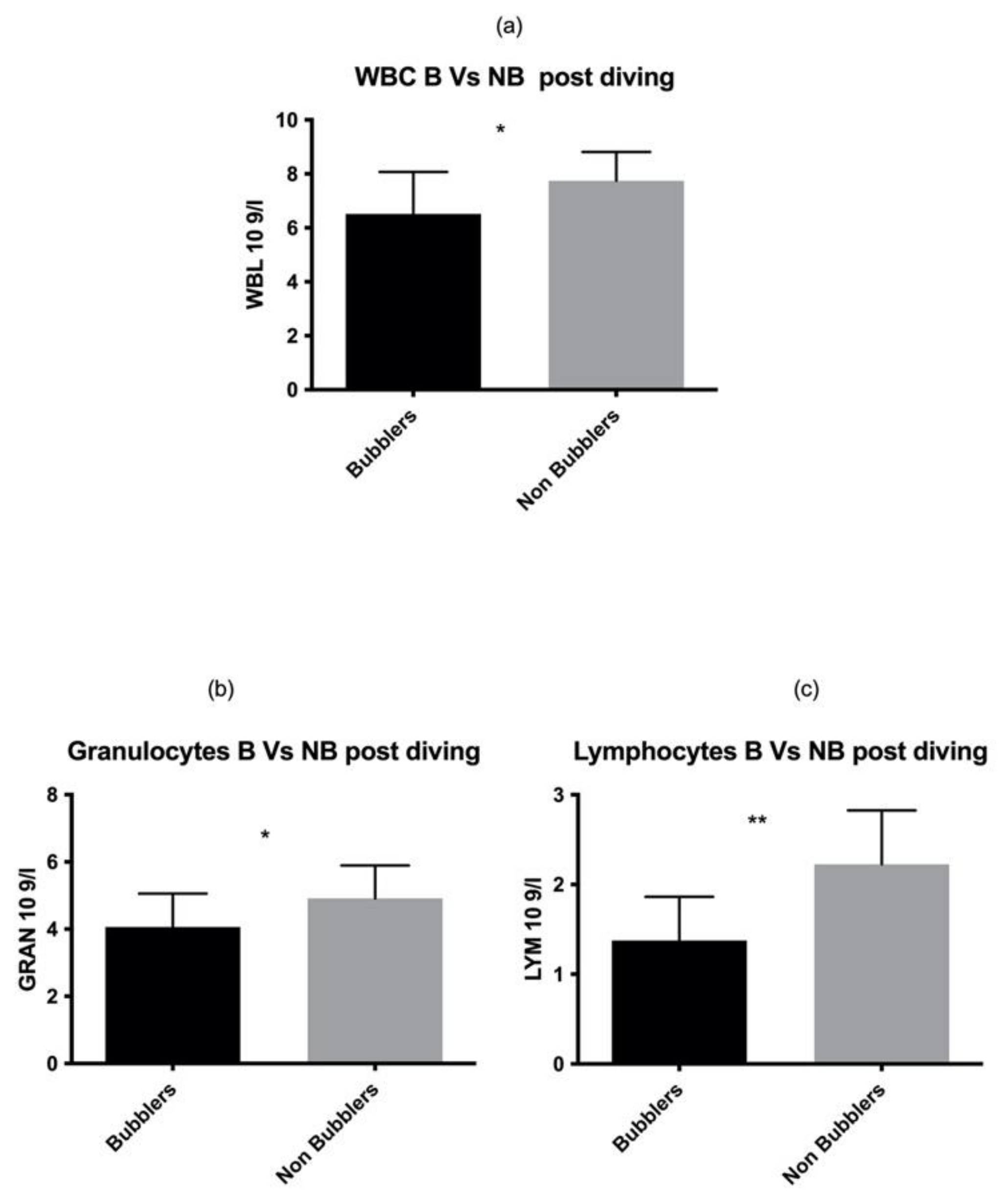
| White Series | B | NB | Results |
|---|---|---|---|
| WBC pre (109) | 5.81 ± 0.62 | 7.39 ± 1.21 | p = 0.001 |
| WBC post (109) | 6.51 ± 1.56 | 7.74 ± 1.07 | p = 0.021 |
| GRANs pre (109) | 3.70 ± 0.69 | 4.61 ± 1.01 | p = 0.031 |
| GRAN post (109) | 4.07 ± 0.99 | 4.92 ± 0.98 | p = 0.041 |
| LYM pre (109) | 1.49 ± 0.39 | 2.29 ± 0.50 | p = 0.0003 |
| LYM post (109) | 1.38 ± 0.49 | 2.23 ± 0.60 | p = 0.001 |
| MONO pre (109) | 0.39 ± 0.10 | 0.49 ± 0.12 | N.S. 1 |
| MONO post (109) | 0.42 ± 0.13 | 0.42 ± 0.11 | N.S. |
| Pre | Post | ||
| WBC (109) | 6.82 ± 1.23 | 7.32 ± 1.34 | p = 0.0050 |
| GRAN (109) | 4.19 ± 1.06 | 4.60 ± 1.00 | p = 0.001 |
| LYM (109) | 2.09 ± 0.62 | 2.00 ± 0.71 | N.S. |
| MONO (109) | 0.45 ± 0.13 | 0.43 ± 0.11 | N.S. |
| RBC | B | NB | Results |
|---|---|---|---|
| RBC pre (1012) | 5.13 ± 0.79 | 3.92 ± 0.95 | N.S. 1 |
| RBC post (1012) | 5.26 ± 0.56 | 5.20 ± 0.65 | N.S. |
| HGB pre (g/L) | 15.94 ± 1.60 | 15.02 ± 2.45 | N.S. |
| HGB post (g/L) | 15.74 ± 1.02 | 14.66 ± 1.05 | N.S. |
| MCV pre (fL) | 86.36 ± 3.85 | 85.49 ± 13.36 | N.S. |
| MCV post (fL) | 86.97 ± 3.90 | 83.78 ± 9.72 | N.S. |
| HCT pre (%) | 45.09 ± 2.82 | 42.88 ± 5.81 | N.S. |
| HCT post (%) | 45.48 ± 3.13 | 43.03 ± 3.75 | N.S. |
| MCH pre (pg) | 30.56 ± 1.90 | 28.83 ± 4.61 | N.S. |
| MCH post (pg) | 30.12 ± 2.34 | 28.47 ± 4.20 | N.S. |
| MCHC pre (g/L) | 35.14 ± 2.02 | 33.99 ± 2.20 | N.S. |
| MCHC post (g/L) | 34.64 ± 1.50 | 33.38 ± 3.22 | N.S. |
| Pre | Post | ||
| RBC(1012) | 5.12 ± 0.88 | 5.22 ± 0.61 | N.S. |
| HGB (g/L) | 15.32 ± 2.23 | 15.01 ±1.84 | p = 0.026 |
| MCV (fL) | 85.77 ± 11.11 | 84.77 ± 8.35 | p = 0.019 |
| HCT (%) | 43.59 ± 5.10 | 43.81 ±3.69 | N.S. |
| MCH (pg) | 29.38 ± 3.99 | 29.00 ± 3.74 | N.S. |
| MCHC pre (g/L) | 34.36 ± 2.17 | 33.79 ± 2.82 | N.S. |
| Platelet | B | NB | Results |
|---|---|---|---|
| PLT pre (109) | 183.20 ± 56.3 | 196.80 ± 70.9 | N.S. 1 |
| PLT post (109) | 198.8 ± 55.4 | 218.2 ± 67.6 | N.S. |
| MPV pre (fL) | 9.56 ± 0.92 | 9.29 ± 1.03 | N.S. |
| MPV pre (fL) | 9.20 ± 1.26 | 8.67 ± 1.17 | N.S. |
| PCT pre (%) | 0.17 ± 0.06 | 1.01 ± 3.63 | N.S. |
| PCT post (%) | 0.18 ± 0.05 | 0.19 ± 0.05 | N.S. |
| Pre | Post | ||
| PLT (109) | 192.5 ± 65.89 | 212.0 ± 63.56 | p = 0.01 |
| MPV (fL) | 12.56 ± 16.97 | 8.85 ± 1.20 | p = 0.0003 |
| PCT (%) | 0.74 ± 2.99 | 0.18 ± 0.05 | N.S. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cialoni, D.; Brizzolari, A.; Barassi, A.; Bosco, G.; Pieri, M.; Lancellotti, V.; Marroni, A. White Blood Cells, Platelets, Red Blood Cells and Gas Bubbles in SCUBA Diving: Is There a Relationship? Healthcare 2022, 10, 182. https://doi.org/10.3390/healthcare10020182
Cialoni D, Brizzolari A, Barassi A, Bosco G, Pieri M, Lancellotti V, Marroni A. White Blood Cells, Platelets, Red Blood Cells and Gas Bubbles in SCUBA Diving: Is There a Relationship? Healthcare. 2022; 10(2):182. https://doi.org/10.3390/healthcare10020182
Chicago/Turabian StyleCialoni, Danilo, Andrea Brizzolari, Alessandra Barassi, Gerardo Bosco, Massimo Pieri, Valentina Lancellotti, and Alessandro Marroni. 2022. "White Blood Cells, Platelets, Red Blood Cells and Gas Bubbles in SCUBA Diving: Is There a Relationship?" Healthcare 10, no. 2: 182. https://doi.org/10.3390/healthcare10020182
APA StyleCialoni, D., Brizzolari, A., Barassi, A., Bosco, G., Pieri, M., Lancellotti, V., & Marroni, A. (2022). White Blood Cells, Platelets, Red Blood Cells and Gas Bubbles in SCUBA Diving: Is There a Relationship? Healthcare, 10(2), 182. https://doi.org/10.3390/healthcare10020182