The Use of Dietary Interventions in Pediatric Patients

Abstract
1. Introduction
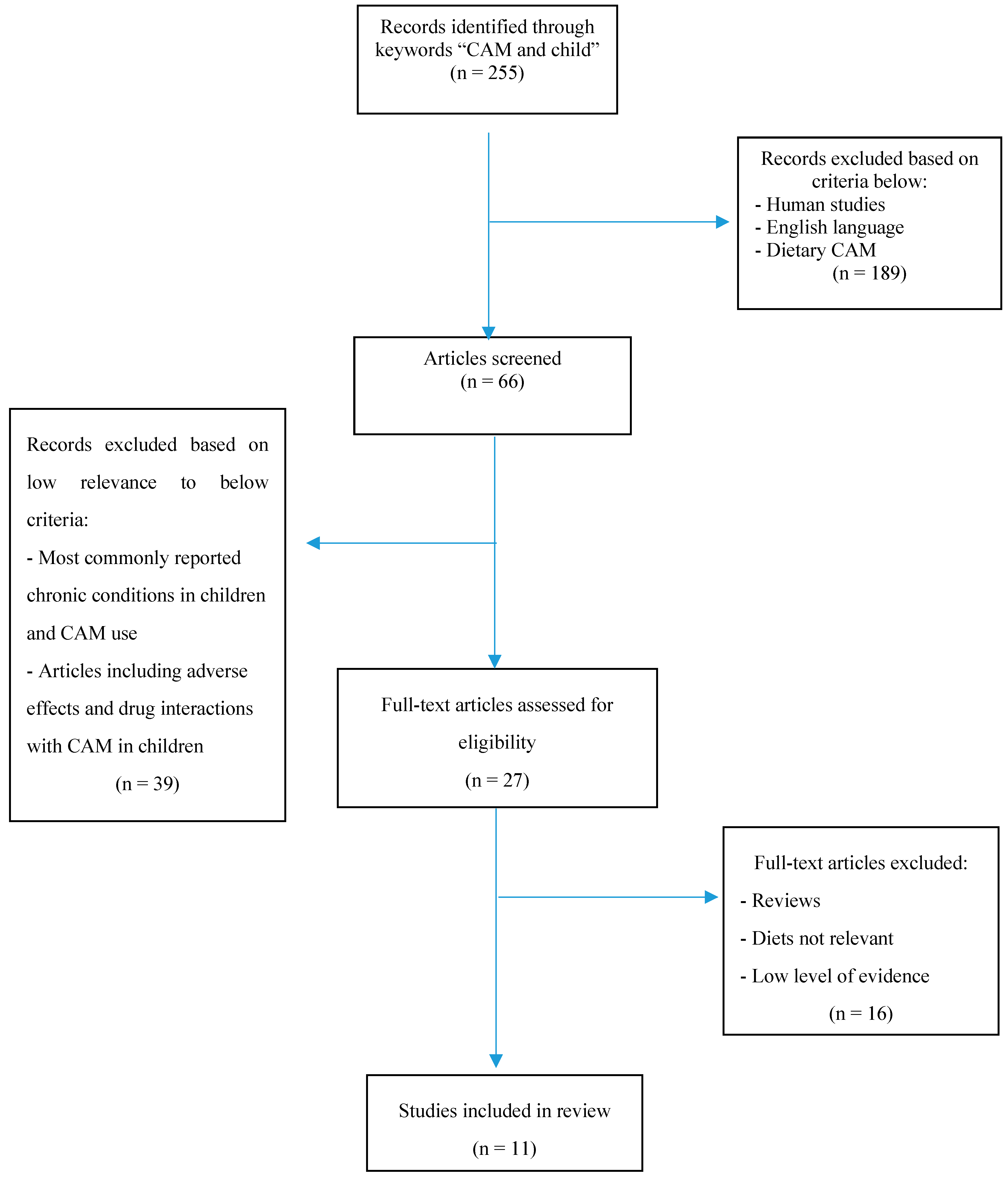
2. Review of the Literature
3. Ketogenic Diet for Epilepsy
4. Gluten-Free Casein-Free Diet for Autism Spectrum Disorder
5. Specific Carbohydrate Diet (low FODMAPs) for Irritable Bowel Syndrome
6. Dietary Interventions for ADHD
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Diet | Diet Modality | Target Condition | Evidence | Potential Adverse Effects | Pharmacist Considerations |
|---|---|---|---|---|---|
| Ketogenic Classic MCT Modified Atkins LGI | Calories from 90% fat and 10% carbohydrate and proteins Medium-chain triglycerides Long-chain triglycerides | Refractory Epilepsy | RCT’s and meta-analyses available show statistically significant positive results [16,17] | Vomiting, diarrhea, acidosis, dehydration, hypoglycemia, poor growth, kidney stones, vitamin deficiency, etc. | Monitor carbohydrate content in liquid formulations; bicarbonate levels; concomitant anticonvulsants |
| Gluten-free Casein-free | Exclusion of gluten and casein (e.g., products containing wheat, oats, barley, or rye; and milk and dairy products) | ASD | Results are inconclusive with weak evidence for positive effects. A subset of patient with GI disturbances may benefit [30,31,32,33,34] | Potential decrease in bone mass; deficiencies in essential amino acids, vitamin D, calcium, and protein | Counseling on vitamin supplementation; availability of gluten-free medications (both OTC and Rx) |
| Low FODMAPs | Exclusion of short-chain carbohydrates (wheat, rye, garlic, legumes, etc.) and sugar alcohols (mannitol, sorbitol, etc.) | IBS | Results are inconclusive with weak evidence for positive effects. Diet did show improvement in symptoms such as bloating, nausea, and abdominal pain. [39,40] | Diminished microflora; lack of fiber intake leading to constipation; possible effect on growth; eating disorders | Counseling on vitamin supplementation; monitor for presence of high-FODMAP excipients in medications (both OTC and Rx) |
| Feingold Oligoantigenic | Elimination of artificial food coloring, flavors, fragrances, preservatives and sweetners. Elimination of antigenic foods (diet restricted to hypoallergenic foods: turkey, pears, rice, lettuce, water) | ADHD | Meta-analyses showed weak or no evidence for positive effects. Children with severe ADHD may experience larger effects on symptom resolution. [58,59,60] | Possible vitamin, mineral, fiber and protein deficiencies | Counseling on vitamin supplementation; selection of medications without artificial dyes or sweeteners. |
References
- Black, L.I.; Clarke, T.C.; Barnes, P.M.; Stussman, B.J.; Nahin, R.L. Use of complementary health approaches among children aged 4–17 years in the United States: National Health Interview Survey, 2007–2012. Natl. Health Stat. Rep. 2015, 78, 1–19. [Google Scholar]
- Harris, P.E.; Cooper, K.L.; Relton, C.; Thomas, K.J. Prevalence of complementary and alternative medicine (CAM) use by the general population: A systematic review and update. Int. J. Clin. Pract. 2012, 66, 924–939. [Google Scholar] [CrossRef] [PubMed]
- Purohit, M.P.; Wells, R.E.; Zafonte, R.D.; Davis, R.B.; Phillips, R.S. Neuropsychiatric symptoms and the use of complementary and alternative medicine. Spine J. 2013, 13, 719. [Google Scholar] [CrossRef] [PubMed]
- Treat, L.; Liesinger, J.; Ziegenfuss, J.Y.; Humeniuk, K.; Prasad, K.; Tilburt, J.C. Patterns of complementary and alternative medicine use in children with common neurological conditions. Glob. Adv. Health Med. 2014, 3, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Akins, R.S.; Angkustsiri, K.; Hansen, R.L. Complementary and alternative medicine in autism: An evidence-based approach to negotiating safe and efficacious interventions with families. Neurotherapeutics 2010, 7, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Liptak, G.S. Complementary and alternative therapies for cerebral palsy. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Roizen, N.J. Complementary and alternative therapies for Down syndrome. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 149–155. [Google Scholar] [CrossRef]
- Wong, H.H.L.; Smith, R.G. Patterns of complementary and alternative medical therapy use in children diagnosed with autism spectrum disorders. J. Autism. Dev. Disord. 2006, 36, 901–909. [Google Scholar] [CrossRef]
- Sibinga, E.M.; Ottolini, M.C.; Duggan, A.K.; Wilson, M.H. Parent-pediatrician communication about complementary and alternative medicine use for children. Clin. Pediatr. 2004, 43, 367–373. [Google Scholar] [CrossRef]
- Pubmed. Available online: https://www.ncbi.nlm.nih.gov/pubmed (accessed on 10 January 2019).
- Lee, P.R.; Kossoff, E.H. Dietary treatments for epilepsy: Management guidelines for the general practitioner. Epilepsy Behav. 2011, 21, 115–121. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Zupec-Kania, B.A.; Amark, P.E.; Ballaban-Gil, K.R.; Christina Bergqvist, A.G.; Blackford, R.; Buchhalter, J.R.; Caraballo, R.H.; Helen Cross, J.; Dahlin, M.G.; et al. Optimal clinical management of children receiving the ketogenic diet: Recommendations of the International Ketogenic Diet Study Group. Epilepsia 2009, 50, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Selter, J.H.; Turner, Z.; Doerrer, S.C.; Kossoff, E.H. Dietary and Medication Adjustments to Improve Seizure Control in Patients Treated with the Ketogenic Diet. J. Child Neurol. 2015, 30, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Freeman, J.M.; Kossoff, E.H.; Hartman, A.L. The ketogenic diet: One decade later. Pediatrics 2007, 119, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Yudkoff, M.; Daikhin, Y.; Melo, T.M.; Nissim, I.; Sonnewald, U.; Nissim, I. The ketogenic diet and brain metabolism of amino acids: Relationship to the anticonvulsant effect. Ann. Rev. Nutr. 2007, 27, 415–430. [Google Scholar] [CrossRef] [PubMed]
- Parakh, M.; Katewa, V. Non-Pharmacologic Management of Epilepsy. Indian J. Pediatr. 2014, 81, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Henderson, C.B.; Filloux, F.M.; Alder, S.C.; Lyon, J.L.; Caplin, D.A. Efficacy of the ketogenic diet as a treatment option for epilepsy: Meta-analysis. J. Child Neurol. 2006, 21, 193–198. [Google Scholar]
- Neal, E.G.; Chaffe, H.M.; Schwartz, R.H.; Lawson, M.S.; Edwards, N.; Fitzsimmons, G.; Whitney, A.; Cross, J.H. The ketogenic diet in the treatment of epilepsy in children: A randomised, controlled trial. Lancet Neurol. 2008, 7, 500–506. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Krauss, G.L.; McGrogan, J.R. Efficacy of the Atkins diet as therapy for intractable epilepsy. Neurology 2003, 61, 1789–1791. [Google Scholar] [CrossRef]
- Kossoff, E.H.; McGrogan, J.R.; Bluml, R.M.; Pillas, D.J.; Rubenstein, J.E.; Vining, E.P. A modified atkins diet is effective for the treatment of intractable pediatric epilepsy. Epilepsia 2006, 47, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Wheless, J.W. The ketogenic diet: An effective medical therapy with side-effects. J. Child Neurol. 2001, 16, 633. [Google Scholar] [CrossRef]
- Runyon, A.M.; So, T.Y. The use of ketogenic diet in pediatric patients with epilepsy. ISRN Pediatr. 2012, 2012. [Google Scholar] [CrossRef]
- Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders: Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States 2008. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2012, 61, 1–19. [Google Scholar]
- American Psychiatric Association. Neurodevelopmental disorders. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Update; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- American Psychiatric Association. Pervasive developmental disorders. In Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Text Revision (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000; Volume 6970. [Google Scholar]
- Muhle, R.; Trentacoste, S.V.; Rapin, I. The genetics of autism. Pediatrics 2004, 113, e472. [Google Scholar] [CrossRef] [PubMed]
- Valicenti-McDermott, M.; McVicar, K.; Rapin, I.; Wershil, B.K.; Cohen, H.; Shinnar, S. Frequency of gastrointestinal symptoms et al. Frequency of gastrointestinal symptoms in children with autistic spectrum disorders and association with family history of autoimmune disease. J. Dev. Behav. Pediatr. 2006, 27, S128–S136. [Google Scholar] [CrossRef]
- Campbell, D.B.; Buie, T.M.; Winter, H.; Bauman, M.; Sutcliffe, J.S.; Perrin, J.M.; Levitt, P. Distinct genetic risk based on association of MET in families with co-occurring autism and gastrointestinal conditions. Pediatrics 2009, 123, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Elder, J.H. The gluten-free, casein-free diet in autism: An overview with clinical implications. Nutr. Clin. Pract. 2008, 23, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Hanson, E.; Kalish, L.; Bunce, E.; Curtis, C.; McDaniel, S.; Ware, J.; Petry, J. Use of complementary and alternative medicine among children diagnosed with autism spectrum disorder. J. Autism Dev. Disord. 2007, 37, 628–636. [Google Scholar] [CrossRef]
- Millward, C.; Ferriter, M.; Calver, S.; Connell-Jones, G. Gluten- and casein-free diets for autistic spectrum disorder. Cochrane Database Syst. Rev. 2008, 2, CD003498. [Google Scholar] [CrossRef]
- Johnson, C.; Handen, B.; Zimmer, M.; Sacco, K.; Turner, K. Effects of gluten free/casein free diet in young children with autism: A pilot study. J. Dev. Phys. Disabil. 2011, 23, 213–225. [Google Scholar] [CrossRef]
- Zhang, J.; Mayton, M.R.; Wheeler, J.J. Effectiveness of gluten-free and casein-free diets for individuals with autism spectrum disorders: An evidence-based research synthesis. Educ. Train. Autism Dev. Disabil. 2013, 48, 276–287. [Google Scholar]
- Greenspan, S.I.; Brazelton, T.B.; Cordero, J.; Solomon, R.; Bauman, M.L.; Robinson, R.; Shanker, S.; Breinbauer, C. Guidelines for Early Identification, Screening, and Clinical Management of Children with Autism Spectrum Disorders. Pediatrics 2008, 121, 828–830. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Mental Health (UK). Autism: The Management and Support of Children and Young People on the Autism Spectrum; NICE Clinical Guidelines National Institute for Health and Care Excellence (UK): London, UK, 2013. [Google Scholar]
- Dosma, C.; Adams, D.; Wudel, B.; Vogels, L.; Turner, J.; Vohra, S. Complementary, Holistic, and Integrative Medicine: Autism Spectrum Disorder and Gluten- and Casein-Free Diet. Pediatr. Rev. 2013, 34, e36. [Google Scholar] [CrossRef] [PubMed]
- Plogsted, S. Medications and Celiac Disease—Tips from a Pharmacist. Pract. Gastroenterol. 2007, 31, 58–64. [Google Scholar]
- National Foundation for Celiac Disease Awareness. Gluten in Medications for Patients. 2013. Available online: http://www.celiaccentral.org/Resources/Gluten-in-Medications/111/ (accessed on 12 September 2018).
- Rasquin, A.; Di Lorenzo, C.; Forbes, D.; Guiraldes, E.; Hyams, J.S.; Staiano, A.; Walker, L.S. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterology 2006, 130, 1527–1537. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012, 142, 46–54. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Irving, P.M.; Lomer, M.C.; Whelan, K. Mechanisms and efficacy of dietary FODMAP restriction in IBS. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 256–266. [Google Scholar] [CrossRef]
- Eswaran, S.; Farida, J.P.; Green, J.; Miller, J.D.; Chey, W.D. Nutrition in the management of gastrointestinal diseases and disorders: The evidence for the low FODMAP diet. Curr. Opin. Pharmacol. 2017, 37, 151–157. [Google Scholar] [CrossRef]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology 2014, 146, 67–75. [Google Scholar] [CrossRef]
- Gomara, R.E.; Halata, M.S.; Newman, L.J.; Bostwick, H.E.; Berezin, S.H.; Cukaj, L.; See, M.C.; Medow, M.S. Fructose intolerance in children presenting with abdominal pain. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 303–308. [Google Scholar] [CrossRef]
- Wintermeyer, P.; Baur, M.; Pilic, D.; Schmidt-Choudhury, A.; Zilbauer, M.; Wirth, S. Fructose malabsorption in children with recurrent abdominal pain: Positive effects of dietary treatment. Klin. Padiatr. 2012, 224, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Chumpitazi, B.P.; Weidler, E.M.; Shulman, R. A multi-substrate carbohydrate elimination diet decreases gastrointestinal symptoms in a subpopulation of children with IBS. Gastroenterology 2011, 140, S745. [Google Scholar] [CrossRef]
- Tilburg, M.A.; Felix, T. Diet and functional abdominal pain in children and adolescents. JPGN 2013, 57, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.S.; Gibson, P.R. Fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) and nonallergic food intolerance: FODMAPs or food chemicals? Ther. Adv. Gastroenterol. 2012, 5, 261. [Google Scholar] [CrossRef] [PubMed]
- Swanson, J.M.; Sergeant, J.A.; Taylor, E.; Sonuga-Barke, E.J.S.; Jensen, P.S.; Cantwell, D.P. Attention-deficit hyperactivity disorder and hyperkinetic disorder. Lancet 1998, 351, 429–433. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Biederman, J.; Monuteaux, M.C.; Mick, E.; Spencer, T.; Wilens, T.E.; Silva, J.M.; Snyder, L.E.; Faraone, S.V. Young adult outcome of attention deficit hyperactivity disorder: A controlled 10-year follow-up study. Psychol. Med. 2006, 36, 167–179. [Google Scholar] [CrossRef]
- Feingold, B.F. Why Your Child Is Hyperactive; Random House: New York, NY, USA, 1975. [Google Scholar]
- Harley, J.P.; Ray, R.S.; Tomasi, L.; Eichman, P.L.; Matthews, C.G.; Chun, R.; Cleeland, C.S.; Traisman, E. Hyperkinesis and food additives: Testing the Feingold hypothesis. Pediatrics 1978, 61, 818–828. [Google Scholar]
- Kanarek, R.B. Artificial food dyes and attention deficit hyperactivity disorder. Nutr. Rev. 2011, 69, 385–391. [Google Scholar] [CrossRef]
- Nigg, J.T.; Lewis, K.; Edinger, T.; Falk, M. Meta-analysis of attention-deficit/hyperactivity disorder or attention-deficit/hyperactivity disorder symptoms, restriction diet, and synthetic food color additives. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 86–97. [Google Scholar] [CrossRef]
- Pelsser, L.M.; Frankena, K.; Toorman, J.; Savelkoul, H.F.; Dubois, A.E.; Pereira, R.R.; Haagen, T.A.; Rommelse, N.N.; Buitelaar, J.K. Effects of a restricted elimination diet on the behaviour of children with attention-deficit hyperactivity disorder (INCA study): A randomised controlled trial. Lancet 2011, 377, 494–503. [Google Scholar] [CrossRef]
- Ly, V.; Bottelier, M.; Hoekstra, P.J.; Arias Vasquez, A.; Buitelaar, J.K.; Rommelse, N.N. Elimination diets’ efficacy and mechanisms in attention deficit hyperactivity disorder and autism spectrum disorder. Eur. Child Adolesc. Psychiatry 2017, 26, 1067–1079. [Google Scholar] [CrossRef] [PubMed]
- Grimshaw, K.E. Dietary management of food allergy in children. Proc. Nutr. Soc. 2006, 65, 412–417. [Google Scholar] [PubMed]
- Sonuga-Barke, E.J.; Brandeis, D.; Cortese, S.; Daley, D.; Ferrin, M.; Holtmann, M.; Stevenson, J.; Danckaerts, M.; van der Oord, S.; Döpfner, M.; et al. Nonpharmacological interventions for ADHD: Systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am. J. Psychiatry 2013, 170, 275–289. [Google Scholar] [CrossRef] [PubMed]

| Dosage Unit | |
|---|---|
| Acetaminophen liquid suspension (cherry) (Tylenol) | 160 mg/5 mL |
| Acetaminophen elixir with codeine (Tylenol with Codeine) × 0.35 g ethyl alcohol/5 mL | 120 mg/5 mL |
| Amoxicillin oral suspension (Trimox) | 125 mg/5 mL |
| Ampicillin oral suspension (Omnipen) | 125 mg/5 mL |
| Carbamazepine suspension (TEGretol) | 100 mg/5 mL |
| Cephalexin oral suspension (Keflex) | 125 mg/5 mL |
| Phenobarbital elixir ×0.71 g ethyl alcohol/5 mL | 20 mg/5 mL |
| Valproic acid syrup (Depakene) | 250 mg/5 mL |
| Excipient | Gluten-Free Botanical Source | Gluten Containing Botanical Source |
|---|---|---|
| Starch | Corn, potato, tapioca | Wheat |
| Pregelatinized starch, pregelatinized modified starch, sodium starch glycolate | Corn, rice, potato | Wheat |
| Dextrans | Corn, potato | Wheat, barley |
| Dextrose | Corn | Wheat, barley |
| Dextrates, dextrins | Corn, potato | Wheat, barley |
| Maltodextrin | Corn, potato | Wheat, barley |
| Caramel coloring | Corn | Barley malt |
| List of medications verified to be gluten-free | www.glutenfreedrugs.com |
| “A guide through the Medicine Cabinet” (book) | In print |
| Walgreens and CVS pharmacy OTC brand medication list | Available upon request |
| Additional information on gluten in foods and products | www.celiac.org www.celiaccentral.org |
| Fructo-oligosaccharides (fructans) | Wheat, rye, onions, garlic, artichokes |
| Galacto-oligosaccharides (GOS) | Legumes |
| Lactose | Milk and milk products |
| Fructose | Honey, apples, pears, watermelon, mango |
| Sorbitol | Apples, pears, stone fruits, sugar-free mints/gums |
| Mannitol | Mushrooms, cauliflower, sugar-free mints/gums |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madzhidova, S.; Sedrakyan, L. The Use of Dietary Interventions in Pediatric Patients. Pharmacy 2019, 7, 10. https://doi.org/10.3390/pharmacy7010010
Madzhidova S, Sedrakyan L. The Use of Dietary Interventions in Pediatric Patients. Pharmacy. 2019; 7(1):10. https://doi.org/10.3390/pharmacy7010010
Chicago/Turabian StyleMadzhidova, Shirin, and Lusine Sedrakyan. 2019. "The Use of Dietary Interventions in Pediatric Patients" Pharmacy 7, no. 1: 10. https://doi.org/10.3390/pharmacy7010010
APA StyleMadzhidova, S., & Sedrakyan, L. (2019). The Use of Dietary Interventions in Pediatric Patients. Pharmacy, 7(1), 10. https://doi.org/10.3390/pharmacy7010010