

The Potential Mechanisms behind Loperamide-Induced Cardiac Arrhythmias Associated with Human Abuse and Extreme Overdose

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Compounds
2.2. Ion-Channel Screening of hERG, Nav1.5, and Cav1.2
2.3. In Silico Modeling
2.4. Isolated Arterially Perfused Rabbit Ventricular Wedge and Electrophysiological Recordings
2.5. Anesthetized Guinea Pigs
2.6. Plasma Protein Binding Determinations
2.7. Analysis of Well or Bath Loperamide Concentrations
2.8. Cardiac Safety Margin Calculations
3. Results
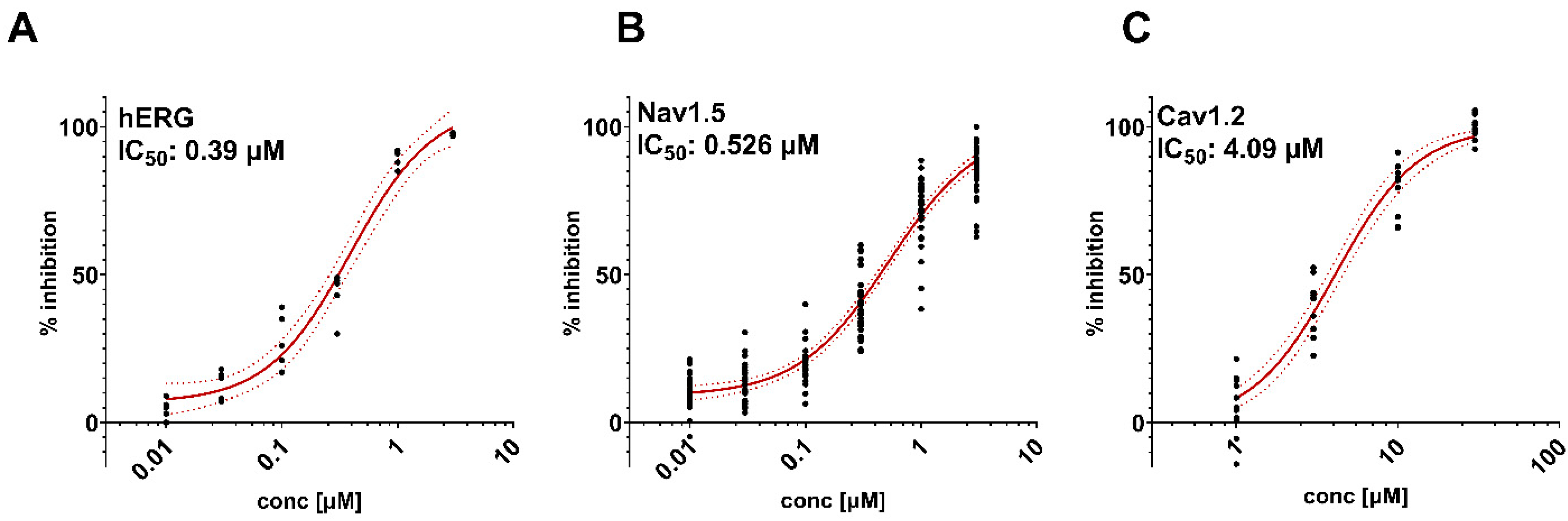
3.1. Effects of Loperamide on Cardiac Ion Channels
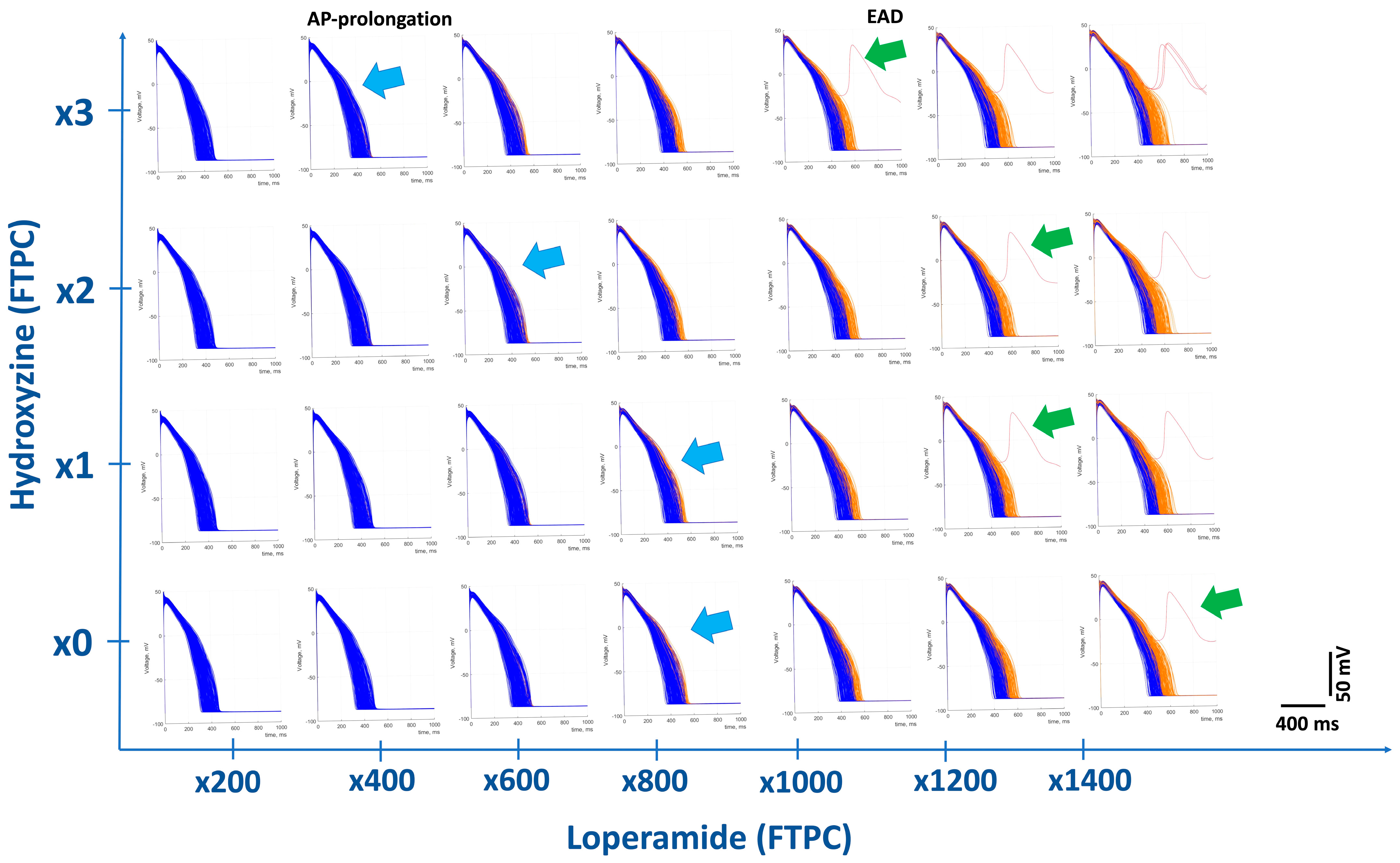
3.2. In Silico Modeling of Loperamide Effects on Human Cardiac Action Potentials
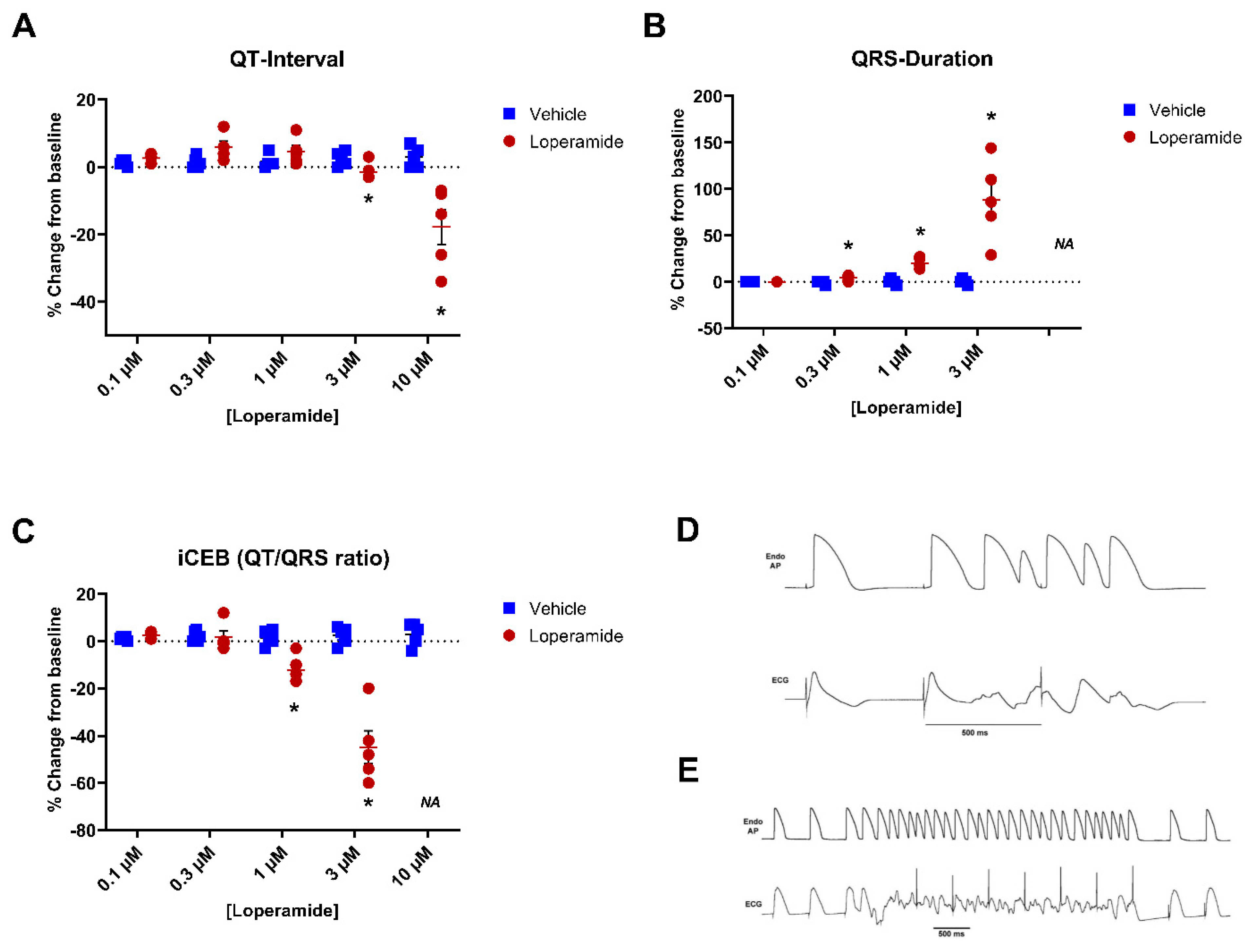
3.3. Isolated Arterially Perfused Rabbit Left Ventricular Wedge
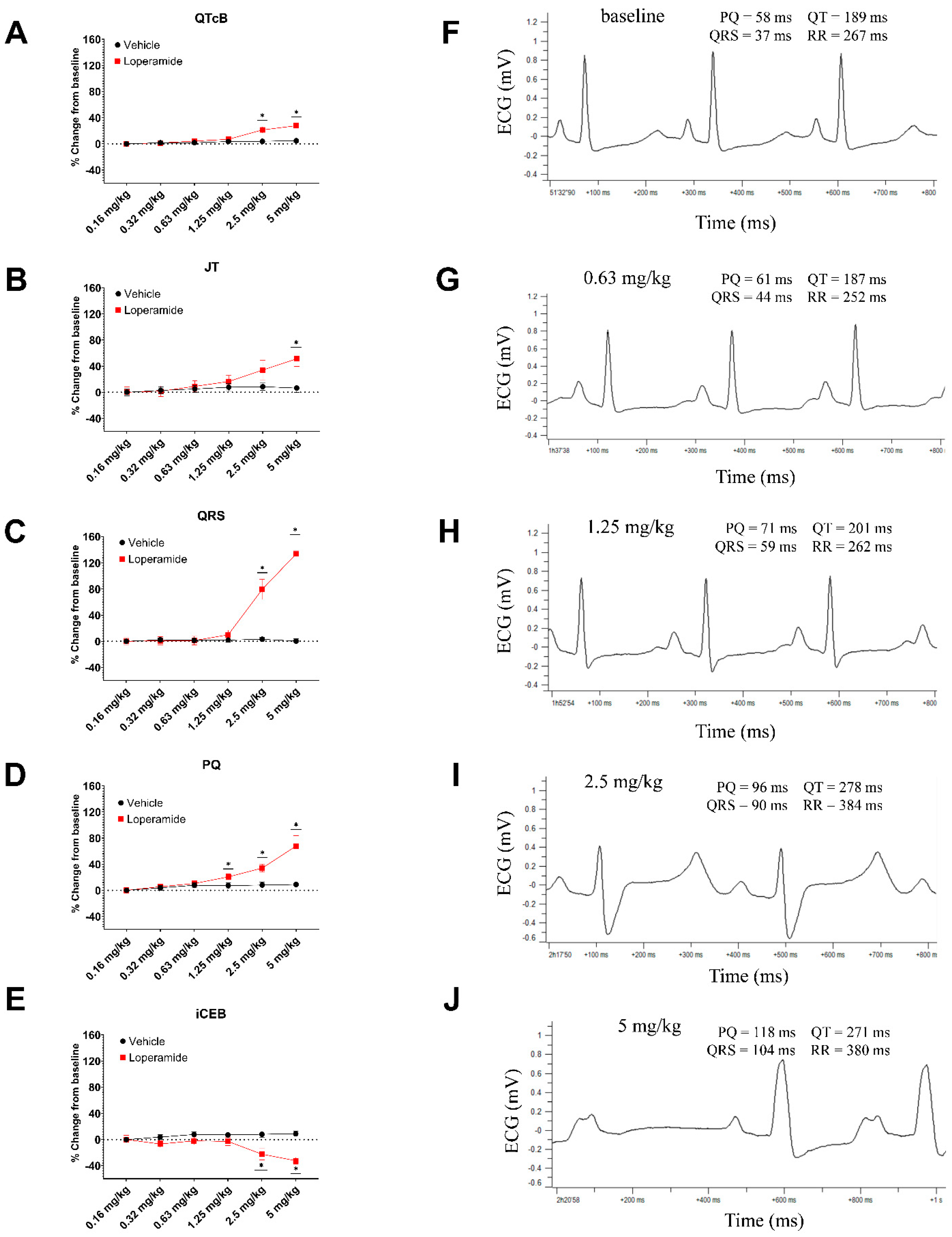
3.4. Anesthetized Guinea Pigs
3.5. Plasma Protein Binding
3.6. Safety Margin Calculations
4. Discussion
4.1. Safety Margins over Loperamide’s Free Therapeutic Peak Concentration (FTPC)
4.2. Relationship between Exposures for Nonclinical Cardiotoxicity and Plasma Levels Associated with Intentional Overdose
- (1)
- Concomitant medications as well as underlying conditions (e.g., hypokalemia) may alter the sensitivity to loperamide’s actions. Concomitant medications in reported cases included sotalol, nintedanib, methadone, amitriptyline, fluoxetine, clonazepam, and alprazolam, etc., [37], which are known to have direct effects on cardiac ion-channels (e.g., hERG) and may induce long QT and TdP in humans by themselves. In addition, drug misusers often took P-glycoprotein inhibitors to increase brain levels of loperamide to achieve an opiate “high” (e.g., ketoconazole, fluoxetine, citalopram, omeprazole, quinine, verapamil, erythromycin, Hydroxyzine). Many of these P-glycoprotein inhibitors also directly affect ventricular depolarization and repolarization (QT-interval) [12,71].
- (2)
- As previously mentioned, the available estimates of loperamide exposure associated with overdose cases were not systematically collected and were taken at varying times after loperamide ingestion or the presentation of cardiac toxicity, suggesting the actual peak concentrations may have been much higher at the time of events.
- (3)
- Loperamide, a substrate for P-glycoprotein [4,72], may saturate this transporter at toxic concentrations or in the presence of other drugs that inhibit P-glycoprotein [73,74], resulting in significantly higher plasma levels. As this transporter also excludes loperamide from cardiac cells, intracellular levels may be significantly higher [75].
- (4)
- In vitro or in silico studies do not account for the potential pharmacological activity of metabolites. Two human metabolites of loperamide (N-desmethyl loperamide and N-hydroxymethyl-mono-desmethylloperamide) are generated at levels greater than the parent drug. In two overdose cases, desmethyl loperamide concentrations were 5- to 8-fold the parent levels [28]. Desmethylloperamide has been shown to inhibit hERG with an IC50 of 245 nM and INa with an IC50 of 483 nM [76] and therefore may accentuate the ion channel effects of loperamide itself in the heart.
- (5)
- Compound solubility in aqueous buffer and variable drug adherence to the perfusate tubing and apparatus used in in vitro studies potentially limit actual testing exposure, leading to potential underestimates of potency and the overestimating of safety margins. For the internal hERG assessments, the recovery of loperamide in the perfusate ranged from 43 to 60%, and comparable recovery was found in the isolated rabbit ventricular wedge experiments.
- (6)
- Significant physiological consequences of ion-channel inhibition (ie., effects on conduction and repolarization) have been documented to occur at much lower levels of channel inhibition (e.g., IC10 to IC20) for both IKr [77] and for INa [38,78]. The safety margin was 186-fold when we applied the IC10 value of hERG.
4.3. Potential Mechanisms of Cardiac Arrhythmias Associated with Abuse and Extreme Overdose of Loperamide
4.4. In Silico Assessment of Loperamide Cardiotoxicity at Concentrations Associated with Overdose
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- DeHaven-Hudkins, D.L.; Burgos, L.C.; Cassel, J.A.; Daubert, J.D.; DeHaven, R.N.; Mansson, E.; Nagasaka, H.; Yu, G.; Yaksh, T. Loperamide (ADL 2-1294), an opioid antihyperalgesic agent with peripheral selectivity. J. Pharmacol. Exp. Ther. 1999, 289, 494–502. [Google Scholar] [PubMed]
- Baker, D.E. Loperamide: A pharmacological review. Rev. Gastroenterol. Disord. 2007, 7 (Suppl. S3), S11–S18. [Google Scholar] [PubMed]
- Awouters, F.; Megens, A.; Verlinden, M.; Schuurkes, J.; Niemegeers, C.; Janssen, P.A. Loperamide. Survey of studies on mechanism of its antidiarrheal activity. Dig. Dis. Sci. 1993, 38, 977–995. [Google Scholar] [CrossRef]
- Vandenbossche, J.; Huisman, M.; Xu, Y.; Sanderson-Bongiovanni, D.; Soons, P. Loperamide and P-glycoprotein inhibition: Assessment of the clinical relevance. J. Pharm. Pharmacol. 2010, 62, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Litovitz, T.; Clancy, C.; Korberly, B.; Temple, A.R.; Mann, K.V. Surveillance of loperamide ingestions: An analysis of 216 poison center reports. J. Toxicol. Clin. Toxicol. 1997, 35, 11–19. [Google Scholar] [CrossRef]
- Li, S.T.; Grossman, D.C.; Cummings, P. Loperamide therapy for acute diarrhea in children: Systematic review and meta-analysis. PLoS Med. 2007, 4, e98. [Google Scholar] [CrossRef]
- Ericsson, C.D.; Johnson, P.C. Safety and efficacy of loperamide. Am. J. Med. 1990, 88, 10S–14S. [Google Scholar] [CrossRef]
- Swank, K.A.; Wu, E.; Kortepeter, C.; McAninch, J.; Levin, R.L. Adverse event detection using the FDA post-marketing drug safety surveillance system: Cardiotoxicity associated with loperamide abuse and misuse. J. Am. Pharm. Assoc. 2017, 57, S63–S67. [Google Scholar] [CrossRef]
- Daniulaityte, R.; Carlson, R.; Falck, R.; Cameron, D.; Perera, S.; Chen, L.; Sheth, A. “I just wanted to tell you that loperamide WILL WORK”: A web-based study of extra-medical use of loperamide. Drug Alcohol. Depend. 2013, 130, 241–244. [Google Scholar] [CrossRef]
- MacDonald, R.; Heiner, J.; Villarreal, J.; Strote, J. Loperamide dependence and abuse. BMJ Case Rep. 2015, 2015, bcr2015209705. [Google Scholar] [CrossRef]
- Vakkalanka, J.P.; Charlton, N.P.; Holstege, C.P. Epidemiologic Trends in Loperamide Abuse and Misuse. Ann. Emerg. Med. 2017, 69, 73–78. [Google Scholar] [CrossRef]
- Wu, P.E.; Juurlink, D.N. Clinical Review: Loperamide Toxicity. Ann. Emerg. Med. 2017, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Schifano, F.; Chiappini, S. Is there such a thing as a ‘lope’ dope? Analysis of loperamide-related European Medicines Agency (EMA) pharmacovigilance database reports. PLoS ONE 2018, 13, e0204443. [Google Scholar] [CrossRef] [PubMed]
- Ollitrault, P.; Dolladille, C.; Chrétien, B.; Milliez, P.; Alexandre, J. Cardiovascular Toxicities Associated With Loperamide. Circulation 2021, 143, 403–405. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S.; Fayyaz, S.M.; Saeed, Y.; Aqeel, M. Loperamide-induced cardiotoxicity: A case overlooked? BMJ Case Rep. 2021, 14, e243325. [Google Scholar] [CrossRef] [PubMed]
- Tayeb, T.; Dalia, T.; Hegde, V.; Cotter, E.; Zoubek, S.; Vidic, A. Cryptic cardiogenic shock-long term loperamide abuse presenting with biventricular failure and failure to pace. J. Am. Coll. Cardiol. 2022, 79, 2560. [Google Scholar] [CrossRef]
- Miller, H.; Panahi, L.; Tapia, D.; Tran, A.; Bowman, J.D. Loperamide misuse and abuse. J. Am. Pharm. Assoc. 2017, 57, S45–S50. [Google Scholar] [CrossRef]
- Marraffa, J.M.; Holland, M.G.; Sullivan, R.W.; Morgan, B.W.; Oakes, J.A.; Wiegand, T.J.; Hodgman, M.J. Cardiac conduction disturbance after loperamide abuse. Clin. Toxicol. 2014, 52, 952–957. [Google Scholar] [CrossRef]
- Enakpene, E.O.; Riaz, I.B.; Shirazi, F.M.; Raz, Y.; Indik, J.H. The long QT teaser: Loperamide abuse. Am. J. Med. 2015, 128, 1083–1086. [Google Scholar] [CrossRef]
- Spinner, H.L.; Lonardo, N.W.; Mulamalla, R.; Stehlik, J. Ventricular tachycardia associated with high-dose chronic loperamide use. Pharmacotherapy 2015, 35, 234–238. [Google Scholar] [CrossRef]
- Eggleston, W.; Nacca, N.; Marraffa, J.M. Loperamide toxicokinetics: Serum concentrations in the overdose setting. Clin. Toxicol. 2015, 53, 495–496. [Google Scholar] [CrossRef]
- Mancano, M.A. High-Dose Loperamide Abuse Inducing Life-Threatening Cardiac Arrhythmias; Topiramate-Induced Diarrhea in a Breastfed Infant; Danazol-Induced Stevens-Johnson Syndrome; Asenapine-Induced Myasthenic Syndrome; Black Hairy Tongue Due to Linezolid; Adalimumab-Induced Priapism. Hosp. Pharm. 2015, 50, 351–355. [Google Scholar] [CrossRef]
- Dierksen, J.; Gonsoulin, M.; Walterscheid, J.P. Poor Man’s Methadone: A Case Report of Loperamide Toxicity. Am. J. Forensic Med. Pathol. 2015, 36, 268–270. [Google Scholar] [CrossRef] [PubMed]
- Wightman, R.S.; Hoffman, R.S.; Howland, M.A.; Rice, B.; Biary, R.; Lugassy, D. Not your regular high: Cardiac dysrhythmias caused by loperamide. Clin. Toxicol. 2016, 54, 454–458. [Google Scholar] [CrossRef]
- Marzec, L.N.; Katz, D.F.; Peterson, P.N.; Thompson, L.E.; Haigney, M.C.; Krantz, M.J. Torsades de pointes associated with high-dose loperamide ingestion. J. Innov. Card. Rhythm. Manag. 2015, 6, 1897–1899. [Google Scholar]
- Boppana, V.S.; Kahlon, A.; Bhatta, L. Ventricular tachycardia storm - can it be a side-effect from over the counter anti- diarrheal? Crit. Care Med. 2012, 40, 1204. [Google Scholar] [CrossRef]
- Pokhrel, K.; Rajbhandary, A.; Thapa, J. Loperamide The Unexpected Culprit. Crit. Care Med. 2013, 41, A328. [Google Scholar] [CrossRef]
- Katz, K.D.; Cannon, R.D.; Cook, M.D.; Amaducci, A.; Day, R.; Enyart, J.; Burket, G.; Porter, L.; Roach, T.; Janssen, J.; et al. Loperamide-Induced Torsades de Pointes: A Case Series. J. Emerg. Med. 2017, 53, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Rasla, S.; Parikh, P.; Hoffmeister, P.; St Amand, A.; Garas, M.K.; El Meligy, A.; Minami, T.; Shah, N.R. Unexpected Serious Cardiac Arrhythmias in the Setting of Loperamide Abuse. Rhode Isl. Med. J. 2017, 100, 33–36. [Google Scholar]
- Salama, A.; Levin, Y.; Jha, P.; Alweis, R. Ventricular fibrillation due to overdose of loperamide, the "poor man's methadone". J. Community Hosp. Intern. Med. Perspect. 2017, 7, 222–226. [Google Scholar] [CrossRef]
- Teigeler, T.; Stahura, H.; Alimohammad, R.; Kalahasty, G.; Koneru, J.N.; Ellenbogen, M.; Ellenbogen, K.A.; Padala, S.K. Electrocardiographic Changes in Loperamide Toxicity: Case Report and Review of Literature. J. Cardiovasc. Electrophysiol. 2019, 20, 14129. [Google Scholar] [CrossRef]
- Simon, M.; Rague, J. A Case Report of Torsade de Pointes and Brugada Pattern Associated with Loperamide Misuse and Supratherapeutic Loperamide Concentrations. J. Emerg. Med. 2021, 61, e54–e59. [Google Scholar] [CrossRef] [PubMed]
- Rojas, S.F.; Oglat, A.; Bonilla, H.M.G.; Jeroudi, O.; Sharp, W.; Valderrábano, M.; Schurmann, P.A. Loperamide Mimicking Brugada Pattern. Methodist. DeBakey Cardiovasc. J. 2018, 14, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Lammoglia, B.C.; Hasselmann, G.; Pires-Oliveira, M.; Duarte Nicolau, L.A.; Rolim Medeiros, J.V.; Sabia Tallo, F.; Omar Taha, M.; Yamaguti Lima, R.; Caricati-Neto, A.; Menezes-Rodrigues, F.S. Risk of Cardiac Lesion with Chronic and Acute Use of Loperamide-An Integrative Review. J. Cardiovasc. Dev. Dis. 2022, 9, 431. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhou, P.; He, N.; Zhai, S. Drug-induced torsades de pointes: Disproportionality analysis of the United States Food and Drug Administration adverse event reporting system. Front. Cardiovasc. Med. 2022, 9, 966331. [Google Scholar] [CrossRef]
- Krumpholz, L.; Wiśniowska, B.; Polak, S. Correction to: Open-access database of literature derived drug-related Torsade de Pointes cases. BMC Pharmacol. Toxicol. 2022, 23, 11. [Google Scholar] [CrossRef]
- Sahu, K.K.; El Meligy, A.; Mishra, A.K.; Goyal, S. A tale of twists: Loperamide-induced torsades de pointes and ventricular tachycardia storm. BMJ Case Rep. 2020, 13, 1. [Google Scholar] [CrossRef]
- Harmer, A.R.; Valentin, J.P.; Pollard, C.E. On the relationship between block of the cardiac Na(+) channel and drug-induced prolongation of the QRS complex. Br. J. Pharmacol. 2011, 164, 260–273. [Google Scholar] [CrossRef]
- Kang, J.; Compton, D.R.; Vaz, R.J.; Rampe, D. Proarrhythmic mechanisms of the common anti-diarrheal medication loperamide: Revelations from the opioid abuse epidemic. Naunyn-Schmiedeberg's Arch. Pharmacol. 2016, 389, 1133–1137. [Google Scholar] [CrossRef]
- Klein, M.G.; Haigney, M.C.P.; Mehler, P.S.; Fatima, N.; Flagg, T.P.; Krantz, M.J. Potent Inhibition of hERG Channels by the Over-the-Counter Antidiarrheal Agent Loperamide. JACC Clin. Electrophysiol. 2016, 2, 784–789. [Google Scholar] [CrossRef]
- Sheng, J.; Tran, P.N.; Li, Z.; Dutta, S.; Chang, K.; Colatsky, T.; Wu, W.W. Characterization of loperamide-mediated block of hERG channels at physiological temperature and its proarrhythmia propensity. J. Pharmacol. Toxicol. Methods 2017, 19, 30091–30094. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.M. Drug-induced prolongation of the QT interval. N. Engl. J. Med. 2004, 350, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Sanguinetti, M.C.; Jiang, C.; Curran, M.E.; Keating, M.T. A mechanistic link between an inherited and an acquired cardiac arrhythmia and HERG encodes the IKr potassium channel. Cell 1995, 81, 299–307. [Google Scholar] [CrossRef]
- Lu, H.R.; Rohrbacher, J.; Vlaminckx, E.; Van Ammel, K.; Yan, G.X.; Gallacher, D.J. Predicting drug-induced slowing of conduction and pro-arrhythmia: Identifying the 'bad' sodium current blockers. Br. J. Pharmacol. 2010, 160, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Nattel, S. Experimental evidence for proarrhythmic mechanisms of antiarrhythmic drugs. Cardiovasc. Res. 1998, 37, 567–577. [Google Scholar] [CrossRef]
- Wilde, A. Proarrhythmia related to sodium channel blockade: Mechanisms, monitory and prevention and management. Card. Electrophysiol. Rev. 1998, 2, 136–141. [Google Scholar] [CrossRef]
- Lu, H.R.; Vlaminckx, E.; Van de Water, A.; Rohrbacher, J.; Hermans, A.; Gallacher, D.J. Corrigendum to “In vitro experimental models for the risk assessment of antibiotic-induced QT prolongation” [European Journal of Pharmacology 553 (2007) 229–239]. Eur. J. Pharmacol. 2007, 577, 221. [Google Scholar] [CrossRef]
- Britton, O.J.; Bueno-Orovio, A.; Van Ammel, K.; Lu, H.R.; Towart, R.; Gallacher, D.J.; Rodriguez, B. Experimentally calibrated population of models predicts and explains intersubject variability in cardiac cellular electrophysiology. Proc. Natl. Acad. Sci. USA 2013, 110, E2098–E2105. [Google Scholar] [CrossRef]
- Passini, E.; Britton, O.J.; Lu, H.R.; Rohrbacher, J.; Hermans, A.N.; Gallacher, D.J.; Greig, R.J.H.; Bueno-Orovio, A.; Rodriguez, B. Human In Silico Drug Trials Demonstrate Higher Accuracy than Animal Models in Predicting Clinical Pro-Arrhythmic Cardiotoxicity. Front. Physiol. 2017, 8, 668. [Google Scholar] [CrossRef]
- Paci, M.; Koivumäki, J.T.; Lu, H.R.; Gallacher, D.J.; Passini, E.; Rodriguez, B. Comparison of the Simulated Response of Three in Silico Human Stem Cell-Derived Cardiomyocytes Models and in Vitro Data Under 15 Drug Actions. Front. Pharmacol. 2021, 12, 604713. [Google Scholar] [CrossRef]
- Danielsson, B.; Collin, J.; Nyman, A.; Bergendal, A.; Borg, N.; State, M.; Bergfeldt, L.; Fastbom, J. Drug use and torsades de pointes cardiac arrhythmias in Sweden: A nationwide register-based cohort study. BMJ Open 2020, 10, e034560. [Google Scholar] [CrossRef]
- Schlit, A.F.; Delaunois, A.; Colomar, A.; Claudio, B.; Cariolato, L.; Boev, R.; Valentin, J.P.; Peters, C.; Sloan, V.S.; Bentz, J.W.G. Risk of QT prolongation and torsade de pointes associated with exposure to hydroxyzine: Re-evaluation of an established drug. Pharmacol. Res. Perspect. 2017, 5, e00309. [Google Scholar] [CrossRef]
- Blinova, K.; Stohlman, J.; Vicente, J.; Chan, D.; Johannesen, L.; Hortigon-Vinagre, M.P.; Zamora, V.; Smith, G.; Crumb, W.J.; Pang, L.; et al. Comprehensive Translational Assessment of Human-Induced Pluripotent Stem Cell Derived Cardiomyocytes for Evaluating Drug-Induced Arrhythmias. Toxicol. Sci. 2017, 155, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, K.; Nagatomo, T.; Abe, H.; Kikuchi, K.; Takemasa, H.; Anson, B.D.; Delisle, B.P.; January, C.T.; Nakashima, Y. Comparison of HERG channel blocking effects of various beta-blockers-- implication for clinical strategy. Br. J. Pharmacol. 2006, 147, 642–652. [Google Scholar] [CrossRef]
- Li, Z.; Ridder, B.J.; Han, X.; Wu, W.W.; Sheng, J.; Tran, P.N.; Wu, M.; Randolph, A.; Johnstone, R.H.; Mirams, G.R.; et al. Assessment of an In Silico Mechanistic Model for Proarrhythmia Risk Prediction Under the CiPA Initiative. Clin. Pharmacol. Ther. 2018. [Google Scholar] [CrossRef]
- Lu, H.R.; Gallacher, D.J.; Yan, G.X. Assessment of drug-induced proarrhythmia: The importance of study design in the rabbit left ventricular wedge model. J. Pharmacol. Toxicol. Methods 2016, 81, 151–160. [Google Scholar] [CrossRef]
- Liu, T.; Liu, J.; Lu, H.R.; Li, H.; Gallacher, D.J.; Chaudhary, K.; Wang, Y.; Yan, G.X. Utility of Normalized TdP Score System in Drug Proarrhythmic Potential Assessment: A Blinded in vitro Study of CiPA Drugs. Clin. Pharmacol. Ther. 2021, 109, 1606–1617. [Google Scholar] [CrossRef]
- Liu, T.; Brown, B.S.; Wu, Y.; Antzelevitch, C.; Kowey, P.R.; Yan, G.X. Blinded validation of the isolated arterially perfused rabbit ventricular wedge in preclinical assessment of drug-induced proarrhythmias. Heart Rhythm. 2006, 3, 948–956. [Google Scholar] [CrossRef]
- Guo, D.; Lian, J.; Liu, T.; Cox, R.; Margulies, K.B.; Kowey, P.R.; Yan, G.X. Contribution of late sodium current (I(Na-L)) to rate adaptation of ventricular repolarization and reverse use-dependence of QT-prolonging agents. Heart Rhythm. 2011, 8, 762–769. [Google Scholar] [CrossRef]
- Yan, G.X.; Wu, Y.; Liu, T.; Wang, J.; Marinchak, R.A.; Kowey, P.R. Phase 2 early afterdepolarization as a trigger of polymorphic ventricular tachycardia in acquired long-QT syndrome: Direct evidence from intracellular recordings in the intact left ventricular wall. Circulation 2001, 103, 2851–2856. [Google Scholar] [CrossRef]
- De Clerck, F.; Van de Water, A.; D'Aubioul, J.; Lu, H.R.; van Rossem, K.; Hermans, A.; Van Ammel, K. In vivo measurement of QT prolongation, dispersion and arrhythmogenesis: Application to the preclinical cardiovascular safety pharmacology of a new chemical entity. Fundam. Clin. Pharmacol. 2002, 16, 125–140. [Google Scholar] [CrossRef]
- Testai, L.; Breschi, M.C.; Martinotti, E.; Calderone, V. QT prolongation in guinea pigs for preliminary screening of torsadogenicity of drugs and drug-candidates. II. J. Appl. Toxicol. 2007, 27, 270–275. [Google Scholar] [CrossRef]
- Yao, X.; Anderson, D.L.; Ross, S.A.; Lang, D.G.; Desai, B.Z.; Cooper, D.C.; Wheelan, P.; McIntyre, M.S.; Bergquist, M.L.; MacKenzie, K.I.; et al. Predicting QT prolongation in humans during early drug development using hERG inhibition and an anaesthetized guinea-pig model. Br. J. Pharmacol. 2008, 154, 1446–1456. [Google Scholar] [CrossRef]
- Doser, K.; Meyer, B.; Nitsche, V.; Binkert-Graber, P. Bioequivalence evaluation of two different oral formulations of loperamide (Diarex Lactab vs Imodium capsules). Int. J. Clin. Pharmacol. Ther. 1995, 33, 431–436. [Google Scholar]
- Lu, H.R.; Vlaminckx, E.; Van Ammel, K.; De Clerck, F. Drug-induced long QT in isolated rabbit Purkinje fibers: Importance of action potential duration, triangulation and early afterdepolarizations. Eur. J. Pharmacol. 2002, 452, 183–192. [Google Scholar] [CrossRef]
- Kohli, U.; Altujjar, M.; Sharma, R.; Hassan, S. Wide interindividual variability in cardiovascular toxicity of loperamide: A case report and review of literature. Hear. Case Rep. 2019, 5, 221–224. [Google Scholar] [CrossRef]
- Anon. S7B: The Nonclinical Evaluation of the Potential for Delayed Ventricular Repolarization (QT Interval Prolongation) By Human Pharmaceuticals (S7B). Fed. Regist. 2005, 70, 61133–61134. [Google Scholar]
- Stanciu, C.N.; Gnanasegaram, S.A. Loperamide, the "Poor Man's Methadone": Brief Review. J. Psychoact. Drugs 2017, 49, 18–21. [Google Scholar] [CrossRef]
- Bishop-Freeman, S.C.; Feaster, M.S.; Beal, J.; Miller, A.; Hargrove, R.L.; Brower, J.O.; Winecker, R.E. Loperamide-Related Deaths in North Carolina. J. Anal. Toxicol. 2016, 40, 677–686. [Google Scholar] [CrossRef]
- Cay, E.; Yam, J. S2744 Loperamide-Induced Ventricular Fibrillation Cardiac Arrest in the Setting of Recently Diagnosed Ulcerative Colitis. Off. J. Am. Coll. Gastroenterol. 2022, 117, e1803. [Google Scholar] [CrossRef]
- Powell, J.W.; Presnell, S.E. Loperamide as a Potential Drug of Abuse and Misuse: Fatal Overdoses at the Medical University of South Carolina. J. Forensic Sci. 2019, 64, 1726–1730. [Google Scholar] [CrossRef] [PubMed]
- Schinkel, A.H.; Wagenaar, E.; Mol, C.A.; van Deemter, L. P-glycoprotein in the blood-brain barrier of mice influences the brain penetration and pharmacological activity of many drugs. J. Clin. Invest. 1996, 97, 2517–2524. [Google Scholar] [CrossRef] [PubMed]
- Glaeser, H. Importance of P-glycoprotein for drug-drug interactions. Handb. Exp. Pharmacol. 2011, 285–297. [Google Scholar] [CrossRef]
- Konig, J.; Muller, F.; Fromm, M.F. Transporters and drug-drug interactions: Important determinants of drug disposition and effects. Pharmacol. Rev. 2013, 65, 944–966. [Google Scholar] [CrossRef] [PubMed]
- Couture, L.; Nash, J.A.; Turgeon, J. The ATP-binding cassette transporters and their implication in drug disposition: A special look at the heart. Pharmacol. Rev. 2006, 58, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Vaz, R.J.; Kang, J.; Luo, Y.; Rampe, D. Molecular determinants of loperamide and N-desmethyl loperamide binding in the hERG cardiac K(+) channel. Bioorg Med. Chem. Lett. 2018, 28, 446–451. [Google Scholar] [CrossRef]
- Jonker, D.M.; Kenna, L.A.; Leishman, D.; Wallis, R.; Milligan, P.A.; Jonsson, E.N. A pharmacokinetic-pharmacodynamic model for the quantitative prediction of dofetilide clinical QT prolongation from human ether-a-go-go-related gene current inhibition data. Clin. Pharmacol. Ther. 2005, 77, 572–582. [Google Scholar] [CrossRef]
- Gintant, G.A.; Gallacher, D.J.; Pugsley, M.K. The 'overly-sensitive' heart: Sodium channel block and QRS interval prolongation. Br. J. Pharmacol. 2011, 164, 254–259. [Google Scholar] [CrossRef]
- Modi, V.; Krinock, M.; Desai, R.; Stevens, S.; Nanda, S. Loperamide-Induced Cardiac Events: Case Reports and Review. Cureus 2021, 13, e20744. [Google Scholar] [CrossRef]
- Kirsch, G.E.; Trepakova, E.S.; Brimecombe, J.C.; Sidach, S.S.; Erickson, H.D.; Kochan, M.C.; Shyjka, L.M.; Lacerda, A.E.; Brown, A.M. Variability in the measurement of hERG potassium channel inhibition: Effects of temperature and stimulus pattern. J. Pharmacol. Toxicol. Methods 2004, 50, 93–101. [Google Scholar] [CrossRef]
- Wisniowska, B.; Polak, S. hERG in vitro interchange factors--development and verification. Toxicol. Mech. Methods 2009, 19, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Elkins, R.C.; Davies, M.R.; Brough, S.J.; Gavaghan, D.J.; Cui, Y.; Abi-Gerges, N.; Mirams, G.R. Variability in high-throughput ion-channel screening data and consequences for cardiac safety assessment. J. Pharmacol. Toxicol. Methods 2013, 68, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Hanson, L.A.; Bass, A.S.; Gintant, G.; Mittelstadt, S.; Rampe, D.; Thomas, K. ILSI-HESI cardiovascular safety subcommittee initiative: Evaluation of three non-clinical models of QT prolongation. J. Pharmacol. Toxicol. Methods 2006, 54, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Takahara, A.; Izawa, S.; Seki, S.; Aimoto, M.; Nagasawa, Y. Cardiac Electropharmacological Effects of Antidiarrheal Drug Loperamide and Its Antidote Naloxone in Anesthetized Guinea Pigs. Biol. Pharm. Bull. 2022, 45, 542–546. [Google Scholar] [CrossRef]
- Lu, H.R.; Yan, G.X.; Gallacher, D.J. A new biomarker—Index of cardiac electrophysiological balance (iCEB)—Plays an important role in drug-induced cardiac arrhythmias: Beyond QT-prolongation and Torsades de Pointes (TdPs). J. Pharmacol. Toxicol. Methods 2013, 68, 250–259. [Google Scholar] [CrossRef]
- Robyns, T.; Lu, H.R.; Gallacher, D.J.; Garweg, C.; Ector, J.; Willems, R.; Janssens, S.; Nuyens, D. Evaluation of Index of Cardio-Electrophysiological Balance (iCEB) as a New Biomarker for the Identification of Patients at Increased Arrhythmic Risk. Ann. Noninvasive Electrocardiol. 2016, 21, 294–304. [Google Scholar] [CrossRef]
- Afsin, A.; Asoglu, R.; Kobat, M.A.; Asoglu, E.; Suner, A. Evaluation of Index of Cardio-Electrophysiological Balance in Patients With Atrial Fibrillation on Antiarrhythmic-Drug Therapy. Cardiol. Res. 2021, 12, 37–46. [Google Scholar] [CrossRef]
- O'Hara, T.; Virag, L.; Varro, A.; Rudy, Y. Simulation of the undiseased human cardiac ventricular action potential: Model formulation and experimental validation. PLoS Comput. Biol. 2011, 7, e1002061. [Google Scholar] [CrossRef]
- Grandi, E.; Pasqualini, F.S.; Bers, D.M. A novel computational model of the human ventricular action potential and Ca transient. J. Mol. Cell. Cardiol. 2010, 48, 112–121. [Google Scholar] [CrossRef]
- ten Tusscher, K.H.; Noble, D.; Noble, P.J.; Panfilov, A.V. A model for human ventricular tissue. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H1573–H1589. [Google Scholar] [CrossRef]
- Sager, P.T.; Gintant, G.; Turner, J.R.; Pettit, S.; Stockbridge, N. Rechanneling the cardiac proarrhythmia safety paradigm: A meeting report from the Cardiac Safety Research Consortium. Am. Heart J. 2014, 167, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Colatsky, T.; Fermini, B.; Gintant, G.; Pierson, J.B.; Sager, P.; Sekino, Y.; Strauss, D.G.; Stockbridge, N. The Comprehensive in Vitro Proarrhythmia Assay (CiPA) initiative-Update on progress. J. Pharmacol. Toxicol. Methods 2016, 81, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Dutta, S.; Sheng, J.; Tran, P.N.; Wu, W.; Chang, K.; Mdluli, T.; Strauss, D.G.; Colatsky, T. Improving the In Silico Assessment of Proarrhythmia Risk by Combining hERG (Human Ether-a-go-go-Related Gene) Channel-Drug Binding Kinetics and Multichannel Pharmacology. Circ. Arrhythmia Electrophysiol. 2017, 10, e004628. [Google Scholar] [CrossRef] [PubMed]
- Mirams, G.R.; Davies, M.R.; Cui, Y.; Kohl, P.; Noble, D. Application of cardiac electrophysiology simulations to pro-arrhythmic safety testing. Br. J. Pharmacol. 2012, 167, 932–945. [Google Scholar] [CrossRef] [PubMed]
- Beattie, K.A.; Luscombe, C.; Williams, G.; Munoz-Muriedas, J.; Gavaghan, D.J.; Cui, Y.; Mirams, G.R. Evaluation of an in silico cardiac safety assay: Using ion channel screening data to predict QT interval changes in the rabbit ventricular wedge. J. Pharmacol. Toxicol. Methods 2013, 68, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.H.; Lee, S.H.; Chu, D.; Hyun, J.W.; Choe, H.; Choi, B.H.; Jo, S.H. Effects of the histamine H(1) receptor antagonist hydroxyzine on hERG K(+) channels and cardiac action potential duration. Acta Pharmacol. Sin. 2011, 32, 1128–1137. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Action Potential Biomarkers (Parameters) (Lower and Upper Limit) | ||
|---|---|---|
| Parameter | Lower limit | Upper limit |
| Peak Voltage (mV) | 10 | 55 |
| RMP (mV) | −95 | −80 |
| APD 90 (ms) | 180 | 440 |
| APD 50 (ms) | 110 | 350 |
| APD 40 (ms) | 85 | 320 |
| Tri 90–40 (ms) | 50 | 150 |
| Hydroxyzine | ||
| Ion-channel inhibited | IC50 (µM) | Hill coefficient. |
| hERG (IKr) | 0.39 | 1 |
| Nav1.5 (INa) | 13.3 | 1 |
| Cav1.2 (ICa) | 8.6 | 1 |
| Loperamide | ||
| Ion-channel | IC50 (µM) | Hill coefficient |
| hERG (IKr) | 0.3897 | 1.21 |
| Nav1.5 (INa) | 0.526 | 1.11 |
| Cav1.2 (ICa) | 4.084 | 1.64 |
| Free Therapeutic Plasma Concentration (FTPC) | ||
| Loperamide | 0.25 nM | |
| Hydroxyzine | 0.013 µM | |
| Test System | Parameter | Tested Dose | Margin |
|---|---|---|---|
| X FTPC | |||
| IKr (hERG) | IC50 | 390 nM | 1560 |
| INa | IC50 | 526 nM | 2104 |
| ICa | IC50 | 4091 nM | 16,364 |
| In Silico Modelling | NE on APs | 150 nM | 600 |
| Significant effects on APs | 200 nM | 800 | |
| Rabbit ventricular wedge | NE | 100 nM | 400 |
| ↑ QRS | 300 nM | 1200 | |
| ↓ iCEB | 1000 nM | 4000 | |
| Cardiac arrhythmias | 3000 nM | 12,000 | |
| Anesthetized guinea pig | NE | 1.25 mg/kg i.v. (FPC = 36 ng/mL) | 304 |
| ↑iCEB, QRS | 2.5 mg/kg i.v. (FPC = 105 ng/mL) | 879 | |
| ↑ QTcB, Incidence of AV Block (type II/III). | 2.5 mg/kg i.v. (FPC = 105 ng/mL) | 879 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, H.R.; Damiano, B.P.; Kreir, M.; Rohrbacher, J.; van der Linde, H.; Saidov, T.; Teisman, A.; Gallacher, D.J. The Potential Mechanisms behind Loperamide-Induced Cardiac Arrhythmias Associated with Human Abuse and Extreme Overdose. Biomolecules 2023, 13, 1355. https://doi.org/10.3390/biom13091355
Lu HR, Damiano BP, Kreir M, Rohrbacher J, van der Linde H, Saidov T, Teisman A, Gallacher DJ. The Potential Mechanisms behind Loperamide-Induced Cardiac Arrhythmias Associated with Human Abuse and Extreme Overdose. Biomolecules. 2023; 13(9):1355. https://doi.org/10.3390/biom13091355
Chicago/Turabian StyleLu, Hua Rong, Bruce P. Damiano, Mohamed Kreir, Jutta Rohrbacher, Henk van der Linde, Tamerlan Saidov, Ard Teisman, and David J. Gallacher. 2023. "The Potential Mechanisms behind Loperamide-Induced Cardiac Arrhythmias Associated with Human Abuse and Extreme Overdose" Biomolecules 13, no. 9: 1355. https://doi.org/10.3390/biom13091355
APA StyleLu, H. R., Damiano, B. P., Kreir, M., Rohrbacher, J., van der Linde, H., Saidov, T., Teisman, A., & Gallacher, D. J. (2023). The Potential Mechanisms behind Loperamide-Induced Cardiac Arrhythmias Associated with Human Abuse and Extreme Overdose. Biomolecules, 13(9), 1355. https://doi.org/10.3390/biom13091355