
Historical Cohort Study of Congenital Isolated Hypoganglionosis of the Intestine: Determining the Best Surgical Interventions
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Histological Analysis
2.4. Measurement of the Intestinal Length, Intestinal Ratio, Stoma Output, and PN Depnedency
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics (Table 1)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Current Age | Birth History (Weight at Birth: g) | Day of Initial Surgery and the Procedure | Stoma Site at the Initial Surgery, Length (cm) from the LT and * a Percentage of the Total Estimated Small Intestinal Length | Hu C/D Count Jejunum /cm | Hu C/D Count Ileum /cm | Hu C/D Count Colon /cm | |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 29 | Term 39 (3484) | Day 2, Ileostomy | 160 cm (89.8%) | 12 | 5 | 15 |
| 2 | M | 25 | Term 37 (3012) | Day 3, Ileostomy | NA | 10 | NA | 4 |
| 3 | M | 25 | Term 39 (3452) | 2 months, Jejunostomy | 60 cm (33.8%) | 3 | 11 | 11 |
| 4 | F | 20 | Term 39 (2788) | 1 month, Ileostomy | 30 cm from TI (81.1%) | NA | 3 | 9 |
| 5 | F | 18 | Term 37 (2368) | Day 2, Jejunostomy | 70 cm (47.9%) | NA | 9 | 7 |
| 6 | M | 17 | Term 40 (3480) | Day 2, Jejunostomy | 75 cm (42.1%) | 1.6 | NA | NA |
| 7 | F | 14 | Term 41 (2966) | Day 1, Ileostomy | NA | NA | 6.4 | NA |
| 8 | F | 12 | Term 37 (2832) | 1 month, Ileostomy | 45 cm from TI (71.9%) | NA | 10 | 7 |
| 9 | M | 12 | Preterm 35 (1828) | Day 16, Gastrostomy | 0 cm (0%) | 14 | 3 | 9 |
| 10 | F | 12 | Term 40 (3408) | Day 2, Ileostomy | 40 cm from TI (77.3%) | NA | 4 | NA |
| 11 | M | 11 | Term 40 (3380) | Day 0, Ileostomy | 5 cm from TI (97.1%) | NA | 9 | NA |
| 12 | F | 10 | Term 38 (3084) | Day 1, Jejunostomy | 30 cm (17.9%) | 10 | 5 | NA |
| 13 | F | 9 | Term 37 (2625) | Day 3, Ileostomy | 115 cm (74.6%) | 7 | 15 | NA |
| 14 | F | 7 | Term 39 (3456) | Day 1, Jejunostomy | 70 cm (39.5%) | 3 | 3 | NA |
| 15 | M | 7 | Term 37 (2917) | Day 20, Jejunostomy (Full thickness biopsy at day 2) | 45 cm (27.7%) | 13 | NA | NA |
| 16 | F | 5 | Term 38 (3340) | Day 0, Jejunostomy | 70 cm (40.2%) | 10 | 0 | 5 |
| 17 | F | 3 | Term 39 (3240) | Day 30, Jejunostomy (Full thickness biopsy at day 3) | 50 cm (29.1%) | 14.5 | 11.7 | 11.2 |
| 18 | F | 3 | Term 40 (3334) | Day 8, Jejunostomy (Full thickness biopsy at day 2) | 40 cm (23%) | NA | 10 | NA |
| 19 | F | 2 | Term 38 (2836) | Day 19, Jejunostomy | 40 cm (25%) | 23 | 3 | 22 |
3.2. Initial Diverting Enterostomy
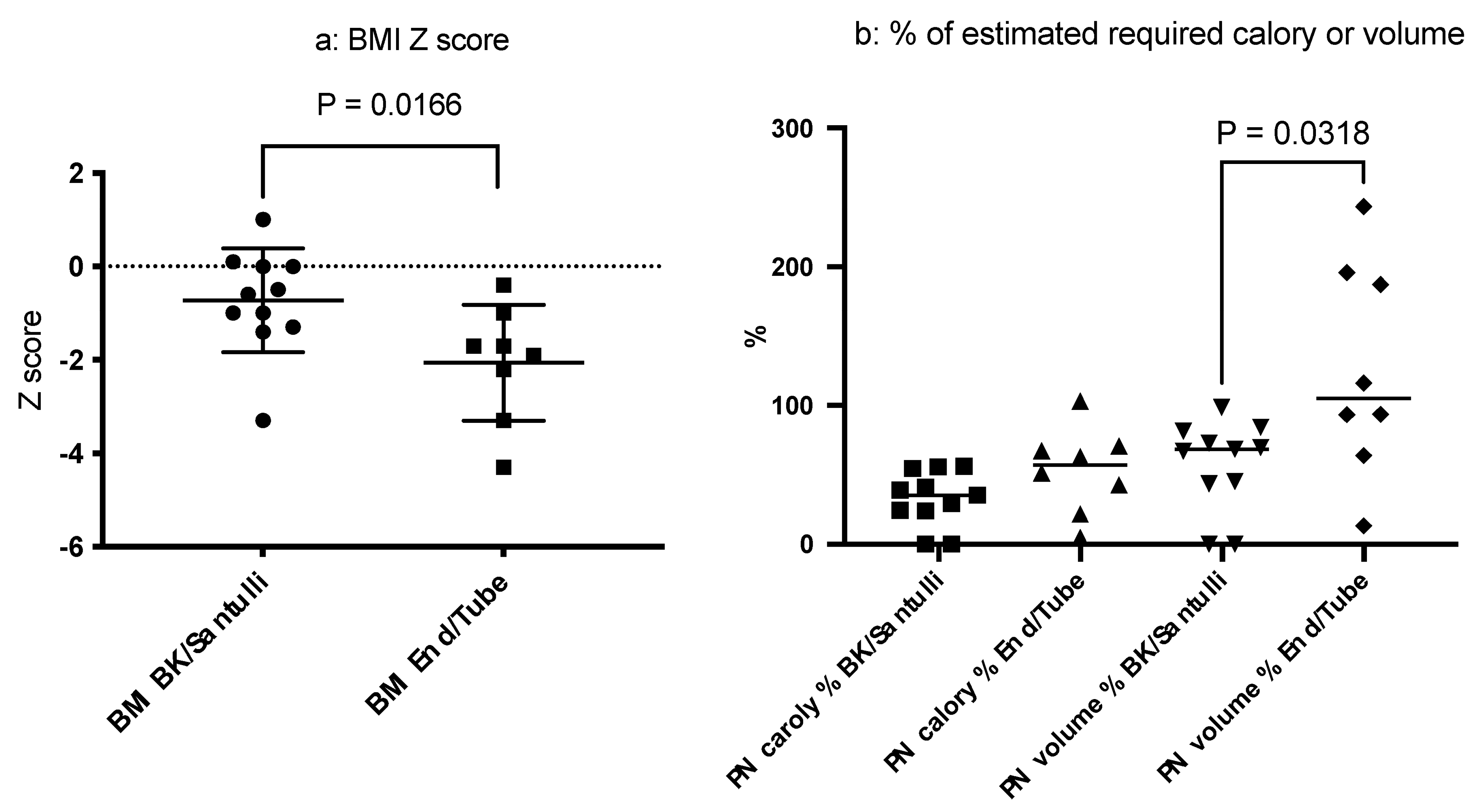
3.3. Type of Stoma, Residual Intestinal Length, and Distal Colon (Table 2 and Figure 2)

| IR = Small Intestine (cm)/Height (cm), Measured at the Latest Surgery | Stoma Type | Distal Colon | Stoma Output mL/kg/day | PN Dependency % of the Total Estimated Calories | PN Dependency % of the Total Estimated Volume | Height Z Score | BW Z Score | BW /Height | BMI Z Score | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 76/147.4 = 0.51 (14 years old) *Measured at iTx | Tube enterostoma | T/C | 75 *before iTx | 103.2 | 243.4 | −2.5 | −1.3 | 0.27 | −0.4 |
| 2 | 102/156 = 0.65 (15 years old) *Measured at iTx | End stoma | T/C | 30.6 *before iTx | 51.3 | 116.1 | −1.8 | −2.4 | 0.21 | −4.3 |
| 3 | 107/103 = 1.03 (11 years old) *Measured at iTx | End stoma | T/C | 25.5 *before iTx | 42.8 | 93.3 | −6.0 | −2.6 | 0.15 | −1.7 |
| 4 | 120/148 = 0.81 (12 years old) | Santulli | S/C | 28.8 | 24 | 45.2 | −0.9 | 0.4 | 0.37 | 1.0 |
| 5 | 160/126 = 1.27 (9 years old) | Santulli | S/C | 28.8 | 35.2 | 98.6 | −0.8 | −0.9 | 0.3 | −0.6 |
| 6 | 75/128.5 = 0.58 (10 years old) *Measured at iTx | Tube enterostoma | Rectum | 107.2 *before iTx | 70.8 | 195.9 | −1.1 | −1.6 | 0.16 | −3.3 |
| 7 | 90/135.9 = 0.66 (12 years old) | BK | T/C | 46.4 | 29.4 | 81.4 | 0.1 | −0.4 | 0.25 | −0.5 |
| 8 | 115/92.5 = 1.24 (4 years old) | End stoma | T/C | 31.2 | 67.4 | 63.8 | −2.0 | −1.4 | 0.23 | −1.0 |
| 9 | 63/65.5 = 0.96 (1.5 years old) | Santulli | S/C | 44.3 | 56.2 | 68.5 | −4.3 | −2.6 | 0.16 | −3.3 |
| 10 | 160/96.8 = 1.65 (4 years old) | End stoma | Total colon | 38.7 | 4.8 | 13.3 | −3.3 | −2.1 | 0.2 | −1.9 |
| 11 | 75/125 = 0.6 (8 years old) | End stoma | T/C | 52 | 21.8 | 93.7 | −0.1 | −1.1 | 0.18 | −2.2 |
| 12 | 100/93 = 1.075 (3 years old) | BK | T/C | 32.9 | 0 | 0 | −1.3 | −0.8 | 0.17 | −0.0 |
| 13 | 90/104.8 = 0.86 (8 years old) | End stoma | S/C | 124.8 | 63.2 | 187.2 | −3.9 | −2.2 | 0.15 | −1.7 |
| 14 | 100/88.3 = 1.13 (3 years old) | BK | T/C | 26.9 | 54.6 | 67 | −3.0 | −2.3 | 0.13 | −2.1 |
| 15 | 55/67 = 0.82 (2 years old) | BK | T/C | 51.1 | 0 | 0 | −2.1 | −1.1 | 0.18 | 0.1 |
| 16 | 65/85 = 0.76 (3 years old) | BK | Ileum + total colon | 78.4 | 55.8 | 84.4 | −1.6 | −1.6 | 0.14 | −1.4 |
| 17 | 75/88 = 0.85 (3 years old) | BK | T/C | 46.5 | 24.4 | 43.7 | −0.6 | −0.4 | 0.14 | 0.0 |
| 18 | 50/66 = 0.75 (10 months old) | BK | T/C | 57.9 | 39 | 69.6 | −3.5 | −2.7 | 0.12 | −1.0 |
| 19 | 40/78.9 = 0.51 (2 years old) | BK | T/C | 93 | 40.9 | 73 | −1.8 | −2.0 | 0.12 | −1.3 |
3.4. Associations among the Intestinal Length, Stoma Revision, PN Dependency, and Growth Parameters
3.5. iTx
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Borchard, F.; Meier-Ruge, W.; Wiebecke, B.; Briner, J.; Müntefering, H.; Födisch, H.F.; Holschneider, A.M.; Schmidt, A.; Enck, P.; Stolte, M. Disorders of the innervation of the large intestine--classification and diagnosis. Results of a consensus conference of the Society of Gastroenteropathology 1 December 1990 in Frankfurt/Main. Pathologe 1991, 12, 171–174. [Google Scholar] [PubMed]
- Holschneider, A.M.; Meier-Ruge, W.; Ure, B.M. Hirschsprung’s disease and allied disorders--a review. Eur. J. Pediatr. Surg. 1994, 4, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Dingemann, J.; Puri, P. Isolated hypoganglionosis: Systematic review of a rare intestinal innervation defect. Pediatr. Surg. Int. 2010, 26, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Martucciello, G.; Pini Prato, A.; Puri, P.; Holschneider, A.M.; Meier-Ruge, W.; Jasonni, V.; Grosfeld, J.L. Controversies concerning diagnostic guidelines for anomalies of the enteric nervous system: A report from the fourth International Symposium on Hirschsprung’s disease and related neurocristopathies. J. Pediatr. Surg. 2005, 40, 1527–1531. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, C.D.; Hyman, P.E.; Altschuler, S.M.; Christensen, J.; Colletti, R.B.; Cucchiara, S.; Carlo, D.L.; Alex, F.; Hillemeier, A.; McCallum, R.; et al. Diagnosis and treatment of chronic intestinal pseudo-obstruction in children: Report of consensus workshop. J. Pediatr. Gastroenterol. Nutr. 1997, 24, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Thapar, N.; Saliakellis, E.; Benninga, M.A.; Borrelli, O.; Curry, J.; Faure, C.; De Giorgio, R.; Gupte, G.; Knowles, C.H.; Staiano, A.; et al. Paediatric Intestinal Pseudo-obstruction: Evidence and Consensus-based Recommendations From an ESPGHAN-Led Expert Group. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 991–1019. [Google Scholar] [CrossRef] [PubMed]
- Meier-Ruge, W.A.; Brunner, L.A.; Engert, J.; Heminghaus, M.; Holschneider, A.M.; Jordan, P.; Piket, G.; Posselt, H.G.; Schärli, A. A correlative morphometric and clinical investigation of hypoganglionosis of the colon in children. Eur. J Pediatr. Surg. 1999, 9, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Puri, P. Variant Hirschsprung’s disease. J. Pediatr. Surg. 1997, 32, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Puri, P.; Gosemann, J.H. Variants of Hirschsprung disease. Semin. Pediatr. Surg. 2012, 21, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, T.; Masumoto, K.; Ieiri, S.; Nakatsuji, T.; Akiyoshi, J. New classification of hypoganglionosis: Congenital and acquired hypoganglionosis. J. Pediatr. Surg. 2006, 41, 2046–2051. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, T.; Ieiri, S.; Miyoshi, K.; Kohashi, K.; Oda, Y.; Kubota, A.; Watanabe, Y.; Matsufuji, H.; Fukuzawa, M.; Tomomasa, T. The incidence and outcome of allied disorders of Hirschsprung’s disease in Japan: Results from a nationwide survey. Asian J. Surg. 2017, 40, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Kanamori, Y.; Uchida, K.; Taguchi, T. Isolated hypoganglionosis: Results of a nationwide survey in Japan. Pediatr. Surg. Int. 2013, 29, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Sumida, W.; Takasu, H.; Oshima, K.; Kanamori, Y.; Uchida, K.; Taguchi, T. Early jejunostomy creation in cases of isolated hypoganglionosis: Verification of our own experience based on a national survey. Surg. Today 2015, 45, 1509–1512. [Google Scholar] [CrossRef] [PubMed]
- Yoshimaru, K.; Taguchi, T.; Obata, S.; Takemoto, J.; Takahashi, Y.; Iwanaka, T.; Yanagi, Y.; Kuda, M.; Miyoshi, K.; Matsuura, T.; et al. Immunostaining for Hu C/D and CD56 is useful for a definitive histopathological diagnosis of congenital and acquired isolated hypoganglionosis. Virchows Arch. 2017, 470, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, M.; Kapur, R.P. Counting myenteric ganglion cells in histologic sections: An empirical approach. Hum. Pathol. 2010, 41, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Kapur, R.P.; Bellizzi, A.M.; Bond, S.; Chen, H.; Han, J.S.; LeGallo, R.D.; Midgen, C.; Poulin, A.A.; Uddin, N.; Warren, M.; et al. Congenital Myenteric Hypoganglionosis. Am. J. Surg. Pathol. 2021, 45, 1047–1060. [Google Scholar] [CrossRef] [PubMed]
- Struijs, M.C.; Diamond, I.R.; de Silva, N.; Wales, P.W. Establishing norms for intestinal length in children. J. Pediatr. Surg. 2009, 44, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Muto, M.; Matsufuji, H.; Taguchi, T.; Tomomasa, T.; Nio, M.; Tamai, H.; Tamura, M.; Sago, H.; Toki, A.; Nosaka, S.; et al. Japanese clinical practice guidelines for allied disorders of Hirschsprung’s disease, 2017. Pediatr. Int. 2018, 60, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Graham, K.D.; López, S.H.; Sengupta, R.; Shenoy, A.; Schneider, S.; Wright, C.M.; Feldman, M.; Furth, E.; Valdivieso, F.; Lemke, A.; et al. Robust, 3-Dimensional Visualization of Human Colon Enteric Nervous System Without Tissue Sectioning. Gastroenterology 2020, 158, 2221–2235.e5. [Google Scholar] [CrossRef]


| a | Stoma Revision (Santulli or BK), n = 11 (Median) | End-Stoma or Tube-Stoma Only, n = 8 (Median) | p Value |
|---|---|---|---|
| Age | 2–20 (7) | 9–14 (11.5) | 0.2791 |
| Age at intervention | 0.8–12 (3) | 0.5–8 (4) | 0.7037 |
| Sex | Male: 2 Female: 9 | Male: 5 Female: 3 | 0.0739 |
| Intestinal ratio (IR) | 0.51–1.27 (0.82) | 0.51–1.65 (0.755) | 0.7345 |
| b | Stoma Revision (Santulli or BK), n = 11, (Median) | End Stoma or Tube Stoma Only, n = 8 (Median) | p Value |
| Stoma output mL/kg | 28.8–93 (46.4) | 25.5–124.8 (45.35) | 0.7002 |
| Height Z score | −4.3–0.1 (−1.6) | −5.8–−0.7 (−2.25) | 0.2816 |
| BW Z score | −3.5–0.4 (−1.1) | −2.6–−1.3 (−2.2) | 0.1704 |
| BMI Z score | −3.3–1.0 (−0.6) | −4.3–−0.4 (−1.8) | 0.0166 |
| PN calories | 0–56.2 (35.2) | 4.8–103.2 (57.2) | 0.1051 |
| PN volume | 0–98.6 (68.5) | 13.3–243.4 (104.9) | 0.0318 |
| Pt No | Sex | Age at iTx (Years) | Length of the Native Intestine Proximal to the Graft (cm) | Graft Length (cm) | Native Intestine Distal to the Graft | Status of Stoma | PN Dependency | Time since iTx (Years) | BMI Pre-iTx (Z Score) | BMI Post-iTx (Z Score) | Height Pre-iTx (Z Score) | Height Post-iTx (Z Score) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 14 | 30 | 150 | S/C | Reversed 3 years after iTx | Off for 13 years | 15 | −0.04 | 0.94 | −3.55 | −1.92 |
| 2 | M | 11 | 5 | 110 | S/C | Reversed 11 years after iTx | Off for 3 years | 14 | −1.74 | −1.46 | −5.97 | −4.2 |
| 3 | M | 15 | 26 | 150 | NA | End stoma | Back to PN | Graftectomy 2 years after iTx due to chronic rejection | −4.28 | NA | −2.19 | NA |
| 6 | M | 10 | 15 | 150 | Ileum (30 cm) + Rectum | Reversed 2 years after iTx | Off for 5 years | 7 | −3.34 | −2.57 | −1.39 | −0.86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamada, Y.; Mori, T.; Takahashi, N.; Fujimura, T.; Kano, M.; Kato, M.; Takahashi, M.; Shimojima, N.; Watanabe, T.; Yoshioka, T.; et al. Historical Cohort Study of Congenital Isolated Hypoganglionosis of the Intestine: Determining the Best Surgical Interventions. Biomolecules 2023, 13, 1560. https://doi.org/10.3390/biom13101560
Yamada Y, Mori T, Takahashi N, Fujimura T, Kano M, Kato M, Takahashi M, Shimojima N, Watanabe T, Yoshioka T, et al. Historical Cohort Study of Congenital Isolated Hypoganglionosis of the Intestine: Determining the Best Surgical Interventions. Biomolecules. 2023; 13(10):1560. https://doi.org/10.3390/biom13101560
Chicago/Turabian StyleYamada, Yohei, Teizaburo Mori, Nobuhiro Takahashi, Takumi Fujimura, Motohiro Kano, Mototoshi Kato, Masataka Takahashi, Naoki Shimojima, Toshihiko Watanabe, Takako Yoshioka, and et al. 2023. "Historical Cohort Study of Congenital Isolated Hypoganglionosis of the Intestine: Determining the Best Surgical Interventions" Biomolecules 13, no. 10: 1560. https://doi.org/10.3390/biom13101560
APA StyleYamada, Y., Mori, T., Takahashi, N., Fujimura, T., Kano, M., Kato, M., Takahashi, M., Shimojima, N., Watanabe, T., Yoshioka, T., Kanamori, Y., Kuroda, T., & Fujino, A. (2023). Historical Cohort Study of Congenital Isolated Hypoganglionosis of the Intestine: Determining the Best Surgical Interventions. Biomolecules, 13(10), 1560. https://doi.org/10.3390/biom13101560