Over-Expression of Allograft Inflammatory Factor-1 (AIF-1) in Patients with Rheumatoid Arthritis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Quantitative Real-Time Polymerase Chain Reaction
2.3. Real-Time PCR Reaction
2.4. Stimulation of Peripheral Blood Mononuclear Cells (PBMCs)
2.5. Flow Cytometry
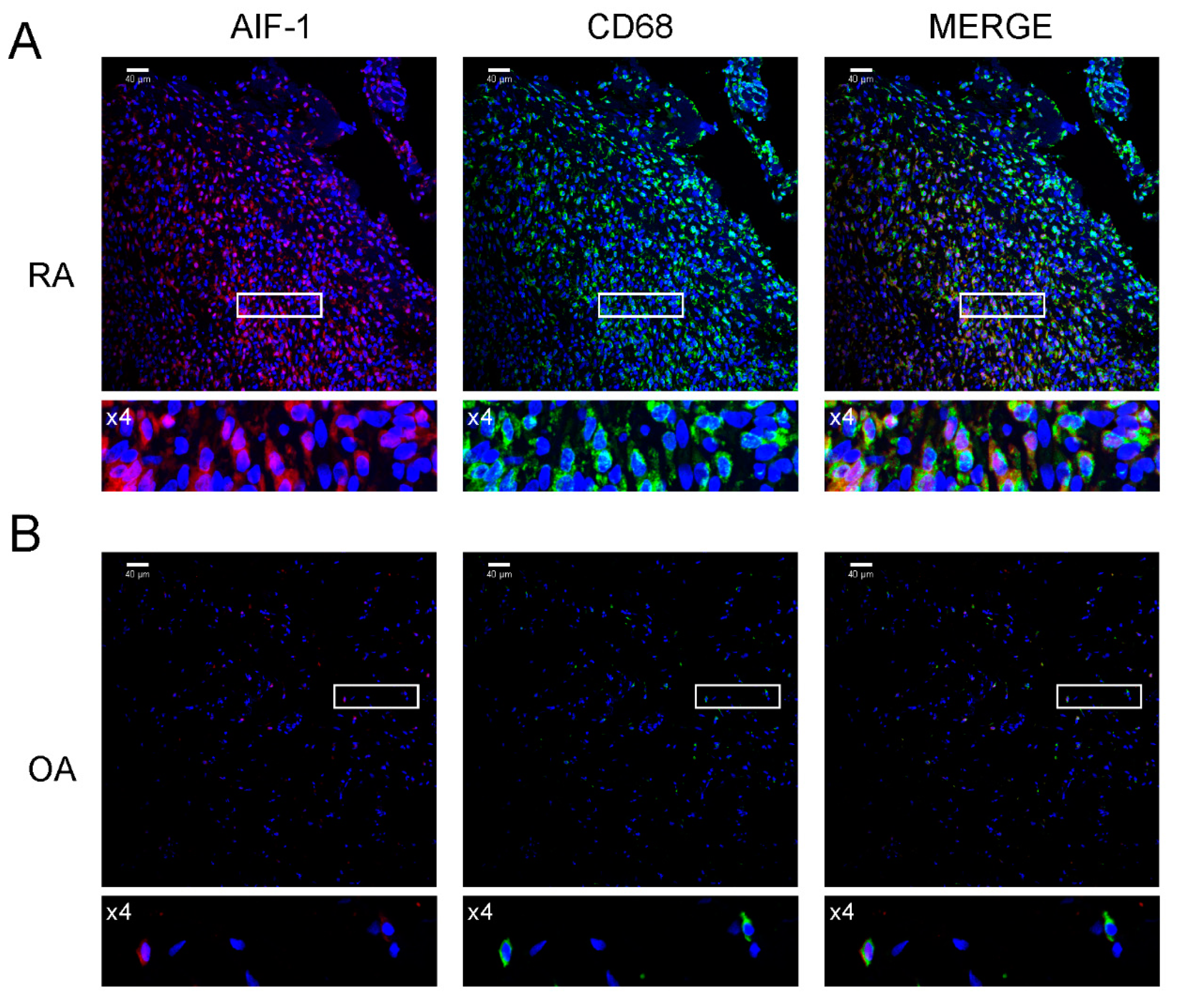
2.6. Immunofluorescence Analysis of Synovial Samples
2.7. Statistical Analysis
3. Results
3.1. Expression of AIF-1 Isoforms in PBMCs and SMs in Patients with RA and OA
3.2. Correlations of AIF-1 Variant mRNA Expression
3.3. Correlation of AIF-1 Variant mRNA Expression Between PBMCs and SMs in Patient Groups
3.4. Percentage of AIF-1 Positive Cells in Blood and SMs of Patients with RA and OA
3.5. The Effect of IL-6, IL-21, and IL-34 Stimulation of PBMCs on the Percentage of AIF-1-Positive Cells
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Scott, D.; Wolfe, F.; Huizinga, T.W. Rheumatoid arthritis. Lancet 2010, 376, 1094–1108. [Google Scholar] [CrossRef]
- Buckwalter, J.A.; Martin, J.A. Osteoarthritis. Add. Drug Del. Rev. 2006, 58, 150–176. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.D.; Triantafillou, S.; Parker, A.; Youssef, P.P.; Coleman, M. Synovial membrane inflammation and cytokine production in patients with early osteoarthritis. J. Reumatol. 1997, 24, 365–371. [Google Scholar]
- Utans, U.; Arceci, R.J.; Yamashita, Y.; Russell, M.E. Cloning and characterization of allograft inflammatory factor-1: A novel macrophage factor identified in rat cardiac allografts with chronic rejection. J. Clin. Investig. 1995, 95, 2954–2962. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Kelemen, S.E.; Autieri, M.V. Inhibition of AIF-1 expression by constitutive siRNA expression reduces macrophage migration, proliferation, and signal transduction initiated by atherogenic stimuli. Am. J. Physiol.-Cell Physiol. 2006, 290, 1083–1091. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yang, Z.F.; Ho, D.W.; Lau, C.K.; Lam, C.T.; Lum, C.T.; Poon, R.T.; Fan, S.T. Allograft inflammatory factor-1 (AIF-1) is crucial for the survival and pro-inflammatory activity of macrophages. Int. Immunol. 2005, 17, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Kelemen, S.E.; Autieri, M.V. Expression of allograft inflammatory factor-1 in T lymphocytes: A role in T-lymphocyte activation and proliferative arteriopathies. Am. J. Pathol. 2005, 167, 619–626. [Google Scholar] [CrossRef]
- Otieno, F.G.; Lopez, A.M.; Jimenez, S.A.; Gentiletti, J.; Artlett, C.M. Allograft inflammatory factor-1 and tumor necrosis factor single nucleotide polymorphisms in systemic sclerosis. Tissue Antigens 2007, 69, 583–591. [Google Scholar] [CrossRef]
- Mishima, T.; Iwabuchi, K.; Fujii, S.; Tanaka, S.Y.; Ogura, H.; Watano-Miyata, K.; Ishimori, N.; Andoh, Y.; Nakai, Y.; Iwabuchi, C.; et al. Allograft inflammatory factor-1 augments macrophage phagocytotic activity and accelerates the progression of atherosclerosis in ApoE-/- mice. Int. J. Mol. Med. 2008, 21, 181–187. [Google Scholar] [CrossRef][Green Version]
- Broglio, L.; Erne, B.; Tolnay, M.; Schaeren-Wiemers, N.; Fuhr, P.; Steck, A.J.; Renaud, S. Allograft inflammatory factor-1: A pathogenetic factor for vasculitic neuropathy. Muscle Nerve 2008, 38, 1272–1279. [Google Scholar] [CrossRef]
- Yamamoto, A.; Ashihara, E.; Nakagawa, Y.; Obayashi, H.; Ohta, M.; Hara, H.; Adachi, T.; Seno, T.; Kadoya, M.; Hamaguchi, M.; et al. Allograft inflammatory factor-1 is overexpressed and induces fibroblast chemotaxis in the skin of sclerodermatous GVHD in a murine model. Immunol. Lett. 2011, 135, 144–150. [Google Scholar] [CrossRef]
- Kadoya, M.; Yamamoto, A.; Hamaguchi, M.; Obayashi, H.; Mizushima, K.; Ohta, M.; Seno, T.; Oda, R.; Fujiwara, H.; Kohno, M.; et al. Allograft inflammatory factor-1 stimulates chemokine production and induces chemotaxis in human peripheral blood mononuclear cells. Biochem. Biophys. Res. Commun. 2014, 448, 287–291. [Google Scholar] [CrossRef]
- Liu, S.; Tan, W.Y.; Chen, Q.R.; Chen, X.P.; Fu, K.; Zhao, Y.Y.; Chen, Z.W. Daintain/AIF-1 promotes breast cancer proliferation via activation of the NF- kappaB/cyclin D1 pathway and facilitates tumor growth. Cancer Sci. 2008, 99, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Slim, F.A.; Ouellette, G.; Ennour-Idrissi, K.; Jacob, S.; Diorio, C.; Durocher, F. An isoform of AIF1 involved in breast cancer. Cancer Cell Int. 2018, 18, 167. [Google Scholar] [CrossRef]
- Kimura, M.; Kawahito, Y.; Obayashi, H.; Ohta, M.; Hara, H.; Adachi, T.; Tokunaga, D.; Hojo, T.; Hamaguchi, M.; Omoto, A.; et al. A critical role for allograft inflammatory factor-1 in the pathogenesis of rheumatoid arthritis. J. Immunol. 2007, 178, 3316–3322. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, A.; Kurzawski, M.; Szczepanik, T.; Dziedziejko, V.; Safranow, K.; Borowiec-Chłopek, Z.; Giedrys-Kalemba, S.; Drozdzik, M. Association of allograft inflammatory factor-1 gene polymorphism with rheumatoid arthritis. Tissue Antigens 2008, 72, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, A.; Kotrych, D.; Paczkowska, E.; Roginska, D.; Dziedziejko, V.; Safranow, K.; Machalinski, B. Expression of allograft inflammatory factor-1 in peripheral blood monocytes and synovial membranes in patients with rheumatoid arthritis. Hum. Immunol. 2016, 77, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Mei, C.; Du, R.; Shen, L. Protective effect of allograft inflammatory factor-1 on the apoptosis of fibroblast-like synoviocytes in patients with rheumatic arthritis induced by nitrooxide donor sodium nitroprusside. Scand. J. Rheumatol. 2013, 42, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Deininger, M.H.; Meyermann, R.; Schluesener, H.J. The allograft inflammatory factor-1 family of proteins. FEBS Lett. 2002, 514, 115–121. [Google Scholar] [CrossRef]
- Home—Gene—NCBI—NIH. Available online: https://www.ncbi.nlm.nih.gov./gene/ (accessed on 20 November 2019).
- Del Galdo, F.; Maul, G.G.; Jime´nez, S.A.; Carol, M.; Artlett, C.M. Expression of Allograft Inflammatory Factor 1 in Tissues from Patients With Systemic Sclerosis and In Vitro Differential Expression of Its Isoforms in Response to Transforming Growth Factor. Arthritis Rheum. 2006, 54, 2616–2625. [Google Scholar] [CrossRef]
- Harney, S.M.; Vilariño-Güell, C.; Adamopoulos, I.E.; Sims, A.M.; Lawrence, R.W.; Cardon, L.R.; Newton, J.L.; Meisel, C.; Pointon, J.J.; Darke, C.; et al. Fine mapping of the MHC Class III region demonstrates association of AIF1 and rheumatoid arthritis. Rheumatology 2008, 47, 1761–1767. [Google Scholar] [CrossRef] [PubMed][Green Version]
- UniProtKB—P55008 (AIF1_HUMAN). Available online: https://www.uniprot.org/uniprot/P55008# (accessed on 20 November 2019).
- McDaniel, D.O.; Piazza, L.K.; Barker, A.; Robertson, H.; Moore, C.K.; Zhou, X. AIF-1 Gene Expression and Polymorphism in Association with Cardiac Allograft Rejection. J. Clin. Exp. Cardiolog. 2012, S11. [Google Scholar] [CrossRef]
- Chinnasamy, P.; Lutz, S.E.; Riascos-Bernal, D.F.; Jeganathan, V.; Casimiro, I.; Brosnan, C.F.; Sibinga, N.E.S. Loss of Allograft Inflammatory Factor-1 Ameliorates Experimental Autoimmune Encephalomyelitis by Limiting Encephalitogenic CD4 T-Cell expansion. Mol. Med. 2015, 21, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Nomoto, S.; Kato, Y.; Montgomery, R.A.; Williams, G.M.; Klein, A.S.; Sun, Z. Over-expression of AIF- in liver allografts and peripheral blood correlates with acute rejection after transplantation in rats. Am. J. Transplant. 2004, 12, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Barker, A.K.; McDaniel, D.O.; Zhou, X.; He, Z.; Aru, G.; Thomas, T.; Moore, C.K. Combined analysis of allograft inflammatory factor-1, interleukin-18, and Toll-like receptor expression and association with allograft rejection and coronary vasculopathy. Am. Surg. 2010, 76, 872–878. [Google Scholar] [CrossRef]
- McDaniel, D.O.; Rigney, D.A.; McDaniel, K.Y.; Windham, W.J.; Redmond, P.; Williams, B.; Zhoub, X.; Hawxby, A.; Butt, F. Early expression profile of inflammatory markers and kidney allograft status. Transplant. Proc. 2013, 45, 1520–1523. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | OA | RA | OA vs. RA | |||||
|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | Median (Q1–Q3) | n | Mean ± SD | Median (Q1–Q3) | p& | ||
| PBMC | AIF1v1 | 12 | 4.23 ± 1.33 | 4.21 (3.38–4.81) | 15 | 4.33 ± 1.30 | 4.06 (3.49–4.59) | 1.00 |
| AIF1v4 | 12 | 2.60 ± 0.87 | 2.36 (2.12–3.42) | 15 | 3.14 ± 1.10 | 2.80 (2.37–3.72) | 0.20 | |
| AIF1v3 | 12 | 3.72 ± 1.28 | 3.60 (2.82–4.87) | 15 | 4.36 ± 1.22 | 3.88 (3.51–5.67) | 0.16 | |
| SM | AIF1v1 | 12 | 1.00 ± 0.37 | 1.02 (0.73–1.32) | 8 | 0.95 ± 0.31 | 0.90 (0.73–1.20) | 0.76 |
| AIF1v4 | 12 | 1.00 ± 0.36 | 1.16 (0.69–1.26) | 8 | 0.93 ± 0.26 | 0.82 (0.74–1.14) | 0.70 | |
| AIF1v3 | 12 | 1.00 ± 0.36 | 1.04 (0.72–1.27) | 8 | 1.09 ± 0.35 | 0.99 (0.83–1.36) | 0.82 | |
| Parameters | OA | RA | OA vs. RA | |||||
|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | Median (Q1–Q3) | n | Mean ± SD | Median (Q1–Q3) | p& | ||
| SM/PBMC | AIF1v1 | 12 | 0.27 ± 0.15 | 0.21 (0.16–0.36) | 8 | 0.22 ± 0.08 | 0.22 (0.17–0.27) | 0.76 |
| AIF1v4 | 12 | 0.44 ± 0.26 | 0.38 (0.28–0.56) | 8 | 0.31 ± 0.10 | 0.33 (0.24–0.39) | 0.25 | |
| AIF1v3 | 12 | 0.32 ± 0.23 | 0.28 (0.19–0.36) | 8 | 0.27 ± 0.09 | 0.27 (0.23–0.31) | 0.94 | |
| Parameters | OA | RA | |||||||
|---|---|---|---|---|---|---|---|---|---|
| AIF1v4 | AIF1v3 | AIF1v4 | AIF1v3 | ||||||
| Rs | p | Rs | p | Rs | p | Rs | p | ||
| PBMC | AIF1v1 | 0.82 | 0.0011 | 0.86 | 0.00033 | 0.91 | 0.000003 | 0.66 | 0.0078 |
| AIF1v4 | - | - | 0.94 | 0.000007 | - | - | 0.73 | 0.0021 | |
| SM | AIF1v1 | 0.76 | 0.0045 | 0.78 | 0.0030 | 0.95 | 0.00026 | 0.88 | 0.0039 |
| AIF1v4 | - | - | 0.83 | 0.0010 | - | - | 0.95 | 0.00026 | |
| Parameters | OA | RA | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PBMC | PBMC | ||||||||||||
| AIF1v1 | AIF1v4 | AIF1v3 | AIF1v1 | AIF1v4 | AIF1v3 | ||||||||
| Rs | p | Rs | p | Rs | p | Rs | p | Rs | p | Rs | p | ||
| SM | AIF1v1 | −0.05 | 0.88 | −0.23 | 0.47 | −0.12 | 0.71 | 0.52 | 0.18 | 0.31 | 0.46 | 0.55 | 0.16 |
| AIF1v4 | 0.09 | 0.78 | −0.12 | 0.71 | 0.10 | 0.75 | 0.40 | 0.32 | 0.14 | 0.74 | 0.33 | 0.42 | |
| AIF1v3 | 0.04 | 0.90 | −0.13 | 0.70 | 0.08 | 0.80 | 0.26 | 0.53 | 0.10 | 0.82 | 0.12 | 0.78 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piotrowska, K.; Słuczanowska-Głabowska, S.; Kurzawski, M.; Dziedziejko, V.; Kopytko, P.; Paczkowska, E.; Rogińska, D.; Safranow, K.; Machaliński, B.; Pawlik, A. Over-Expression of Allograft Inflammatory Factor-1 (AIF-1) in Patients with Rheumatoid Arthritis. Biomolecules 2020, 10, 1064. https://doi.org/10.3390/biom10071064
Piotrowska K, Słuczanowska-Głabowska S, Kurzawski M, Dziedziejko V, Kopytko P, Paczkowska E, Rogińska D, Safranow K, Machaliński B, Pawlik A. Over-Expression of Allograft Inflammatory Factor-1 (AIF-1) in Patients with Rheumatoid Arthritis. Biomolecules. 2020; 10(7):1064. https://doi.org/10.3390/biom10071064
Chicago/Turabian StylePiotrowska, Katarzyna, Sylwia Słuczanowska-Głabowska, Mateusz Kurzawski, Violetta Dziedziejko, Patrycja Kopytko, Edyta Paczkowska, Dorota Rogińska, Krzysztof Safranow, Bogusław Machaliński, and Andrzej Pawlik. 2020. "Over-Expression of Allograft Inflammatory Factor-1 (AIF-1) in Patients with Rheumatoid Arthritis" Biomolecules 10, no. 7: 1064. https://doi.org/10.3390/biom10071064
APA StylePiotrowska, K., Słuczanowska-Głabowska, S., Kurzawski, M., Dziedziejko, V., Kopytko, P., Paczkowska, E., Rogińska, D., Safranow, K., Machaliński, B., & Pawlik, A. (2020). Over-Expression of Allograft Inflammatory Factor-1 (AIF-1) in Patients with Rheumatoid Arthritis. Biomolecules, 10(7), 1064. https://doi.org/10.3390/biom10071064