

Role of Insulin Resistance as a Mediator of the Relationship between Body Weight, Waist Circumference, and Systolic Blood Pressure in a Pediatric Population
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Baseline and Follow-Up Assessments
2.3. Anthropometric Parameters and Blood Pressure
2.4. Biochemical Parameters
2.5. Recommended Lifestyle Modifications
2.6. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sorof, J.M.; Lai, D.; Turner, J.; Poffenbarger, T.; Portman, R.J. Overweight, Ethnicity, and the Prevalence of Hypertension in School-Aged Children. Pediatrics 2004, 113, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Giussani, M.; Pieruzzi, F.; Vigorita, F.; Arcovio, C.; Cavuto, S.; Stella, A. Results of Blood Pressure Screening in a Population of School-Aged Children in the Province of Milan: Role of Overweight. J. Hypertens. 2005, 23, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Lo, K.; Wong, M.; Khalechelvam, P.; Tam, W. Waist-to-Height Ratio, Body Mass Index and Waist Circumference for Screening Paediatric Cardio-Metabolic Risk Factors: A Meta-Analysis. Obes. Rev. 2016, 17, 1258–1275. [Google Scholar] [CrossRef] [PubMed]
- Genovesi, S.; Antolini, L.; Giussani, M.; Pieruzzi, F.; Galbiati, S.; Valsecchi, M.G.; Brambilla, P.; Stella, A. Usefulness of Waist Circumference for the Identification of Childhood Hypertension. J. Hypertens. 2008, 26, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Blüher, S.; Schwarz, P. Metabolically Healthy Obesity from Childhood to Adulthood-Does Weight Status Alone Matter? Metabolism 2014, 63, 1084–1092. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, T.; Wolters, B.; Knop, C.; Lass, N.; Holl, R.W. Strong Effect of Pubertal Status on Metabolic Health in Obese Children: A Longitudinal Study. J. Clin. Endocrinol. Metab. 2015, 100, 301–308. [Google Scholar] [CrossRef]
- Genovesi, S.; Antolini, L.; Giussani, M.; Brambilla, P.; Barbieri, V.; Galbiati, S.; Mastriani, S.; Sala, V.; Valsecchi, M.G.; Stella, A. Hypertension, Prehypertension, and Transient Elevated Blood Pressure in Children: Association with Weight Excess and Waist Circumference. Am. J. Hypertens 2010, 23, 756–761. [Google Scholar] [CrossRef]
- Genovesi, S.; Brambilla, P.; Giussani, M.; Galbiati, S.; Mastriani, S.; Pieruzzi, F.; Stella, A.; Valsecchi, M.G.; Antolini, L. Insulin Resistance, Prehypertension, Hypertension and Blood Pressure Values in Paediatric Age. J. Hypertens. 2012, 30, 327. [Google Scholar] [CrossRef]
- Shashaj, B.; Luciano, R.; Contoli, B.; Morino, G.S.; Spreghini, M.R.; Rustico, C.; Sforza, R.W.; Dallapiccola, B.; Manco, M. Reference Ranges of HOMA-IR in Normal-Weight and Obese Young Caucasians. Acta Diabetol. 2016, 53, 251–260. [Google Scholar] [CrossRef]
- Genovesi, S.; Orlando, A.; Rebora, P.; Giussani, M.; Antolini, L.; Nava, E.; Parati, G.; Valsecchi, M.G. Effects of Lifestyle Modifications on Elevated Blood Pressure and Excess Weight in a Population of Italian Children and Adolescents. Am. J. Hypertens. 2018, 31, 1147–1155. [Google Scholar] [CrossRef]
- Giussani, M.; Orlando, A.; Tassistro, E.; Lieti, G.; Patti, I.; Antolini, L.; Parati, G.; Genovesi, S. Impact of Lifestyle Modifications on Alterations in Lipid and Glycemic Profiles and Uric Acid Values in a Pediatric Population. Nutrients 2022, 14, 1034. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a Standard Definition for Child Overweight and Obesity Worldwide: International Survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988; ISBN 978-0-87322-121-4. [Google Scholar]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar] [CrossRef]
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society of Hypertension Guidelines for the Management of High Blood Pressure in Children and Adolescents. J. Hypertens. 2016, 34, 1887–1920. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and β-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Gołacki, J.; Matuszek, M.; Matyjaszek-Matuszek, B. Link between Insulin Resistance and Obesity—From Diagnosis to Treatment. Diagnostics 2022, 12, 1681. [Google Scholar] [CrossRef]
- Schofield, W.N. Predicting Basal Metabolic Rate, New Standards and Review of Previous Work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. S1), 5–41. [Google Scholar]
- Torun, B.; Davies, P.S.; Livingstone, M.B.; Paolisso, M.; Sackett, R.; Spurr, G.B. Energy Requirements and Dietary Energy Recommendations for Children and Adolescents 1 to 18 Years Old. Eur. J. Clin. Nutr. 1996, 50 (Suppl. S1), S37–S80; discussion S80–S81. [Google Scholar]
- Flegal, K.M.; Cole, T.J. Construction of LMS Parameters for the Centers for Disease Control and Prevention 2000 Growth Charts. Natl. Health Stat. Rep. 2013, 63, 1–3. [Google Scholar]
- Tagi, V.M.; Mainieri, F.; Chiarelli, F. Hypertension in Patients with Insulin Resistance: Etiopathogenesis and Management in Children. Int. J. Mol. Sci. 2022, 23, 5814. [Google Scholar] [CrossRef]
- Di Pino, A.; DeFronzo, R.A. Insulin Resistance and Atherosclerosis: Implications for Insulin-Sensitizing Agents. Endocr. Rev. 2019, 40, 1447–1467. [Google Scholar] [CrossRef] [PubMed]
- Miniello, V.L.; Faienza, M.F.; Scicchitano, P.; Cortese, F.; Gesualdo, M.; Zito, A.; Basile, M.; Recchia, P.; Leogrande, D.; Viola, D.; et al. Insulin Resistance and Endothelial Function in Children and Adolescents. Int. J. Cardiol. 2014, 174, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Lembo, G.; Napoli, R.; Capaldo, B.; Rendina, V.; Iaccarino, G.; Volpe, M.; Trimarco, B.; Saccà, L. Abnormal Sympathetic Overactivity Evoked by Insulin in the Skeletal Muscle of Patients with Essential Hypertension. J. Clin. Investig. 1992, 90, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Izzo, R.; di Gioia, G.; Losi, M.A.; Barbato, E.; Morisco, C. Insulin Resistance the Hinge Between Hypertension and Type 2 Diabetes. High Blood Press. Cardiovasc. Prev. 2020, 27, 515–526. [Google Scholar] [CrossRef]
- Yuan, Y.; Sun, W.; Kong, X. Comparison between Distinct Insulin Resistance Indices in Measuring the Development of Hypertension: The China Health and Nutrition Survey. Front. Cardiovasc. Med. 2022, 9, 912197. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, W.; Jiang, X. Association between Triglyceride-Glucose Index and Hypertension: A Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 644035. [Google Scholar] [CrossRef]
- Simental-Mendía, L.E.; Hernández-Ronquillo, G.; Gamboa-Gómez, C.I.; Gómez-Díaz, R.; Rodríguez-Morán, M.; Guerrero-Romero, F. The Triglycerides and Glucose Index Is Associated with Elevated Blood Pressure in Apparently Healthy Children and Adolescents. Eur. J. Pediatr. 2019, 178, 1069–1074. [Google Scholar] [CrossRef]
- DeFronzo, R.A. Insulin Resistance, Lipotoxicity, Type 2 Diabetes and Atherosclerosis: The Missing Links. The Claude Bernard Lecture 2009. Diabetologia 2010, 53, 1270–1287. [Google Scholar] [CrossRef]
- Maffeis, C.; Banzato, C.; Brambilla, P.; Cerutti, F.; Corciulo, N.; Cuccarolo, G.; Di Pietro, M.; Franzese, A.; Gennari, M.; Balsamo, A.; et al. Insulin Resistance Is a Risk Factor for High Blood Pressure Regardless of Body Size and Fat Distribution in Obese Children. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 266–273. [Google Scholar] [CrossRef]
- Taittonen, L.; Uhari, M.; Nuutinen, M.; Turtinen, J.; Pokka, T.; Akerblom, H.K. Insulin and Blood Pressure among Healthy Children. Cardiovascular Risk in Young Finns. Am. J. Hypertens. 1996, 9, 194–199. [Google Scholar] [CrossRef]
- Genovesi, S.; Antolini, L.; Orlando, A.; Gilardini, L.; Bertoli, S.; Giussani, M.; Invitti, C.; Nava, E.; Battaglino, M.G.; Leone, A.; et al. Cardiovascular Risk Factors Associated with the Metabolically Healthy Obese (MHO) Phenotype Compared to the Metabolically Unhealthy Obese (MUO) Phenotype in Children. Front. Endocrinol. 2020, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Serbis, A.; Giapros, V.; Paschou, S.A.; Siomou, E. Children with Metabolically Healthy Obesity Have a Worse Metabolic Profile Compared to Normal-Weight Peers: A Cross-Sectional Study. Endocrine 2021, 73, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Savoye, M.; Shaw, M.; Dziura, J.; Tamborlane, W.V.; Rose, P.; Guandalini, C.; Goldberg-Gell, R.; Burgert, T.S.; Cali, A.M.G.; Weiss, R.; et al. Effects of a Weight Management Program on Body Composition and Metabolic Parameters in Overweight Children: A Randomized Controlled Trial. JAMA 2007, 297, 2697–2704. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, C.; Ding, E.L.; Townsend, M.K.; Lipsitz, L.A. Adiponectin Levels and the Risk of Hypertension: A Systematic Review and Meta-Analysis. Hypertension 2013, 62, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Antolini, L.; Street, M.E.; Giussani, M.; Galbiati, S.; Valsecchi, M.G.; Stella, A.; Zuccotti, G.V.; Bernasconi, S.; Genovesi, S. Adiponectin and Hypertension in Normal-Weight and Obese Children. Am. J. Hypertens. 2013, 26, 257–264. [Google Scholar] [CrossRef]
- Su, X.; Peng, D. Adipokines as Novel Biomarkers of Cardio-Metabolic Disorders. Clin. Chim. Acta 2020, 507, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Viazzi, F.; Antolini, L.; Giussani, M.; Brambilla, P.; Galbiati, S.; Mastriani, S.; Stella, A.; Pontremoli, R.; Valsecchi, M.G.; Genovesi, S. Serum Uric Acid and Blood Pressure in Children at Cardiovascular Risk. Pediatrics 2013, 132, e93–e99. [Google Scholar] [CrossRef]
- Loeffler, L.F.; Navas-Acien, A.; Brady, T.M.; Miller, E.R.; Fadrowski, J.J. Uric Acid Level and Elevated Blood Pressure in US Adolescents: National Health and Nutrition Examination Survey, 1999–2006. Hypertension 2012, 59, 811–817. [Google Scholar] [CrossRef]
- Agbaje, A.O. Mediating Role of Body Composition and Insulin Resistance on the Association of Arterial Stiffness with Blood Pressure among Adolescents: The ALSPAC Study. Front. Cardiovasc. Med. 2022, 9, 939125. [Google Scholar] [CrossRef]
- Genovesi, S.; Montelisciani, L.; Viazzi, F.; Giussani, M.; Lieti, G.; Patti, I.; Orlando, A.; Antolini, L.; Salvi, P.; Parati, G. Uric Acid and Arterial Stiffness in Children and Adolescents: Role of Insulin Resistance and Blood Pressure. Front. Cardiovasc. Med. 2022, 9, 978366. [Google Scholar] [CrossRef]
- Wang, R.; Bai, Z.; Zhang, D.; Zhang, R.; Yang, J.; Yin, C.; Huang, W.; Huang, P.; Wang, Y.; Liu, N.; et al. Mediating Effects of Insulin Resistance on the Development of Hypertension Associated with Elevated Serum Uric Acid: A Prospective Cohort Study. J. Hum. Hypertens. 2022, 36, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and obesity. Int. J. Epidemiol. 2014, 43, 655–665. [Google Scholar] [CrossRef]
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; Armstrong, S.C.; Barlow, S.E.; Bolling, C.F.; Avila Edwards, K.C.; Eneli, I.; Hamre, R.; Joseph, M.M.; et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents with Obesity. Pediatrics 2023, 151, e2022060640. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Trieu, K.; Yoshimura, S.; Neal, B.; Woodward, M.; Campbell, N.R.C.; Li, Q.; Lackland, D.T.; Leung, A.A.; Anderson, C.A.M.; et al. Effect of dose and duration of reduction in dietary sodium on blood pressure levels: Systematic review and meta-analysis of randomized trials. BMJ 2020, 368, m315. [Google Scholar] [CrossRef] [PubMed]
- Leyvraz, M.; Chatelan, A.; Da Costa, B.R.; Taffé, P.; Paradis, G.; Bovet, P.; Bochud, M.; Chiolero, A. Sodium intake and blood pressure in children and adolescents: A systematic review and meta-analysis of experimental and observational studies. Int. J. Epidemiol. 2018, 47, 1796–1810. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.W.; Han, K.H.; Han, S.Y.; Koo, H.S.; Kim, S.; Chin, H.J. Association of Sodium Excretion with Metabolic Syndrome, Insulin Resistance, and Body Fat. Medicine 2015, 94, e1650. [Google Scholar] [CrossRef]
- Keske, M.A.; Przewlocka-Kosmala, M.; Woznicka, A.K.; Mysiak, A.; Jankowska, E.A.; Ponikowski, P.; Kosmala, W. Role of Skeletal Muscle Perfusion and Insulin Resistance in the Effect of Dietary Sodium on Heart Function in Overweight. ESC Heart Fail. 2021, 8, 5304–5315. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Baseline (n = 419) | Follow-Up (n = 419) | p-Value |
|---|---|---|---|
| Age (years), mean (SD) | 10.70 (2.46) | 12.21 (2.48) | <0.001 |
| Gender (males), n (%) | 239 (57.04) | - | - |
| Puberty, n (%) | 190 (45.35) | 313 (74.70) | <0.001 |
| Weight (kg), mean (SD) | 52.67 (18.34) | 57.28 (18.12) | <0.001 |
| Height (m), mean (SD) | 1.46 (0.15) | 1.54 (0.14) | <0.001 |
| BMI (kg/m2), mean (SD) | 24.04 (4.76) | 23.70 (4.64) | 0.004 |
| BMI (z-score), mean (SD) | 1.54 (0.92) | 1.24 (0.93) | <0.001 |
| Excess weight (OW + OB), n (%) | 344 (82.10) | 292 (69.69) | <0.001 |
| Waist circumference (cm), mean (SD) | 77.41 (12.94) | 77.19 (12.00) | 0.090 |
| WtHr (%), mean (SD) | 53.10 (7.10) | 50.22 (6.62) | <0.001 |
| SBP (mmHg), mean (SD) | 116.01 (13.86) | 115.00 (13.03) | 0.039 |
| SBP (z-score), mean (SD) | 1.06 (1.08) | 0.70 (1.02) | <0.001 |
| DBP (mmHg), mean (SD) | 67.62 (8.55) | 66.68 (8.21) | 0.038 |
| DBP (z-score), mean (SD) | 0.53 (0.72) | 0.33 (0.69) | <0.001 |
| SBP and/or DBP ≥ 90th percentile, n (%) | 182 (43.44) | 121 (28.88) | <0.001 |
| SBP ≥ 90th percentile, n (%) | 170 (40.57) | 116 (27.68) | <0.001 |
| DBP ≥ 90th percentile, n (%) | 64 (15.27) | 36 (8.59) | 0.001 |
| Glucose (mg/dL), mean (SD) | 83.56 (7.14) | 84.39 (7.68) | 0.044 |
| Insulin (µU//mL), mean (SD) | 13.46 (8.66) | 13.05 (9.11) | 0.357 |
| HOMA-Index, mean (SD) | 2.80 (1.94) | 2.72 (2.06) | 0.654 |
| Total cholesterol (mg/dL), mean (SD) | 97.17 (28.36) | 92.07 (27.14) | <0.001 |
| HDL cholesterol (mg/dL), mean (SD) | 54.00 (12.47) | 54.16 (12.38) | 0.500 |
| Triglycerides (mg/dL), mean (SD) | 76.24 (38.33) | 74.02 (35.95) | 0.249 |
| SBP z-Score | |||||
|---|---|---|---|---|---|
| Coefficient | Std. Err. | p-Value | [95% Conf. Interval] | ||
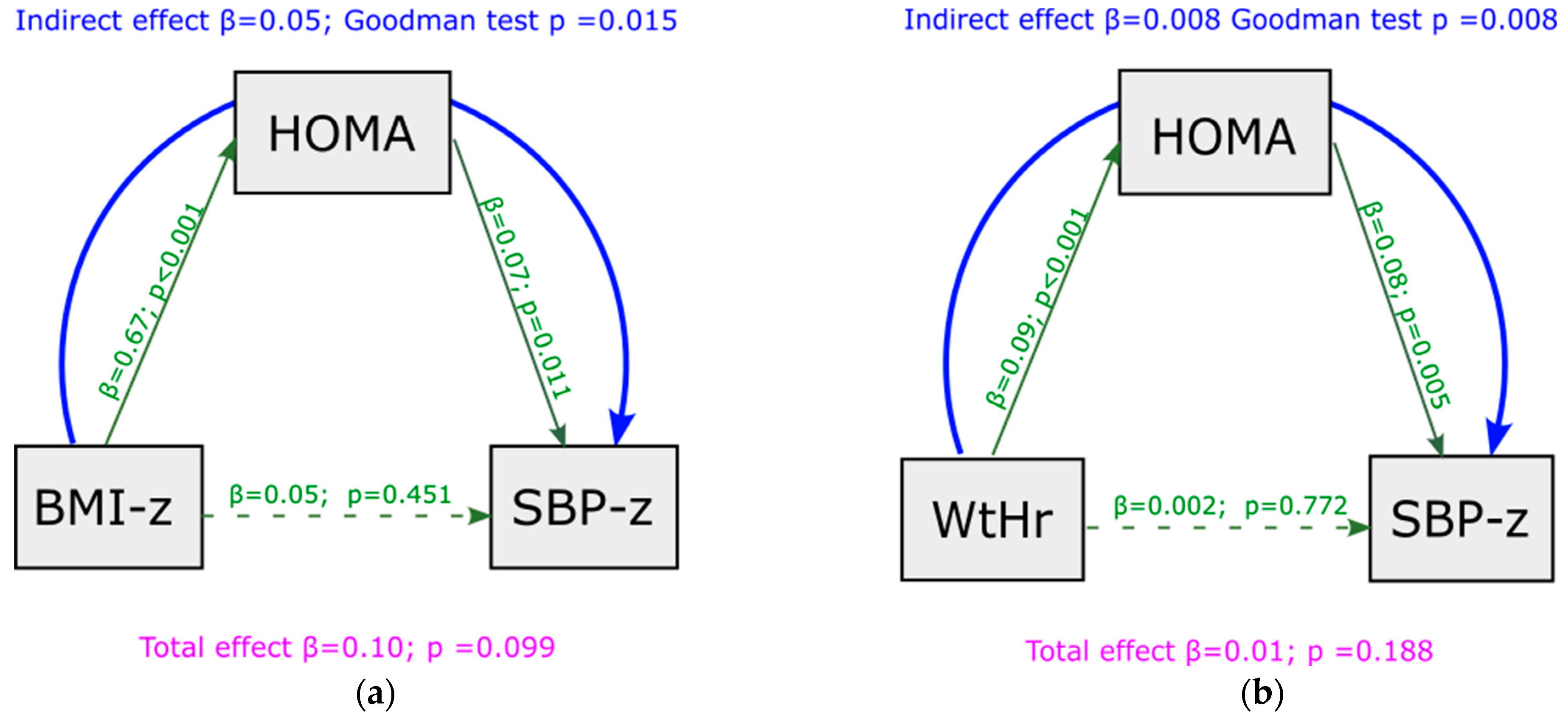
| Model a | HOMA index | 0.08 | 0.03 | 0.003 | (0.027–0.135) |
| Model b | HOMA index | 0.07 | 0.03 | 0.011 | (0.017–0.131) |
| BMI z-score | 0.05 | 0.06 | 0.451 | (−0.074–0.165) | |
| Model b | HOMA index | 0.08 | 0.23 | 0.005 | (0.026–0.142) |
| WtHr | 0.002 | 0.01 | 0.772 | (−0.013–0.018) | |
| DBP z-score | |||||
| Coefficient | Std. Err. | p-value | [95% conf. Interval] | ||
| Model a | HOMA index | 0.03 | 0.02 | 0.123 | (−0.008–0.064) |
| Model b | HOMA index | 0.02 | 0.02 | 0.256 | (−0.016–0.059) |
| BMI z-score | 0.04 | 0.04 | 0.306 | (−0.038–0.120) | |
| Model b | HOMA index | 0.02 | 0.02 | 0.253 | (−0.016–0.060) |
| WtHr | 0.01 | 0.01 | 0.072 | (−0.001–0.020) | |
| Coefficient | Std. Err. | p-Value | [95% Conf. Interval] | |
|---|---|---|---|---|
| Delta BMI (z-Score) | 0.26 | 0.11 | 0.025 | (0.03–0.48) |
| Delta WtHr | 0.03 | 0.01 | 0.002 | (0.01–0.06) |
| Delta HOMA-index | 0.08 | 0.02 | 0.001 | 0.03–0.13 |
| Coefficient | Std. Err. | p-Value | [95% Conf. Interval] | |
|---|---|---|---|---|
| Delta HOMA Index | 0.07 | 0.02 | 0.004 | (0.023–0.121) |
| Delta BMI (z-score) | 0.13 | 0.12 | 0.273 | (−0.104–0.367) |
| Delta HOMA Index | 0.05 | 0.03 | 0.045 | (0.001–0.103) |
| Delta WtHr | 0.03 | 0.01 | 0.011 | (0.007–0.050) |
| Delta HOMA Index | 0.07 | 0.03 | 0.017 | (0.012–0.121) |
| Delta BMI (z-score) | 0.17 | 0.13 | 0.193 | (−0.090–0.424) |
| Pre-puberty to Puberty | −0.15 | 0.12 | 0.221 | (−0.395–0.092) |
| Delta HOMA Index | 0.05 | 0.03 | 0.064 | (−0.003–0.106) |
| Delta WtHr | 0.03 | 0.01 | 0.029 | (0.003–0.048) |
| Pre-puberty to Puberty | −0.17 | 0.13 | 0.179 | (−0.424–0.080) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genovesi, S.; Montelisciani, L.; Giussani, M.; Lieti, G.; Patti, I.; Orlando, A.; Antolini, L.; Parati, G. Role of Insulin Resistance as a Mediator of the Relationship between Body Weight, Waist Circumference, and Systolic Blood Pressure in a Pediatric Population. Metabolites 2023, 13, 327. https://doi.org/10.3390/metabo13030327
Genovesi S, Montelisciani L, Giussani M, Lieti G, Patti I, Orlando A, Antolini L, Parati G. Role of Insulin Resistance as a Mediator of the Relationship between Body Weight, Waist Circumference, and Systolic Blood Pressure in a Pediatric Population. Metabolites. 2023; 13(3):327. https://doi.org/10.3390/metabo13030327
Chicago/Turabian StyleGenovesi, Simonetta, Laura Montelisciani, Marco Giussani, Giulia Lieti, Ilenia Patti, Antonina Orlando, Laura Antolini, and Gianfranco Parati. 2023. "Role of Insulin Resistance as a Mediator of the Relationship between Body Weight, Waist Circumference, and Systolic Blood Pressure in a Pediatric Population" Metabolites 13, no. 3: 327. https://doi.org/10.3390/metabo13030327
APA StyleGenovesi, S., Montelisciani, L., Giussani, M., Lieti, G., Patti, I., Orlando, A., Antolini, L., & Parati, G. (2023). Role of Insulin Resistance as a Mediator of the Relationship between Body Weight, Waist Circumference, and Systolic Blood Pressure in a Pediatric Population. Metabolites, 13(3), 327. https://doi.org/10.3390/metabo13030327