
Feasibility of Provision and Vaccine Hesitancy at a Central Hospital COVID-19 Vaccination Site in South Africa after Four Waves of the Pandemic

 , , ,
, , ,
Abstract
1. Introduction
2. Aim and Objectives
2.1. Aim
2.2. Objectives
- To assess vaccination uptake, coverage, and hesitancy among people attending a central hospital.
- To determine factors associated with and influencing vaccination status.
- To document the implementation and assess the acceptability of the vaccination project among staff and persons attending the hospital.
3. Materials and Methods
3.1. Study Design
3.2. Setting
3.3. Sample Population, Size, and Sampling
3.3.1. Enrolment for the Quantitative Component
3.3.2. Enrolment for the Qualitative Component
3.4. Data Collection
3.5. Data Analysis
3.5.1. Quantitative Data
3.5.2. Qualitative Data
4. Results
4.1. Quantitative Component
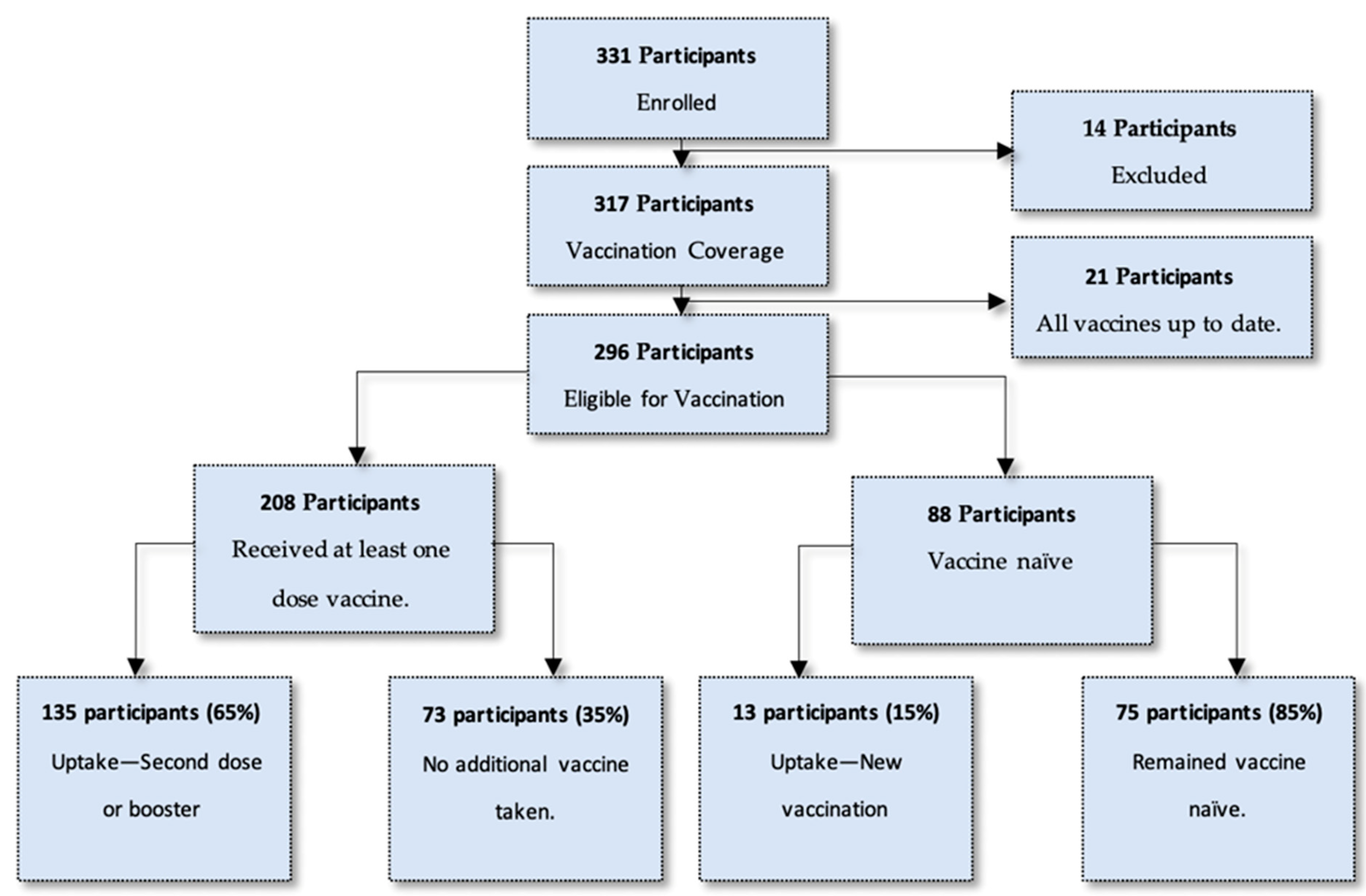
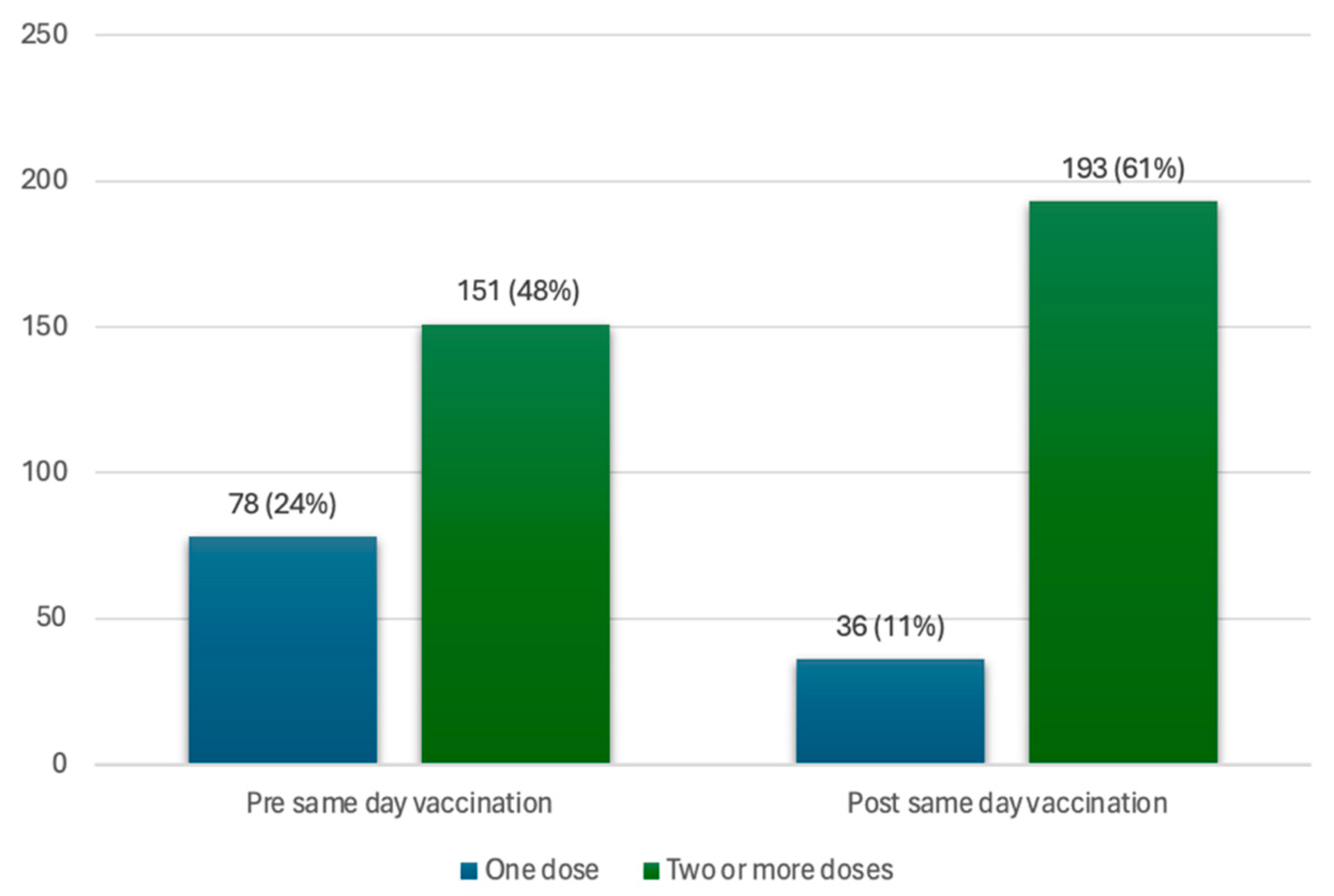
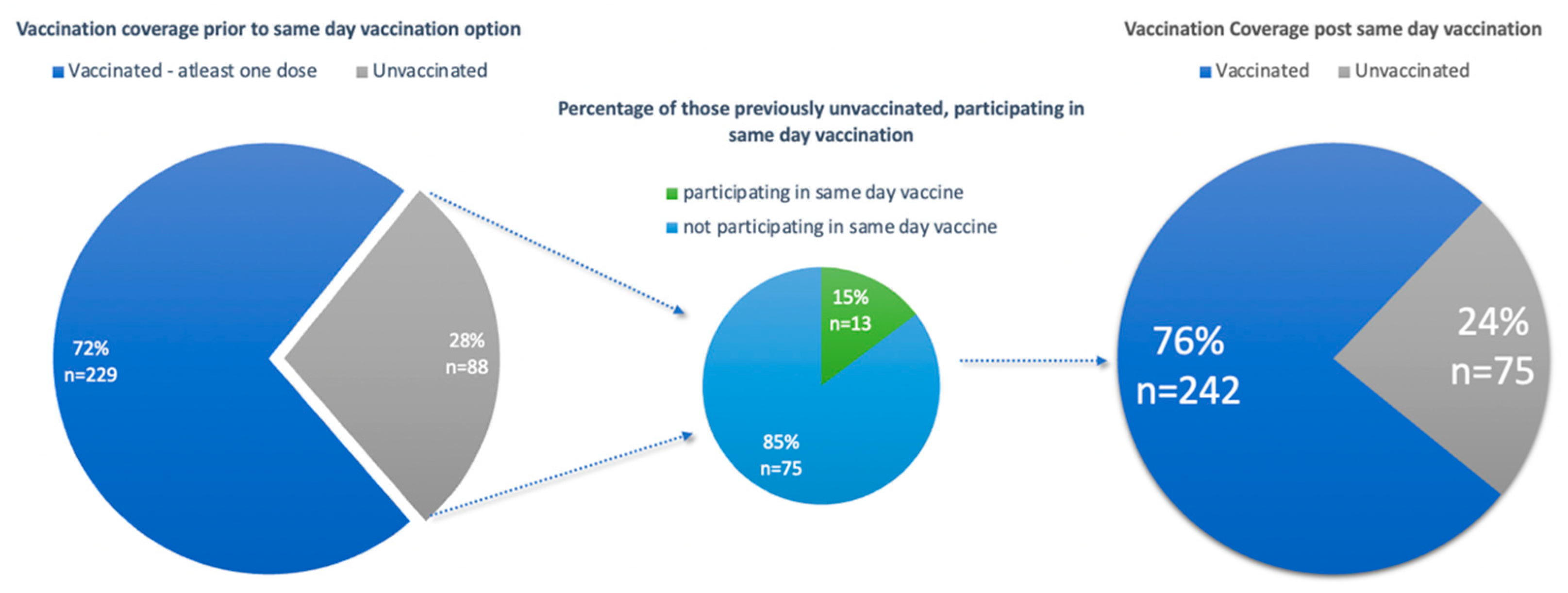
4.1.1. Vaccination Uptake at Enrolment
4.1.2. Vaccination Coverage and Vaccination hesitancy
4.1.3. Sociodemographic Information of Participants
4.1.4. Factors Associated with Vaccination Status
4.1.5. Knowledge of the Vaccination Site
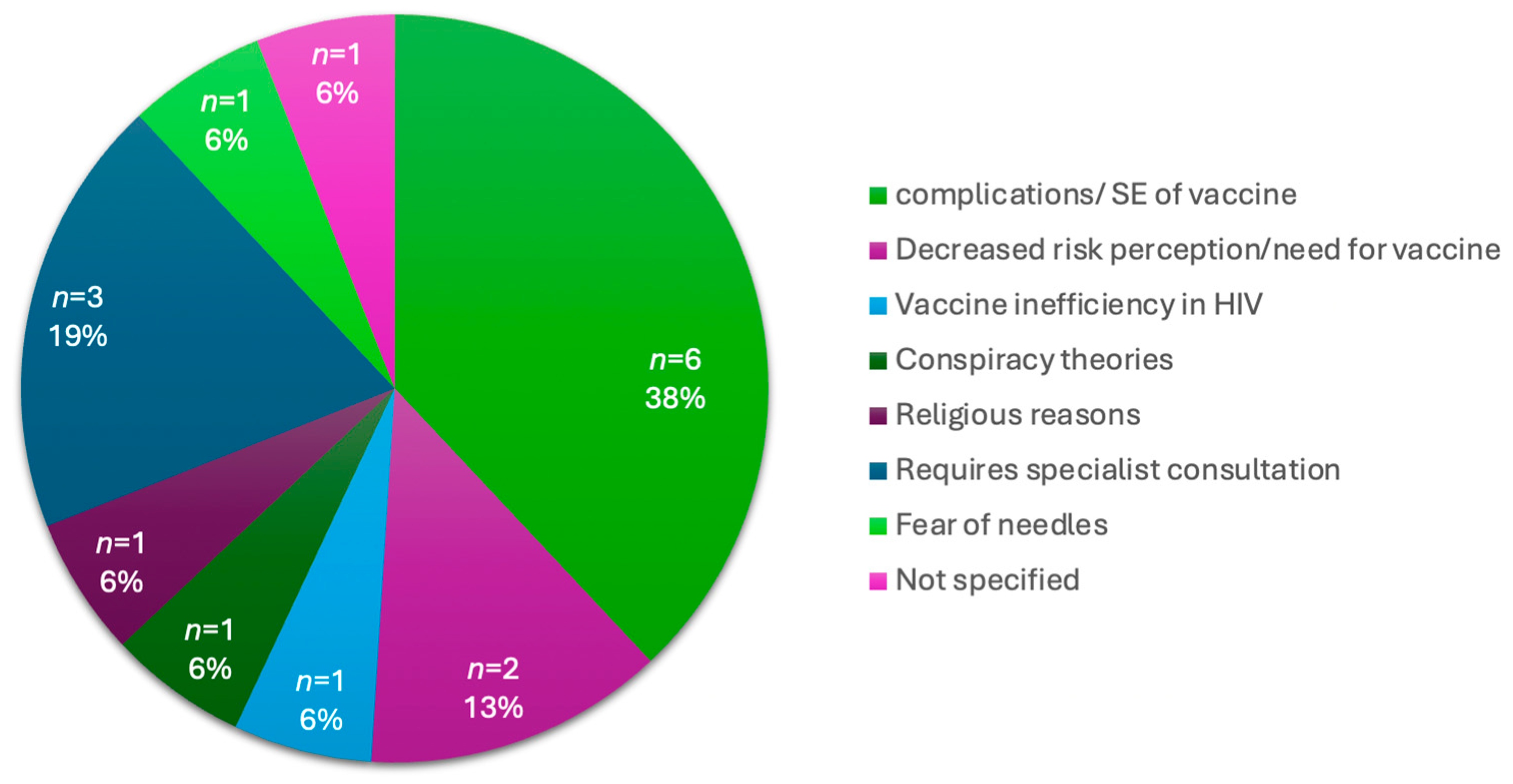
4.1.6. Vaccine Hesitancy in Vaccine Naïve Participants
4.2. Qualitative Findings
4.2.1. Perceptions of Vulnerability
“It helps with COVID-19; so that one does not get infected with COVID.”(Key Informant 19)
“It’s not that I don’t want to be vaccinated in your site, the thing is I have already gotten an injection already, so I no longer see the importance of getting the booster.”(Key Informant 10)
4.2.2. Vaccine Safety and Efficacy Concerns
“I want to ask my doctor first about it is safe to do it or it’s not safe. Because if I can do it, and then have complications, the doctor he will say that I didn’t tell you to do it. So, I must ask him first that’s when I will come back and get it.”(Key Informant 12)
“I’m not saying that the vaccine is not helping people, it is. But me personally—like I said—yeah, I’m worried about it affecting my diabetic treatment.”(Key Informant 18)
“I’m scared it’s going to be the 666 and I don’t want to go to hell, I want to go to heaven.”(Key Informant 27)
4.2.3. Information Gaps and Mistrust Leading to Hesitancy
“I personally feel that the amount of research that went into the vaccine was not enough, the timeframe was very short since the announcement of the COVID pandemic and the vaccine coming out.”(Key Informant 35)
“Healthcare workers have been very resistant to coming in for vaccination and to a large extent, they influenced the patient, the caregivers, and the patient’s opinion about vaccination.(Key Informant 35)
4.2.4. Value of Convenience in Decisions to Vaccinate
“It is easy to come to the hospital to fetch the medication and to get vaccinated.”(Key Informant 26)
“What I can say is that maybe it’s a little bit convenient [speaking of the vaccination site]. It’s a little bit more convenient than visiting an outside place.”(Key Informant 38)
4.2.5. The Role of Health Promoters
“I was about to go home (after) finishing collecting my medication, so I met the sister (nurse) there, (s)he told me about the vaccination, that there is a vaccination site here at the hospital.”(Key Informant 24)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Department of Health, Republic of South Africa. COVID-19 Daily Updates & Cases COVID-19 Online Resource & News Portal 2024. Available online: https://sacoronavirus.co.za/covid-19-daily-cases/ (accessed on 13 February 2024).
- Zar, H.J.; MacGinty, R.; Workman, L.; Botha, M.; Johnson, M.; Hunt, A.; Bird, T.; Nicol, M.P.; Flasche, S.; Quilty, B.J.; et al. Natural and hybrid immunity following four COVID-19 waves in a South African cohort. medRxiv, 2022; preprint. [Google Scholar]
- Madhi, S.A.; Kwatra, G.; Myers, J.E.; Jassat, W.; Dhar, N.; Mukendi, C.K.; Nana, A.J.; Blumberg, L.; Welch, R.; Ngorima-Mabhena, N.; et al. Population Immunity and COVID-19 Severity with Omicron Variant in South Africa. N. Engl. J. Med. 2022, 386, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Bertagnolio, S.; Thwin, S.S.; Silva, R.; Nagarajan, S.; Jassat, W.; Fowler, R.; Haniffa, R.; Reveiz, L.; Ford, N.; Doherty, M.; et al. Clinical features of, and risk factors for, severe or fatal COVID-19 among people living with HIV admitted to hospital: Analysis of data from the WHO Global Clinical Platform of COVID-19. Lancet HIV 2022, 9, e486–e495. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Deaprtment of Health, Republic of South Africa. National Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2022–2027; National Department of Health: Cape Town, South Africa, 2022. [Google Scholar]
- Department of Health, Republic of South Africa. COVID-19 Vaccine Rollout Strategy COVID-19 Online Resource & News Portal. 2021. Available online: https://sacoronavirus.co.za/2021/01/12/what-does-south-africas-covid-vaccine-roll-out-plan-say/ (accessed on 13 February 2024).
- WHO. Interim Recommendations for the Use of the Jannesn Ad26.COV2.S (COVID-19) Vaccine; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; De Villiers, T.; Van der Walt, Z.; et al. Decreased severity of disease during the first global omicron variant COVID-19 outbreak in a large hospital in Tshwane, South Africa. Int. J. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; Denis, K.J.S.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef] [PubMed]
- Sifunda, S.; Mbewu, A.D.; Mabaso, M.; Manyaapelo, T.; Sewpaul, R.; Morgan, J.W.; Harriman, N.W.; Williams, D.R.; Reddy, S.P. Prevalence and Psychosocial Correlates of Diabetes Mellitus in South Africa: Results from the South African National Health and Nutrition Examination Survey (SANHANES-1). Int. J. Environ. Res. Public Health 2023, 20, 5798. [Google Scholar] [CrossRef] [PubMed]
- SANAC. National Strategic Plan For HIV, TB and STIs 2023–2028; South African National AIDS Council (SANAC): Pretoria, South Africa, 2023. [Google Scholar]
- Jassat, W.; Mudara, C.; Ozougwu, L.; Welch, R.; Arendse, T.; Masha, M.; Blumberg, L.; Kufa, T.; Puren, A.; Groome, M.; et al. Trends in COVID-19 admissions and deaths among people living with HIV in South Africa: Analysis of national surveillance data. Lancet HIV 2024, 11, e96–e105. [Google Scholar] [CrossRef] [PubMed]
- Western Cape Dept Health in Collaboration with the NICD SA. Risk factors for coronavirus disease 2019 (COVID-19) death in a population cohort study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, Republic of South Africa. Latest Vaccine Statistics 2024. 2024. Available online: https://sacoronavirus.co.za/latest-vaccine-statistics/ (accessed on 13 February 2024).
- Yuan, J.; Lam, W.W.T.; Xiao, J.; Ni, M.Y.; Cowling, B.J.; Liao, Q. Why do Chinese older adults in Hong Kong delay or refuse COVID-19 vaccination? A qualitative study based on Grounded Theory. J. Gerontol. Ser. B 2023, 78, 736–748. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Adu, P.; Popoola, T.; Medvedev, O.N.; Collings, S.; Mbinta, J.; Aspin, C.; Simpson, C.R. Implications for COVID-19 vaccine uptake: A systematic review. J. Infect. Public Health 2023, 16, 441–466. [Google Scholar] [CrossRef] [PubMed]
- Cokro, F. Supporting and inhibiting factors of accepting COVID-19 booster vaccination in the elderly in north Jakarta, Indonesia. Pharm. Pract. 2022, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lu, X.; Lai, X.; Lyu, Y.; Zhang, H.; Fenghuang, Y.; Jing, R.; Li, L.; Yu, W.; Fang, H. The Changing Acceptance of COVID-19 Vaccination in Different Epidemic Phases in China: A Longitudinal Study. Vaccines 2021, 9, 191. [Google Scholar] [CrossRef]
- Hajissa, K.; Mutiat, H.A.; Kaabi, N.A.; Alissa, M.; Garout, M.; Alenezy, A.A.; Almaghrabi, R.H.; Alrasheed, H.A.; Al-Subaie, M.F.; Alhani, H.M.; et al. COVID-19 Vaccine Acceptance and Hesitancy among Migrants, Refugees, and Foreign Workers: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 1070. [Google Scholar] [CrossRef]
- Engelbrecht, M.; Heunis, C.; Kigozi, G. COVID-19 vaccine hesitancy in South Africa: Lessons for future pandemics. Int. J. Environ. Res. Public Health 2022, 19, 6694. [Google Scholar] [CrossRef] [PubMed]
- Sarker, R.; Roknuzzaman, A.; Hossain, M.J.; Bhuiyan, M.A.; Islam, M.R. The WHO declares COVID-19 is no longer a public health emergency of international concern: Benefits, challenges, and necessary precautions to come back to normal life. Int. J. Surg. 2023, 109, 2851–2852. [Google Scholar] [CrossRef]
- Kennedy, E.B.; Daoust, J.-F.; Vikse, J.; Nelson, V. “Until I Know It’s Safe for Me”: The Role of Timing in COVID-19 Vaccine Decision-Making and Vaccine Hesitancy. Vaccines 2021, 9, 1417. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Department of Health, Republic of South Africa. National Vaccination Programme Circular 2 of 2022. In Health NDo; Government Printers: Pretoria, South Africa, 2022. [Google Scholar]
- Department of Health, Republic of South Africa. National Vaccination Programme Circular 1 of 2023. In Health NDo; Government Printers: Pretoria, South Africa, 2023. [Google Scholar]
- WHO. International Classification of Diseases, Eleventh Revision (ICD-11); World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Kandeel, A.; Eldeyahy, I.; Abu ElSood, H.; Fahim, M.; Afifi, S.; Abu Kamar, S.; BahaaEldin, H.; Ahmed, E.; Mohsen, A.; Abdelghaffar, K.; et al. COVID-19 vaccination coverage in Egypt: A large-scale national survey–to help achieve vaccination target, March-May, 2022. BMC Public Health 2023, 23, 397. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Miraglia del Giudice, G.; Folcarelli, L.; Della Polla, G.; Napoli, A.; Angelillo, I.F. Investigating the reasons for receiving the second booster dose of the COVID-19 vaccine in adults and in people with chronic medical conditions in southern Italy. Vaccines 2023, 11, 737. [Google Scholar] [CrossRef]
- Morgan, A.K.; Aziire, M.A.; Cobbold, J.; Agbobada, A.A.; Kudzawu, S.K. Hesitant or not: A cross-sectional study of socio-demographics, conspiracy theories, trust in public health information, social capital and vaccine hesitancy among older adults in Ghana. Hum. Vaccines Immunother. 2023, 19, 2211495. [Google Scholar] [CrossRef]
- Heidari, S.; Palmer-Ross, A.; Goodman, T. A systematic review of the sex and gender reporting in COVID-19 clinical trials. Vaccines 2021, 9, 1322. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, M.A.; Jones, B.L.; Gandhi, M. COVID-19 outcomes and risk factors among people living with HIV. Curr. HIV/AIDS Rep. 2022, 19, 425–432. [Google Scholar] [CrossRef]
- Celewicz, A.; Celewicz, M.; Michalczyk, M.; Woźniakowska-Gondek, P.; Krejczy, K.; Misiek, M.; Rzepka, R. Pregnancy as a risk factor of severe COVID-19. J. Clin. Med. 2021, 10, 5458. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, K.L.; Oyenuga, R.O.; Olafuyi, O.; Schwartz, D.A. Focus: Pregnancy and Child Development: Causes and Effects of COVID-19 Vaccine Hesitancy Among Pregnant Women and its Association with Adverse Maternal, Placental, and Perinatal Outcomes. Yale J. Biol. Med. 2024, 97, 73. [Google Scholar] [CrossRef]
- Sialubanje, C.; Mukumbuta, N.; Ng’andu, M.; Sumani, E.M.; Nkonkomalimba, M.; Lyatumba, D.E.; Mwale, A.; Mpiana, F.; Zulu, J.M.; Mweempwa, B.; et al. Perspectives on the COVID-19 vaccine uptake: A qualitative study of community members and health workers in Zambia. BMJ Open 2022, 12, e058028. [Google Scholar] [CrossRef] [PubMed]
- Miraglia del Giudice, G.; Napoli, A.; Corea, F.; Folcarelli, L.; Angelillo, I.F. Evaluating COVID-19 vaccine willingness and hesitancy among parents of children aged 5–11 years with chronic conditions in Italy. Vaccines 2022, 10, 396. [Google Scholar] [CrossRef]
- Algabbani, A.; AlOmeir, O.; Algabbani, F. Vaccine hesitancy in the Gulf Cooperation Council countries. East. Mediterr. Health J. 2023, 29, 402–411. [Google Scholar] [CrossRef]
- Papageorgiou, C.; Mazeri, S.; Karaiskakis, M.; Constantinou, D.; Nikolaides, C.; Katsouris, S.; Patsalou, M.; Kourouzidou, D.; Pantelas, G.; Koliou, M. Exploring vaccination coverage and attitudes of health care workers towards influenza vaccine in Cyprus. Vaccine 2022, 40, 1775–1782. [Google Scholar] [CrossRef]
- Fisk, R.J. Barriers to vaccination for coronavirus disease 2019 (COVID-19) control: Experience from the United States. Glob. Health J. 2021, 5, 51–55. [Google Scholar] [CrossRef]
- Gallant, A.J.; Flowers, P.; Deakin, K.; Cogan, N.; Rasmussen, S.; Young, D.; Williams, L. Barriers and enablers to influenza vaccination uptake in adults with chronic respiratory conditions: Applying the behaviour change wheel to specify multi-levelled tailored intervention content. Psychol. Health 2023, 38, 147–166. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category of Participants | Number (N)—Vaccinated (%) | Number (N)—Vaccine Naïve (%) | Total |
|---|---|---|---|
| Patient | 122 (75.3) | 40 (25.7) | 162 |
| Hospital Visit | 59 | 34 | 69 |
| Medication Collection | 63 | 6 | 93 |
| Patient Companion | 58 (72.5) | 22 (27.5) | 80 |
| Accompanied Patient for Visit | 43 | 17 | 60 |
| Mediation Collection on Behalf of Patient | 8 | 4 | 12 |
| Visiting Inpatient | 7 | 1 | 8 |
| Staff | 28 (70) | 12 (30) | 40 |
| Community members—Attending for Vaccination | 32 (100) | 0 (0) | 32 |
| Other | 2 (66.6) * | 1 (33.3) ** | 3 |
| Total | 242 (76.3) | 75 (23.7) | 317 |
| Characteristics | Number Vaccinated out of 242 (n) | Percentage of Those Vaccinated (%) | Number Vaccine Naïve out of 75 (n) | Percentage of Those Vaccine naïve (%) | Total Participants out of 317 (N) | p-Value |
|---|---|---|---|---|---|---|
| Socio-demographic | ||||||
| Age Category | ||||||
| 18–39 | 83 | 34.3 | 45 | 60.0 | 128 | 0.000 |
| 40–64 | 109 | 45.0 | 22 | 29.3 | 131 | |
| 65–90 | 50 | 20.7 | 8 | 10.1 | 58 | |
| Gender | ||||||
| Male | 106 | 43.8 | 38 | 50.7 | 144 | 0.297 |
| Female | 136 | 56.2 | 37 | 49.3 | 173 | |
| Employment Status | ||||||
| Employed | 90 | 37.2 | 25 | 33.3 | 115 | 0.544 |
| Unemployed | 152 | 62.8 | 50 | 66.7 | 202 | |
| Nationality | ||||||
| South African | 236 | 97.5 | 72 | 96.0 | 308 | 0.488 |
| Non-South African | 6 | 2.5 | 3 | 4.0 | 9 | |
| Underlying medical condition | ||||||
| Diabetes | ||||||
| Yes | 25 | 10.3 | 6 | 8.0 | 31 | 0.553 |
| No | 217 | 89.7 | 69 | 92.0 | 286 | |
| Hypertension | ||||||
| Yes | 86 | 35.5 | 16 | 21.3 | 102 | 0.021 |
| No | 156 | 64.5 | 59 | 78.7 | 215 | |
| HIV | ||||||
| Yes | 16 | 6.6 | 3 | 4.0 | 19 | 0.405 |
| No | 226 | 93.4 | 72 | 96.0 | 298 | |
| Other | ||||||
| Yes | 79 | 32.6 | 32 | 42.7 | 111 | 0.112 |
| Category of Other Diseases | Number (n)—Vaccinated | Number (n)—Vaccine Naïve | Total |
|---|---|---|---|
| Neoplasms | 4 | 1 | 5 |
| Diseases of circulatory systems | 24 | 16 | 40 |
| Diseases of digestive system | 4 | 2 | 6 |
| Diseases of blood or blood forming organs | 1 | 0 | 1 |
| Diseases of immune systems | 1 | 1 | 2 |
| Diseases of endocrine and nutrition | 7 | 1 | 8 |
| Diseases of genitourinary systems | 2 | 0 | 2 |
| Diseases of infectious and parasitic | 2 | 1 | 3 |
| Diseases of mental, behavioural | 4 | 1 | 5 |
| Diseases of musculoskeletal | 16 | 4 | 20 |
| Diseases of nervous systems | 4 | 2 | 6 |
| Diseases of respiratory system | 7 | 2 | 9 |
| Diseases of skin | 2 | 0 | 2 |
| Diseases of visual systems | 1 | 0 | 1 |
| Other | 0 | 1 | 0 |
| Total | 79 | 32 | 111 |
| Univariable Analysis | |||
| Characteristics | Crude OR | 95% CI | p-Value |
| Socio-demographic | |||
| Age category (years) | |||
| 18–39 | 1.00 | ||
| 40–64 | 2.69 | 1.50–4.82 | 0.001 |
| 65–90 | 3.38 | 1.48–7.77 | 0.004 |
| Gender | |||
| Male | 1.00 | ||
| Female | 1.38 | 0.78–2.21 | 0.298 |
| Employment status | |||
| Unemployed | 1.00 | ||
| Employed | 1.18 | 0.69–2.04 | 0.544 |
| Nationality | |||
| South African | 1.00 | ||
| Non-South African | 0.61 | 0.15–2.50 | 0.493 |
| Underlying medical condition | |||
| Diabetes | |||
| Yes | 1.32 | 0.52–3.36 | 0.554 |
| No | 1.00 | ||
| Hypertension | |||
| Yes | 2.03 | 1.10–3.74 | 0.023 |
| No | 1.00 | ||
| HIV | |||
| Yes | 1.69 | 0.48–6.00 | 0.410 |
| No | 1.00 | ||
| Other Disease | |||
| Yes | 0.68 | 0.40-1.15 | 0.148 |
| No | 1.00 | ||
| Multivariable analysis | |||
| Characteristic | Adjusted OR | 95% CI | p-Value |
| Age category (years) | |||
| 18–39 | 1.00 | ||
| 40–64 | 3.48 | 1.85–6.53 | 0.000 |
| 65–90 | 5.22 | 2.13–12.83 | 0.000 |
| Other Disease | |||
| Yes | 0.39 | 0.21–0.72 | 0.003 |
| No | 1.00 | ||
| Characteristics | Number (n) | Percentage of Total Participants n = 317 (%) |
|---|---|---|
| Knowledge of vaccination site | ||
| Doctor/Nurse | 50 | 15.8 |
| Overheard another patient | 2 | 0.6 |
| Visual | 23 | 7.3 |
| Community | 15 | 4.7 |
| Healthcare promoter | 202 | 63.7 |
| Hospital department | 19 | 6.0 |
| Other | 6 | 1.9 |
| Total | 317 | 100 |
| Reasons for Vaccine Hesitancy in Vaccine Naïve Participants | Number (n) | Percentage of Total Participants n = 75 (%) |
|---|---|---|
| Do not believe in vaccines | 21 | 28 |
| Do not have the time | 7 | 9.3 |
| Do not want to get vaccine | 23 | 30.7 |
| Will come back another time | 8 | 10.7 |
| Other | 16 | 21.3 |
| Total | 75 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nair, S.; Tshabalala, K.; Slingers, N.; Vanleeuw, L.; Basu, D.; Abdullah, F. Feasibility of Provision and Vaccine Hesitancy at a Central Hospital COVID-19 Vaccination Site in South Africa after Four Waves of the Pandemic. Diseases 2024, 12, 113. https://doi.org/10.3390/diseases12060113
Nair S, Tshabalala K, Slingers N, Vanleeuw L, Basu D, Abdullah F. Feasibility of Provision and Vaccine Hesitancy at a Central Hospital COVID-19 Vaccination Site in South Africa after Four Waves of the Pandemic. Diseases. 2024; 12(6):113. https://doi.org/10.3390/diseases12060113
Chicago/Turabian StyleNair, Shanal, Khanyisile Tshabalala, Nevilene Slingers, Lieve Vanleeuw, Debashis Basu, and Fareed Abdullah. 2024. "Feasibility of Provision and Vaccine Hesitancy at a Central Hospital COVID-19 Vaccination Site in South Africa after Four Waves of the Pandemic" Diseases 12, no. 6: 113. https://doi.org/10.3390/diseases12060113
APA StyleNair, S., Tshabalala, K., Slingers, N., Vanleeuw, L., Basu, D., & Abdullah, F. (2024). Feasibility of Provision and Vaccine Hesitancy at a Central Hospital COVID-19 Vaccination Site in South Africa after Four Waves of the Pandemic. Diseases, 12(6), 113. https://doi.org/10.3390/diseases12060113