
Systematic Review on the Effectiveness and Outcomes of Nivolumab Treatment Schemes in Advanced and Metastatic Cervical Cancer

 , , and
, , and
Abstract
1. Introduction
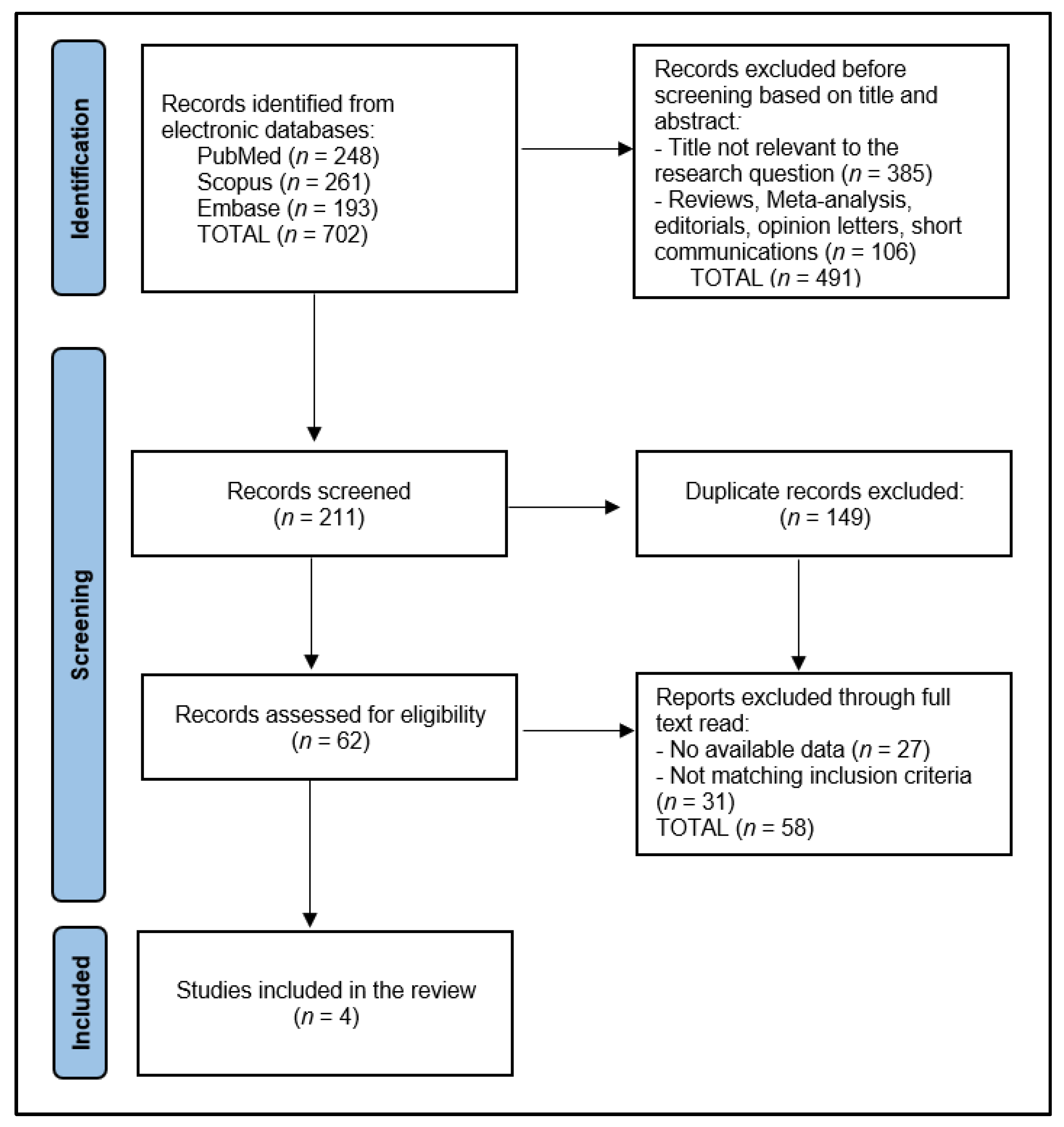
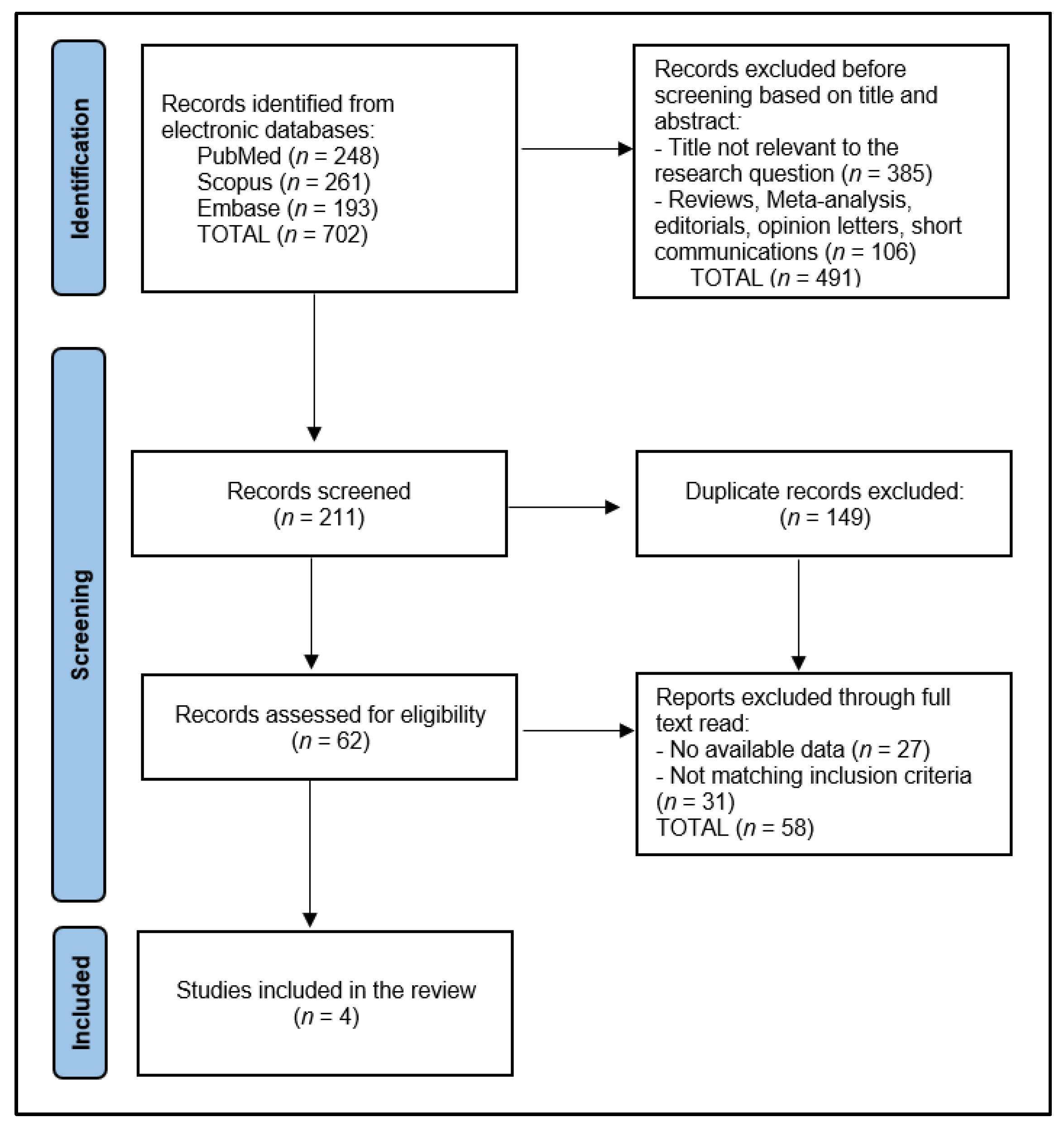
2. Materials and Methods
2.1. Protocol and Registration
2.2. Inclusion and Exclusion Criteria
2.3. Definitions
2.4. Data Collection Protocol
2.5. Quality Assessment
3. Results
3.1. Study Characteristics
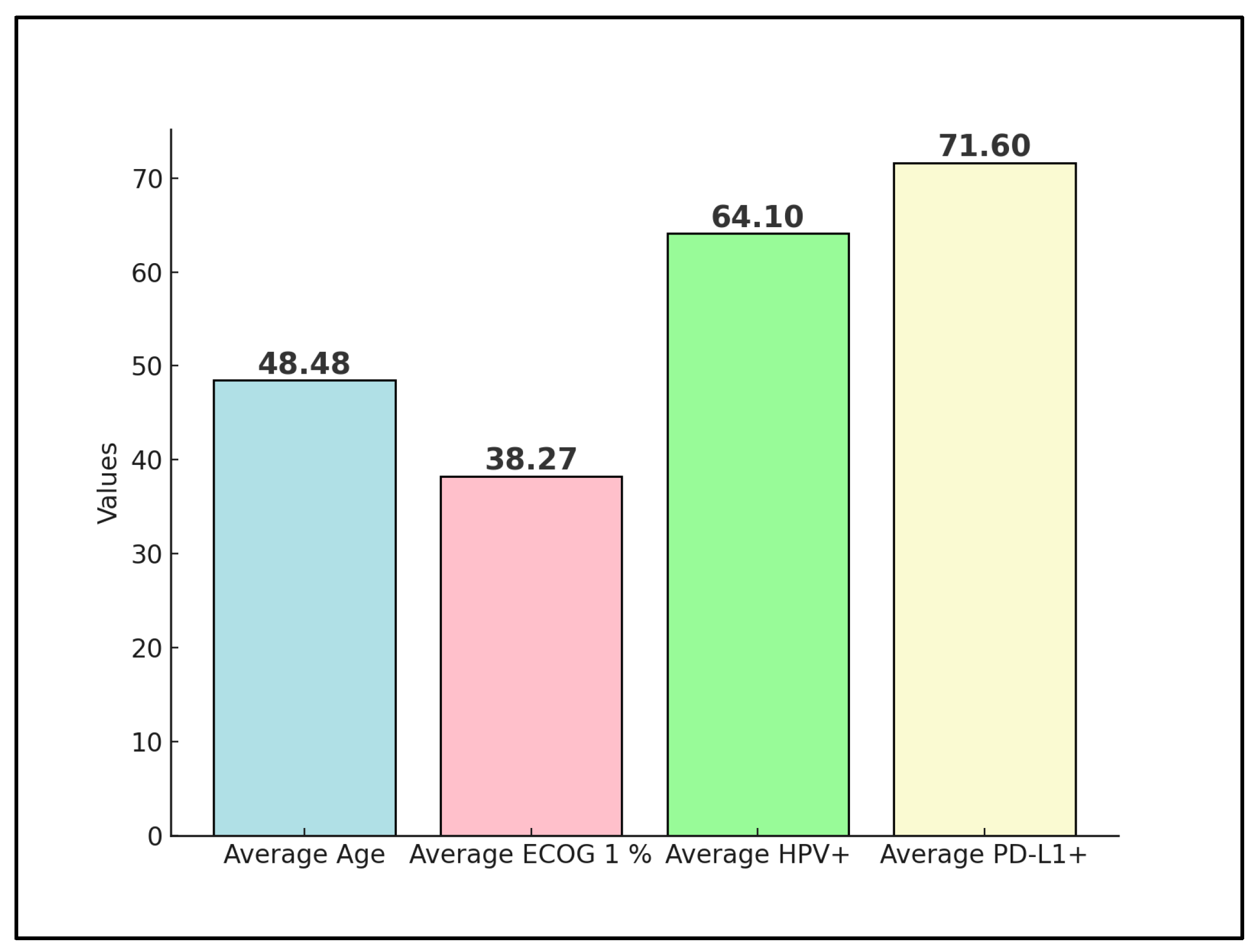
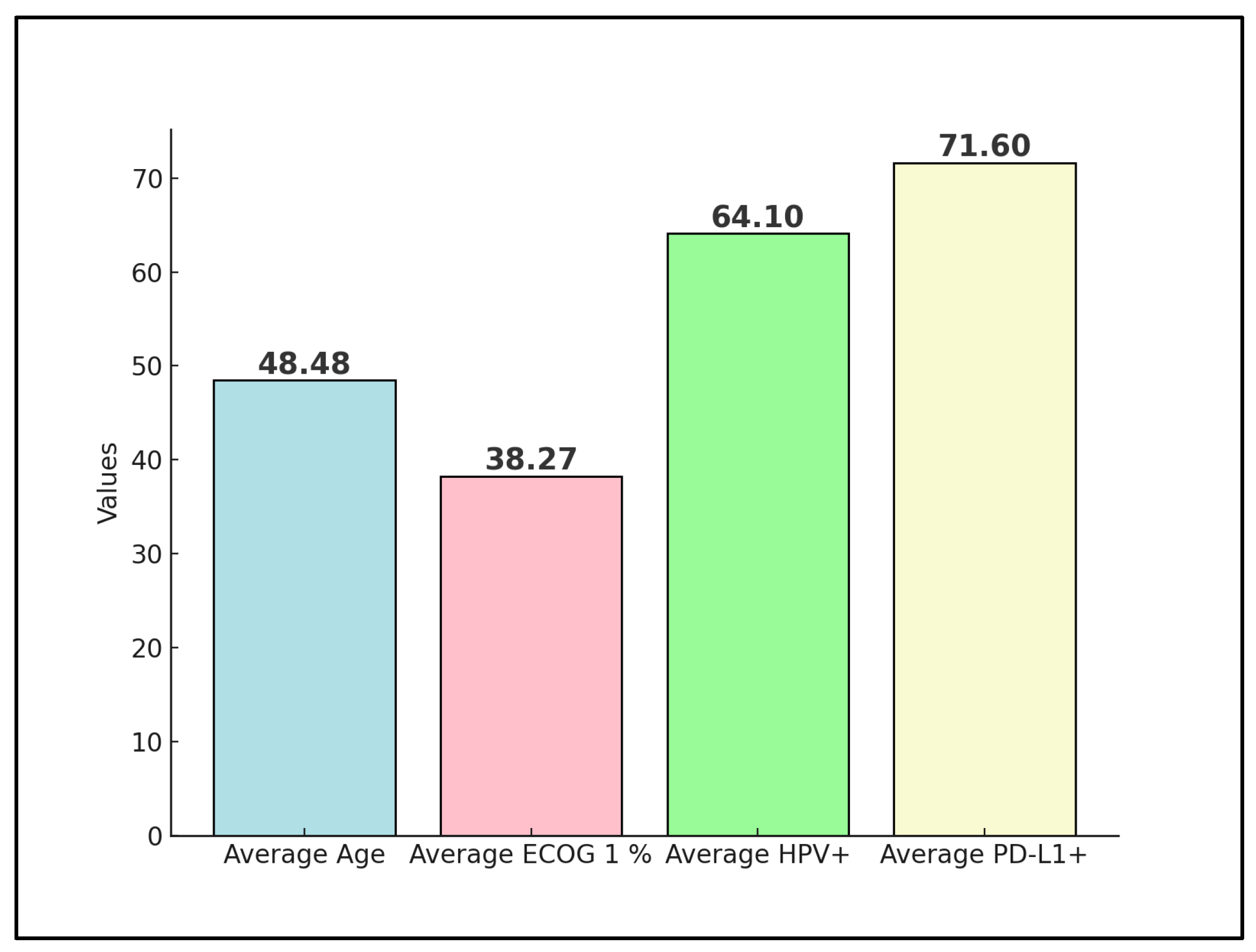
3.2. Patients’ Characteristics
3.3. Disease Characteristics
3.4. Outcomes
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pimple, S.; Mishra, G. Cancer cervix: Epidemiology and disease burden. Cytojournal 2022, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Ismail, A.; Pappas-Gogos, G.; Boussios, S. HPV and Cervical Cancer: A Review of Epidemiology and Screening Uptake in the UK. Pathogens 2023, 12, 298. [Google Scholar] [CrossRef]
- Chan, C.K.; Aimagambetova, G.; Ukybassova, T.; Kongrtay, K.; Azizan, A. Human Papillomavirus Infection and Cervical Cancer: Epidemiology, Screening, and Vaccination-Review of Current Perspectives. J. Oncol. 2019, 2019, 3257939. [Google Scholar] [CrossRef]
- Khan, I.; Harshithkumar, R.; More, A.; Mukherjee, A. Human Papilloma Virus: An Unraveled Enigma of Universal Burden of Malignancies. Pathogens 2023, 12, 564. [Google Scholar] [CrossRef] [PubMed]
- Dorji, T.; Nopsopon, T.; Tamang, S.T.; Pongpirul, K. Human papillomavirus vaccination uptake in low-and middle-income countries: A meta-analysis. EclinicalMedicine. 2021, 34, 100836. [Google Scholar] [CrossRef]
- Zhang, S.; Xu, H.; Zhang, L.; Qiao, Y. Cervical cancer: Epidemiology, risk factors and screening. Chin. J. Cancer Res. 2020, 32, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Koyama, T.; Otsuka, F. Impact of the cervical cancer awareness months on public interest in Japan: A Google Trends analysis, 2012–2021. Sci. Rep. 2022, 12, 15391. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Kong, W.; Zhao, X.; Zhang, H.; Luo, D.; Chen, S. Immune checkpoint inhibitors in cervical cancer: Current status and research progress. Front. Oncol. 2022, 12, 984896. [Google Scholar] [CrossRef] [PubMed]
- Watkins, D.E.; Craig, D.J.; Vellani, S.D.; Hegazi, A.; Fredrickson, K.J.; Walter, A.; Stanbery, L.; Nemunaitis, J. Advances in Targeted Therapy for the Treatment of Cervical Cancer. J. Clin. Med. 2023, 12, 5992. [Google Scholar] [CrossRef]
- Duranti, S.; Pietragalla, A.; Daniele, G.; Nero, C.; Ciccarone, F.; Scambia, G.; Lorusso, D. Role of Immune Checkpoint Inhibitors in Cervical Cancer: From Preclinical to Clinical Data. Cancers 2021, 13, 2089. [Google Scholar] [CrossRef]
- Rajan, A.; Kim, C.; Heery, C.R.; Guha, U.; Gulley, J.L. Nivolumab, anti-programmed death-1 (PD-1) monoclonal antibody immunotherapy: Role in advanced cancers. Hum. Vaccin. Immunother. 2016, 12, 2219–2231. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zhang, H.; Chen, B. Nivolumab as Programmed Death-1 (PD-1) Inhibitor for Targeted Immunotherapy in Tumor. J. Cancer. 2017, 8, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Baxevanis, C.N. Immune Checkpoint Inhibitors in Cancer Therapy-How Can We Improve Clinical Benefits? Cancers 2023, 15, 881. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Day, D.; Nicholls, S.J.; Segelov, E. Immune Checkpoint Inhibitor Therapy in Oncology: Current Uses and Future Directions: JACC: CardioOncology State-of-the-Art Review. JACC Cardio Oncol. 2022, 4, 579–597. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhang, Z.; Zheng, X.; Tao, H.; Zhang, S.; Ma, J.; Liu, Z.; Wang, J.; Qian, Y.; Cui, P.; et al. Response Efficacy of PD-1 and PD-L1 Inhibitors in Clinical Trials: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 562315. [Google Scholar] [CrossRef] [PubMed]
- Mamat Yusof, M.N.; Chew, K.T.; Kampan, N.C.; Shafiee, M.N. Expression of PD-1 and PD-L1 in Endometrial Cancer: Molecular and Clinical Significance. Int. J. Mol. Sci. 2023, 24, 15233. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Fowler, J.R.; Maani, E.V.; Dunton, C.J.; Gasalberti, D.P.; Jack, B.W. Cervical Cancer. In StatPearls; Updated 12 November 2023; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK431093/ (accessed on 15 February 2024).
- Chen, R.Y.; Zhu, Y.; Shen, Y.Y.; Xu, Q.Y.; Tang, H.Y.; Cui, N.X.; Jiang, L.; Dai, X.M.; Chen, W.Q.; Lin, Q.; et al. The role of PD-1 signaling in health and immune-related diseases. Front. Immunol. 2023, 14, 1163633. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Tamura, K.; Hasegawa, K.; Katsumata, N.; Matsumoto, K.; Mukai, H.; Takahashi, S.; Nomura, H.; Minami, H. Efficacy and safety of nivolumab in Japanese patients with uterine cervical cancer, uterine corpus cancer, or soft tissue sarcoma: Multicenter, open-label phase 2 trial. Cancer Sci. 2019, 110, 2894–2904. [Google Scholar] [CrossRef]
- Naumann, R.W.; Hollebecque, A.; Meyer, T.; Devlin, M.J.; Oaknin, A.; Kerger, J.; López-Picazo, J.M.; Machiels, J.P.; Delord, J.P.; Evans, T.R.; et al. Safety and Efficacy of Nivolumab Monotherapy in Recurrent or Metastatic Cervical, Vaginal, or Vulvar Carcinoma: Results from the Phase I/II CheckMate 358 Trial. J. Clin. Oncol. 2019, 37, 2825–2834. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Deng, W.; Frumovitz, M.; Buza, N.; Bellone, S.; Huh, W.; Khleif, S.; Lankes, H.A.; Ratner, E.S.; O’Cearbhaill, R.E.; et al. Phase II evaluation of nivolumab in the treatment of persistent or recurrent cervical cancer (NCT02257528/NRG-GY002). Gynecol. Oncol. 2020, 157, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Vanoni, G.; Loap, P.; Dubot, C.; Timperi, E.; Minsat, M.; Bazire, L.; Durdux, C.; Fourchotte, V.; Laas, E.; et al. Nivolumab plus chemoradiotherapy in locally-advanced cervical cancer: The NICOL phase 1 trial. Nat. Commun. 2023, 14, 3698. [Google Scholar] [CrossRef] [PubMed]
- Shieh, K.R.; Huang, A.; Xu, Y. Response to Immune Checkpoint Inhibitor Treatment in Advanced Cervical Cancer and Biomarker Study. Front. Med. 2021, 8, 669587. [Google Scholar] [CrossRef] [PubMed]
- Baettig, F.; Vlajnic, T.; Vetter, M.; Glatz, K.; Hench, J.; Frank, S.; Bihl, M.; Lopez, R.; Dobbie, M.; Heinzelmann-Schwarz, V.; et al. Nivolumab in chemotherapy-resistant cervical cancer: Report of a vulvitis as a novel immune-related adverse event and molecular analysis of a persistent complete response. J. Immunother. Cancer 2019, 7, 281. [Google Scholar] [CrossRef] [PubMed]
- Devabhaktuni, S.; Singh, A.; Georgy, J.T.; Antonisamy, J.; Thumaty, D.B.; John, A.O. Efficacy of low dose nivolumab in recurrent/metastatic cervical cancer. Ann. Oncol. 2023, 34 (Suppl. S4), S1585. [Google Scholar] [CrossRef]
- Naumann, R.W.; Oaknin, A.; Meyer, T.; Lopez-Picazo, J.M.; Lao, C.; Bang, Y.J.; Boni, V.; Sharfman, W.H.; Park, J.C.; Devriese, L.A.; et al. Efficacy and safety of nivolumab (Nivo) + ipilimumab (Ipi) in patients (pts) with recurrent/metastatic (R/M) cervical cancer: Results from CheckMate 358. Ann. Oncol. 2019, 30, v898–v899. [Google Scholar] [CrossRef]
- Nakamura, K.; Yabuno, A.; Satoh, T.; Fujiwara, H.; Kurosaki, A.; Yamashita, S.; Misumi, T.; Noda, S.E.; Hasegawa, K. Efficacy and final safety analysis of pre- and co-administration of nivolumab (Nivo) with concurrent chemoradiation (CCRT) followed by Nivo maintenance therapy in patients (pts) with locally advanced cervical carcinoma (LACvCa): Results from the phase I trial, GOTIC-018. J. Clin. Oncol. 2023, 41, 5519. [Google Scholar] [CrossRef]
- Oaknin, A.; Moore, K.N.; Meyer, T.; González, J.L.; Devriese, L.; Amin, A.; Lao, C.D.; Boni, V.; Sharfman, W.H.; Park, J.C.; et al. Safety and efficacy of nivolumab (NIVO) ± ipilimumab (IPI) in patients (pts) with recurrent/metastatic cervical cancer (R/M Cx Ca) in checkmate 358. Ann. Oncol. 2022, 33 (Suppl. S7), S782. [Google Scholar] [CrossRef]
- Massarelli, E.; William, W.; Johnson, F.; Kies, M.; Ferrarotto, R.; Guo, M.; Feng, L.; Lee, J.J.; Tran, H.; Kim, Y.U.; et al. Combining Immune Checkpoint Blockade and Tumor-Specific Vaccine for Patients with Incurable Human Papillomavirus 16-Related Cancer: A Phase 2 Clinical Trial. JAMA Oncol. 2019, 5, 67–73. [Google Scholar] [CrossRef]
- Pouyiourou, M.; Kraft, B.N.; Wohlfromm, T.; Stahl, M.; Kubuschok, B.; Löffler, H.; Hacker, U.T.; Hübner, G.; Weiss, L.; Bitzer, M.; et al. Nivolumab and ipilimumab in recurrent or refractory cancer of unknown primary: A phase II trial. Nat. Commun. 2023, 14, 6761. [Google Scholar] [CrossRef]
- Wolf, J.; Xu, Y. Immune checkpoint inhibitor therapy in advanced cervical cancer: Deepened response with prolonged treatment and repeat response to re-initiation of therapy. Gynecol. Oncol. Rep. 2023, 48, 101244. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Xiong, H.; Yang, M.; Li, L.; Wu, P.; Lazare, C.; Cao, C.; Gao, P.; Meng, Y.; Zhi, W.; et al. Co-infections of HPV16/18 with other high-risk HPV types and the risk of cervical carcinogenesis: A large population-based study. Gynecol. Oncol. 2019, 155, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Senapati, R.; Nayak, B.; Kar, S.K.; Dwibedi, B. HPV genotypes co-infections associated with cervical carcinoma: Special focus on phylogenetically related and non-vaccine targeted genotypes. PLoS ONE 2017, 12, e0187844. [Google Scholar] [CrossRef] [PubMed]
- Sugarman, R.; Betts, K.A.; Nie, X.; Hartman, J.; Nguyen, H. Nivolumab Plus Chemotherapy for Advanced Gastric, Gastroesophageal Junction, and Esophageal Adenocarcinoma: Analysis of Number Needed to Treat and Number Needed To Harm. Clin. Ther. 2023, 45, 1155–1158. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.W.; Battista, M.J.; Schmidt, M.; Garcia, M.; Siepmann, T.; Hasenburg, A.; Anic, K. Efficacy and Safety of Immunotherapy for Cervical Cancer-A Systematic Review of Clinical Trials. Cancers 2022, 14, 441. [Google Scholar] [CrossRef] [PubMed]
- Arak, H.; Aytekin, A.; Canoz, O.; Ozkan, M. Prognostic and Predictive Significance of PD-L1 Expression in Non-Small Cell Lung Cancer Patients: A Single-Center Experience. Turk. J. Pathol. 2021, 37, 239–248. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study and Author | Country | Study Year | Study Design | Study Quality |
|---|---|---|---|---|
| 1 [21] Tamura et al. | Japan | 2019 | RCT (phase II) | High |
| 2 [22] Naumann et al. | United States | 2019 | RCT (phase I/II) | High |
| 3 [23] Santin et al. | United States | 2019 | RCT (phase II) | High |
| 4 [24] Rodrigues et al. | France | 2023 | RCT (phase I) | High |
| Study Number | Sample Size | Age (Years) | Comparison Group | Performance Status |
|---|---|---|---|---|
| 1 [21] Tamura et al. | 20 | Median: 50 Range: 32–68 | PD-L1 positive vs. PD-L1 negative | ECOG 0: 75% ECOG 1: 25% |
| 2 [22] Naumann et al. | 19 | Median: 51 Range: 28–75 | Cervical cancer vs. Vaginal-vulvar cancer | ECOG 0: 52.6% ECOG 1: 42.1% |
| 3 [23] Santin et al. | 25 | Median: 45 | NR | ECOG 0: 64% ECOG 1: 36% |
| 4 [24] Rodrigues et al. | 16 | Mean: 47.9 Range: 27–77 | NR | ECOG 0: 50% ECOG 1: 50% |
| Study Number | Stage | Histology | Metastases | HPV/PD-L Status | Prior Treatment |
|---|---|---|---|---|---|
| 1 [21] Tamura et al. | III: 5% IV: 35% Recurrent: 60% | SCC: 70% ACC: 25% ASC: 5% | <2: 45% 2: 35% >2: 20% | HPV 16–18 positive: 45% PD-L1 positive: 75% | Radiotherapy: 85% Chemotherapy: 100% |
| 2 [22] Naumann et al. | IIB: 5.3% IIIB–IIIC: 10.5% IVA–IVB: 84.2% | SCC: 100% | Lymph nodes: 63.2% Lungs: 42.1% Pelvis: 26.3% Uterus: 15.8% Peritoneum: 10.5% Bones: 10.5% | HPV 6,11,16,18,33 positive: 83.3% PD-L1 positive: 62.5% | Radiotherapy: 89.5% Chemotherapy: 100% |
| 3 [23] Santin et al. | I–II: 60% III: 20% IV: 20% | SCC: 60% ACC: 24% ASC: 16% | 28% of patients | PD-L1 positive: 77.3% | Radiotherapy: 92% Immunotherapy: 8% Surgery: 68% |
| 4 [24] Rodrigues et al. | I–II: 62.5% III: 31.3% IV: 6.2% | SCC: 87.5% ACC: 12.5% | 0% | HPV 16–18 positive: 64% | Concomitant chemotherapy: 100% Radiotherapy: 100% Brachytherapy: 100% |
| Risk Factors | Treatment/Dose | Follow-Up | Survival | Conclusions |
|---|---|---|---|---|
| 1 [21] Tamura et al. | 240 mg at 2-week intervals Median duration of treatment: 5.4 months | ORR: 25% PD-L1(+) vs. 0% PD-L1(−) DCR: 75% Median follow-up time: 8.6 months | 6-month PFS: 86% PD-L1(+) vs. 80% PD-L1(−) Median PFS: 5.5 months PD-L1(+) vs. 6.2 months | Nivolumab showed acceptable toxicity in all cohorts, with evidence of clinical activity in advanced cervical cancer. |
| 2 [22] Naumann et al. | 240 mg at 2-week intervals Median duration of treatment: 5.6 months | ORR: 26.3% DCR: 68.4% Complete response: 15.8% Median follow-up time: 19.2 months | Median OS: 21.9 months 12-month PFS: 26.3% Median PFS: 5.1 months | Nivolumab proved a good safety record and efficacy in advanced cervical cancer. |
| 3 [23] Santin et al. | Four doses of IV nivolumab (3 mg/kg every 2 weeks), followed by an additional 42 doses of 3 mg/kg every 2 weeks for a maximum of 46 doses | Median ORR: 5.7 months ORR: 36% Adverse events: 84% | Median OS: 14.5 months Median PFS: 3.5 months 6-month PFS: 16% 6-month OS: 78.4% | Nivolumab proved a good safety record besides the number of adverse events. Low antitumor activity as monotherapy. |
| 4 [24] Rodrigues et al. | 240 mg at 2-week intervals | ORR: 93.8% Median follow-up time: 23.8 months Dose-limiting adverse events: 20% | 2-years PFS: 75% Median PFS: has not been reached | Nivolumab associated with concomitant chemoradiotherapy is safe and shows promising PFS. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petre, I.; Vernic, C.; Petre, I.; Vlad, C.S.; Sipos, S.I.; Bordianu, A.; Luciana, M.; Dragomir, R.D.; Fizedean, C.M.; Daliborca, C.V. Systematic Review on the Effectiveness and Outcomes of Nivolumab Treatment Schemes in Advanced and Metastatic Cervical Cancer. Diseases 2024, 12, 77. https://doi.org/10.3390/diseases12040077
Petre I, Vernic C, Petre I, Vlad CS, Sipos SI, Bordianu A, Luciana M, Dragomir RD, Fizedean CM, Daliborca CV. Systematic Review on the Effectiveness and Outcomes of Nivolumab Treatment Schemes in Advanced and Metastatic Cervical Cancer. Diseases. 2024; 12(4):77. https://doi.org/10.3390/diseases12040077
Chicago/Turabian StylePetre, Ion, Corina Vernic, Izabella Petre, Cristian Sebastian Vlad, Simona Ioana Sipos, Anca Bordianu, Marc Luciana, Radu Dumitru Dragomir, Camelia Melania Fizedean, and Cristina Vlad Daliborca. 2024. "Systematic Review on the Effectiveness and Outcomes of Nivolumab Treatment Schemes in Advanced and Metastatic Cervical Cancer" Diseases 12, no. 4: 77. https://doi.org/10.3390/diseases12040077
APA StylePetre, I., Vernic, C., Petre, I., Vlad, C. S., Sipos, S. I., Bordianu, A., Luciana, M., Dragomir, R. D., Fizedean, C. M., & Daliborca, C. V. (2024). Systematic Review on the Effectiveness and Outcomes of Nivolumab Treatment Schemes in Advanced and Metastatic Cervical Cancer. Diseases, 12(4), 77. https://doi.org/10.3390/diseases12040077