Abstract
One of the most common causes of maternal death during pregnancy is preeclampsia. A deeper understanding of the patient’s features can aid in the hospital’s clinical care distribution. However, at the IESS Los Ceibos Hospital, these types of studies have not been carried out for preeclampsia. Therefore, in this work, we describe the application of descriptive and clustering analysis to characterize preeclamptic patients. Preeclamptic patients treated at the IESS Los Ceibos Hospital in Guayaquil comprised the dataset used in this study. Descriptive and clustering analysis allowed us to find that severe preeclampsia (O141) is the most common diagnosis when preeclamptic patients arrive at the hospitalization unit, representing 79.5% of the cases. Moreover, women whose maternal age falls between 26 and 35 years have the highest prevalence of preeclampsia, representing 55.4% of the cases. Finally, adult patients in their late 30s or older are often diagnosed with severe preeclampsia (O141) and often require many hours of hospital care during the first two visits. These findings will help to generate care and prevention policies, such as the use of a low dose of aspirin, in these age groups to avoid the complications that preeclampsia can cause.
1. Introduction
Preeclampsia, a pregnancy-related condition caused by the placenta, currently accounts for 10–15% of all maternal deaths globally [1,2]. Preeclampsia is a progressive multisystem illness that usually develops in women with a previously normal blood pressure after 20 weeks of gestation or postpartum [3]. It is typified by the beginning of newly formed arterial hypertension, which may also involve proteinuria and the malfunction of several organs, including the liver, as well as hematopoietic abnormalities and changes in biochemical indicators of coagulation. Additionally, neurological issues or signs of uteroplacental dysfunction, such as fetal growth restriction [4], may accompany it.
As per the Ministry of Public Health’s 2020 report, the primary cause of maternal death in Guayas Province, Ecuador, is a hypertensive condition resulting from severe preeclampsia [5]. Therefore, maternal and perinatal outcomes can be significantly improved through the timely treatment of this disease [6,7,8]. Machine learning (ML) methods such as clustering analysis can be helpful in identifying and describing groups that differ from one another while sharing similarities [9,10]. In our situation, this method can be helpful in characterizing patients and providing the IESS Los Ceibos Hospital with pertinent data that will enable its personnel to more effectively organize medical facilities where preeclamptic patients are treated.
This manuscript is an extension of our previous work presented in [2]. In particular, we extend the application of descriptive analysis to characterize preeclampsia patients, in addition to contrasting the findings those of various studies of this disease within the Ecuadorian context. It is important to perform this analysis to understand, in the context of the IESS Los Ceibos Hospital, the age, demographic, and diagnostic profile of the patients in order to provide the majority group with preventive treatment, such as low doses of aspirin, a treatment that has been recommended by [11].
The following is the structure of the remainder of the paper. Previous studies that are pertinent to this inquiry are given in Section 2. A brief synopsis of this work’s approach is provided in Section 3. Section 4 presents a full description of the findings. Finally, Section 5 includes the closing remarks.
2. Related Work
Our study focuses on the characterization of preeclampsia patients that attended the IESS Los Ceibos Hospital in Guayaquil, Ecuador. Therefore, in this section, we will review those works that have used descriptive analysis to study preeclampsia in the Ecuadorian context, pointing out in italics their most relevant conclusions. After this, we will review studies from other countries to identify the maternal age with the highest incidence of preeclampsia.
In addition, we will review the use of clustering techniques, which are considered in various studies when grouping patients with similar characteristics, as we wish to do in our study to prepare the necessary medical resources according to the characteristics of each group.
2.1. Descriptive Analysis for the Study of Preeclampsia in the Ecuadorian Context
A cross-sectional study was conducted in [7] to find correlations between prenatal control and the preeclampsia incidence in pregnant women in Ecuador. Since diagnosing and preventing pregnancy difficulties like preeclampsia is one of the key goals of prenatal care, descriptive analysis assisted them in reaching the conclusion that adequate prenatal care (more than five visits beginning in the first trimester of pregnancy) has an impact on the prevention of pregnancy complications like preeclampsia.
In [12], medical records from the gyneco-obstetrics service at the emergency room of the Hospital Sagrado Corazón de Jesús, in the city of Quevedo in the province of Los Ríos, Ecuador, were used to conduct a descriptive, retrospective, correlational study with the goal of describing hypertensive disorders and their most common complications that occur during adolescent pregnancy, focusing on the period between March and August 2016. They reached the conclusion that, in 41% of the cases, the group aged 17 years old was the most likely to suffer from pregnancy-induced hypertension (PIH). Furthermore, it was determined that 7% of the cases were hospitalized due to gestational diabetes, and 92% of the cases examined had preeclampsia in one of its several forms.
A population-based study of preeclampsia and eclampsia in Ecuador was conducted in [13], taking into account variations in altitude, geography, and ethnicity. They were able to determine, through descriptive analysis, that eclampsia is primarily found at lower altitudes, whereas preeclampsia is common in both low- and high-altitude regions. The ethnic group with a higher risk of preeclampsia is represented by Montubios, who reside at middle or high altitudes. Conversely, ethnicity was not found to be a possible eclampsia risk factor. Furthermore, eclampsia appears to carry a larger risk for young women than preeclampsia.
In [14], a descriptive study was conducted on the relationship between pathological Doppler flowmetry and the prediction of preeclampsia. The study concluded that the use of Doppler in this investigation did not demonstrate predictive value in the screening of preeclampsia. Despite this, the descriptive analysis allowed them to conclude that the diagnosis of preeclampsia was predominant between the ages of 20 and 34 years, with 27.2 years being the average age.
In summary, descriptive studies have allowed us to conclude that
- Adequate prenatal care has an impact on the prevention of pregnancy complications like preeclampsia [7];
- The age at which the diagnosis of preeclampsia predominates is not entirely clear—while, in [12], this age is 17 years old, in [14], preeclampsia is predominant between the ages of 20 and 34 years;
- Montubios who live at middle or high altitudes may be the ethnic group that is most at risk for preeclampsia [13];
- Eclampsia appears to carry a larger risk for young women than preeclampsia [13].
Our descriptive analysis will try to verify whether these conclusions apply to our study population.
2.2. Maternal Age and Incidence of Preeclampsia Around the World
Below, we will review various studies carried out in different parts of the world, with the aim of determining the maternal age at which there is the highest incidence of preeclampsia.
- In [15], the authors applied descriptive analytics to study the preeclampsia prevalence in a Malaysian referral maternity hospital and the association between preeclampsia and maternal characteristics and outcomes. In it, an association was seen between chronic hypertension and advanced maternal age (≥35 years old) regarding preeclampsia.
- In [16], the authors studied the relationship between age and the incidence of preeclampsia at Dustira Hospital in Cimahi City, Indonesia. They found that mothers with an age <20 years or >35 years had a seven times greater risk of experiencing preeclampsia compared to mothers aged between 20 and 35 years.
- In [17], a study was carried out at healthcare units in the Multan district, Pakistan, and involved patients with gestational hypertension. The authors found that the majority of preeclamptic patients were less than 24 years of age (33.3%), belonged to lower socioeconomic classes (44.4%), and had low educational levels (81.1%).
- In [18], the authors studied differences in the epidemiology of patients with preeclampsia between China and the US. They found that, in China and the US, the risk of preeclampsia rises in an exponential manner with maternal age, particularly in females above the age of 40 years.
- In [19], the authors examined the risk factors and fetal outcomes for preeclampsia in a Colombian cohort. They found that a high incidence of preeclampsia occurs when the maternal age is less than 20 or greater than 35 years.
In summary, various studies carried out in different regions of the world have found that there is a high incidence of preeclampsia when the mother’s age is below 20 years or above 35 years. This finding will be taken into account when considering whether the same situation also occurs in patients treated at the IESS Los Ceibos Hospital in Guayaquil.
2.3. Clustering Analysis in the Pregnancy Context
De La Cruz Gutiérrez et al. [20] characterized the causes of maternal morbidity in a cohort of 1686 expecting mothers from the San Bartolomé Hospital in Lima using the k-Means technique for unsupervised learning, with K equal to 10. This clustering technique made it possible to identify and examine common characteristics that raise the risk of maternal morbidity. In fact, they found that four of the groups had the most common characteristics that may present a picture of maternal morbidity. Moreover, cluster 5 presented the most significant and common characteristics constituting a picture of maternal morbidity, representing 1.1% of the total population and 13.4% of the population studied (n = 138). In conclusion, they found that, in the San Bartolomé Hospital, there was a high tendency for morbidity in pregnant mothers who presented the following characteristics: ruptured membranes, no hemorrhage, no tears, incomplete abortions, no infection during pregnancy, an unknown last menstrual period, and no pregnancies greater than zero.
Moreover, in [21], the researchers examined the relationship between prenatal antidepressant exposure patterns and the risk of preeclampsia and postpartum hemorrhage. These scientists used longitudinal k-Means to find women who, throughout the first 20 and 35 weeks of their pregnancy, had comparable antidepressant exposure patterns or trajectory groups. Their findings indicated that women who took antidepressants for an extended period of time, particularly at higher doses, had a higher risk of preeclampsia and PPH; however, the increased risk may also be attributed to underlying sadness and anxiety.
In addition, a clustering strategy was examined by Pereira et al. [22] to categorize the reasons for which pregnant women visited the Porto Hospital Center for Obstetrics. They also suggested using k-Means, EM, and Farthefirst to segment patients based on their attributes. In their paper, the optimal model for the identification of the features of the patients receiving this type of care was found to be a four-cluster k-Means model.
Furthermore, using longitudinal k-Means clustering, the authors of [23] created blood pressure trajectory clusters and looked at birth outcomes, early pregnancy factors, and demographics in connection to these clusters. According to their findings, the prepregnancy BMI, parity, and maternal age varied significantly between the blood pressure clusters of patients. Moreover, both those with a higher initial blood pressure and those with a more rapid rise in blood pressure had significantly worse pregnancy outcomes, including preterm births, small infacts for their gestational age, and lower birthweight Z scores.
To summarize, the previously stated studies employed distinct datasets and utilized the k-Means and EM algorithms to characterize expectant patients. It is for this reason that we shall group the preeclamptic patients treated at the IESS Los Ceibos Hospital in Guayaquil using the clustering approach.
3. Methodology
Figure 1 shows a summary of the aspects that will be reviewed in this section regarding the descriptive and clustering analysis to characterize preeclampsia patients. In the following paragraphs, we offer a more extensive description of them.

Figure 1.
Summary of the aspects that will be reviewed in this study.
3.1. Descriptive Analysis
A descriptive statistical analysis aids in describing the essential components of a data collection to offer a succinct explanation of it. Descriptive statistics, in general, aim to provide an easy-to-read summary of the evidence—that is, the observations derived from variables—so that it may be interpreted with clarity.
Descriptive analysis can be carried out when using summary statistics like measurements of dispersion (standard deviation, range) and measures of the central tendency (mean, median, mode), in addition to visual techniques like barplots, boxplots and line graphs. These will be considered in this work to study the demographic, age and diagnostic characteristics of preeclampsia patients, alongside a discussion of the observed results and contrasting them with the findings of other works on this subject.
3.2. Clustering Analysis
As reviewed in the previous section, k-Means is a widely used method for clustering tasks. However, because the k-Means method can be affected by outliers, in this work, we will use the Partitioning Around Medoids (PAM) method to perform the clustering task.
It is important to note that, because our dataset contains both nominal and continuous variables, a better alternative for the transformation of nominal variables into binary numerical attributes is the use of Gower’s distance instead of the Euclidean distance. For this reason, we will consider Gower’s distance to measure the distances between the elements of each cluster.
Moreover, we will consider the silhouette coefficient to measure the clustering quality, performing the analysis of the best number of clusters under the silhouette metric (those that achieve the highest silhouette coefficient).
4. Results and Discussion
4.1. Collecting Data
From the medical records of patients treated in the gynecological unit of the IESS Los Ceibos Hospital in Guayaquil, Ecuador, retrospective medical data were gathered. Informed permission was not required because the study was retrospective, non-interventional, and used deidentified data.
Since May 2017 marked the opening of the IESS Los Ceibos Hospital, data were gathered from this point until December 2023. In total, 11,497 records were retrieved from this hospital. To carry out the descriptive analysis of the characteristics of the patients treated for preeclampsia, we did not consider those records that referred to the same patient but to different dates of hospitalization, leaving a total of 6406 EMRs.
The following factors were included in the collection of medical features: age group, nationality, province, canton, diagnosis type, diagnosis type, type of care, specialty, date of medical care, time, and dependency. It was not possible to collect all data for every patient in a systematic manner because this was a retrospective study. However, unlike the province data, the diagnosis and age data were collected for all 6406 EMRs, enabling us to carry out a descriptive analysis on them.
Furthermore, we discovered that many date formats were supported by the “date of medical care” attribute. It was therefore required to process them in order to bring them together. Lastly, the records were numbered and sorted by month and year in order to obtain a time series.
4.2. Demographic Characteristics
Table 1 and Table 2 show the nationalities and provinces of the patients. Below, we present the distribution of the patients by nationality.

Table 1.
Nationality frequency in descending order.
Table 2.
Province frequency in descending order.
In Table 1, we see that the majority of the patients were of Ecuadorian nationality. However, it is important to note that, despite the sharp increase in Venezuelan citizens in the city of Guayaquil, we only found one case of a patient with preeclampsia who was treated during the study period. One possible explanation is that many of these citizens do not enjoy social security (IESS) affiliation, being treated by units attached to the Ministry of Public Health and not by those of the IESS. The same explanation can be given for other nationalities, such as those from Switzerland, Andorra or Laos.
Below, we present the distribution of the patients by province of residence. It is important to mention that any non-Ecuadorian citizen residing in any province of Ecuador is taken into account in the following table.
Only 6391 patient records had provincial data. In Table 2, only these EMRs are taken into account. Here, we see that the majority of the patients resided in the province of Guayas. Patients residing in provinces close to Guayas, such as Manabí, Los Ríos, El Oro and Santa Elena, also had good representation. A single case was observed in the province of Pichincha. However, a possible explanation is that Quito is a city in this province, and there is significant flow between Quito and Guayaquil for economic, work, tourism and other reasons. Provinces such as Cañar, Imbabura or Zamora Chinchipe are shown as places of residence for a few patients. This is due to the distance of these places from the province of Guayas, in addition to the lack of commercial exchange with these places.
4.3. Age Characteristics
Figure 2 shows the age distribution of the patients with preeclampsia. We can observe that the minimum and maximum values are 14 and 49 years, respectively, while the values of the first, second, and third quartiles are 26, 30, and 35, respectively. Moreover, we have two atypical data within the records (47 and 49 years); these values are far from the edge of the box and at least 1.5 times the interquartile range (Q3–Q1).

Figure 2.
Boxplot of the ages of patients with preeclampsia when ordered by age.
Table 3 shows the age distribution of the patients. A few examples of preeclampsia in teenagers are shown; these cases fall into the first quartile of the distribution of preeclampsia hospitalizations when ordered by age. Obviously, adolescent patients may not have social security (IESS) affiliation because they do not officially work as they are minors. Even so, they can access services when one or both parents are affiliated with the IESS. However, if neither of their parents is affiliated, they are not able to access care at the study hospital.
Table 3.
Age and frequency (Freq.) in descending order.
As illustrated in Figure 3, cases of preeclampsia presented in adolescents (up to 19 years old) comprised only 3.5% of the cases treated, according to our data collection. However, this only includes preeclampsia patients who received care in the IESS hospitalization unit. In a future study, it could be worthwhile to examine the incidence of preeclampsia cases concerning the number of pregnancies by age so as to determine the proportion of instances at each age.
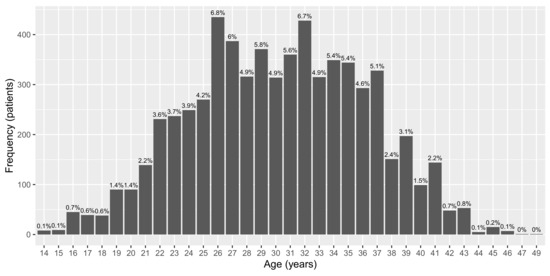
Figure 3.
Number of preeclamptic patients by age.
Finally, according to Figure 3, the highest incidence of preeclampsia occurred within the interquartile range, which comprised women whose maternal age was between 26 and 35 years, similar to the predominant age range presented in [14]. Moreover, unlike the global trend [15,16,17,18,19], in our local context, there was not a high incidence of preeclampsia in women over 35 years of age, but there was a high incidence in women between 26 and 35 years of age. This may be due to the young age at motherhood among women in Ecuador, a factor that causes the incidence of pregnancy to decrease in women over 35 years of age. A study on the number of pregnancies and the incidence of preeclampsia in women over 35 years of age is left for future work.
4.4. Diagnostic Characteristics
Figure 4 shows a bar diagram with the frequency of diagnosis among the preeclamptic patients who arrived at the hospitalization unit. The prefix O is used to indicate diagnostic labels (X-axis), which are related to the ICD10 codes, the definitions of which are given below.

Figure 4.
Bar diagram of the diagnosis of preeclampsia patients treated in the hospitalization unit.
- O140: Moderate Preeclampsia;
- O141: Severe Preeclampsia;
- O149: Preeclampsia, unspecified.
Severe preeclampsia (O141), accounting for 79.5% of the diagnoses, is the most common diagnosis among patients with preeclampsia who present to the hospitalization unit. Because it affects the mother during pregnancy and delivery and causes endothelial dysfunction in multiple organs after birth, increasing the risk of cardiovascular disease and other consequences [24], it is an obstetric emergency that needs to be quickly and appropriately identified and treated. Figure 5 illustrates the incidence of cases with severe preeclampsia (O141).
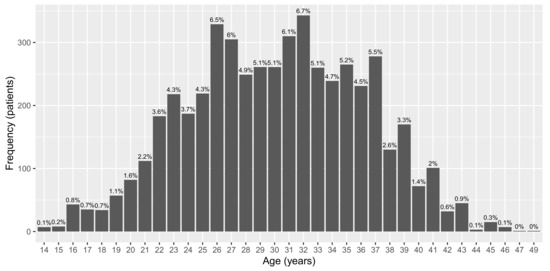
Figure 5.
Frequencies of inpatients with severe preeclampsia by age.
Figure 5 shows that the majority of cases fall within the interquartile range of ages (26 to 35 years), accounting for 55.4% of the cases. The authors of [12,25] concluded that a higher risk of developing severe preeclampsia is linked to a younger age. Nevertheless, our data collection indicates that instances of preeclampsia presented by teenagers (up to 19 years old) constituted only 3.6% of the cases treated, as shown in Figure 5. It is crucial to remember that, as previously stated, our findings only apply to patients with severe preeclampsia who sought care in the hospitalization unit. To determine the percentage of cases at each age, additional prospective studies might look at the incidence of severe preeclampsia concerning the number of pregnancies by age.
4.5. Clustering Analysis
Figure 6 presents the values of the silhouette coefficient obtained by considering two, three, four and five clusters using the PAM method. It can be seen that the highest value is obtained when the number of clusters is four. Therefore, we will consider this parameter (k = 4) to group patients with preeclampsia.
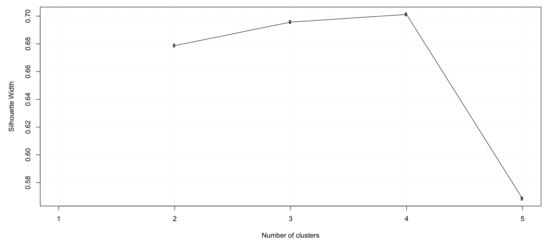
Figure 6.
Silohuette coefficient obtained by considering 2, 3, 4 and 5 clusters using the PAM method.
Table 4 presents the means and modes of each attribute considered for clustering with PAM and k = 4. In it, we can see the following:
Table 4.
Cluster means and modes of every attribute.
- In cluster 1, young patients are grouped and are usually diagnosed with moderate preeclampsia (O140), not requiring much care time during hospital visits;
- Cluster 2 includes adult patients who are approaching 40 years of age and who are usually diagnosed with severe preeclampsia (O141), whose care time at the first hospital visit is usually extensive, reaching an average of 113.49 h;
- Cluster 3 describes those patients who are around 25 years old and who are diagnosed with severe preeclampsia (O141), although it is not until the fourth hospital visit that they require more care and attention;
- Finally, cluster 4 includes patients around 30 years of age, diagnosed with severe preeclampsia (O141) and requiring many hours of hospital care at the second visit (mean of 110.91 h).
Overall, we can conclude that adult patients close to or older than 30 years of age are usually diagnosed with severe preeclampsia (O141) and tend to require many hours of hospital care in the first two visits. On the other hand, younger patients diagnosed with preeclampsia usually require many hours of hospital care at the fourth hospital visit.
4.6. Summary of the Findings
In summary, we can point the following findings.
- The first, second, and third quartiles have values of 26, 30, and 35, respectively, whereas the minimum and maximum values are 14 and 49 years, respectively.
- We have two atypical cases within the preeclampsia records (47 and 49 years).
- When patients with preeclampsia present to the hospitalization unit, the most common diagnosis is severe preeclampsia (O141), which accounts for 79.5% of the diagnoses.
- Contrary to the studies presented in [12,25], only a few cases of preeclampsia are presented in teenagers.
- Rather, women whose maternal age falls between 26 and 35 years have the highest prevalence of preeclampsia, which is similar to the main age range reported in [14].
- Adult patients in their late 30s or older are often diagnosed with severe preeclampsia (O141) and often require many hours of hospital care during the first two visits.
4.7. Recommended Actions to Prevent Complications from Preeclampsia
Actions have been recommended worldwide to prevent the development of complications from preeclampsia. For example, in the study presented in [11], the use of low-dose aspirin (81 mg/d) as a preventive medication for preeclampsia after 12 weeks of gestation is highly recommended in persons who are at a high risk for preeclampsia. This measure is also recommended by other studies [26,27,28]. In our case, due to the high incidence of preeclampsia, this measure could be applied to pregnant patients whose age ranges between 26 and 35 years.
Furthermore, according to [29], low-molecular-weight heparin, enoxaparin, PETN, yoga, L-arginine, folic acid, and vitamin D alone or combined with calcium can be used as cost-effective, available, and acceptable measures to prevent preeclampsia. However, given the cost and the diversity of studies supporting its use, we recommend the use of aspirin to prevent health complications from preeclampsia.
5. Conclusions and Future Work
5.1. Conclusions
Since preeclampsia is one of the most common causes of maternal death during pregnancy, this work applied descriptive and cluster analyses to characterize patients with preeclampsia treated at the IESS Los Ceibos Hospital in Guayaquil. This work was motivated by the fact that deeper knowledge of these patients’ characteristics could help in the distribution of clinical care at the hospital.
Based on the descriptive analysis, we discovered that 79.5% of the patients with preeclampsia who arrive at the hospitalization unit have severe preeclampsia (O141), which is the most common diagnosis. Furthermore, preeclampsia is most common in women whose maternal age falls between 26 and 35 years old, accounting for 55.4% of all cases. Moreover, only a few cases of preeclampsia are presented in teenagers (up to 19 years old), comprising only 3.5% of the cases.
The clustering analysis showed that adult patients close to or older than 30 years of age are usually diagnosed with severe preeclampsia (O141) and require many hours of hospital care in the first two visits. On the other hand, younger patients diagnosed with preeclampsia usually require many hours of hospital care at the fourth hospital visit.
Based on the findings, in our context, to avoid complications from preeclampsia, the use of aspirin is recommended for pregnant women between the ages of 26 and 35 years who are being treated at the IESS Los Ceibos Hospital.
5.2. Limitations and Future Work
This study was limited to characterizing the demographic, age and diagnostic data of patients treated in the Gynecology Unit of the IESS Los Ceibos Hospital in Guayaquil, Ecuador. Thus, its conclusions are limited to this context and cannot be extrapolated to other hospitals or other locations.
Future work could consider the study of more clinical characteristics, as well as the extension of the research to other hospitals in the city or region, so as to review the impact of demographic and regional differences on the preeclampsia prevalence.
Author Contributions
All authors contributed to the work presented in this paper. Conceptualization, F.P.-B.; methodology, F.P.-B.; validation, F.P.-B.; investigation, F.P.-B.; writing—original draft preparation, F.P.-B., R.C.-Q., L.V.-C., E.T.-B., J.C.-A., J.B.-M. and L.C.-T.; writing—review and editing, F.P.-B., R.C.-Q., L.V.-C., E.T.-B., J.C.-A., J.B.-M. and L.C.-T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the “Universidad de Guayaquil” under project FCI-008-2021. Moreover, it was co-financed by the “Universidad Bolivariana del Ecuador” under project PROY-INV-UBE-013-2022.
Institutional Review Board Statement
Ethical approval was obtained from their Scientific Research Ethics Committee at "IESS Los Ceibos" hospital in Guayaquil-Ecuador (Reference Number IESS-FRPB-PREC-2021).
Informed Consent Statement
Due to its retrospective, non-interventional nature with the use of deidentified information, the requirement for informed consent was waived.
Data Availability Statement
The datasets presented in this article are not readily available because the data are part of an ongoing study. Requests to access the datasets should be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Rodríguez-Larraburu, E.; Barzola-Monteses, J. ACME: A Classification Model for Explaining the Risk of Preeclampsia Based on Bayesian Network Classifiers and a Non-Redundant Feature Selection Approach. Informatics 2024, 11, 31. [Google Scholar] [CrossRef]
- Parrales-Bravo, F.; Saltos-Cedeño, J.; Tomalá-Esparza, J.; Barzola-Monteses, J. Clustering-Based Approach for Characterization of Patients with Preeclampsia Using a Non-Redundant Feature Selection. In Proceedings of the 2023 3rd International Conference on Electrical, Computer, Communications and Mechatronics Engineering (ICECCME), Tenerife, Spain, 19–21 July 2023; pp. 1–6. [Google Scholar]
- Ukah, U.V.; Payne, B.; Hutcheon, J.A.; Ansermino, J.M.; Ganzevoort, W.; Thangaratinam, S.; Magee, L.A.; Von Dadelszen, P. Assessment of the fullPIERS risk prediction model in women with early-onset preeclampsia. Hypertension 2018, 71, 659–665. [Google Scholar] [CrossRef]
- Koulouraki, S.; Paschos, V.; Pervanidou, P.; Christopoulos, P.; Gerede, A.; Eleftheriades, M. Short- and Long-Term Outcomes of Preeclampsia in Offspring: Review of the Literature. Children 2023, 10, 826. [Google Scholar] [CrossRef]
- Ministerio de Salud Pública del Ecuador. Gaceta de Muerte Materna SE14. 2020. Available online: https://bit.ly/3Poz79o (accessed on 11 September 2024).
- Parrales-Bravo, F.; Caicedo-Quiroz, R.; Barzola-Monteses, J.; Cevallos-Torres, L. Prediction of Emergency Room Arrivals of Patients with Preeclampsia Disease Using Artificial Neural Network Model. In Proceedings of the 2024 IEEE 4th International Conference on Electronic Communications, Internet of Things and Big Data (ICEIB), Taipei, Taiwan, 19–21 April 2024; pp. 34–39. [Google Scholar]
- Tite-Tibanquiza, K.; Guzman-Chávez, I.; Dutan-Yupangui, L.; del Cisne Quito-Cabrera, M.; León-Santillán, E. Association between Prenatal Control and the Incidence of Preeclampsia in Ecuadorian Pregnant Women: A Cross-Sectional Study. J. Med. Health Stud. 2024, 5, 1–10. [Google Scholar] [CrossRef]
- De Kat, A.C.; Hirst, J.; Woodward, M.; Kennedy, S.; Peters, S.A. Prediction models for preeclampsia: A systematic review. Pregnancy Hypertens. 2019, 16, 48–66. [Google Scholar] [CrossRef] [PubMed]
- Shea, A. Patient Clustering Using Electronic Medical Records. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 2020. [Google Scholar]
- Qin, Y.; Ma, Z. A traditional Chinese medicine prescription recommendation method based on mutual information clustering. Proc. J. Phys. Conf. Ser. IOP 2020, 1544, 012065. [Google Scholar] [CrossRef]
- Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Kubik, M.; Li, L.; et al. Aspirin use to prevent preeclampsia and related morbidity and mortality: US Preventive Services Task Force recommendation statement. JAMA 2021, 326, 1186–1191. [Google Scholar] [PubMed]
- Farfán-Cano, S.; Farfán-Cano, H.; Altamirano-Rodas, D.; Quinde-Zambrano, R.; Loor-Parada, W.; Zambrano-Velásquez, J.; Cuadrado-Suárez, E. Hypertensive disorders of pregnancy in adolescents. Cienc. Ecuad. 2022, 4, 22–34. Available online: https://cienciaecuador.com.ec/index.php/ojs/article/view/60/175 (accessed on 11 September 2024).
- Tejera, E.; Sánchez, M.E.; Henríquez-Trujillo, A.R.; Pérez-Castillo, Y.; Coral-Almeida, M. A population-based study of preeclampsia and eclampsia in Ecuador: Ethnic, geographical and altitudes differences. BMC Pregnancy Childbirth 2021, 21, 116. [Google Scholar] [CrossRef]
- Borbón, H.F. Caracterización del Doppler patológico como predictor de preeclampsia. Rev. Cuba. Med. Gen. Integr. 2024, 40. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252024000100017&lng=es&nrm=iso (accessed on 11 September 2024).
- Sutan, R.; Aminuddin, N.A.; Mahdy, Z.A. Prevalence, maternal characteristics, and birth outcomes of preeclampsia: A cross-sectional study in a single tertiary healthcare center in greater Kuala Lumpur Malaysia. Front. Public Health 2022, 10, 973271. [Google Scholar] [CrossRef] [PubMed]
- Fitriani, H.; Keni, M.; Keni, M. Risk factors of preeclampsia among pregnant women in Indonesia. KnE Life Sci. 2021, 2021, 836–841. [Google Scholar] [CrossRef]
- Khan, B.; Yar, R.A.; khan Khakwani, A.; Karim, S.; Ali, H.A. Preeclampsia incidence and its maternal and neonatal outcomes with associated risk factors. Cureus 2022, 14, e31143. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Zhao, L.; Yu, S.; Zhou, J.; Li, J.; Zhang, N.; Xing, B.; Cui, X.; Yang, S. Differences in epidemiology of patients with preeclampsia between China and the US. Exp. Ther. Med. 2021, 22, 1012. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Ramírez, P.; Serrano, N.; Barrera, V.; Bejarano, J.P.; Silva, J.L.; Martínez, R.; Gil, F.; Olaya-C, M.; García-Robles, R. Risk factors and fetal outcomes for preeclampsia in a Colombian cohort. Heliyon 2020, 6, e05079. [Google Scholar] [CrossRef]
- Gutiérrez, K.D.L.C.; Rivasplata, J.C.; Sahuanga, C.F. Aplicación del modelo de clusterización basado en el algoritmo de k-means para la segmentación de la morbilidad materna en el hospital san bartolomé de la ciudad de LIMA-2012. Rev. Investig. Bus. Intell. 2015, 2, 15–21. [Google Scholar]
- Palmsten, K.; Chambers, C.D.; Wells, A.; Bandoli, G. Patterns of prenatal antidepressant exposure and risk of preeclampsia and postpartum haemorrhage. Paediatr. Perinat. Epidemiol. 2020, 34, 597–606. [Google Scholar] [CrossRef]
- Pereira, S.; Portela, F.; Santos, M.F.; Machado, J.; Abelha, A. Clustering-based approach for categorizing pregnant women in obstetrics and maternity care. In Proceedings of the Eighth International Conference on Computer Science & Software Engineering, Yokohama, Japan, 13–15 July 2015; pp. 98–101. [Google Scholar]
- Roell, K.R.; Harmon, Q.E.; Klungsøyr, K.; Bauer, A.E.; Magnus, P.; Engel, S.M. Clustering longitudinal blood pressure trajectories to examine heterogeneity in outcomes among preeclampsia cases and controls. Hypertension 2021, 77, 2034–2044. [Google Scholar] [CrossRef]
- Sriwandoko, H.; Purnomo, W.; Trijanto, B.; Darmawan, E.S. The Effect of Referral and Treatment of Severe Preeclampsia on Maternal Death at Sultan Imanudin General Hospital Pangkalan Bun, Central Kalimantan. In Proceedings of the International Conference on Public Health Proceeding, Surakarta, Indonesia, 23–24 October 2023; Volume 4, pp. 174–182. [Google Scholar]
- Lisonkova, S.; Bone, J.N.; Muraca, G.M.; Razaz, N.; Wang, L.Q.; Sabr, Y.; Boutin, A.; Mayer, C.; Joseph, K. Incidence and risk factors for severe preeclampsia, hemolysis, elevated liver enzymes, and low platelet count syndrome, and eclampsia at preterm and term gestation: A population-based study. Am. J. Obstet. Gynecol. 2021, 225, 538.e1–538.e19. [Google Scholar] [CrossRef]
- Van Doorn, R.; Mukhtarova, N.; Flyke, I.P.; Lasarev, M.; Kim, K.; Hennekens, C.H.; Hoppe, K.K. Dose of aspirin to prevent preterm preeclampsia in women with moderate or high-risk factors: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0247782. [Google Scholar] [CrossRef]
- Jin, J. Use of aspirin during pregnancy to prevent preeclampsia. JAMA 2021, 326, 1222. [Google Scholar] [CrossRef] [PubMed]
- Loussert, L.; Vidal, F.; Parant, O.; Hamdi, S.M.; Vayssiere, C.; Guerby, P. Aspirin for prevention of preeclampsia and fetal growth restriction. Prenat. Diagn. 2020, 40, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Rahnemaei, F.A.; Fashami, M.A.; Abdi, F.; Abbasi, M. Factors effective in the prevention of Preeclampsia: A systematic review. Taiwan J. Obstet. Gynecol. 2020, 59, 173–182. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).