
Leveraging Digital Technologies for Public Health Education in High-Density Community Spaces: A Geospatial Analysis


Abstract
1. Introduction
2. Related Work
2.1. Educational Technology and Public Health
2.2. Application of DTs to Promote PHE in CPSS
3. Methods
3.1. Data Sources and Ethics
3.2. Data Analysis
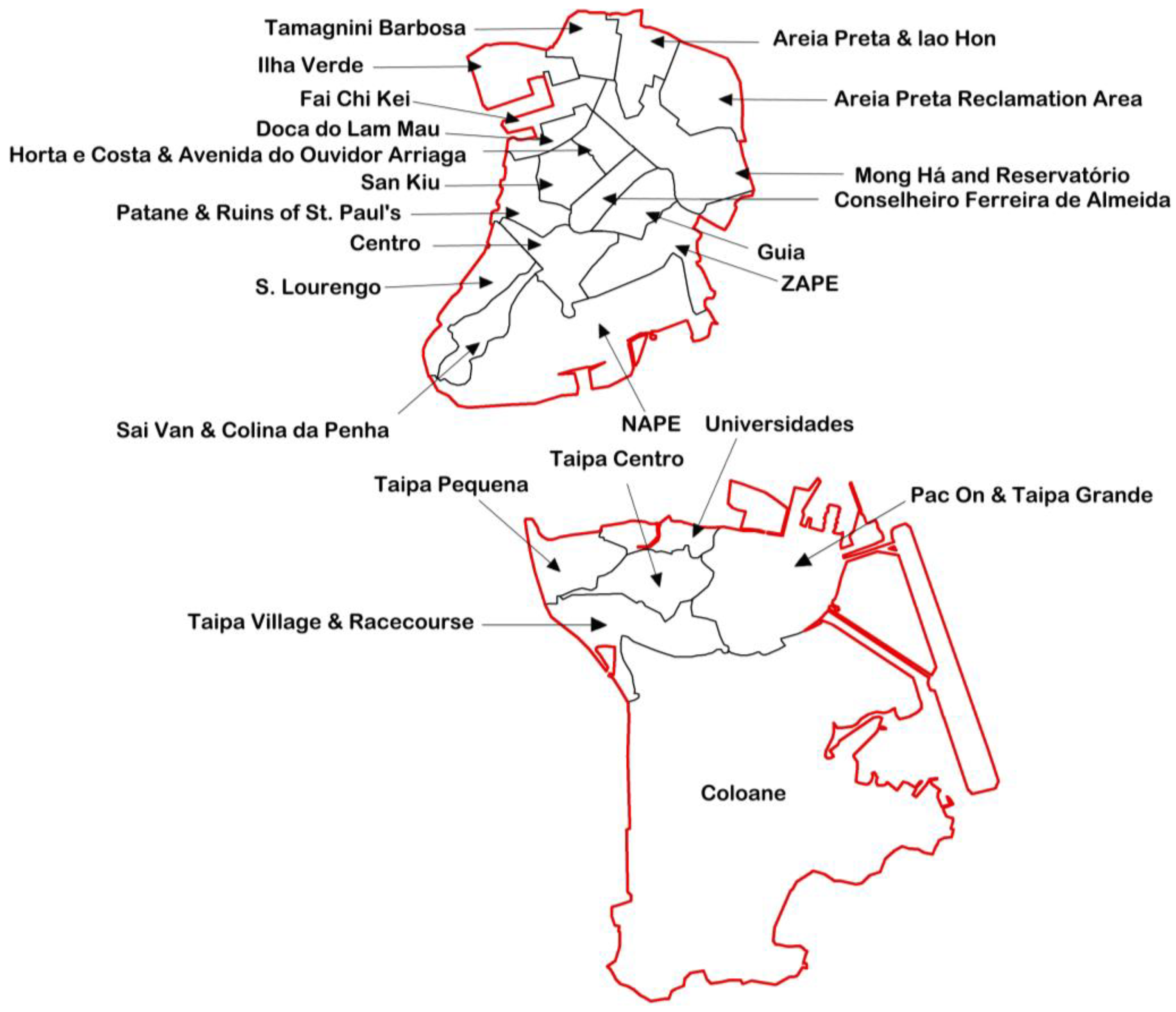
3.3. Location of Study
4. Results
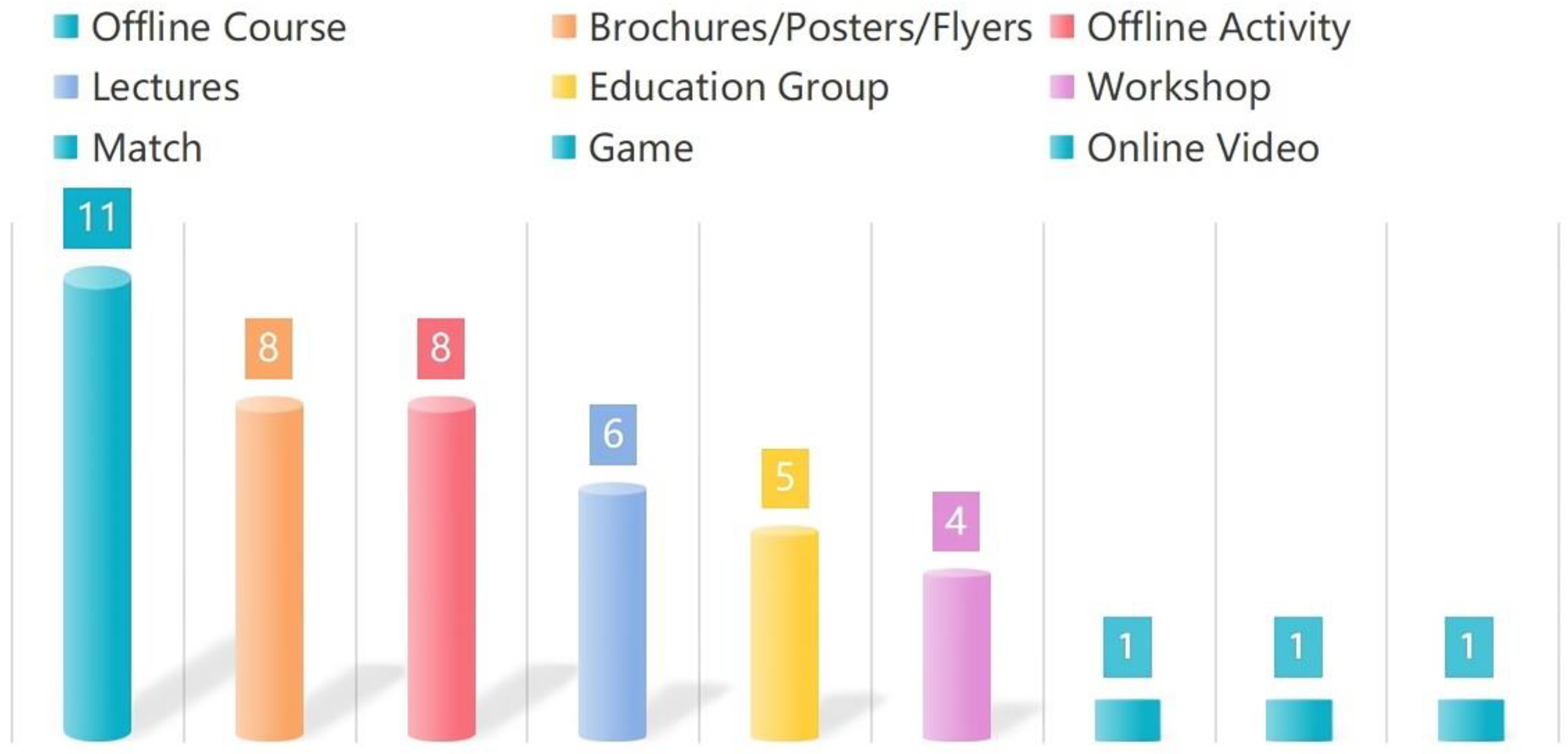
4.1. Descriptive Analysis
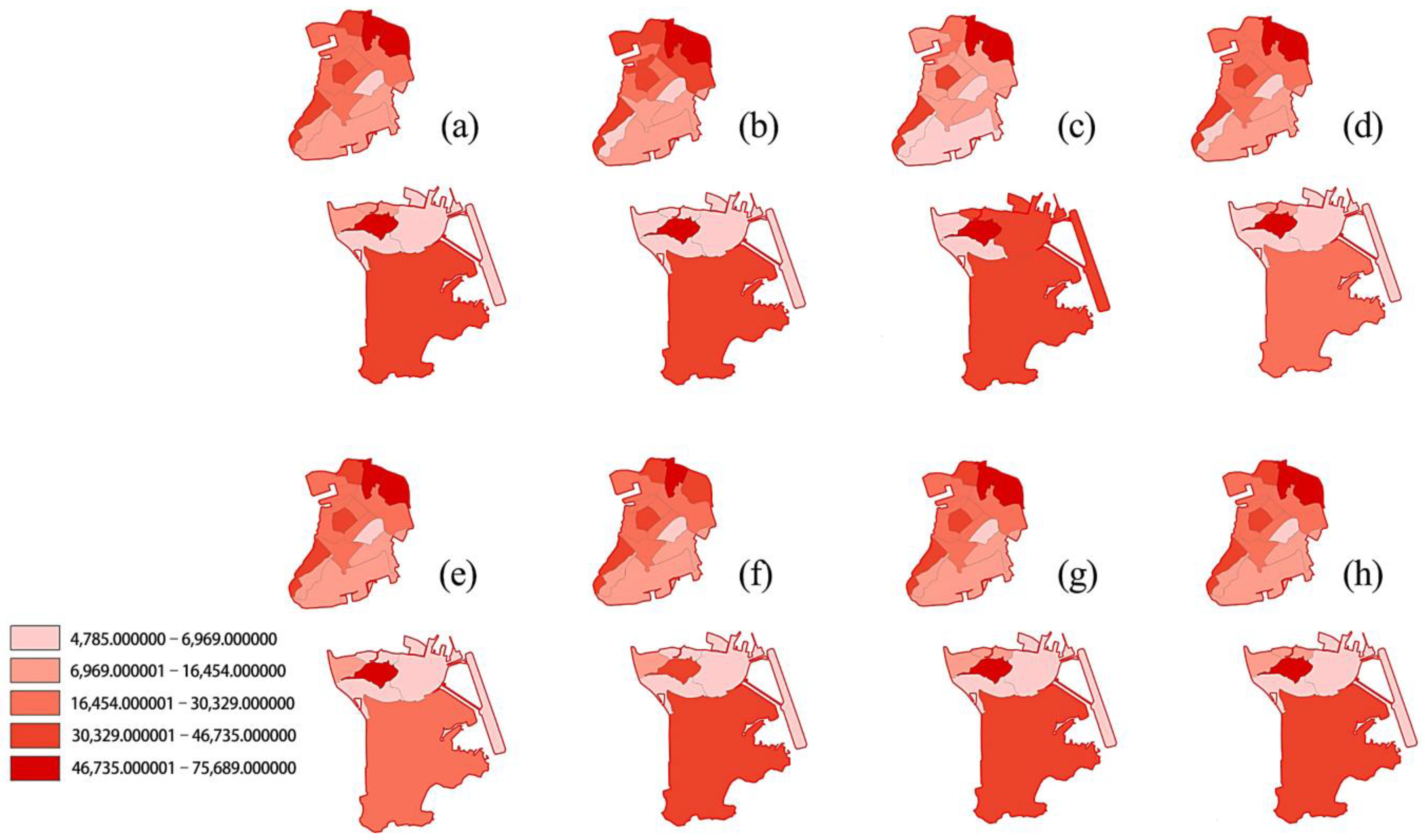
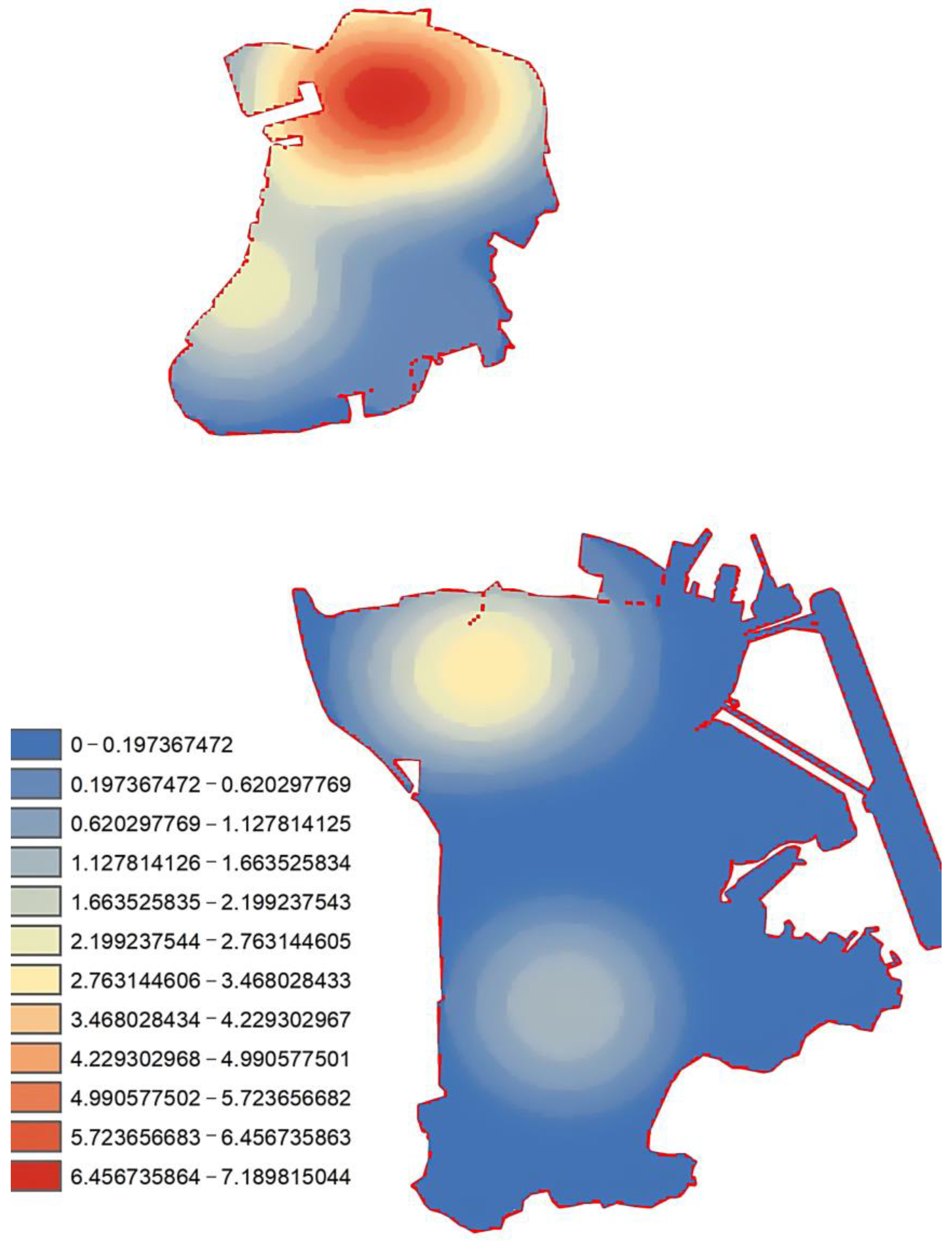
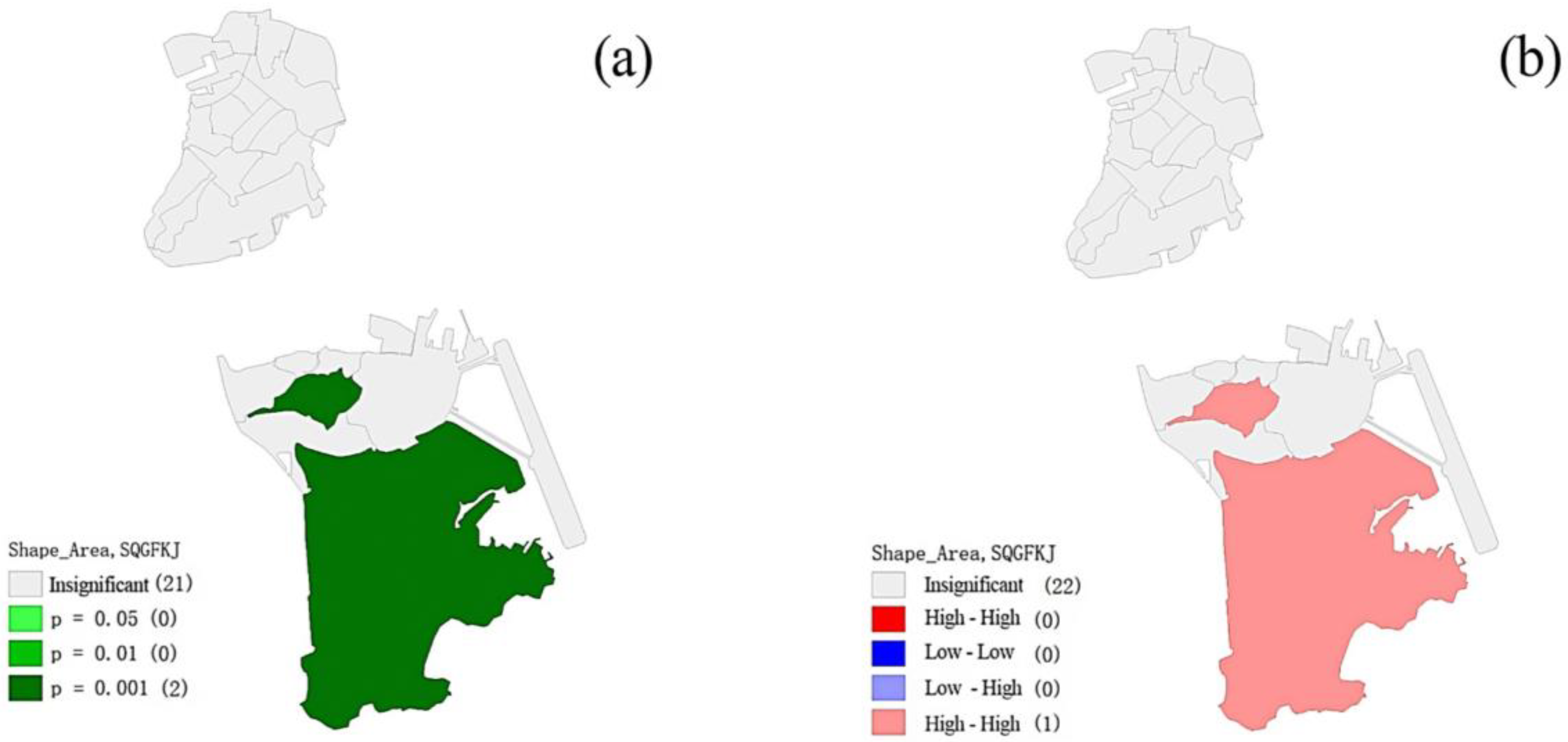
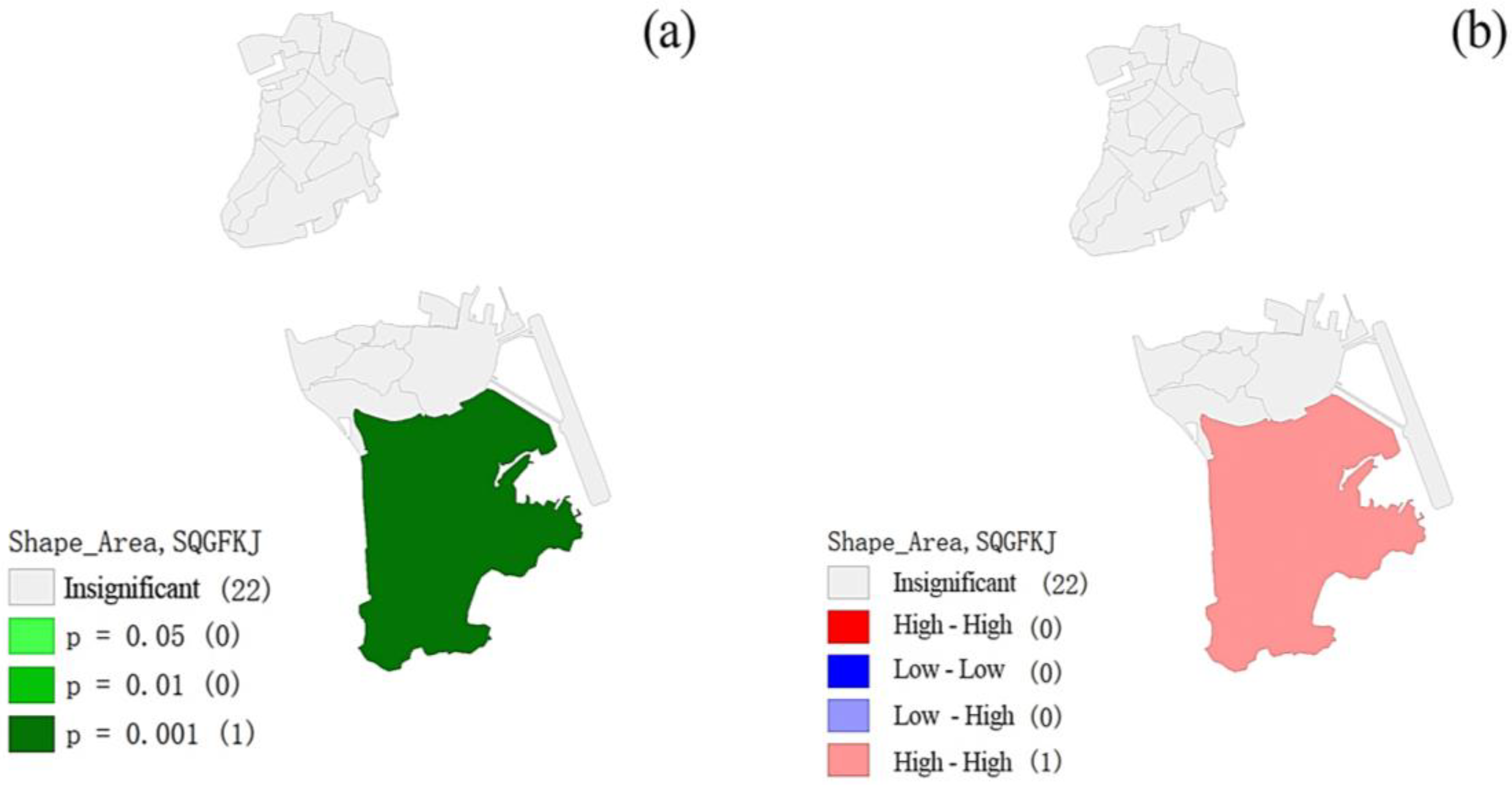
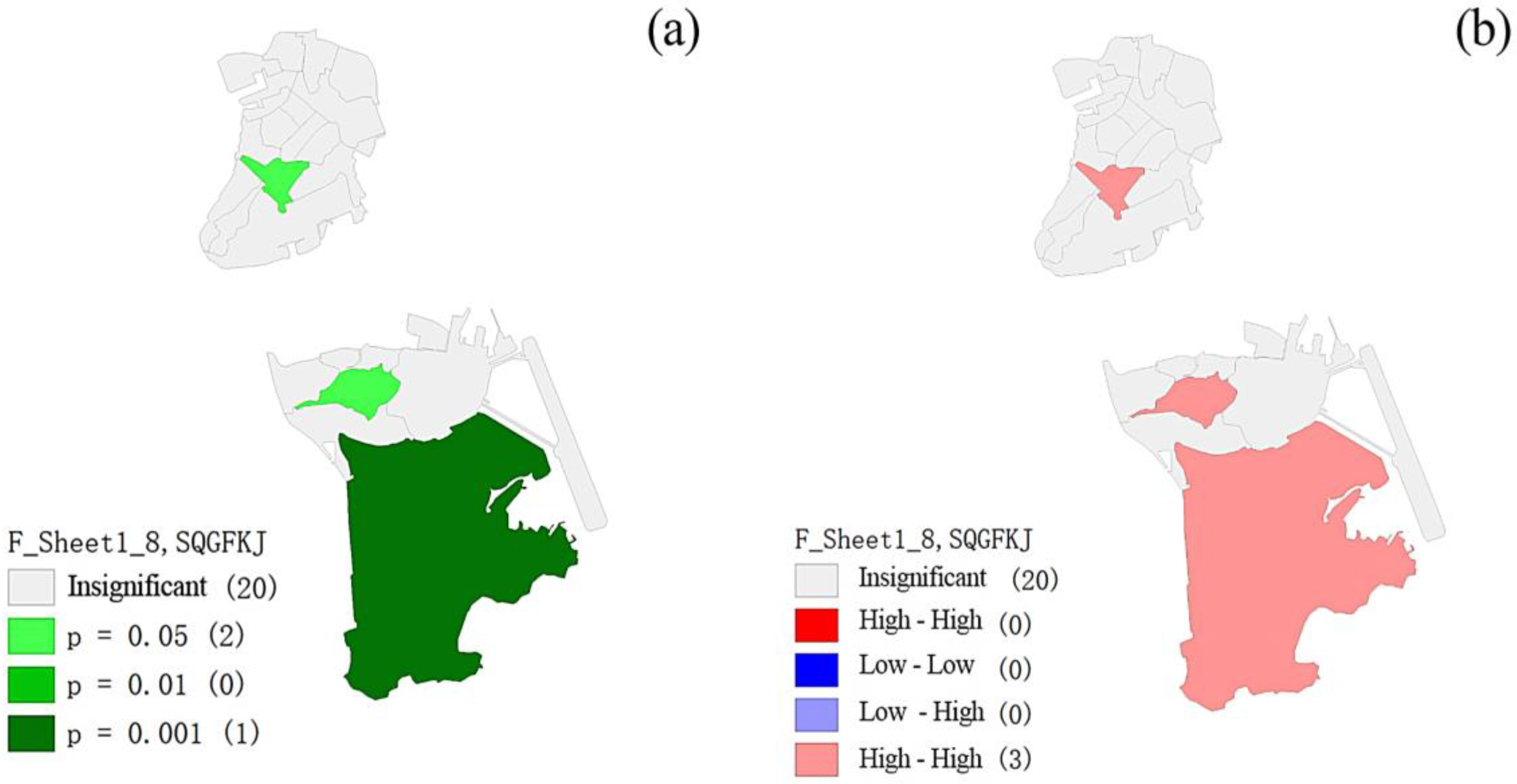
4.2. Spatial Correlation Analysis
5. Discussion
5.1. Challenges
5.1.1. Health Education in CPSSs Lacking the Integration of DTs
5.1.2. Acceptability of Educational Behavior Implemented by DTs in a Social Environment
5.2. Opportunities and Suggestions
5.3. Limitations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Population Density (Number of People per Kilometer of Land Area) [Internet]. World Bank Open Data. Available online: https://data.worldbank.org.cn/indicator/EN.POP.DNST?end=2021&most_recent_value_desc=true&start=1961&view=map (accessed on 27 May 2024).
- Freiman, V. Types of technology in Mathematics Education. Encycl. Math. Educ. 2014, 623–629. [Google Scholar] [CrossRef]
- Henderson, M.; Selwyn, N.; Aston, R. What works and why? student perceptions of ‘useful’ digital technology in Univer-sity Teaching and learning. Stud. High. Educ. 2015, 42, 1567–1579. [Google Scholar] [CrossRef]
- Gray, L.; Thomas, N.; Lewis, L.; Tice, P. Teachers’ Use of Educational Technology in U.S. Public Schools, 2009: First Look; National Center for Education Statistics, Institute of Education Sciences, U.S. Dept. of Education: Washington, DC, USA, 2010. [Google Scholar]
- Gerhardus, A.; Schilling, I.; Voss, M. Public health als anwendungsorientiertes fach und multidisziplin—“Forschendes Lernen” als antwort auf die herausforderungen für lehren und lernen? Das Gesundheitswesen 2016, 79, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Zeeb, H.; Pigeot, I.; Schüz, B. Digital Public Health—Ein überblick. Bundesgesundheitsbl 2020, 63, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.B.; Dorsey, E.R.; Mathews, S.C.; Bates, D.W.; Safavi, K. A digital health industry cohort across the Health Continuum. NPJ Digit. Med. 2020, 3, 68. [Google Scholar] [CrossRef] [PubMed]
- Anthony Jnr, B. Investigating the implementation of telehealth and digital technologies during Public Health Crisis: A qualitative review. Int. J. Health Plan. Manag. 2023, 38, 1212–1227. [Google Scholar] [CrossRef]
- Parisien, R.L.; Shin, M.; Constant, M.; Saltzman, B.M.; Li, X.; Levine, W.N.; Trofa, D.P. Telehealth utilization in response to the novel coronavirus (COVID-19) pandemic in Orthopaedic Surgery. J. Am. Acad. Orthop. Sur. Geons. 2020, 28, e487–e492. [Google Scholar] [CrossRef]
- De Santis, K.K.; Mergenthal, L.; Christianson, L.; Busskamp, A.; Vonstein, C.; Zeeb, H. Digital Technologies for Health Pro-motion and Disease Prevention in Older people: Scoping review. J. Med. Internet Res. 2023, 25, e43542. [Google Scholar] [CrossRef]
- Hong, Y.-R.; Lawrence, J.; Williams, D., Jr.; Mainous, I.I.I.A. Population-level interest and telehealth capacity of US hospitals in response to covid-19: Cross-sectional analysis of Google Search and National Hospital Survey Data. JMIR Public Health Surveill. 2020, 6, e18961. [Google Scholar] [CrossRef]
- Sun, L. As a medium of space—Rethinking community public space. Southeast Commun. 2020, 2, 94–96. [Google Scholar]
- He, D. Thoughts on research on establishment of cultural public space in urban communities. In Proceedings of the 2016 International Conference on Education, Sports, Arts and Management Engineering, Xi’an, China, 12–13 March 2016. [Google Scholar] [CrossRef]
- Crilly, P. The Use of eHealth Tools by Community Pharmacists to Improve Public Health—An Exploratory Study to Determine the Feasibility of a Community Pharmacy Weight Management Service with Private Facebook Support Group. Ph.D. Thesis, Kingston University, London, UK, 2022. [Google Scholar]
- Crilly, P.; Kayyali, R. A systematic review of randomized controlled trials of telehealth and digital technology use by community pharmacists to improve public health. Pharmacy 2020, 8, 137. [Google Scholar] [CrossRef] [PubMed]
- Chiccarelli, E.; North, S.; Pasternak, R.H. Innovative strategies for addressing adolescent health in primary care through telehealth. Pediatr. Clin. N. Am. 2024, 4, 693–706. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, P.; Bregenzer, A. Integration of eHealth tools in the process of workplace health promotion: Proposal for de-sign and implementation. J. Med. Internet Res. 2018, 20, e8769. [Google Scholar] [CrossRef] [PubMed]
- Manganello, J.; Gerstner, G.; Pergolino, K.; Graham, Y.; Falisi, A.; Strogatz, D. The relationship of health literacy with use of digital technology for health information: Implications for public health practice. J. Public Health Manag. Pract. 2017, 23, 380. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.; Arora, S.; Shah, N.; King, D.; Darzi, A. A regulatory perspective on the influence of health information technol-ogy on organisational quality and safety in England. Health Inf. J. 2020, 26, 897–910. [Google Scholar] [CrossRef]
- De Rosis, S.; Nuti, S. Public strategies for improving eHealth integration and long-term sustainability in public health care systems: Findings from an italian case study. Int. J. Health Plann. Manag. 2018, 33, 131–152. [Google Scholar] [CrossRef]
- Levy, L.; Herzog, A.N. Effects of population density and crowding on health and social adaptation in the Netherlands. J. Health Soc. Behav. 1974, 15, 228–240. [Google Scholar] [CrossRef]
- Myint, S.W. Spatial Autocorrelation; Encyclopedia of Geography: London, UK; Thousand OAKS, CA, USA, 2010. [Google Scholar]
- Cliff, A.D.; Ord, J.K. Spatial Processes: Models & Applications; Pion: London, UK, 1981. [Google Scholar]
- Bulletin of the Seventh National Census [Internet]. Bulletin of the Seventh National Census China Government Website. Available online: http://big5.www.gov.cn/gate/big5/www.gov.cn/guoqing/2021-05/13/content_5606149.htm (accessed on 28 May 2024).
- Pang, P.C.-I.; Jiang, W.; Pu, G.; Chan, K.S.; Lau, Y. Social media engagement in two governmental schemes during the COVID-19 pandemic in Macao. Int. J. Environ. Res. Public Health 2022, 19, 8976. [Google Scholar] [CrossRef]
- Nesterchuk, N.; Rabcheniuk, S.; Kuriata, A.; Boreiko, H.; Skalski, D. Application of fitness technologies to increase motor activity and physical fitness of adolescents. J. Phys. Educ. Sport 2021, 21, 2927–2933. [Google Scholar] [CrossRef]
- Bandura, A. Social Learning Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1977. [Google Scholar]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef]
- De Santis, K.K.; Jahnel, T.; Sina, E.; Wienert, J.; Zeeb, H. Digitization and health in Germany: Cross-sectional nationwide survey. JMIR Public Health Surveill. 2021, 7, e32951. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.A.; Stein, N.; Shemaj, F.; Branch, O.H.; Paruthi, J.; Kanick, S.C. Older adults engage with personalized digital coaching programs at rates that exceed those of younger adults. Front. Digit. Health 2021, 3, 642818. [Google Scholar] [CrossRef] [PubMed]
- Jaana, M.; Paré, G. Comparison of mobile health technology use for self-tracking between older adults and the general adult population in Canada: Cross-sectional survey. JMIR mHealth uHealth 2020, 8, e24718. [Google Scholar] [CrossRef] [PubMed]
- Seifert, A.; Cotten, S.R.; Xie, B. A double burden of exclusion? Digital and social exclusion of older adults in times of COVID-19. J. Gerontol. Ser. B 2020, 76, e99–e103. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Heinsch, M.; Betts, D.; Booth, D.; Kay-Lambkin, F. Barriers and facilitators to the use of e-health by older adults: A scoping review. BMC Public Health 2021, 21, 1556. [Google Scholar] [CrossRef]
- Kampmeijer, R.; Pavlova, M.; Tambor, M.; Golinowska, S.; Groot, W. The use of e-health and M-health tools in health pro-motion and primary prevention among older adults: A systematic literature review. BMC Health Serv. Res. 2016, 16, 467–479. [Google Scholar] [CrossRef]
- Kuerbis, A.; Mulliken, A.; Muench, F.; Moore, A.A.; Gardner, D. Older adults and mobile technology: Factors that enhance and inhibit utilization in the context of Behavioral Health. Ment. Health Addict. Res. 2017, 2, 2. [Google Scholar] [CrossRef]
- Meates, J. Problematic digital technology use of children and adolescents: Psychological impact. Teach. Curric. 2020, 20, 51–62. [Google Scholar] [CrossRef]
- Padilla-Góngora, D.; López-Liria, R.; del Díaz-López, M.; Aguilar-Parra, J.M.; Vargas-Muñoz, M.E.; Rocamora-Pérez, P. Hab-its of the elderly regarding access to the new information and Communication Technologies. Procedia Soc. Behav. Sci. 2017, 237, 1412–1417. [Google Scholar] [CrossRef]
- Reine, I.; Ivanovs, A.; Mieria, I.; Gehtmane-Hofmane, I.; Koroļeva, I. Overcoming social isolation with digital technologies among ageing populations during COVID-19. Soc. Integr. Educ. Proc. Int. Sci. Conf. 2021, 4, 171–178. [Google Scholar] [CrossRef]
- Stara, V.; Santini, S.; Kropf, J.; D’Amen, B. Digital Health coaching programs among older employees in transition to re-tirement: Systematic Literature Review. J. Med. Internet Res. 2020, 22, e17809. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.C.-I.; Munsie, M.; Chang, S.; Tanner, C.; Walker, C. Participatory design and evaluation of the “Stem cells australia” website for delivering complex health knowledge: Mixed Methods Study. J. Med. Internet Res. 2023, 25, e44733. [Google Scholar] [CrossRef]
- Shan, R.; Sarkar, S.; Martin, S.S. Digital health technology and mobile devices for the management of diabetes mellitus: State of the art. Diabetologia 2019, 62, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Kangeswaran, V.; Vasandarai, D.; Eliyas, C.; Munsil, M.; Kodagoda, N.; Suriyawansa, K. A bilingual audio-based online shopping mobile application for visual-ly impaired and elderly people. In Proceedings of the TENCON 2021 IEEE Region 10 Conference (TENCON), Auckland, New Zealand, 7–10 December 2021; IEEE: Piscataway, NJ, USA, 2021; pp. 658–663. [Google Scholar] [CrossRef]
- Wojciechowski, A.; Wiśniewska, A.; Pyszora, A.; Liberacka-Dwojak, M.; Juszczyk, K. Virtual reality immersive environ-ments for motor and cognitive training of elderly people: A scoping review. Hum. Technol. 2021, 17, 145–163. [Google Scholar] [CrossRef]
- Luo, Y.; Wang, Z. Feature mining algorithm for student academic prediction based on interpretable deep neural network. In Proceedings of the 2024 12th International Conference on Information and Education Technology (ICIET), Yamaguchi, Japan, 18–20 March 2024; pp. 1–5. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification of Institutions | Service Content of the Institutions | Amount |
|---|---|---|
| Services for the Aged People | Elderly center, Elderly care center, Elderly service center, Nursing home, Elderly activity center | 18 |
| Integrated Community Services | Community Center, Community Service Center, Neighborhood Associations, Comprehensive Service Center, Service Office | 17 |
| Specific Population Services | Women’s Federation, Family Service Center, Youth Community Center, Youth Service Center, Parent-Child Center | 5 |
| Local Areas | Spatial Formats | Education Formats | Education Themes |
|---|---|---|---|
| Macao Peninsula | Indoor Space | Posters, Education Group | Fitness/Health |
| Macao Peninsula | Indoor and Outdoor Space | Brochures, Lectures, Match, Offline Activity, and Workshop | Health Preserving, Mental, and Psychological Health |
| Macao Peninsula | Indoor Space | Lectures, Education Group | Health Preserving, Sex Education, Fitness/Health, Mental and Psychological Health, and Female Health |
| Macao Peninsula | Indoor Space | Offline Course, Lectures, Offline Activity | Female health, Fitness/Health, Chronic Diseases, and Cancer |
| Macao Peninsula | Indoor Space | Offline activity, Education Group | First Aid Knowledge, Sex Education for Children |
| Macao Peninsula | Indoor Space | Lectures | Fitness/Health, Geriatric Diseases and Chronic Diseases |
| Macao Peninsula | Indoor Space | Education Group, Workshop | Health Preserving, Children’s Health, and Fitness/Health |
| Macao Peninsula | Indoor Space | Brochures, Offline Activity | Cancer, Female Health, and Mental and Psychological Health |
| Macao Peninsula | Indoor Space | Offline Course, Offline Activity | Fitness/Health, Sex education, and Mental and Psychological Health |
| Macao Peninsula | Indoor and Outdoor Space | Offline Course | Health Preserving, Fitness/Health, and Mental and Psychological Health |
| Macao Peninsula | Indoor Space | Offline Course, Offline Activity | Children’s Health |
| Macao Peninsula | Indoor Space | Offline Course, Brochures | Fitness/Health, Geriatric Diseases and Chronic Diseases |
| Coloane | Indoor Space | Lectures | Geriatric Diseases and Chronic Diseases |
| Coloane | Indoor Space | Offline Activity, Lectures | Mental and Psychological Health |
| Taipa | Indoor Space | Offline course, Offline Activity, and Brochures | Fitness/Health, Geriatric Diseases and Chronic Diseases, and Health Preserving |
| Taipa | Indoor Space | Education Group | Education for Life, Female Health, and Children’s Health |
| Taipa | Indoor and Outdoor Space | Offline Course, Offline Activity, and Leaflets | Geriatric Diseases and Chronic Diseases |
| Taipa | Indoor and Outdoor Space | Workshop, Offline Course, and Online Video | First aid knowledge, Sex education, and Mental and Psychological Health |
| Taipa | Indoor and Outdoor Space | Offline Course, Offline Activity | Education for Life, Health Preservation, and Geriatric Diseases and Chronic Diseases |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, T.; Luo, Y.; Pang, P.C.-I.; Xia, Y. Leveraging Digital Technologies for Public Health Education in High-Density Community Spaces: A Geospatial Analysis. Systems 2024, 12, 504. https://doi.org/10.3390/systems12110504
Liu T, Luo Y, Pang PC-I, Xia Y. Leveraging Digital Technologies for Public Health Education in High-Density Community Spaces: A Geospatial Analysis. Systems. 2024; 12(11):504. https://doi.org/10.3390/systems12110504
Chicago/Turabian StyleLiu, Ting, Yiming Luo, Patrick Cheong-Iao Pang, and Yuanze Xia. 2024. "Leveraging Digital Technologies for Public Health Education in High-Density Community Spaces: A Geospatial Analysis" Systems 12, no. 11: 504. https://doi.org/10.3390/systems12110504
APA StyleLiu, T., Luo, Y., Pang, P. C.-I., & Xia, Y. (2024). Leveraging Digital Technologies for Public Health Education in High-Density Community Spaces: A Geospatial Analysis. Systems, 12(11), 504. https://doi.org/10.3390/systems12110504