
Immune-Mediated Diseases from the Point of View of Psychoneuroimmunoendocrinology

 ,
,  , ,
, , 
 ,
,  ,
,  ,
, 
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. What Are Immune-Mediated Diseases?
1.2. What Is Psychoneuroimmunoendocrinology (PNIE)?
1.3. Why Is it Important to Address the Problem of IMIDs from the Perspective of PNIE?
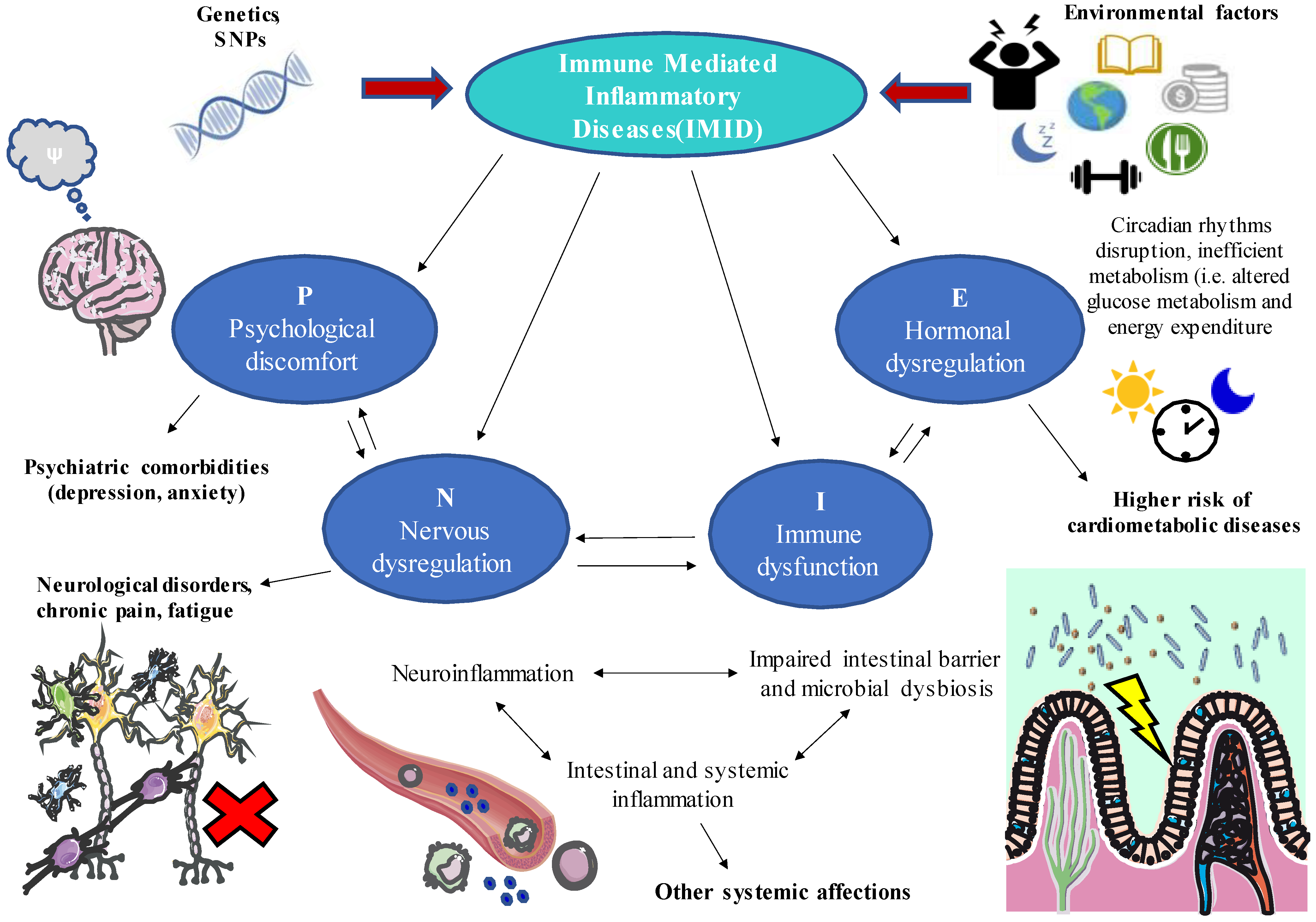
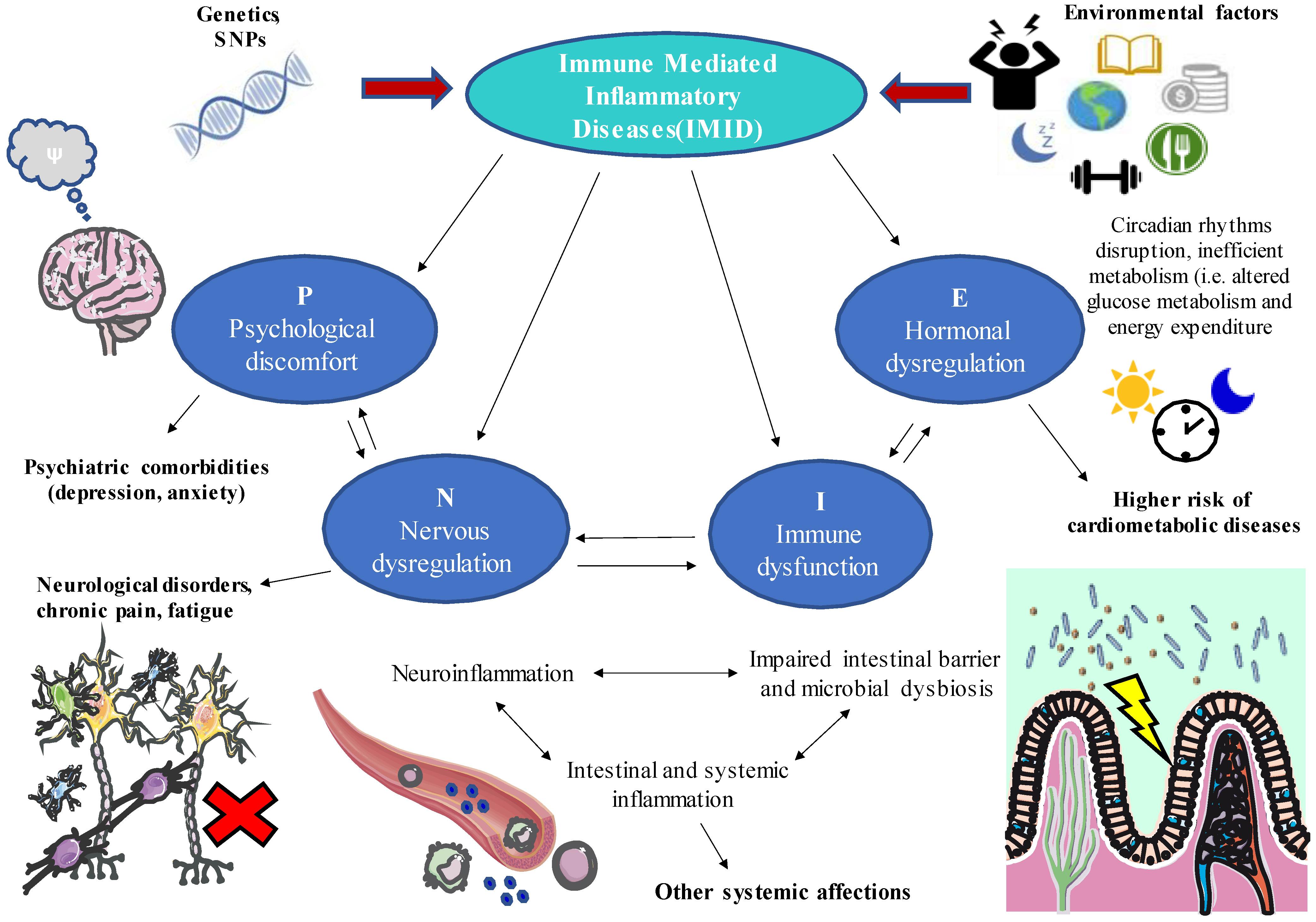
2. IMIDs from the Point of View of the PNIE
2.1. Aetiology of IMIDs
2.2. Unravelling the Key Elements of PNIE to Better Understand IMIDs
- (a)
- Immune system dysfunction in IMIDs
- (b)
- Nervous system dysfunction in IMIDs
- (c)
- Endocrine deregulation in IMIDs
- (d)
- Psychology in IMIDs
- (e)
- The role of gut microbiota as part of the PNIE
2.3. Holistic Integration of the PNIE in IMIDs
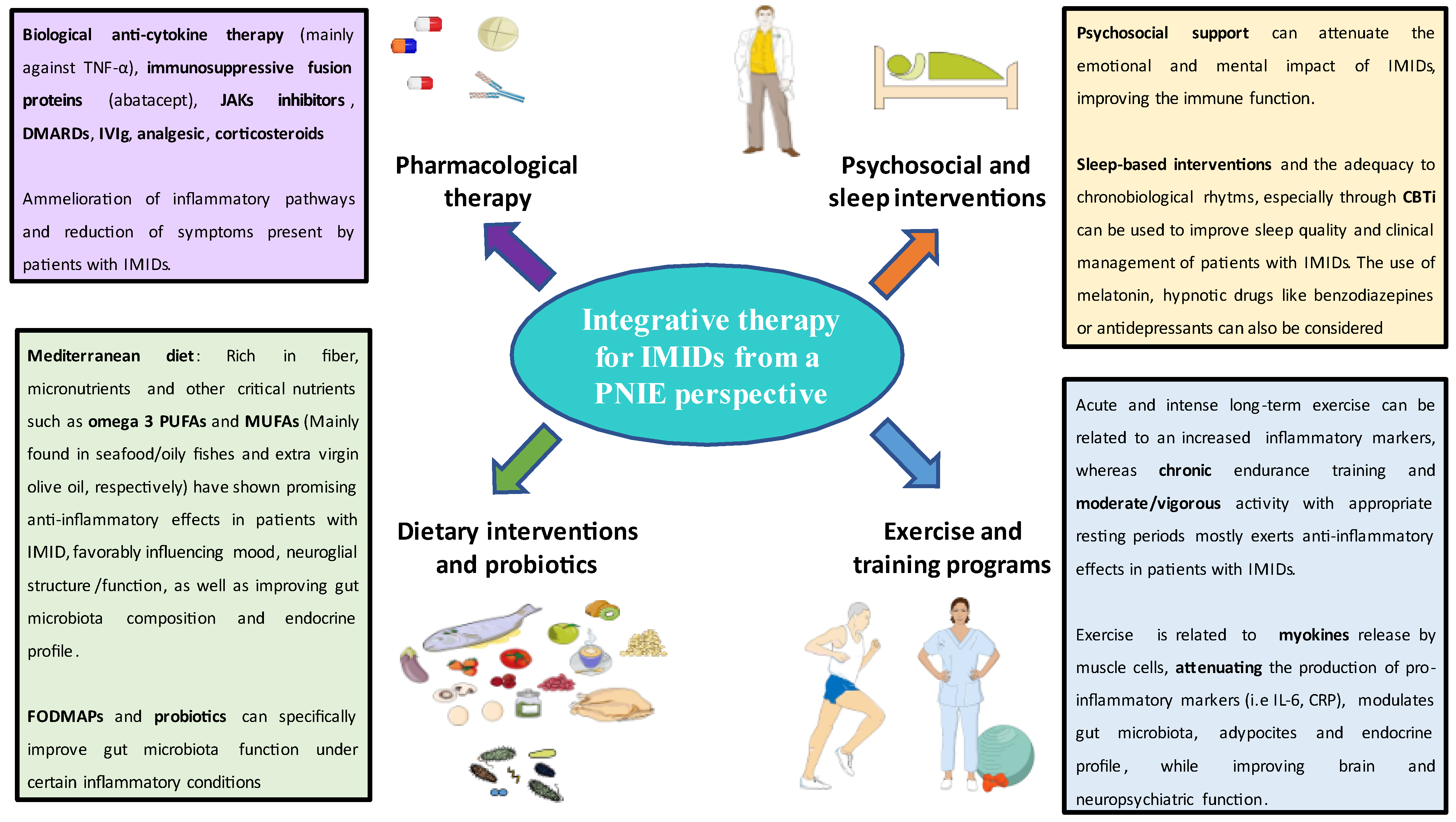
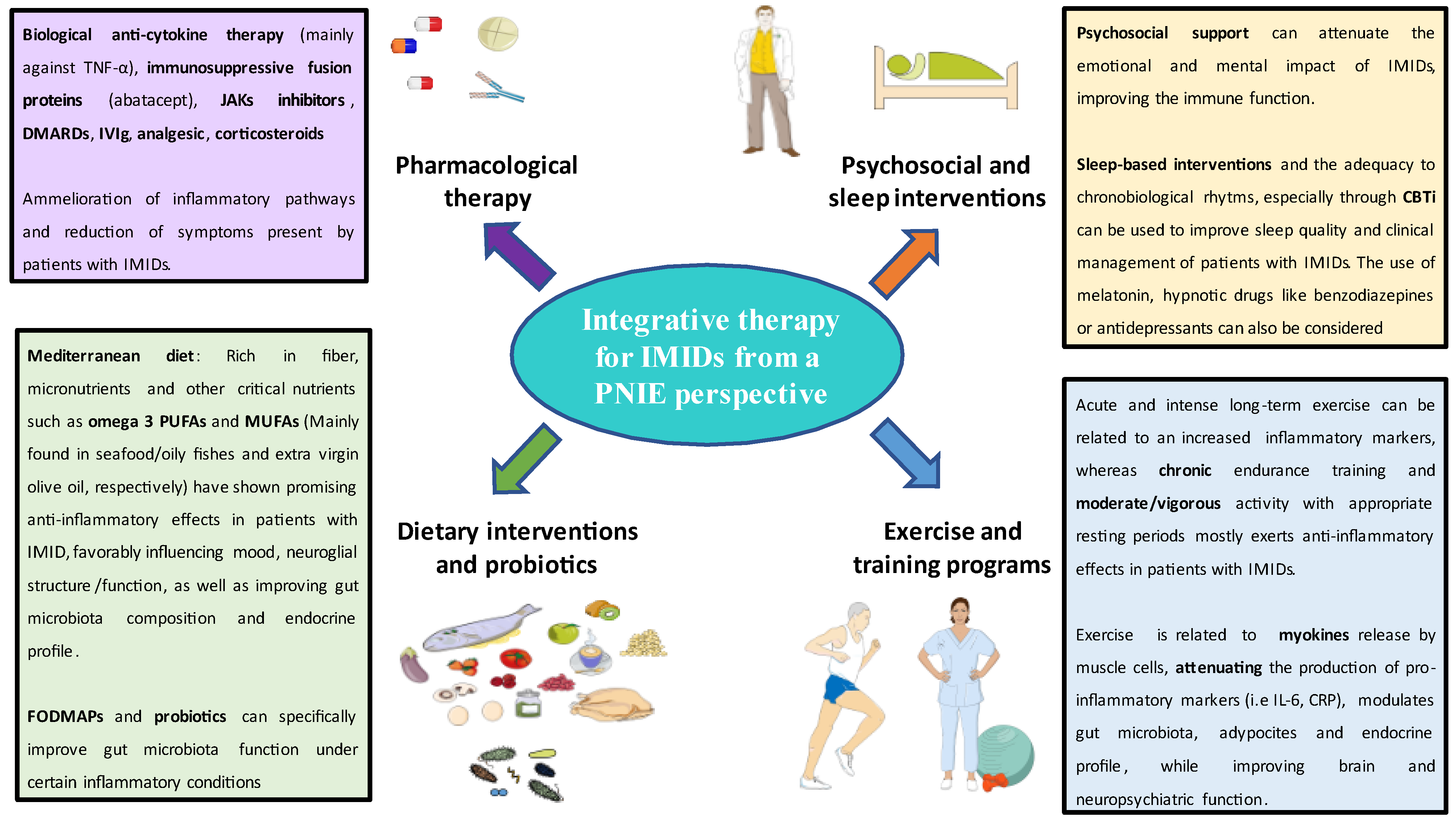
3. IMID Treatments and Their Optimization from the PNIE
3.1. Available Pharmacological Treatments
3.2. Targeted Psychosomatic Therapy and Integrated Medicine
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McInnes, I.B.; Gravallese, E.M. Immune-Mediated Inflammatory Disease Therapeutics: Past, Present and Future. Nat. Rev. Immunol. 2021, 21, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Rahman, P.; Inman, R.D.; El-Gabalawy, H.; Krause, D.O. Pathophysiology and Pathogenesis of Immune-Mediated Inflammatory Diseases: Commonalities and Differences. J. Rheumatol. Suppl. 2010, 85, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.S.; Gulliver, W.P.; Irvine, E.J.; Albani, S.; Dutz, J.P. Quality of Life in Patients with Immune-Mediated Inflammatory Diseases. J. Rheumatol. Suppl. 2011, 88, 7–19. [Google Scholar] [CrossRef] [PubMed]
- El-Gabalawy, H.; Guenther, L.C.; Bernstein, C.N. Epidemiology of Immune-Mediated Inflammatory Diseases: Incidence, Prevalence, Natural History, and Comorbidities. J. Rheumatol. Suppl. 2010, 85, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Chao, W.C.; Chen, Y.H.; Hsieh, T.Y.; Lai, K.L.; Chen, Y.M.; Hung, W.T.; Lin, C.T.; Tseng, C.W.; Lin, C.H. Risk of Immune-Mediated Inflammatory Diseases in Newly Diagnosed Ankylosing Spondylitis Patients: A Population-Based Matched Cohort Study. Arthritis Res. Ther. 2019, 21, 196. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, P.; Bissonnette, R.; Guenther, L.C. Socioeconomic Burden of Immune-Mediated Inflammatory Diseases—Focusing on Work Productivity and Disability. J. Rheumatol. Suppl. 2011, 88, 55–61. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Shahabi, A.; Seabury, S.A.; Lakdawalla, D.N.; Espinosa, O.D.; Green, S.; Brauer, M.; Baldassano, R.N. Lifetime Economic Burden of Crohn’s Disease and Ulcerative Colitis by Age at Diagnosis. Clin. Gastroenterol. Hepatol. 2020, 18, 889–897.e10. [Google Scholar] [CrossRef]
- Lundkvist, J.; Kastäng, F.; Kobelt, G. The Burden of Rheumatoid Arthritis and Access to Treatment: Health Burden and Costs. Eur. J. Health Econ. 2008, 8, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Puig, L.; de Morales, J.G.R.; Dauden, E.; Andreu, J.L.; Cervera, R.; Adán, A.; Marsal, S.; Escobar, C.; Hinojosa, J.; Palau, J.; et al. La Prevalencia de Diez Enfermedades Inflamatorias Inmunomediadas (IMID) En España. Rev. Española Salud Pública 2019, 93, e201903013. [Google Scholar]
- França, K.; Lotti, T.M. Psycho-Neuro-Endocrine-Immunology: A Psychobiological Concept. Adv. Exp. Med. Biol. 2017, 996, 123–134. [Google Scholar] [CrossRef]
- Orlov, D.; Orlov, D.S. In Memoriam and Tribute to George Freeman Solomon Professor Emeritus of Psychiatry & Biobehavioral Sciences, University of California, Los Angeles 1931–2001. Med. Acad. J. 2019, 19, 5–7. [Google Scholar]
- González-Díaz, S.N.; Arias-Cruz, A.; Elizondo-Villarreal, B.; Monge-Ortega, O.P. Psychoneuroimmunoendocrinology: Clinical Implications. World Allergy Organ. J. 2017, 10, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farzanfar, D.; Dowlati, Y.; French, L.E.; Lowes, M.A.; Alavi, A. Inflammation: A Contributor to Depressive Comorbidity in Inflammatory Skin Disease. Ski. Pharmacol. Physiol. 2018, 31, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pryce, C.R.; Fontana, A. Depression in Autoimmune Diseases. Curr. Top. Behav. Neurosci. 2017, 31, 139–154. [Google Scholar] [CrossRef] [Green Version]
- Qiu, W.; Cai, X.; Zheng, C.; Qiu, S.; Ke, H.; Huang, Y. Update on the Relationship between Depression and Neuroendocrine Metabolism. Front. Neurosci. 2021, 15, 1122. [Google Scholar] [CrossRef]
- Lee, C.H.; Giuliani, F. The Role of Inflammation in Depression and Fatigue. Front. Immunol 2019, 10, 1696. [Google Scholar] [CrossRef] [Green Version]
- David, T.; Ling, S.F.; Barton, A. Genetics of Immune-Mediated Inflammatory Diseases. Clin. Exp. Immunol. 2018, 193, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Bogdanos, D.P.; Smyk, D.S.; Rigopoulou, E.I.; Mytilinaiou, M.G.; Heneghan, M.A.; Selmi, C.; Eric Gershwin, M. Twin Studies in Autoimmune Disease: Genetics, Gender and Environment. J. Autoimmun. 2012, 38, J156–J169. [Google Scholar] [CrossRef]
- Agca, R.; Smulders, Y.; Nurmohamed, M. Cardiovascular Disease Risk in Immune-Mediated Inflammatory Diseases: Recommendations for Clinical Practice. Heart 2022, 108, 73–79. [Google Scholar] [CrossRef]
- Medina, G.; Vera-Lastra, O.; Peralta-Amaro, A.L.; Jiménez-Arellano, M.P.; Saavedra, M.A.; Cruz-Domínguez, M.P.; Jara, L.J. Metabolic Syndrome, Autoimmunity and Rheumatic Diseases. Pharmacol. Res. 2018, 133, 277–288. [Google Scholar] [CrossRef]
- Majdan, M. Immune-Mediated Inflammatory Diseases and Accompanying Comorbidities. Wiad. Lek. 2016, 69, 611–615. [Google Scholar] [PubMed]
- De Mattos, B.R.R.; Garcia, M.P.G.; Nogueira, J.B.; Paiatto, L.N.; Albuquerque, C.G.; Souza, C.L.; Fernandes, L.G.R.; Tamashiro, W.M.D.S.C.; Simioni, P.U. Inflammatory Bowel Disease: An Overview of Immune Mechanisms and Biological Treatments. Mediat. Inflamm. 2015, 2015, 493012. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.W.; Barrett, J.C.; Parkes, M.; Satsangi, J. New IBD Genetics: Common Pathways with Other Diseases. Gut 2011, 60, 1739–1753. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, C.M.; Tobin, A.M.; Kirby, B. Innate Immunity in the Pathogenesis of Psoriasis. Arch. Dermatol. Res. 2011, 303, 691–705. [Google Scholar] [CrossRef]
- Dayer, J.M.; Oliviero, F.; Punzi, L. A Brief History of IL-1 and IL-1 Ra in Rheumatology. Front. Pharmacol. 2017, 8, 293. [Google Scholar] [CrossRef]
- He, H.; Guttman-Yassky, E. JAK Inhibitors for Atopic Dermatitis: An Update. Am. J. Clin. Dermatol. 2018, 20, 181–192. [Google Scholar] [CrossRef]
- Flores-Borja, F.; Jury, E.C.; Mauri, C.; Ehrenstein, M.R. Defects in CTLA-4 Are Associated with Abnormal Regulatory T Cell Function in Rheumatoid Arthritis. Proc. Natl. Acad. Sci. USA 2008, 105, 19396–19401. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Xu, J.; Wu, J. The Role of Co-Signaling Molecules in Psoriasis and Their Implications for Targeted Treatment. Front. Pharmacol. 2021, 12, 1872. [Google Scholar] [CrossRef]
- Lee, K.H.; Ahn, B.S.; Cha, D.; Jang, W.W.; Choi, E.; Park, S.; Park, J.H.; Oh, J.; Jung, D.E.; Park, H.; et al. Understanding the Immunopathogenesis of Autoimmune Diseases by Animal Studies Using Gene Modulation: A Comprehensive Review. Autoimmun. Rev. 2020, 19, 102469. [Google Scholar] [CrossRef]
- Turner, M.D.; Nedjai, B.; Hurst, T.; Pennington, D.J. Cytokines and Chemokines: At the Crossroads of Cell Signalling and Inflammatory Disease. Biochim. Biophys. Acta (BBA) Mol. Cell Res. 2014, 1843, 2563–2582. [Google Scholar] [CrossRef] [Green Version]
- Jeppesen, R.; Benros, M.E. Autoimmune Diseases and Psychotic Disorders. Front. Psychiatry 2019, 10, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stüve, O.; Zettl, U. Neuroinflammation of the Central and Peripheral Nervous System: An Update. Clin. Exp. Immunol. 2014, 175, 333–335. [Google Scholar] [CrossRef] [PubMed]
- Varatharaj, A.; Galea, I. The Blood-Brain Barrier in Systemic Inflammation. Brain Behav. Immun. 2017, 60, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Fung, A.; Vizcaychipi, M.; Lloyd, D.; Wan, Y.; Ma, D. Central Nervous System Inflammation in Disease Related Conditions: Mechanistic Prospects. Brain Res. 2012, 1446, 144–155. [Google Scholar] [CrossRef]
- DiSabato, D.J.; Quan, N.; Godbout, J.P. Neuroinflammation: The Devil Is in the Details. J. Neurochem. 2016, 139 (Suppl. 2), 136–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skaper, S.D.; Facci, L.; Zusso, M.; Giusti, P. An Inflammation-Centric View of Neurological Disease: Beyond the Neuron. Front. Cell Neurosci. 2018, 12, 72. [Google Scholar] [CrossRef]
- Gorelick, P.B. Role of Inflammation in Cognitive Impairment: Results of Observational Epidemiological Studies and Clinical Trials. Ann. N. Y. Acad. Sci. 2010, 1207, 155–162. [Google Scholar] [CrossRef]
- Kieseier, B.C.; Mathey, E.K.; Sommer, C.; Hartung, H.P. Immune-Mediated Neuropathies. Nat. Rev. Dis. Primers 2018, 4, 31. [Google Scholar] [CrossRef]
- DeQuattro, K.; Imboden, J.B. Neurologic Manifestations of Rheumatoid Arthritis. Rheum. Dis. Clin. 2017, 43, 561–571. [Google Scholar] [CrossRef]
- Ferro, J.M.; Oliveira, S.N.; Correia, L. Neurologic Manifestations of Inflammatory Bowel Diseases. Handb. Clin. Neurol. 2014, 120, 595–605. [Google Scholar] [CrossRef]
- Straub, R.H. Interaction of the Endocrine System with Inflammation: A Function of Energy and Volume Regulation. Arthritis Res. Ther. 2014, 16, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danve, A.S.; Kulkarni, S. Do Tumor Necrosis Factor (TNF) Inhibitors Improve the Glycemic Control in Patients with Rheumatoid Arthritis and Concomitant Diabetes Mellitus? Am. J. Ther. 2017, 24, e347–e350. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Seriolo, B.; Villaggio, B.; Pizzorni, C.; Craviotto, C.; Sulli, A. Androgens and Estrogens Modulate the Immune and Inflammatory Responses in Rheumatoid Arthritis. Ann. N. Y. Acad. Sci. 2002, 966, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Butchart, J.; Birch, B.; Bassily, R.; Wolfe, L.; Holmes, C. Male Sex Hormones and Systemic Inflammation in Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2013, 27, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, V.E. The Anti-Inflammatory Effects of Testosterone. J. Endocr. Soc. 2019, 3, 91. [Google Scholar] [CrossRef] [Green Version]
- Grandys, M.; Majerczak, J.; Zapart-Bukowska, J.; Duda, K.; Kulpa, J.K.; Zoladz, J.A. Lowered Serum Testosterone Concentration Is Associated with Enhanced Inflammation and Worsened Lipid Profile in Men. Front. Endocrinol. 2021, 12, 735638. [Google Scholar] [CrossRef]
- Araujo, A.B.; Esche, G.R.; Kupelian, V.; O’Donnell, A.B.; Travison, T.G.; Williams, R.E.; Clark, R.V.; McKinlay, J.B. Prevalence of Symptomatic Androgen Deficiency in Men. J. Clin. Endocrinol. Metab. 2007, 92, 4241–4247. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.; Nassau, D.E.; Patel, P.; Ramasamy, R. Low Testosterone in Adolescents & Young Adults. Front. Endocrinol. 2019, 10, 916. [Google Scholar] [CrossRef]
- Traish, A.; Bolanos, J.; Nair, S.; Saad, F.; Morgentaler, A. Do Androgens Modulate the Pathophysiological Pathways of Inflammation? Appraising the Contemporary Evidence. J. Clin. Med. 2018, 7, 549. [Google Scholar] [CrossRef] [Green Version]
- Cai, Z.; Xie, C.; Qiao, W.; Fei, X.; Guo, X.; Liu, H.; Li, X.; Fang, X.; Guo, Y.; Xu, G.; et al. The Role of Estrogen Membrane Receptor (G Protein-Coupled Estrogen Receptor 1) in Skin Inflammation Induced by Systemic Lupus Erythematosus Serum IgG. Front. Immunol. 2017, 8, 1723. [Google Scholar] [CrossRef] [Green Version]
- Straub, R.H.; Cutolo, M. Glucocorticoids and Chronic Inflammation. Rheumatology 2016, 55, ii6–ii14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comas, M.; Gordon, C.J.; Oliver, B.G.; Stow, N.W.; King, G.; Sharma, P.; Ammit, A.J.; Grunstein, R.R.; Phillips, C.L. A Circadian Based Inflammatory Response—Implications for Respiratory Disease and Treatment. Sleep Sci. Pract. 2017, 1, 18. [Google Scholar] [CrossRef]
- Allada, R.; Bass, J. Circadian Mechanisms in Medicine. N. Engl. J. Med 2021, 384, 550. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, I.J.; Huang, C.C.; Liu, S.C.; Tang, C.H. Reconsidering the Role of Melatonin in Rheumatoid Arthritis. Int. J. Mol. Sci. 2020, 21, 2877. [Google Scholar] [CrossRef] [PubMed]
- Buttgereit, F.; Smolen, J.S.; Coogan, A.N.; Cajochen, C. Clocking in: Chronobiology in Rheumatoid Arthritis. Nat. Rev. Rheumatol. 2015, 11, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M. Chronobiology and the Treatment of Rheumatoid Arthritis. Curr. Opin. Rheumatol. 2012, 24, 312–318. [Google Scholar] [CrossRef]
- Kemeny, M.E.; Schedlowski, M. Understanding the Interaction between Psychosocial Stress and Immune-Related Diseases: A Stepwise Progression. Brain Behav. Immun. 2007, 21, 1009–1018. [Google Scholar] [CrossRef]
- Zachariae, R.; Robert Zachariae, P. Psychoneuroimmunology: A Bio-Psycho-Social Approach to Health and Disease. Scand. J. Psychol. 2009, 50, 645–651. [Google Scholar] [CrossRef]
- Segerstrom, S.C.; Miller, G.E. Psychological Stress and the Human Immune System: A Meta-Analytic Study of 30 Years of Inquiry. Psychol. Bull. 2004, 130, 601–630. [Google Scholar] [CrossRef] [Green Version]
- Soria, V.; Uribe, J.; Salvat-Pujol, N.; Palao, D.; Menchón, J.M.; Labad, J. Psychoneuroimmunology of Mental Disorders. Rev. Psiquiatr. Y Salud Ment. 2018, 11, 115–124. [Google Scholar] [CrossRef]
- Reinhorn, I.M.; Bernstein, C.N.; Graff, L.A.; Patten, S.B.; Sareen, J.; Fisk, J.D.; Bolton, J.M.; Hitchon, C.; Marrie, R.A. Social Phobia in Immune-Mediated Inflammatory Diseases. J. Psychosom. Res. 2020, 128, 109890. [Google Scholar] [CrossRef] [PubMed]
- Euesden, J.; Danese, A.; Lewis, C.M.; Maughan, B. A Bidirectional Relationship between Depression and the Autoimmune Disorders—New Perspectives from the National Child Development Study. PLoS ONE 2017, 12, e0173015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, M.A.C.; Wand, G. Stress and the HPA Axis: Role of Glucocorticoids in Alcohol Dependence. Alcohol Res. Curr. Rev. 2012, 34, 468. [Google Scholar]
- Cussotto, S.; Sandhu, K.V.; Dinan, T.G.; Cryan, J.F. The Neuroendocrinology of the Microbiota-Gut-Brain Axis: A Behavioural Perspective. Front. Neuroendocrinol. 2018, 51, 80–101. [Google Scholar] [CrossRef]
- Faresjö, M. The Link between Psychological Stress and Autoimmune Response in Children. Crit. Rev. Immunol. 2015, 35, 117–134. [Google Scholar] [CrossRef]
- Walker, J.R.; Graff, L.A.; Dutz, J.P.; Bernstein, C.N. Psychiatric Disorders in Patients with Immune-Mediated Inflammatory. J. Rheumatol. Rheumatol. 2011, 88, 2020. [Google Scholar] [CrossRef]
- Ortega, M.A.; Alvarez-Mon, M.A.; García-Montero, C.; Fraile-Martinez, O.; Guijarro, L.G.; Lahera, G.; Monserrat, J.; Valls, P.; Mora, F.; Rodríguez-Jiménez, R.; et al. Gut Microbiota Metabolites in Major Depressive Disorder—Deep Insights into Their Pathophysiological Role and Potential Translational Applications. Metabolites 2022, 12, 50. [Google Scholar] [CrossRef]
- Strandwitz, P. Neurotransmitter Modulation by the Gut Microbiota. Brain Res. 2018, 1693, 128. [Google Scholar] [CrossRef]
- Gonz Alez-Sarrías, A.; Espín, J.C.; Tom As-Barber, F.A. Non-Extractable Polyphenols Produce Gut Microbiota Metabolites That Persist in Circulation and Show Anti-Inflammatory and Free Radical-Scavenging Effects. Trends Food Sci. Technol. 2017, 69, 281–288. [Google Scholar] [CrossRef]
- Man, A.W.C.; Zhou, Y.; Xia, N.; Li, H. Involvement of Gut Microbiota, Microbial Metabolites and Interaction with Polyphenol in Host Immunometabolism. Nutrients 2020, 12, 3054. [Google Scholar] [CrossRef]
- Li, S.; Hua, D.; Wang, Q.; Yang, L.; Wang, X.; Luo, A.; Yang, C. The Role of Bacteria and Its Derived Metabolites in Chronic Pain and Depression: Recent Findings and Research Progress. Int. J. Neuropsychopharmacol. 2020, 23, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.D.; Chen, C.Y.; Knox, N.C.; Marrie, R.A.; El-Gabalawy, H.; De Kievit, T.; Alfa, M.; Bernstein, C.N.; Van Domselaar, G. A Comparative Study of the Gut Microbiota in Immune-Mediated Inflammatory Diseases-Does a Common Dysbiosis Exist? Microbiome 2018, 6, 221. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Forbes, J.D. Gut Microbiome in Inflammatory Bowel Disease and Other Chronic Immune-Mediated Inflammatory Diseases. Inflamm. Intest. Dis. 2017, 2, 116. [Google Scholar] [CrossRef] [PubMed]
- Ilchmann-Diounou, H.; Menard, S. Psychological Stress, Intestinal Barrier Dysfunctions, and Autoimmune Disorders: An Overview. Front. Immunol. 2020, 11, 1823. [Google Scholar] [CrossRef]
- Holzer, P.; Farzi, A. Neuropeptides and the Microbiota-Gut-Brain Axis. Adv. Exp. Med. Biol. 2014, 817, 195. [Google Scholar] [CrossRef] [Green Version]
- Lissoni, P.; Messina, G.; Pelizzoni, F.; Rovelli, F.; Brivio, F.; Monzon, A.; Crivelli, N.; Lissoni, A.; Tassoni, S.; Sassola, A.; et al. The Fascination of Cytokine Immunological Science. J. Infect. 2020, 3, 18–28. [Google Scholar] [CrossRef]
- Bialek, K.; Czarny, P.; Strycharz, J.; Sliwinski, T. Major Depressive Disorders Accompanying Autoimmune Diseases—Response to Treatment. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 95, 109678. [Google Scholar] [CrossRef]
- Sjöstedt, P.; Enander, J.; Isung, J. Serotonin Reuptake Inhibitors and the Gut Microbiome: Significance of the Gut Microbiome in Relation to Mechanism of Action, Treatment Response, Side Effects, and Tachyphylaxis. Front. Psychiatry 2021, 12, 778. [Google Scholar] [CrossRef]
- Gregory, J.M.; Mak, M.; McIntyre, R.S. Inflammation and Depression in Patients with Autoimmune Disease, Diabetes, and Obesity. In Inflammation and Immunity in Depression: Basic Science and Clinical Applications; Academic Press: Cambridge, MA, USA, 2018; pp. 377–392. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Giuffrida, G.; Campennì, A. Autoimmune Endocrine Diseases. Minerva Endocrinol. 2018, 43, 305–322. [Google Scholar] [CrossRef]
- Michels, A.W.; Eisenbarth, G.S. Immunologic Endocrine Disorders. J. Allergy Clin. Immunol. 2010, 125, S226–S237. [Google Scholar] [CrossRef] [Green Version]
- The Endocrine System and Autoimmunity-Autoimmunity-NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459473/ (accessed on 17 June 2022).
- de Bellis, A.; Bizzarro, A.; Pivonello, R.; Lombardi, G.; Bellastella, A. Prolactin and Autoimmunity. Pituitary 2005, 8, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Bellastella, G.; Maiorino, M.I.; Bizzarro, A.; Giugliano, D.; Esposito, K.; Bellastella, A.; de Bellis, A. Revisitation of Autoimmune Hypophysitis: Knowledge and Uncertainties on Pathophysiological and Clinical Aspects. Pituitary 2016, 19, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Barthel, A.; Benker, G.; Berens, K.; Diederich, S.; Manfras, B.; Gruber, M.; Kanczkowski, W.; Kline, G.; Kamvissi-Lorenz, V.; Hahner, S.; et al. An Update on Addison’s Disease. Exp. Clin. Endocrinol. Diabetes 2019, 127, 165–170. [Google Scholar] [CrossRef] [Green Version]
- Hellesen, A.; Bratland, E.; Husebye, E.S. Autoimmune Addison’s Disease—An Update on Pathogenesis. Ann. Endocrinol. 2018, 79, 157–163. [Google Scholar] [CrossRef]
- Erichsen, M.M.; Løvås, K.; Skinningsrud, B.; Wolff, A.B.; Undlien, D.E.; Svartberg, J.; Fougner, K.J.; Berg, T.J.; Bollerslev, J.; Mella, B.; et al. Clinical, Immunological, and Genetic Features of Autoimmune Primary Adrenal Insufficiency: Observations from a Norwegian Registry. J. Clin. Endocrinol. Metab. 2009, 94, 4882–4890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterzl, I.; Absolonova, K.; Matucha, P. Psycho-Immuno-Endocrinology of the Thyroid Gland. Vnitr. Lek. 2016, 62, 107–114. [Google Scholar] [PubMed]
- Linares, R.; Francés, R.; Gutiérrez, A.; Juanola, O. Bacterial Translocation as Inflammatory Driver in Crohn’s Disease. Front. Cell Dev. Biol. 2021, 9, 2305. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Selmi, C.; Tang, R.; Gershwin, M.E.; Ma, X. The Microbiome and Autoimmunity: A Paradigm from the Gut–Liver Axis. Cell. Mol. Immunol. 2018, 15, 595–609. [Google Scholar] [CrossRef] [Green Version]
- Melsheimer, R.; Geldhof, A.; Apaolaza, I.; Schaible, T. Remicade® (Infliximab): 20 Years of Contributions to Science and Medicine. Biol. Targets Ther. 2019, 13, 139. [Google Scholar] [CrossRef] [Green Version]
- Lapadula, G.; Marchesoni, A.; Armuzzi, A.; Blandizzi, C.; Caporali, R.; Chimenti, S.; Cimaz, R.; Cimino, L.; Gionchetti, P.; Girolomoni, G.; et al. Adalimumab in the Treatment of Immune-Mediated Diseases. Int. J. Immunopathol. Pharmacol. 2014, 27, 33–48. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, K.; Vogelzang, E.H.; Lambert, J.; Wolbink, G.; Cheifetz, A.S. Therapeutic Drug Monitoring with Biologic Agents in Immune Mediated Inflammatory Diseases. Expert Rev. Clin. Immunol. 2019, 15, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Shyamsundar, K.; Agrawal, M.; Vichare, N.; Biswas, J. Current Knowledge of Biologics in Treatment of Noninfectious Uveitis. J. Ocul. Pharmacol. Ther. 2022, 38, 203–222. [Google Scholar] [CrossRef] [PubMed]
- Figuero-Pérez, L.; Olivares-Hernández, A.; Escala-Cornejo, R.A.; Cruz-Hernández, J.J. Use of Anakinra in The Treatment of SARS-CoV-2 Severe Respiratory Infection. Reumatol. Clin. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef]
- Pope, J.E.; Rampakakis, E.; Sampalis, J. The Durability of Abatacept as a First and Subsequent Biologic and Improvement in HAQ from a Large Multi-Site Real-World Study. Semin. Arthritis Rheum. 2015, 44, 499–505. [Google Scholar] [CrossRef]
- Armuzzi, A.; Lionetti, P.; Blandizzi, C.; Caporali, R.; Chimenti, S.; Cimino, L.; Gionchetti, P.; Girolomoni, G.; Lapadula, G.; Marchesoni, A.; et al. Anti-TNF Agents as Therapeutic Choice in Immune-Mediated Inflammatory Diseases: Focus on Adalimumab. Int. J. Immunopathol. Pharmacol. 2014, 27, 11–32. [Google Scholar] [CrossRef] [Green Version]
- Dinarello, C.A. Interleukin-1 in the Pathogenesis and Treatment of Inflammatory Diseases. Blood 2011, 117, 3720. [Google Scholar] [CrossRef] [Green Version]
- Lopalco, G.; Cantarini, L.; Vitale, A.; Iannone, F.; Anelli, M.G.; Andreozzi, L.; Lapadula, G.; Galeazzi, M.; Rigante, D. Interleukin-1 as a Common Denominator from Autoinflammatory to Autoimmune Disorders: Premises, Perils, and Perspectives. Mediat. Inflamm. 2015, 2015, 194864. [Google Scholar] [CrossRef] [Green Version]
- Nakada, T.; Mager, D.E. Systems Model Identifies Baseline Cytokine Concentrations as Potential Predictors of Rheumatoid Arthritis Inflammatory Response to Biologics. Br. J. Pharmacol. 2022, 1–15. [Google Scholar] [CrossRef]
- Gonzalez-Gay, M.A.; Gonzalez-Juanatey, C.; Vazquez-Rodriguez, T.R.; Miranda-Filloy, J.A.; Llorca, J. Insulin Resistance in Rheumatoid Arthritis: The Impact of the Anti-TNF-Alpha Therapy. Ann. N. Y. Acad. Sci. 2010, 1193, 153–159. [Google Scholar] [CrossRef]
- Stagakis, I.; Bertsias, G.; Karvounaris, S.; Kavousanaki, M.; Virla, D.; Raptopoulou, A.; Kardassis, D.; Boumpas, D.T.; Sidiropoulos, P.I. Anti-Tumor Necrosis Factor Therapy Improves Insulin Resistance, Beta Cell Function and Insulin Signaling in Active Rheumatoid Arthritis Patients with High Insulin Resistance. Arthritis Res. Ther. 2012, 14, R141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paschou, S.A.; Kothonas, F.; Lafkas, A.; Myroforidis, A.; Loi, V.; Terzi, T.; Karagianni, O.; Poulou, A.; Goumas, K.; Vryonidou, A. Favorable Effect of Anti-TNF Therapy on Insulin Sensitivity in Nonobese, Nondiabetic Patients with Inflammatory Bowel Disease. Int. J. Endocrinol. 2018, 2018, 6712901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fragoulis, G.E.; Mcinnes, I.B.; Siebert, S. JAK-Inhibitors. New Players in the Field of Immune-Mediated Diseases, beyond Rheumatoid Arthritis. Rheumatology 2019, 58, i43. [Google Scholar] [CrossRef] [Green Version]
- Benjamin, O.; Bansal, P.; Goyal, A.; Lappin, S.L. Disease Modifying Anti-Rheumatic Drugs (DMARD). StatPearls 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK507863/ (accessed on 17 June 2022).
- Nicolau, J.; Lequerré, T.; Bacquet, H.; Vittecoq, O. Rheumatoid Arthritis, Insulin Resistance, and Diabetes. Jt. Bone Spine 2017, 84, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.; Kaveri, S.V. The Mechanisms of Action of IVIG in Autoimmune and Inflammatory Diseases. ISBT Sci. Ser. 2013, 8, 185–188. [Google Scholar] [CrossRef]
- Anchang, C.G.; Xu, C.; Raimondo, M.G.; Atreya, R.; Maier, A.; Schett, G.; Zaburdaev, V.; Rauber, S.; Ramming, A. The Potential of OMICs Technologies for the Treatment of Immune-Mediated Inflammatory Diseases. Int. J. Mol. Sci. 2021, 22, 7506. [Google Scholar] [CrossRef]
- García-Montero, C.; Fraile-Martínez, O.; Gómez-Lahoz, A.M.; Pekarek, L.; Castellanos, A.J.; Noguerales-Fraguas, F.; Coca, S.; Guijarro, L.G.; García-Honduvilla, N.; Asúnsolo, A.; et al. Nutritional Components in Western Diet Versus Mediterranean Diet at the Gut Microbiota-Immune System Interplay. Implications for Health and Disease. Nutrients 2021, 13, 699. [Google Scholar] [CrossRef]
- Santangelo, C.; Varì, R.; Scazzocchio, B.; De Sancti, P.; Giovannini, C.; D`Archivio, M.; Masella, R. Anti-Inflammatory Activity of Extra Virgin Olive Oil Polyphenols: Which Role in the Prevention and Treatment of Immune-Mediated Inflammatory Diseases? Endocr. Metab. Immune Disord. Drug Targets 2018, 18, 36–50. [Google Scholar] [CrossRef]
- Gammone, M.A.; Riccioni, G.; Parrinello, G.; D’orazio, N. Omega-3 Polyunsaturated Fatty Acids: Benefits and Endpoints in Sport. Nutrients 2019, 11, 46. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C. Omega-3 Polyunsaturated Fatty Acids and Inflammatory Processes: Nutrition or Pharmacology? Br. J. Clin. Pharmacol. 2013, 75, 645–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons, C.L.; Finucane, O.F.; Murphy, A.M.; Cooke, A.A.; Viollet, B.; Vieira, P.M.; Oldham, W.; Kahn, B.B.; Roche, H.M. Monounsaturated Fatty Acids Impede Inflammation Partially Through Activation of AMPK. FASEB J. 2016, 30, 296.5. [Google Scholar] [CrossRef]
- Mocking, R.J.T.; Assies, J.; Ruhé, H.G.; Schene, A.H. Focus on Fatty Acids in the Neurometabolic Pathophysiology of Psychiatric Disorders. J. Inherit. Metab. Dis. 2018, 41, 597–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Jarr, K.; Layton, C.; Gardner, C.D.; Ashouri, J.F.; Abreu, M.T.; Sinha, S.R. Therapeutic Implications of Diet in Inflammatory Bowel Disease and Related Immune-Mediated Inflammatory Diseases. Nutrients 2021, 13, 890. [Google Scholar] [CrossRef]
- Ertek, S.; Cicero, A. Impact of Physical Activity on Inflammation: Effects on Cardiovascular Disease Risk and Other Inflammatory Conditions. Arch. Med. Sci. AMS 2012, 8, 794. [Google Scholar] [CrossRef] [Green Version]
- Ploeger, H.E.; Takken, T.; de Greef, M.H.G.; Timmons, B.W. The Effects of Acute and Chronic Exercise on Inflammatory Markers in Children and Adults with a Chronic Inflammatory Disease: A Systematic Review. Exerc. Immunol. Rev. 2009, 15, 6–41. [Google Scholar]
- Cerqueira, É.; Marinho, D.A.; Neiva, H.P.; Lourenço, O. Inflammatory Effects of High and Moderate Intensity Exercise—A Systematic Review. Front. Physiol. 2020, 10, 1550. [Google Scholar] [CrossRef]
- Benatti, F.B.; Pedersen, B.K. Exercise as an Anti-Inflammatory Therapy for Rheumatic Diseases—Myokine Regulation. Nat. Rev. Rheumatol. 2014, 11, 86–97. [Google Scholar] [CrossRef]
- Leal, L.G.; Lopes, M.A.; Batista, M.L. Physical Exercise-Induced Myokines and Muscle-Adipose Tissue Crosstalk: A Review of Current Knowledge and the Implications for Health and Metabolic Diseases. Front. Physiol. 2018, 9, 1307. [Google Scholar] [CrossRef]
- Suriano, F.; Van Hul, M.; Cani, P.D. Gut Microbiota and Regulation of Myokine-Adipokine Function. Curr. Opin. Pharmacol. 2020, 52, 9–17. [Google Scholar] [CrossRef]
- Kim, S.; Choi, J.Y.; Moon, S.; Park, D.H.; Kwak, H.B.; Kang, J.H. Roles of Myokines in Exercise-Induced Improvement of Neuropsychiatric Function. Pflug. Arch. Eur. J. Physiol. 2019, 471, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Shields, G.S.; Spahr, C.M.; Slavich, G.M. Psychosocial Interventions and Immune System Function: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. JAMA Psychiatry 2020, 77, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, M.S.; Bovbjerg, D.H.; Renna, M.E.; Lekander, M.; Mennin, D.S.; Zachariae, R. Effects of Psychological Interventions on Systemic Levels of Inflammatory Biomarkers in Humans: A Systematic Review and Meta-Analysis. Brain Behav. Immun. 2018, 74, 68–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ditmer, M.; Gabryelska, A.; Turkiewicz, S.; Białasiewicz, P.; Małecka-wojciesko, E.; Sochal, M. Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review. J. Clin. Med. 2022, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- van der Zweerde, T.; Bisdounis, L.; Kyle, S.D.; Lancee, J.; van Straten, A. Cognitive Behavioral Therapy for Insomnia: A Meta-Analysis of Long-Term Effects in Controlled Studies. Sleep Med. Rev. 2019, 48, 101208. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, M.A.; García-Montero, C.; Fraile-Martinez, O.; Alvarez-Mon, M.A.; Gómez-Lahoz, A.M.; Lahera, G.; Monserrat, J.; Rodriguez-Jimenez, R.; Quintero, J.; Álvarez-Mon, M. Immune-Mediated Diseases from the Point of View of Psychoneuroimmunoendocrinology. Biology 2022, 11, 973. https://doi.org/10.3390/biology11070973
Ortega MA, García-Montero C, Fraile-Martinez O, Alvarez-Mon MA, Gómez-Lahoz AM, Lahera G, Monserrat J, Rodriguez-Jimenez R, Quintero J, Álvarez-Mon M. Immune-Mediated Diseases from the Point of View of Psychoneuroimmunoendocrinology. Biology. 2022; 11(7):973. https://doi.org/10.3390/biology11070973
Chicago/Turabian StyleOrtega, Miguel A., Cielo García-Montero, Oscar Fraile-Martinez, Miguel Angel Alvarez-Mon, Ana Maria Gómez-Lahoz, Guillermo Lahera, Jorge Monserrat, Roberto Rodriguez-Jimenez, Javier Quintero, and Melchor Álvarez-Mon. 2022. "Immune-Mediated Diseases from the Point of View of Psychoneuroimmunoendocrinology" Biology 11, no. 7: 973. https://doi.org/10.3390/biology11070973
APA StyleOrtega, M. A., García-Montero, C., Fraile-Martinez, O., Alvarez-Mon, M. A., Gómez-Lahoz, A. M., Lahera, G., Monserrat, J., Rodriguez-Jimenez, R., Quintero, J., & Álvarez-Mon, M. (2022). Immune-Mediated Diseases from the Point of View of Psychoneuroimmunoendocrinology. Biology, 11(7), 973. https://doi.org/10.3390/biology11070973