
Evaluation of T2 Magnetic Resonance (T2MR®) Technology for the Early Detection of ESKAPEc Pathogens in Septic Patients

 ,
,  , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Study Design
2.2. Microbiological Evaluation
2.3. Study Aims
2.4. Statistical Analysis
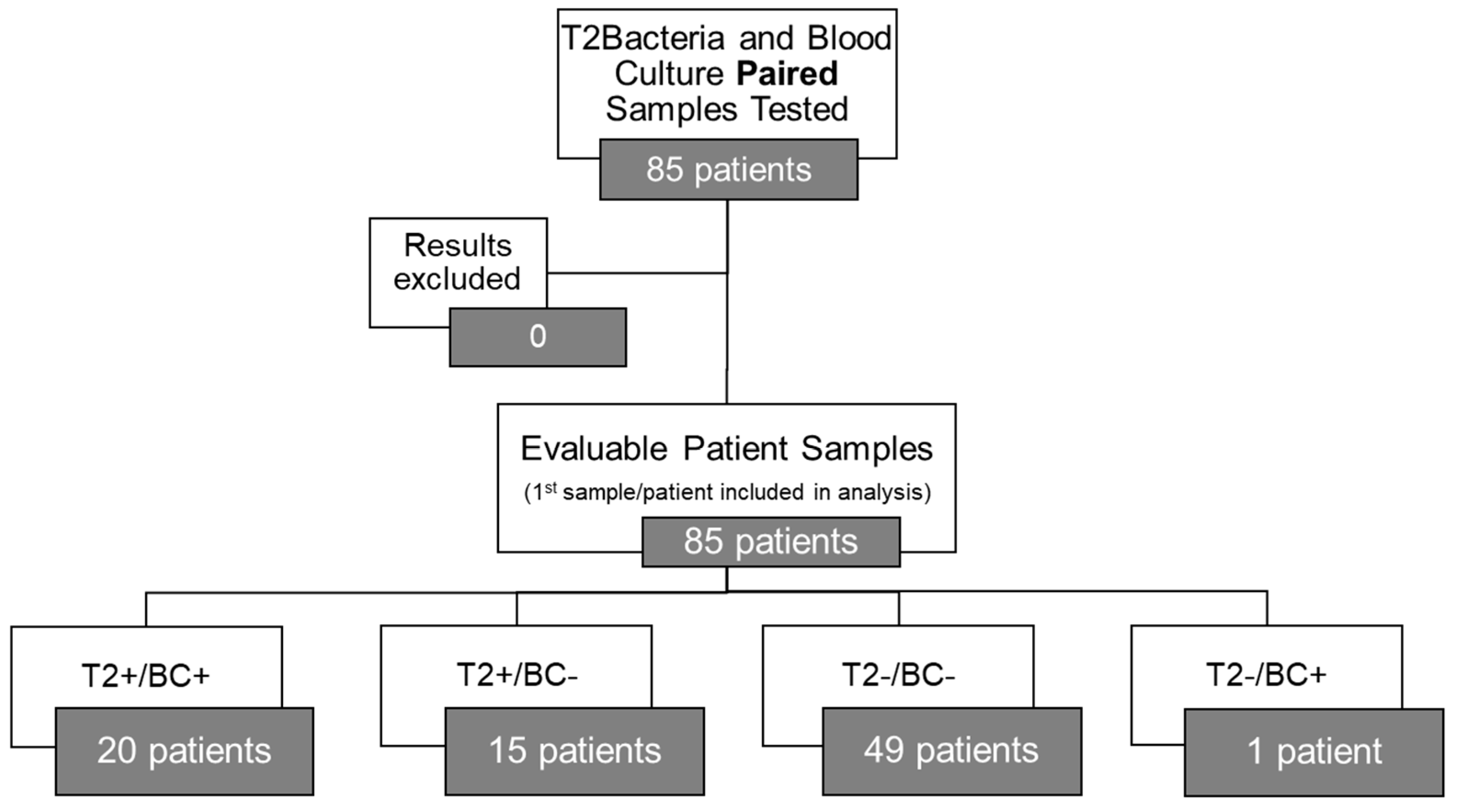
3. Results
3.1. Characteristics
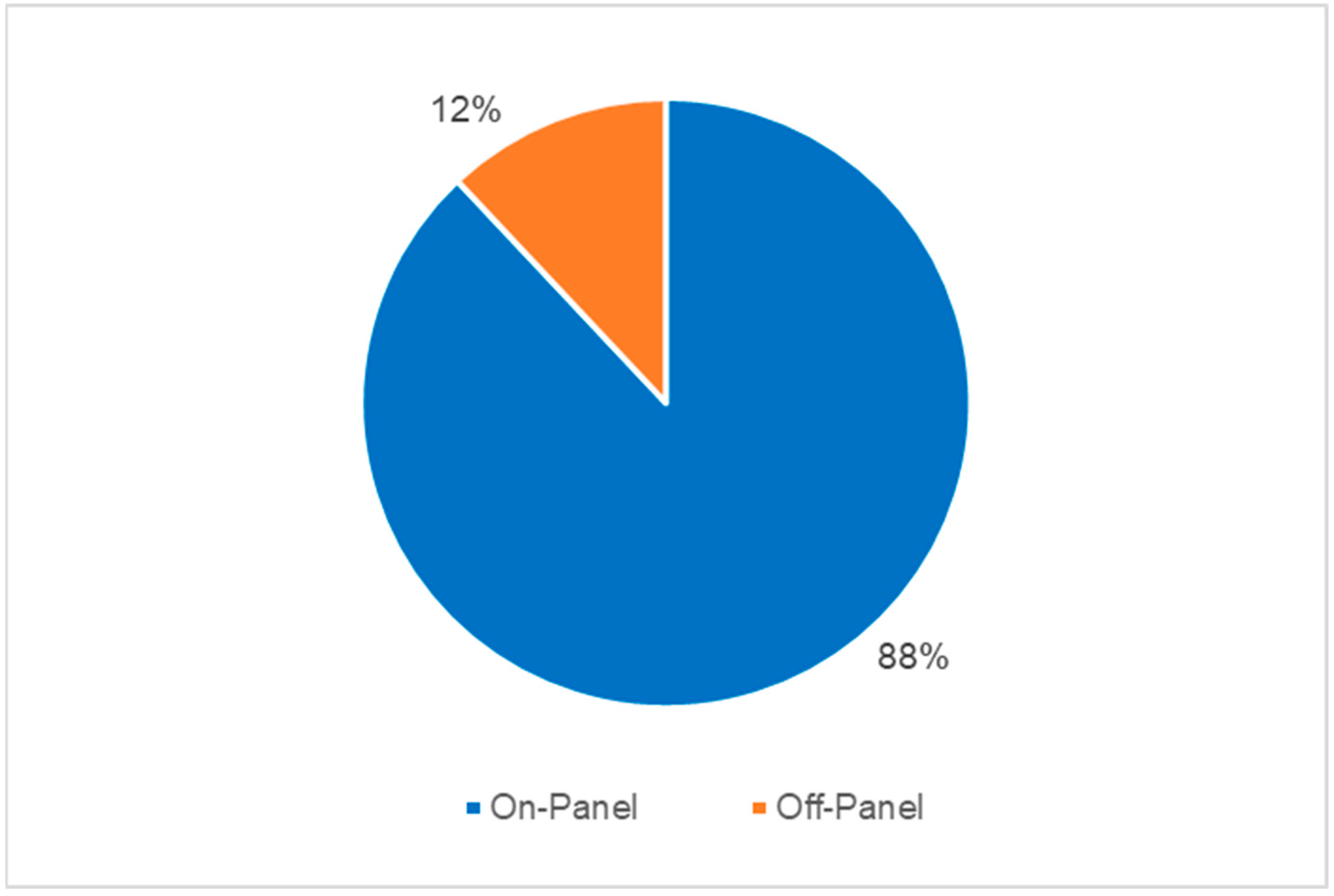
3.2. Microbiological Concordance and Turn-Around Time
3.3. Antibiotic Therapy Prescriptions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bearman, G.M.; Wenzel, R.P. Bacteremias: A leading cause of death. Arch. Med. Res. 2005, 36, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Buehler, S.S.; Madison, B.; Snyder, S.R.; Derzon, J.H.; Cornish, N.E.; Saubolle, M.A.; Weissfeld, A.S.; Weinstein, M.P.; Liebow, E.B.; Wolk, D.M. Effectiveness of Practices To Increase Timeliness of Providing Targeted Therapy for Inpatients with Bloodstream Infections: A Laboratory Medicine Best Practices Systematic Review and Meta-analysis. Clin. Microbiol. Rev. 2016, 29, 59–103. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; Buetti, N.; Staiquly, Q.; Ruckly, S.; Akova, M.; Aslan, A.T.; Leone, M.; Conway Morris, A.; Bassetti, M.; Arvaniti, K.; et al. Epidemiology and outcomes of hospital-acquired bloodstream infections in intensive care unit patients: The EUROBACT-2 international cohort study. Intensive Care Med. 2023, 49, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, M.; Simone, B.; Filisina, C.; Catalanotto, F.R.; Catalisano, G.; Marino, C.; Misseri, G.; Giarratano, A.; Cortegiani, A. Bloodstream infections in hospitalized patients with COVID-19: A systematic re-view and meta-analysis. Microorganisms 2021, 9, 2016. [Google Scholar] [CrossRef] [PubMed]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef]
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Namendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.N.; Vincent, J.L.; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data From the Intensive Care over Nations Audit. Open Forum Infect. Dis. 2018, 5, ofy313. [Google Scholar] [CrossRef]
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial bloodstream infections in US hospitals: Analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Buetti, N.; Tabah, A.; Loiodice, A.; Ruckly, S.; Aslan, A.T.; Montrucchio, G.; Cortegiani, A.; Saltoglu, N.; Kayaaslan, B.; Aksoy, F.; et al. Different epidemiology of bloodstream infections in COVID-19 compared to non-COVID-19 critically ill patients: A descriptive analysis of the Eurobact II study. Crit. Care 2022, 26, 319. [Google Scholar] [CrossRef]
- Cortegiani, A.; Antonelli, M.; Falcone, M.; Giarratano, A.; Girardis, M.; Leone, M.; Pea, F.; Stefani, S.; Viaggi, B.; Viale, P. Rationale and clinical application of antimicrobial stewardship principles in the intensive care unit: A multidisciplinary statement. J. Anesth. Analg. Crit. Care 2023, 3, 11. [Google Scholar] [CrossRef]
- Tabak, Y.P.; Vankeepuram, L.; Ye, G.; Jeffers, K.; Gupta, V.; Murray, P.R. Blood Culture Turnaround Time in U.S. Acute Care Hospitals and Implications for Laboratory Process Optimization. J. Clin. Microbiol. 2018, 56, e00500-18. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Ippolito, M.; Cortegiani, A. Empirical decision-making for antimicrobial therapy in critically ill patients. BJA Edu. 2023, 23, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Doualeh, M.; Payne, M.; Litton, E.; Raby, E.; Currie, A. Molecular Methodologies for Improved Polymicrobial Sepsis Diagnosis. Int. J. Mol. Sci. 2022, 23, 4484. [Google Scholar] [CrossRef]
- Clancy, C.J.; Nguyen, M.H. T2 magnetic resonance for the diagnosis of bloodstream infections: Charting a path forward. J. Antimicrob. Chemother. 2018, 73 (Suppl. S4), iv2–iv5. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, G.; Posteraro, B.; De Carolis, E.; Menchinelli, G.; Franceschi, F.; Tumbarello, M.; De Pascale, G.; Spanu, T.; Sanguinetti, M. T2Bacteria magnetic resonance assay for the rapid detection of ESKAPEc pathogens directly in whole blood. J. Antimicrob. Chemother. 2018, 73 (Suppl. S4), iv20–iv26. [Google Scholar] [CrossRef]
- Giannella, M.; Pankey, G.A.; Pascale, R.; Miller, V.M.; Miller, L.E.; Seitz, T. Antimicrobial and resource utilization with T2 magnetic resonance for rapid diagnosis of bloodstream infections: Systematic review with meta-analysis of controlled studies. Expert. Rev. Med. Devices 2021, 18, 473–482. [Google Scholar] [CrossRef]
- Lucignano, B.; Cento, V.; Agosta, M.; Ambrogi, F.; Albitar-Nehme, S.; Mancinelli, L.; Mattana, G.; Onori, M.; Galaverna, F.; Di Chiara, L.; et al. Effective Rapid Diagnosis of Bacterial and Fungal Bloodstream Infections by T2 Magnetic Resonance Technology in the Pediatric Population. J. Clin. Microbiol. 2022, 60, e0029222. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Clancy, C.J.; Pasculle, A.W.; Pappas, P.G.; Alangaden, G.; Pankey, G.A.; Schmitt, B.H.; Rasool, A.; Weinstein, M.P.; Widen, R.; et al. Performance of the T2Bacteria Panel for Diagnosing Bloodstream Infections: A Diagnostic Accuracy Study. Ann. Intern. Med. 2019, 170, 845–852. [Google Scholar] [CrossRef]
- Seitz, T.; Holbik, J.; Hind, J.; Gibas, G.; Karolyi, M.; Pawelka, E.; Traugott, M.; Wenisch, C.; Zoufaly, A. Rapid Detection of Bacterial and Fungal Pathogens Using the T2MR versus Blood Culture in Patients with Severe COVID-19. Microbiol. Spectr. 2022, 10, e0014022. [Google Scholar] [CrossRef]
- Timbrook, T.T.; Morton, J.B.; McConeghy, K.W.; Caffrey, A.R.; Mylonakis, E.; LaPlante, K.L. The Effect of Molecular Rapid Diagnostic Testing on Clinical Outcomes in Bloodstream Infections: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2017, 64, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public. Health 2017, 5, 307. [Google Scholar] [CrossRef] [PubMed]
- Diekema, D.J.; Hsueh, P.R.; Mendes, R.E.; Pfaller, M.A.; Rolston, K.V.; Sader, H.S.; Jones, R.N. The Microbiology of Bloodstream Infection: 20-Year Trends from the SENTRY Antimicrobial Surveillance Program. Antimicrob. Agents Chemother. 2019, 63, e00355-19. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | T2B-Positive (n = 35) | T2B-Negative (n = 50) |
|---|---|---|
| Male sex, % | 48.48% | 70% |
| Age, years | 65 (50–73) | 65 (51.5–70.5) |
| Weight, kg | 65 (53.5–77) | 76 (68.75, 87) |
| ICU admission, % | 100% | 100% |
| Max PCT, mcg/L | 1.645 (1.285–43.2) | 5.98 (1.52–18.775) |
| Max lactate, mmol/L | 3.05 (1.475–4.225) | 2.3 (1.55–4.6) |
| Max temp, °C | 36.9 (36.5–38) | 37.75 (36.5–38.95) |
| Max WBC, cells/mm3 | 11,750 (6100–22,575) | 11,600 (7600–18,600) |
| Max HR, bpm | 109 (92.25–120.75) | 102 (86–120) |
| Max RR, bpm | 20.5 (16.75–24.25) | 20.5 (16.5–26.5) |
| Min SBP, mmHg | 95 (90–108.75) | 104 (90–115) |
| Hospital LOS, days | 47 (26.25–65.5) | 26 (13–48) |
| ICU LOS, days | 23.5 (8–57.75) | 13 (5–34) |
| Vasopressor, % | 83.3% | 76% |
| Mechanical ventilation, % | 90% | 88% |
| Mortality, % | 70% | 68% |
| SOFA score, median (IQR) | 12 (7–15) | 10 (6–14) |
| Platelet count, cells/μL | ||
| ≥150,000 | 33% | 54% |
| 149,000–100,000 | 27% | 10% |
| 99,999–50,000 | 17% | 15% |
| 49,999–20,000 | 13% | 12% |
| <20,000 | 10% | 10% |
| PaO2/FiO2, % | ||
| ≥400 mmHg | 13% | 12% |
| 399–300 mmHg | 10% | 15% |
| 299–200 mmHg | 43% | 37% |
| 199–199 mmHg with respiratory support | 27% | 22% |
| <100 mmHg with respiratory support | 7% | 15% |
| Bilirubin, % | ||
| <1.2 mg/dl | 60% | 61% |
| 1.2–1.9 mg/dl | 13% | 20% |
| 2.0–5.9 mg/dl | 17% | 15% |
| 6.0–11.9 mg/dl | 10% | 5% |
| ≥12.0 mg/dl | 0% | 0% |
| Cardiovascular SOFA (MAP/Vasopressors) | ||
| MAP ≥ 70 mmHg | 23% | 29% |
| MAP < 70 mmHg | 0% | 5% |
| Dopamine or dobutamine < 5 mcg/kg/min | 0% | 0% |
| Dopamine 5.1–15 mcg/kg/min or NE/EPI ≤ 0.1 mcg/kg/min | 13% | 15% |
| Dopamine > 15 mcg/kg/min or NE/EPI > 0.1 mcg/kg/min | 63% | 46% |
| Glasgow Coma Score, % | ||
| 15 | 13% | 10% |
| 13–14 | 7% | 0% |
| 10–12 | 7% | 0% |
| 6–9 | 7% | 10% |
| <6 | 67% | 80% |
| Creatinine, % | ||
| <1.2 mg/dl | 37% | 37% |
| 1.2–1.9 mg/dl | 23% | 27% |
| 2.0–3.4 mg/dl | 23% | 15% |
| 3.5–4.9 mg/dl | 13% | 17% |
| ≥5.0 mg/dl | 3% | 5% |
| Sepsis source, % | ||
| Undetermined | 60% | 56% |
| Respiratory | 17% | 22% |
| Urine | 3% | 5% |
| Wound | 3% | 0% |
| Abdominal | 17% | 17% |
| Results | T2Bacteria | BC Simultaneous | BC within +/− 5 Days | OTHER Cultures within +/− 5 Days |
|---|---|---|---|---|
| NEGATIVE | 50 | 41 | ||
| Positive—ESKAPEc | ||||
| E. faecium | 9 | 3 | 1 | 6 |
| S. aureus | 1 | 1 | 0 | 0 |
| K. pneumoniae | 9 | 4 | 4 | 1 |
| A. baumannii | 15 | 7 | 5 | 3 |
| P. aeruginosa | 10 | 5 | 2 | 3 |
| E. coli | 4 | 1 | 1 | 2 |
| Positive—NOT ESKAPEc | ||||
| Enterobacter aerogenes | N/A | 1 | ||
| Enterobacter cloacae | N/A | 1 | ||
| Staphylococcus capitis | N/A | 1 | ||
| Staphylococcus epidermidis | N/A | 1 | ||
| Staphylococcus haemolyticus | N/A | 1 | ||
| Staphylococcus hominis | N/A | 3 | ||
| Stenotrophomonas maltophilia | N/A | 1 | ||
| Candida spp. | N/A | 6 |
| Channel | Sensitivity | Specificity | Sensitivity | Specificity | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| Proven BSI † | Proven and Probable BSI † | Proven, Probable, and Possible BSI † | ||||
| E. faecium | 67% | 91% | 75% | 93% | 91% | 100% |
| S. aureus | 100% | 100% | 100% | 100% | 100% | 100% |
| K. pneumoniae | 100% | 94% | 100% | 99% | 100% | 100% |
| A. baumannii | 100% | 90% | 100% | 96% | 100% | 100% |
| P. aeruginosa | 100% | 94% | 100% | 96% | 100% | 100% |
| E. coli | 100% | 96% | 100% | 98% | 100% | 100% |
| Overall | 95% | 94% | 97% | 97% | 98% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonura, C.; Graceffa, D.; Distefano, S.; De Grazia, S.; Guzman, O.; Bohn, B.; Ippolito, M.; Campanella, S.; Ancona, A.; Caputo, M.; et al. Evaluation of T2 Magnetic Resonance (T2MR®) Technology for the Early Detection of ESKAPEc Pathogens in Septic Patients. Antibiotics 2024, 13, 885. https://doi.org/10.3390/antibiotics13090885
Bonura C, Graceffa D, Distefano S, De Grazia S, Guzman O, Bohn B, Ippolito M, Campanella S, Ancona A, Caputo M, et al. Evaluation of T2 Magnetic Resonance (T2MR®) Technology for the Early Detection of ESKAPEc Pathogens in Septic Patients. Antibiotics. 2024; 13(9):885. https://doi.org/10.3390/antibiotics13090885
Chicago/Turabian StyleBonura, Celestino, Domenico Graceffa, Salvatore Distefano, Simona De Grazia, Oscar Guzman, Brian Bohn, Mariachiara Ippolito, Salvatore Campanella, Angelica Ancona, Marta Caputo, and et al. 2024. "Evaluation of T2 Magnetic Resonance (T2MR®) Technology for the Early Detection of ESKAPEc Pathogens in Septic Patients" Antibiotics 13, no. 9: 885. https://doi.org/10.3390/antibiotics13090885
APA StyleBonura, C., Graceffa, D., Distefano, S., De Grazia, S., Guzman, O., Bohn, B., Ippolito, M., Campanella, S., Ancona, A., Caputo, M., Mirasola, P., Palmeri, C., Raineri, S. M., Giarratano, A., Giammanco, G. M., & Cortegiani, A. (2024). Evaluation of T2 Magnetic Resonance (T2MR®) Technology for the Early Detection of ESKAPEc Pathogens in Septic Patients. Antibiotics, 13(9), 885. https://doi.org/10.3390/antibiotics13090885