
Anti-Staphylococcal Activity of Ligilactobacillus animalis SWLA-1 and Its Supernatant against Multidrug-Resistant Staphylococcus pseudintermedius in Novel Rat Model of Acute Osteomyelitis

 , , ,
, , ,
Abstract
1. Introduction
2. Results
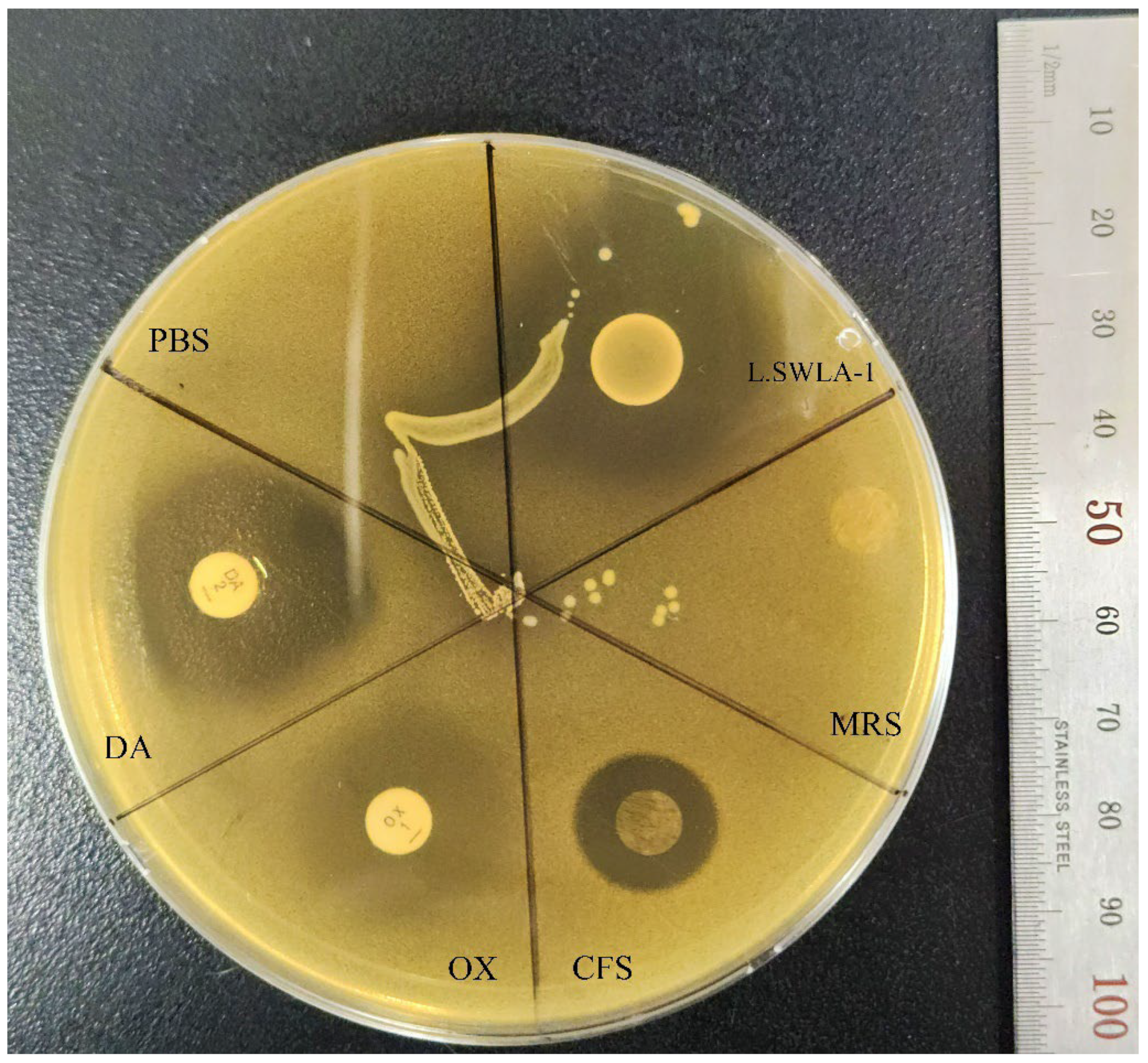
2.1. Antimicrobial Activity of L. animalis SWLA-1 and CFS against MDR Indicator Bacteria
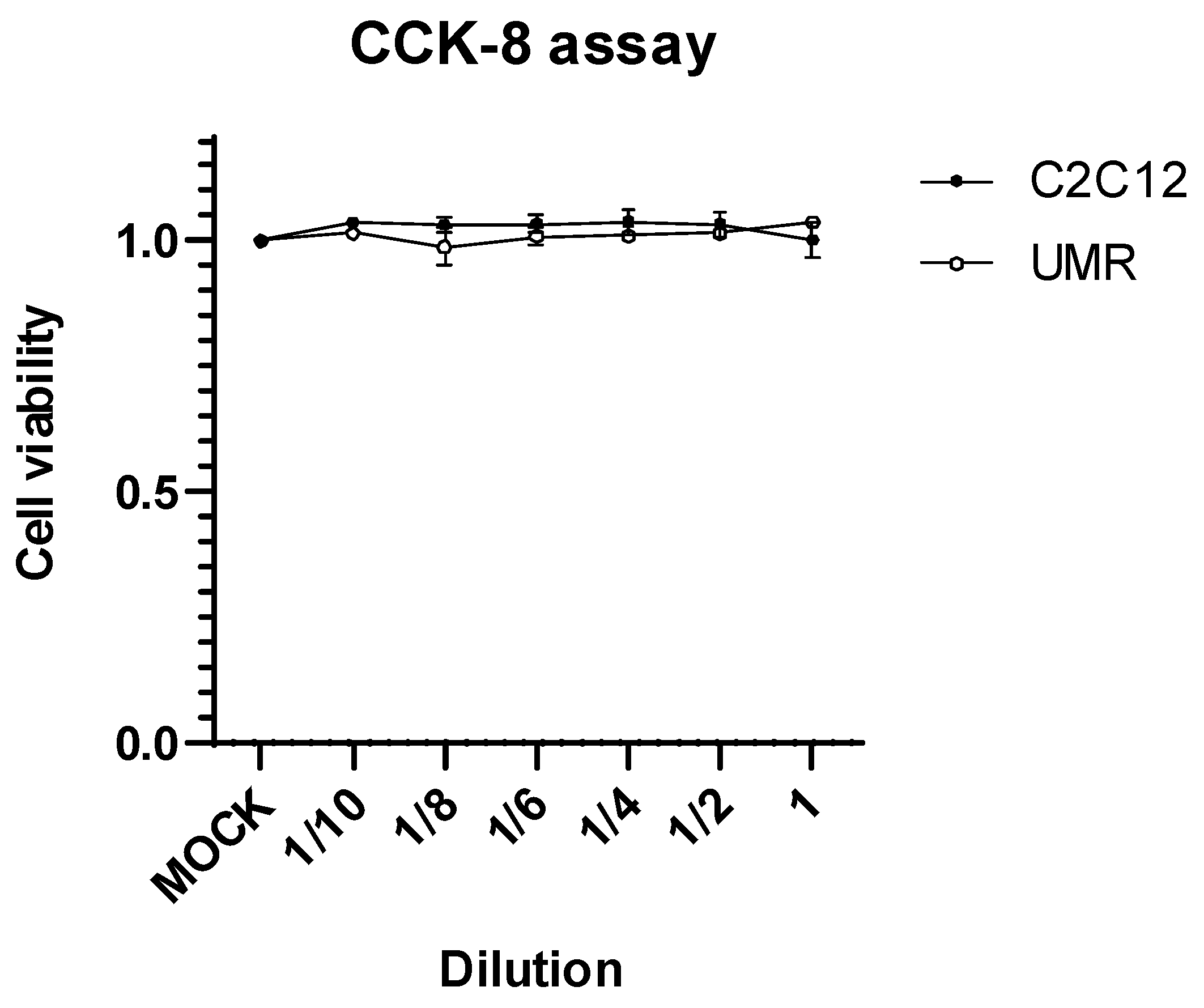
2.2. Cytotoxic Effect on Osteoblast Cell and Myoblast Cell
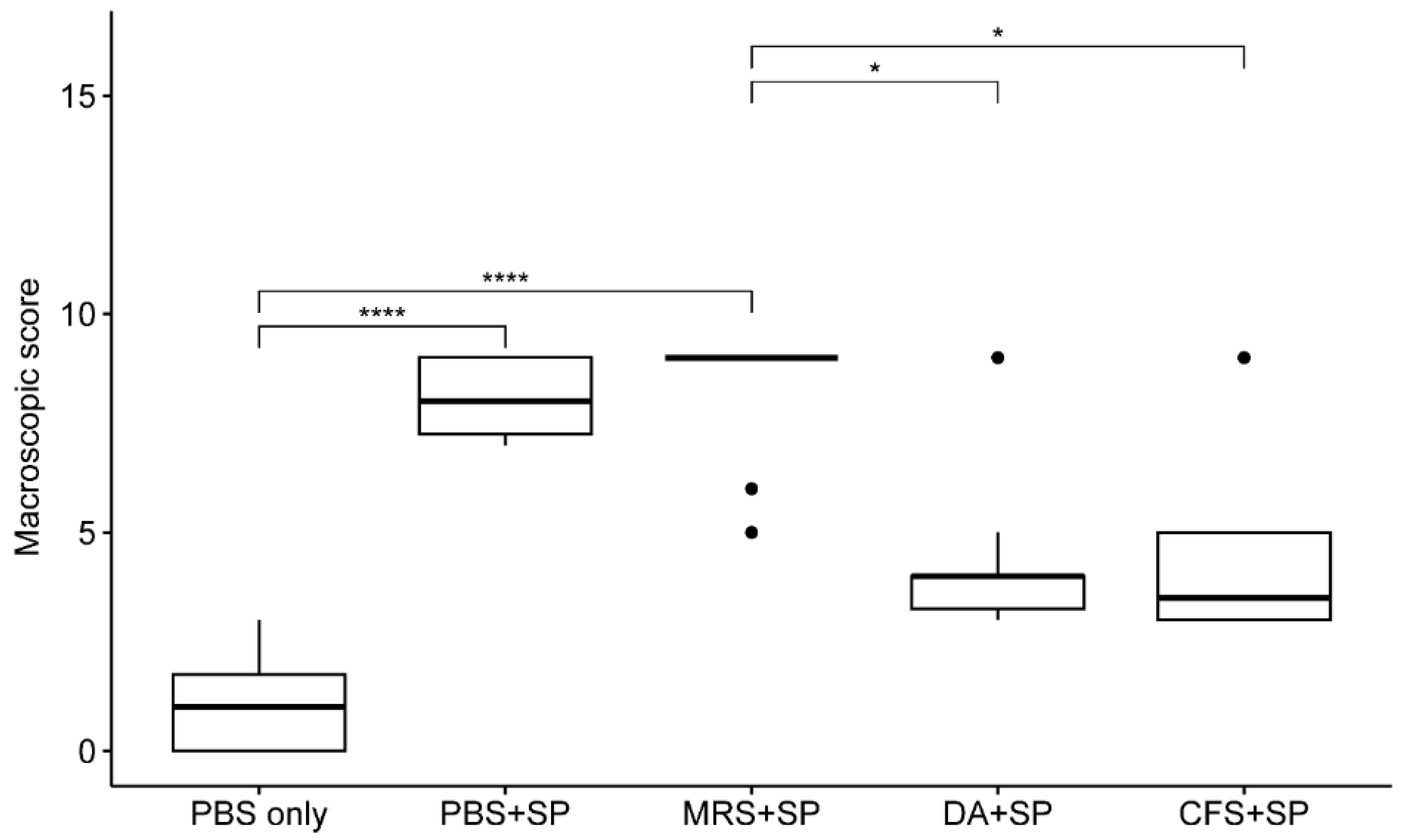
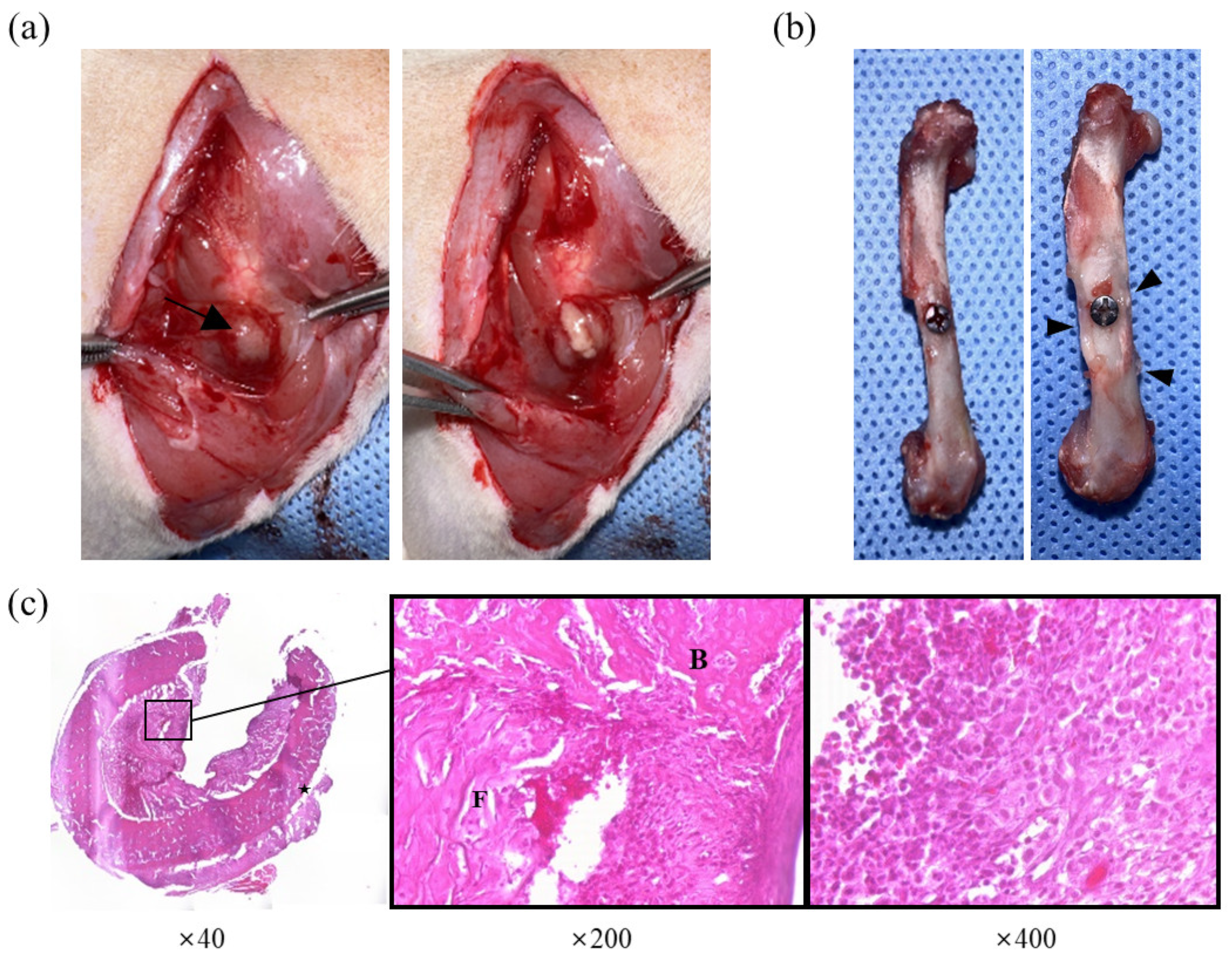
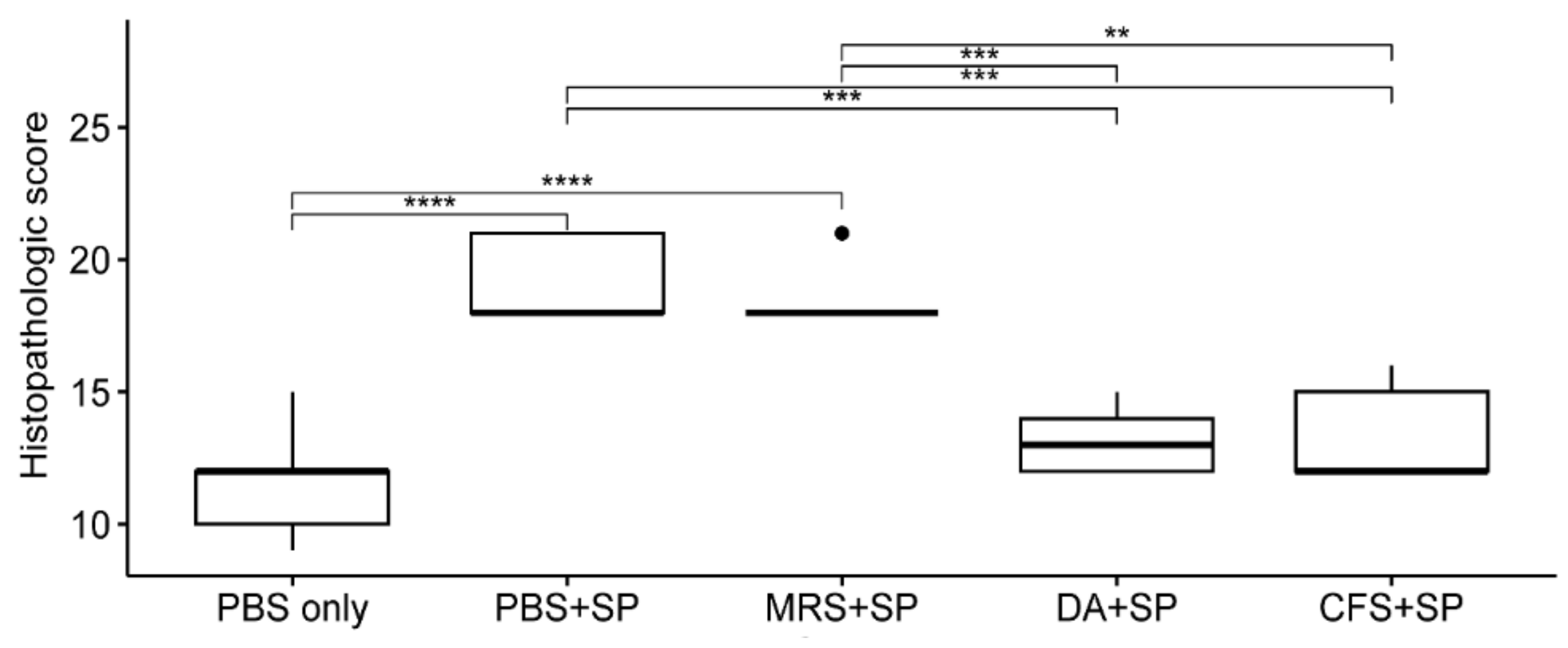
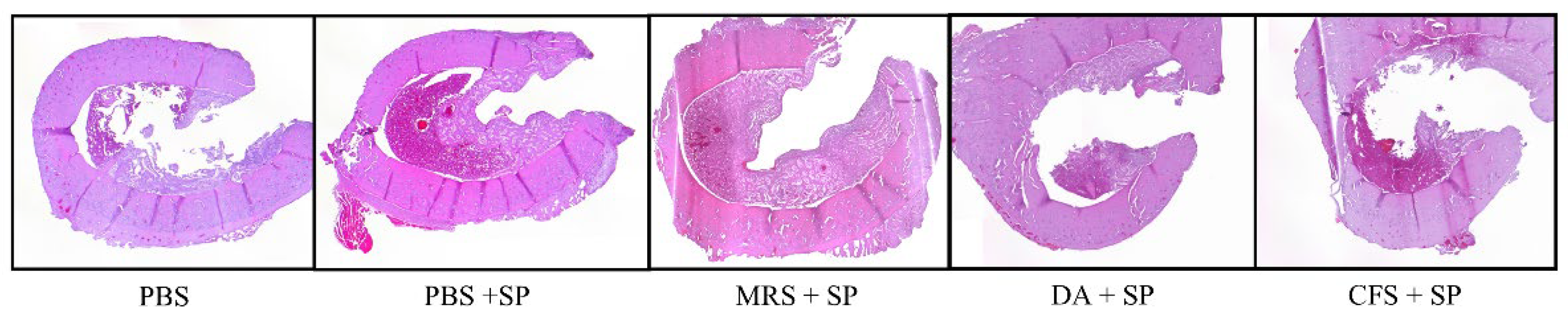
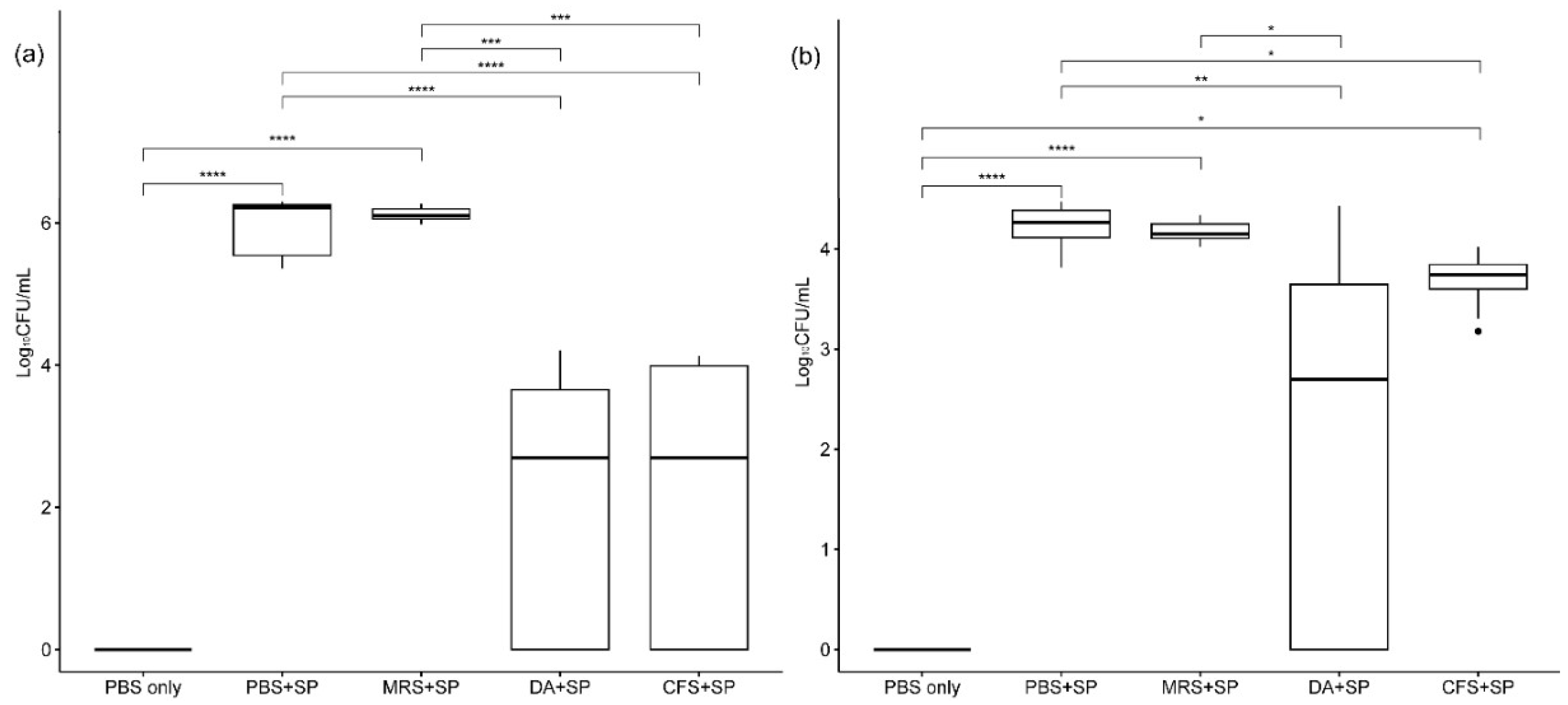
2.3. Antimicrobial Activity of CFS Derived from L. animalis SWLA-1 in Novel Rat Model
3. Discussion
4. Materials and Methods
4.1. Preparation of Bacterial Strains and Crude CFS
4.2. Evaluation of Antimicrobial Activity against MDR Indicator Bacteria
4.3. Cytotoxicity Assay
4.4. Establishment of Novel Acute Osteomyelitis Rat Model Using S. pseudintermedius
4.5. Gross Lesion Evaluation
4.6. Bone Histopathologic Evaluation
4.7. Microbiological Evaluation
4.8. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Giulieri, S.; Graber, P.; Ochsner, P.; Zimmerli, W. Management of infection associated with total hip arthroplasty according to a treatment algorithm. Infection 2004, 32, 222–228. [Google Scholar] [CrossRef]
- Lucke, M.; Schmidmaier, G.; Sadoni, S.; Wildemann, B.; Schiller, R.; Haas, N.; Raschke, M. Gentamicin coating of metallic implants reduces implant-related osteomyelitis in rats. Bone 2003, 32, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zheng, Z.; Zara, J.N.; Hsu, C.; Soofer, D.E.; Lee, K.S.; Siu, R.K.; Miller, L.S.; Zhang, X.; Carpenter, D. The antimicrobial and osteoinductive properties of silver nanoparticle/poly (DL-lactic-co-glycolic acid)-coated stainless steel. Biomaterials 2012, 33, 8745–8756. [Google Scholar] [CrossRef]
- Stewart, S.; Barr, S.; Engiles, J.; Hickok, N.J.; Shapiro, I.M.; Richardson, D.W.; Parvizi, J.; Schaer, T.P. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep: A proof-of-concept study. J. Bone Jt. Surgery. Am. Vol. 2012, 94, 1406. [Google Scholar] [CrossRef] [PubMed]
- Silva, V.; Antão, H.S.; Guimarães, J.; Prada, J.; Pires, I.; Martins, Â.; Maltez, L.; Pereira, J.E.; Capelo, J.L.; Igrejas, G. Efficacy of dalbavancin against MRSA biofilms in a rat model of orthopaedic implant-associated infection. J. Antimicrob. Chemother. 2020, 75, 2182–2187. [Google Scholar] [CrossRef]
- Weese, J.S.; van Duijkeren, E. Methicillin-resistant Staphylococcus aureus and Staphylococcus pseudintermedius in veterinary medicine. Vet. Microbiol. 2010, 140, 418–429. [Google Scholar] [CrossRef]
- Fossum, T.W. Small Animal Surgery E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Frank, L.A.; Loeffler, A. Meticillin-resistant Staphylococcus pseudintermedius: Clinical challenge and treatment options. Vet. Dermatol. 2012, 23, e256–e283. [Google Scholar] [CrossRef] [PubMed]
- Ruscher, C.; Lübke-Becker, A.; Wleklinski, C.-G.; Şoba, A.; Wieler, L.H.; Walther, B. Prevalence of methicillin-resistant Staphylococcus pseudintermedius isolated from clinical samples of companion animals and equidaes. Vet. Microbiol. 2009, 136, 197–201. [Google Scholar] [CrossRef]
- OIE. OIE List of Antimicrobial Agents of Veterinary Importance; World Organization for Animal Health: Paris, France, 2021. [Google Scholar]
- WHO. Critically Important Antimicrobials for Human Medicine, , 6th Revision ed; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Chen, B.; Li, F.; Zhu, X.K.; Xie, W.; Hu, X.; Zan, M.H.; Li, X.; Li, Q.Y.; Guo, S.S.; Zhao, X.Z.; et al. Highly biocompatible and recyclable biomimetic nanoparticles for antibiotic-resistant bacteria infection. Biomater. Sci. 2021, 9, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Kortright, K.E.; Chan, B.K.; Koff, J.L.; Turner, P.E. Phage Therapy: A Renewed Approach to Combat Antibiotic-Resistant Bacteria. Cell Host Microbe 2019, 25, 219–232. [Google Scholar] [CrossRef]
- Soltani, S.; Hammami, R.; Cotter, P.D.; Rebuffat, S.; Said, L.B.; Gaudreau, H.; Bédard, F.; Biron, E.; Drider, D.; Fliss, I. Bacteriocins as a new generation of antimicrobials: Toxicity aspects and regulations. FEMS Microbiol. Rev. 2021, 45, fuaa039. [Google Scholar] [CrossRef]
- Ashrit, P.; Sadanandan, B.; Shetty, K.; Vaniyamparambath, V. Polymicrobial Biofilm Dynamics of Multidrug-Resistant Candida albicans and Ampicillin-Resistant Escherichia coli and Antimicrobial Inhibition by Aqueous Garlic Extract. Antibiotics 2022, 11, 573. [Google Scholar] [CrossRef] [PubMed]
- Hols, P.; Ledesma-García, L.; Gabant, P.; Mignolet, J. Mobilization of Microbiota Commensals and Their Bacteriocins for Therapeutics. Trends Microbiol. 2019, 27, 690–702. [Google Scholar] [CrossRef] [PubMed]
- Kingcha, Y.; Tosukhowong, A.; Zendo, T.; Roytrakul, S.; Luxananil, P.; Chareonpornsook, K.; Valyasevi, R.; Sonomoto, K.; Visessanguan, W. Anti-listeria activity of Pediococcus pentosaceus BCC 3772 and application as starter culture for Nham, a traditional fermented pork sausage. Food Control 2012, 25, 190–196. [Google Scholar] [CrossRef]
- Silva, C.C.G.; Silva, S.P.M.; Ribeiro, S.C. Application of Bacteriocins and Protective Cultures in Dairy Food Preservation. Front. Microbiol. 2018, 9, 594. [Google Scholar] [CrossRef]
- Zhou, Q.; Gu, R.; Li, P.; Lu, Y.; Chen, L.; Gu, Q. Anti-Salmonella mode of action of natural l-phenyl lactic acid purified from Lactobacillus plantarum ZJ316. Appl. Microbiol. Biotechnol. 2020, 104, 5283–5292. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, J.B.; Park, S.Y.; Choi, I.S.; Lee, S.W. Antimicrobial activity of dominant Ligilactobacillus animalis strains in healthy canine feces and their probiotic potential. FEMS Microbiol. Lett. 2022, 369, fnac115. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, J.B.; Park, S.Y.; Choi, I.S.; Lee, S.W. Antimicrobial Activity of Ligilactobacillus animalis SWLA-1 and Its Cell-Free Supernatant against Multidrug-Resistant Bacteria and Its Potential Use as an Alternative to Antimicrobial Agents. Microorganisms 2023, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Reizner, W.; Hunter, J.; O’Malley, N.; Southgate, R.; Schwarz, E.; Kates, S. A systematic review of animal models for Staphylococcus aureus osteomyelitis. Eur. Cells Mater. 2014, 27, 196. [Google Scholar] [CrossRef]
- Patel, M.; Rojavin, Y.; Jamali, A.A.; Wasielewski, S.J.; Salgado, C.J. Animal models for the study of osteomyelitis. Semin. Plast. Surg. 2009, 23, 148–154. [Google Scholar] [CrossRef]
- Roux, K.M.; Cobb, L.H.; Seitz, M.A.; Priddy, L.B. Innovations in osteomyelitis research: A review of animal models. Anim. Models Exp. Med. 2021, 4, 59–70. [Google Scholar]
- Bury, D.C.; Rogers, T.S.; Dickman, M.M. Osteomyelitis: Diagnosis and treatment. Am. Fam. Physician 2021, 104, 395–402. [Google Scholar] [PubMed]
- Pineda, C.; Espinosa, R.; Pena, A. Radiographic imaging in osteomyelitis: The role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin. Plast. Surg. 2009, 23, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Masters, E.A.; Trombetta, R.P.; de Mesy Bentley, K.L.; Boyce, B.F.; Gill, A.L.; Gill, S.R.; Nishitani, K.; Ishikawa, M.; Morita, Y.; Ito, H. Evolving concepts in bone infection: Redefining “biofilm”,“acute vs. chronic osteomyelitis”,“the immune proteome” and “local antibiotic therapy”. Bone Res. 2019, 7, 20. [Google Scholar]
- Gieling, F.; Peters, S.; Erichsen, C.; Richards, R.G.; Zeiter, S.; Moriarty, T.F. Bacterial osteomyelitis in veterinary orthopaedics: Pathophysiology, clinical presentation and advances in treatment across multiple species. Vet. J. 2019, 250, 44–54. [Google Scholar] [PubMed]
- Lonner, J.H.; Desai, P.; Dicesare, P.E.; Steiner, G.; Zuckerman, J.D. The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. JBJS 1996, 78, 1553–1558. [Google Scholar]
- An, Y.H.; Friedman, R.J. Animal models of orthopedic implant infection. J. Investig. Surg. 1998, 11, 139–146. [Google Scholar]
- Harrasser, N.; Gorkotte, J.; Obermeier, A.; Feihl, S.; Straub, M.; Slotta-Huspenina, J.; von Eisenhart-Rothe, R.; Moser, W.; Gruner, P.; de Wild, M. A new model of implant-related osteomyelitis in the metaphysis of rat tibiae. BMC Musculoskelet. Disord. 2016, 17, 152. [Google Scholar]
- Lucke, M.; Schmidmaier, G.; Sadoni, S.; Wildemann, B.; Schiller, R.; Stemberger, A.; Haas, N.; Raschke, M. A new model of implant-related osteomyelitis in rats. J. Biomed. Mater. Res. B 2003, 67, 593–602. [Google Scholar]
- Solberg, B.D.; Gutow, A.P.; Baumgaertner, M.R. Efficacy of gentamycin-impregnated resorbable hydroxyapatite cement in treating osteomyelitis in a rat model. J. Orthop. Trauma 1999, 13, 102–106. [Google Scholar]
- D’Andrea, M.M.; Fraziano, M.; Thaller, M.C.; Rossolini, G.M. The Urgent Need for Novel Antimicrobial Agents and Strategies to Fight Antibiotic Resistance. Antibiotics 2019, 8, 254. [Google Scholar] [CrossRef]
- Fungwithaya, P.; Sontigun, N.; Boonhoh, W.; Boonchuay, K.; Wongtawan, T. Antimicrobial resistance in Staphylococcus pseudintermedius on the environmental surfaces of a recently constructed veterinary hospital in Southern Thailand. Vet. World 2022, 15, 1087–1096. [Google Scholar] [CrossRef]
- Lord, J.; Millis, N.; Jones, R.D.; Johnson, B.; Kania, S.A.; Odoi, A. Patterns of antimicrobial, multidrug and methicillin resistance among Staphylococcus spp. isolated from canine specimens submitted to a diagnostic laboratory in Tennessee, USA: A descriptive study. BMC Vet. Res. 2022, 18, 91. [Google Scholar] [CrossRef]
- Bampidis, V.; Azimonti, G.; Bastos, M.L.; Christensen, H.; Dusemund, B.; Fašmon Durjava, M.; Kouba, M.; López-Alonso, M.; López-Puente, S.; Marcon, F.; et al. Safety and efficacy of a feed additive consisting on Ligilactobacillus animalis ATCC PTA-6750 (formerly Lactobacillus animalis) for all animal species (Chr. Hansen A/S). EFSA J. Eur. Food Saf. Auth. 2021, 19, e06469. [Google Scholar] [CrossRef]
- Rissing, J.P.; Buxton, T.; Weinstein, R.; Shockley, R. Model of experimental chronic osteomyelitis in rats. Infect. Immun. 1985, 47, 581–586. [Google Scholar]
- Fukushima, N.; Yokoyama, K.; Sasahara, T.; Dobashi, Y.; Itoman, M. Establishment of rat model of acute staphylococcal osteomyelitis: Relationship between inoculation dose and development of osteomyelitis. Arch. Orthop. Trauma Surg. 2005, 125, 169–176. [Google Scholar]
- Akiyama, T.; Miyamoto, H.; Yonekura, Y.; Tsukamoto, M.; Ando, Y.; Noda, I.; Sonohata, M.; Mawatari, M. Silver oxide-containing hydroxyapatite coating has in vivo antibacterial activity in the rat tibia. J. Orthop. Res. 2013, 31, 1195–1200. [Google Scholar] [PubMed]
- Blaha, J.D.; Calhoun, J.H.; Nelson, C.L.; Henry, S.L.; Seligson, D.; Esterhai, J.L., Jr.; Heppenstall, R.B.; Mader, J.; Evans, R.P.; Wilkins, J. Comparison of the clinical efficacy and tolerance of gentamicin PMMA beads on surgical wire versus combined and systemic therapy for osteomyelitis. Clin. Orthop. Relat. Res. 1993, 295, 8–12. [Google Scholar]
- Hettfleisch, J.; Schöttle, H. Local preventive antibiotic treatment in intramedullary nailing with gentamycin impregnated biomaterials. Aktuelle Traumatol. 1993, 23, 68–71. [Google Scholar]
- Nelson, C.L.; Hickmon, S.G.; Harrison, B.H. Elution characteristics of gentamicin-PMMA beads after implantation in humans. Orthopedics 1994, 17, 415–416. [Google Scholar] [CrossRef] [PubMed]
- Wahlig, H.; Dingeldein, E. Antibiotics and bone cements: Experimental and clinical long-term observations. Acta Orthop. Scand. 1980, 51, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.E.; Vogely, H.C.; Hoepelman, A.I.; Peters, E.J. ‘To bead or not to bead?’Treatment of osteomyelitis and prosthetic joint-associated infections with gentamicin bead chains. Int. J. Antimicrob. Agents 2011, 38, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Romanò, C.L.; Scarponi, S.; Gallazzi, E.; Romanò, D.; Drago, L. Antibacterial coating of implants in orthopaedics and trauma: A classification proposal in an evolving panorama. J. Orthop. Surg. Res. 2015, 10, 157. [Google Scholar] [CrossRef]
- Schmidmaier, G.; Lucke, M.; Wildemann, B.; Haas, N.P.; Raschke, M. Prophylaxis and treatment of implant-related infections by antibiotic-coated implants: A review. Injury 2006, 37, S105–S112. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.H.; Zendo, T.; Sonomoto, K. Novel bacteriocins from lactic acid bacteria (LAB): Various structures and applications. Microb. Cell Factories 2014, 13 (Suppl. 1), S3. [Google Scholar] [CrossRef]
- Stemberger, A.; Grimm, H.; Bader, F.; Rahn, H.; Ascherl, R. Local treatment of bone and soft tissue infections with the collagen-gentamicin sponge. Eur. J. Surgery. Suppl. Acta Chir. Suppl. 1997, 578, 17–26. [Google Scholar]
- FDA. Oral Dosage Form New Animal Drugs; Clindamycin 67 FR 54954; Food and Drug Administration: Silver Spring, MA, USA, 2002. [Google Scholar]
- Lavy, E.; Ziv, G.; Shem-Tov, M.; Glickman, A.; Dey, A. Pharmacokinetics of clindamycin HCl administered intravenously, intramuscularly and subcutaneously to dogs. J. Vet. Pharmacol. Ther. 1999, 22, 261–265. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Number of Rats | Challenge | Treatment |
|---|---|---|---|
| Group 1 | 10 | PBS | PBS |
| Group 2 | 10 | Staphylococcus pseudintermedius (9 × 104 CFU) | PBS |
| Group 3 | 10 | Staphylococcus pseudintermedius (9 × 104 CFU) | Sterile MRS broth |
| Group 4 | 10 | Staphylococcus pseudintermedius (9 × 104 CFU) | Clindamycin (11 mg/kg) |
| Group 5 | 10 | Staphylococcus pseudintermedius (9 × 104 CFU) | Concentrated CFS of L. animalis SWLA-1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-Y.; Lee, H.-J.; Kim, H.-S.; Kim, D.-H.; Lee, S.-W.; Yoon, H.-Y. Anti-Staphylococcal Activity of Ligilactobacillus animalis SWLA-1 and Its Supernatant against Multidrug-Resistant Staphylococcus pseudintermedius in Novel Rat Model of Acute Osteomyelitis. Antibiotics 2023, 12, 1444. https://doi.org/10.3390/antibiotics12091444
Park S-Y, Lee H-J, Kim H-S, Kim D-H, Lee S-W, Yoon H-Y. Anti-Staphylococcal Activity of Ligilactobacillus animalis SWLA-1 and Its Supernatant against Multidrug-Resistant Staphylococcus pseudintermedius in Novel Rat Model of Acute Osteomyelitis. Antibiotics. 2023; 12(9):1444. https://doi.org/10.3390/antibiotics12091444
Chicago/Turabian StylePark, Sung-Yong, Hong-Jae Lee, Hyo-Sung Kim, Dong-Hwi Kim, Sang-Won Lee, and Hun-Young Yoon. 2023. "Anti-Staphylococcal Activity of Ligilactobacillus animalis SWLA-1 and Its Supernatant against Multidrug-Resistant Staphylococcus pseudintermedius in Novel Rat Model of Acute Osteomyelitis" Antibiotics 12, no. 9: 1444. https://doi.org/10.3390/antibiotics12091444
APA StylePark, S.-Y., Lee, H.-J., Kim, H.-S., Kim, D.-H., Lee, S.-W., & Yoon, H.-Y. (2023). Anti-Staphylococcal Activity of Ligilactobacillus animalis SWLA-1 and Its Supernatant against Multidrug-Resistant Staphylococcus pseudintermedius in Novel Rat Model of Acute Osteomyelitis. Antibiotics, 12(9), 1444. https://doi.org/10.3390/antibiotics12091444