

The Interaction of Two Widely Used Endodontic Irrigants, Chlorhexidine and Sodium Hypochlorite, and Its Impact on the Disinfection Protocol during Root Canal Treatment



Abstract
1. Introduction
1.1. Sodium Hypochlorite (NaOCl)
1.2. Chlorhexidine (CHX)
1.3. Proteolysis
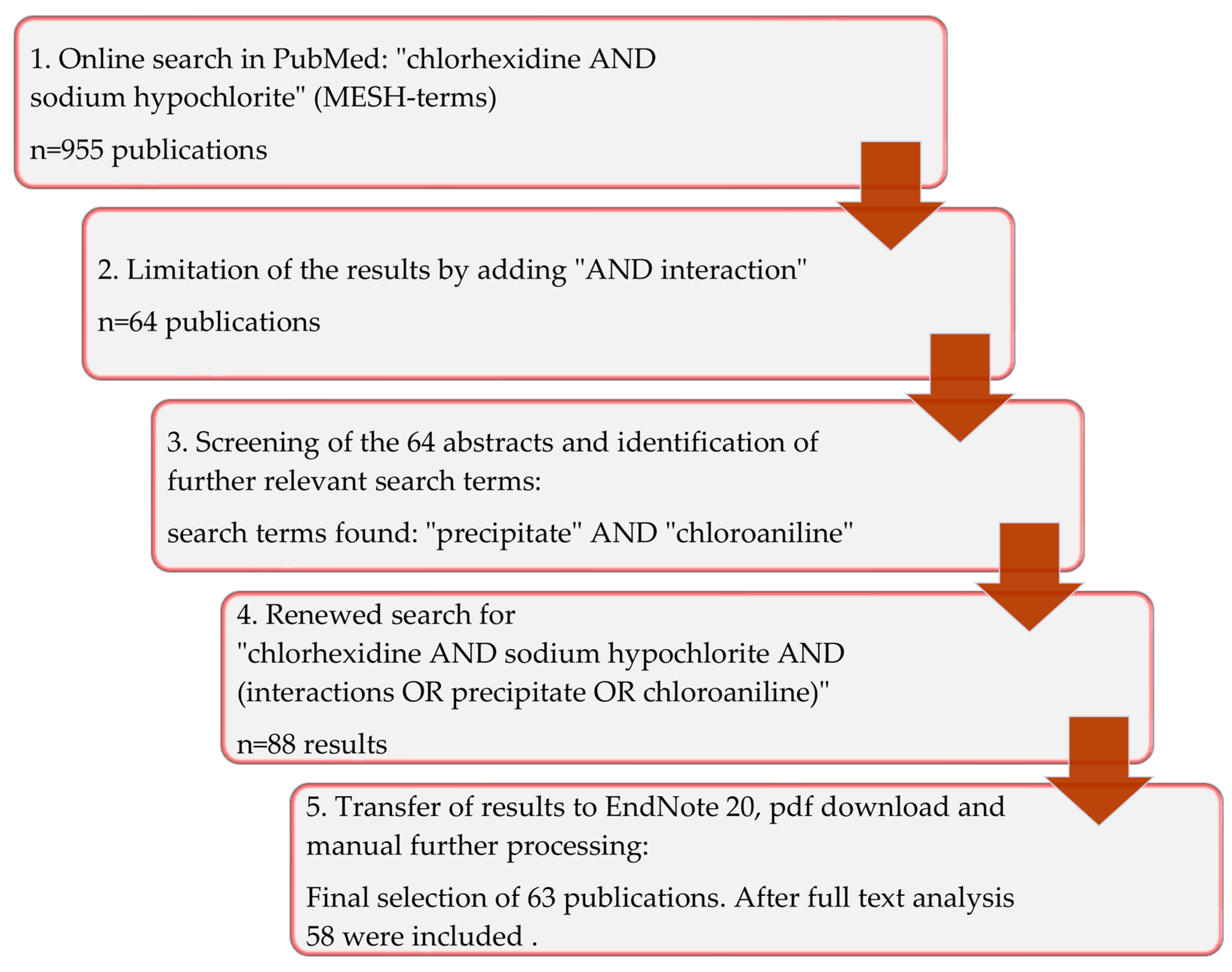
2. Materials and Methods
3. Results
4. Discussion
4.1. Methodology
4.2. Toxicity
4.3. Recommended Irrigation Protocol
4.4. Alternative Irrigation Solutions
4.5. Clinical Impact on Endodontic Therapy
- -
- Dissolution of necrotic and vital tissue;
- -
- Effectiveness against bacteria;
- -
- Effectiveness against fungi;
- -
- Neutralization of endotoxins;
- -
- Opening of the dentinal tubules;
- -
- Removal of iatrogenic impurities;
- -
- Economic efficiency;
- -
- Practicality.
- -
- Irritation of neighboring tissues;
- -
- Cytotoxicity;
- -
- Mutagenicity;
- -
- Changes in the color of dentin or tooth enamel;
- -
- Occlusion of the dentinal tubules;
- -
- Undesirable interactions with other endodontic irrigating solutions and materials.
5. Conclusions
- -
- The chemo-mechanical preparation of the root canal system is currently the gold standard;
- -
- NaOCl should be used as the sole agent during mechanical reprocessing, due to its tissue-dissolving and antimicrobial properties;
- -
- The smear layer can be removed with CA or EDTA after the mechanical preparation. NaOCl should not be mixed with CA or EDTA, since chelators neutralize the tissue-dissolving effect of NaOCl;
- -
- The consecutive use of NaOCl and CHX is obsolete due to the precipitate that forms;
- -
- If NaOCl and CHX (or CHX derivatives) are used in the same tooth, intermediate rinsing is required. Since CHX also forms a precipitate with EDTA, CA is recommended for this.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kandaswamy, D.; Venkateshbabu, N. Root canal irrigants. J Conserv. Dent. 2010, 13, 256–264. [Google Scholar] [CrossRef]
- Kojima, K.; Inamoto, K.; Nagamatsu, K.; Hara, A.; Nakata, K.; Morita, I.; Nakagaki, H.; Nakamura, H. Success rate of endodontic treatment of teeth with vital and nonvital pulps: A meta-analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 97, 95–99. [Google Scholar] [CrossRef]
- Abou-Rass, M.; Piccinino, M.V. The effectiveness of four clinical irrigation methods on the removal of root canal debris. Oral Surg. Oral Med. Oral Pathol. 1982, 54, 323–328. [Google Scholar] [CrossRef]
- Bystrom, A.; Sundqvist, G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand. J. Dent. Res. 1981, 89, 321–328. [Google Scholar] [CrossRef]
- Zehnder, M. Root canal irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef]
- Gomes, B.P.; Vianna, M.E.; Zaia, A.A.; Almeida, J.F.; Souza-Filho, F.J.; Ferraz, C.C. Chlorhexidine in endodontics. Braz. Dent. J. 2013, 24, 89–102. [Google Scholar] [CrossRef]
- Wright, P.P.; Kahler, B.; Walsh, L.J. Alkaline Sodium Hypochlorite Irrigant and Its Chemical Interactions. Materials 2017, 10, 1147. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- Good, M.; El, K.I.; Hussey, D.L. Endodontic ‘solutions’ part 1: A literature review on the use of endodontic lubricants, irrigants and medicaments. Dent. Update 2012, 39, 239–240. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Arias-Moliz, M.T. Present status and future directions—Irrigants and irrigation methods. Int. Endod. J. 2022, 55 (Suppl. S3), 588–612. [Google Scholar] [CrossRef] [PubMed]
- Basrani, B.R.; Manek, S.; Sodhi, R.N.; Fillery, E.; Manzur, A. Interaction between sodium hypochlorite and chlorhexidine gluconate. J. Endod. 2007, 33, 966–969. [Google Scholar] [CrossRef] [PubMed]
- Akisue, E.; Tomita, V.S.; Gavini, G.; Poli de Figueiredo, J.A. Effect of the combination of sodium hypochlorite and chlorhexidine on dentinal permeability and scanning electron microscopy precipitate observation. J. Endod. 2010, 36, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Mortenson, D.; Sadilek, M.; Flake, N.M.; Paranjpe, A.; Heling, I.; Johnson, J.D.; Cohenca, N. The effect of using an alternative irrigant between sodium hypochlorite and chlorhexidine to prevent the formation of para-chloroaniline within the root canal system. Int. Endod. J. 2012, 45, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Nocca, G.; Ahmed, H.M.A.; Martorana, G.E.; Callà, C.; Gambarini, G.; Rengo, S.; Spagnuolo, G. Chromographic Analysis and Cytotoxic Effects of Chlorhexidine and Sodium Hypochlorite Reaction Mixtures. J. Endod. 2017, 43, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, N.; Gangaramani, S.; Singbal, K.P.; Desai, K.; Gupta, K. Efficacy of various solutions in preventing orange-brown precipitate formed during alternate use of sodium hypochlorite and chlorhexidine: An in vitro study. J. Conserv. Dent. 2018, 21, 428–432. [Google Scholar] [CrossRef]
- Siddique, R.; Sureshbabu, N.M.; Somasundaram, J.; Jacob, B.; Selvam, D. Qualitative and quantitative analysis of precipitate formation following interaction of chlorhexidine with sodium hypochlorite, neem, and tulsi. J. Conserv. Dent. 2019, 22, 40–47. [Google Scholar] [CrossRef]
- Estrela, C.; Estrela, C.R.; Barbin, E.L.; Spano, J.C.; Marchesan, M.A.; Pecora, J.D. Mechanism of action of sodium hypochlorite. Braz. Dent. J. 2002, 13, 113–117. [Google Scholar] [CrossRef]
- Cullen, J.K.; Wealleans, J.A.; Kirkpatrick, T.C.; Yaccino, J.M. The effect of 8.25% sodium hypochlorite on dental pulp dissolution and dentin flexural strength and modulus. J. Endod. 2015, 41, 920–924. [Google Scholar] [CrossRef]
- Hulsmann, M.; Hahn, W. Complications during root canal irrigation—Literature review and case reports. Int. Endod. J. 2000, 33, 186–193. [Google Scholar] [CrossRef]
- Karkare, S.R.; Ahire, N.P.; Khedkar, S.U. Comparative evaluation of antimicrobial activity of hydroalcoholic extract of Aloe vera, garlic, and 5% sodium hypochlorite as root canal irrigants against Enterococcus faecalis: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2015, 33, 274–278. [Google Scholar] [CrossRef]
- Gernhardt, C.R.; Eppendorf, K.; Kozlowski, A.; Brandt, M. Toxicity of concentrated sodium hypochlorite used as an endodontic irrigant. Int. Endod. J. 2004, 37, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, H.; Sultan, N.; Cirak, M.; Ruhi, M.Z.; Bodur, H. Antimicrobial effects of various endodontic irrigants on selected microorganisms. Int. Endod. J. 1999, 32, 99–102. [Google Scholar] [CrossRef]
- Ercan, E.; Ozekinci, T.; Atakul, F.; Gul, K. Antibacterial activity of 2% chlorhexidine gluconate and 5.25% sodium hypochlorite in infected root canal: In vivo study. J. Endod. 2004, 30, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Rocas, I.N.; Siqueira, J.F., Jr. Comparison of the in vivo antimicrobial effectiveness of sodium hypochlorite and chlorhexidine used as root canal irrigants: A molecular microbiology study. J. Endod. 2011, 37, 143–150. [Google Scholar] [CrossRef]
- Klein, U.; Kleier, D.J. Sodium hypochlorite accident in a pediatric patient. Pediatr. Dent. 2013, 35, 534–538. [Google Scholar]
- Peters, O.A.; Paqué, F. Root canal preparation of maxillary molars with the self-adjusting file: A micro-computed tomography study. J. Endod. 2011, 37, 53–57. [Google Scholar] [CrossRef]
- Gomes, B.P.; Martinho, F.C.; Vianna, M.E. Comparison of 2.5% sodium hypochlorite and 2% chlorhexidine gel on oral bacterial lipopolysaccharide reduction from primarily infected root canals. J. Endod. 2009, 35, 1350–1353. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, A.; Teixeira, C.S. The properties of chlorhexidine and undesired effects of its use in endodontics. Quintessence Int. 2015, 46, 575–582. [Google Scholar] [CrossRef]
- Vivacqua-Gomes, N.; Ferraz, C.C.; Gomes, B.P.; Zaia, A.A.; Teixeira, F.B.; Souza-Filho, F.J. Influence of irrigants on the coronal microleakage of laterally condensed gutta-percha root fillings. Int. Endod. J. 2002, 35, 791–795. [Google Scholar] [CrossRef]
- Bui, T.B.; Baumgartner, J.C.; Mitchell, J.C. Evaluation of the interaction between sodium hypochlorite and chlorhexidine gluconate and its effect on root dentin. J. Endod. 2008, 34, 181–185. [Google Scholar] [CrossRef]
- Kim, J.W. Precipitate from a combination of sodium hypochlorite and chlorhexidine. Restor. Dent. Endod. 2012, 37, 185–186. [Google Scholar] [CrossRef]
- Keles, A.; Ors, S.A.; Yilmaz, Z. Effect of various solutions on the removal of orange-brown precipitate formed by interaction of sodium hypochlorite and chlorhexidine with or without ultrasonic activationZ. Niger. J. Clin. Pract. 2020, 23, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Khatib, M.S.; Ameer, B.; Ajit Mannur, N.; Ramalingaiahsetty, A.M.; Peerzade, S.M.; Bambawale, A. Decoding the Perplexing Mystery of Para-Chloroaniline Formation: A Systematic Review. J. Int. Soc. Prev. Community Dent. 2020, 10, 142–147. [Google Scholar] [CrossRef]
- Bueso, V.; Parikh, N.; Terlier, T.; Holland, J.N.; Sarmast, N.D.; Jeong, J.W. Comparative evaluation of intermediate solutions in prevention of brown precipitate formed from sodium hypochlorite and chlorhexidine gluconate. Clin. Exp. Dent. Res. 2022, 8, 1591–1597. [Google Scholar] [CrossRef]
- Jeong, J.W.; Sarmast, N.D.; Terlier, T.; van der Hoeven, R.; Holland, J.N.; Parikh, N. Assessment of the cytotoxic effects and chemical composition of the insoluble precipitate formed from sodium hypochlorite and chlorhexidine gluconate. Int. Endod. J. 2021, 54, 1892–1901. [Google Scholar] [CrossRef]
- Czopik, B.; Ciechomska, M.; Zarzecka, J.; Góra, M.; Woźniakiewicz, M. Insight into the Reaction of Alexidine with Sodium Hypochlorite: A Potential Error in Endodontic Treatment. Molecules 2021, 26, 1623. [Google Scholar] [CrossRef]
- Alberto, A.P.L.; Oliveira, D.D.S.; Oliveira, H.E.; Maciel, A.C.C.; Belladonna, F.G.; Silva, E. Does sodium thiosulphate avoid the formation of the brown-coloured precipitate as an intermediate irrigant between NaOCl and chlorhexidine? Aust. Endod. J. 2022, 48, 72–76. [Google Scholar] [CrossRef]
- Buyukozer Ozkan, H.; Terlemez, A.; Orhan, E.O. Proton Nuclear Magnetic Resonance Spectroscopy Analysis of Mixtures of Chlorhexidine with Different Oxidizing Agents Activated by Photon-Induced Photoacoustic Streaming for Root Canal Irrigation. Photobiomodul. Photomed. Laser Surg. 2020, 38, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Abusteit, O.E. Evaluation of resin sealer penetration of dentin following different final rinses for endodontic irrigation using confocal laser scanning microscopy. Aust. Endod. J. 2020, 47, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Abu Zeid, S.T.; Alamoudi, R.A.; Merdad, K. Morphological and chemical analysis of surface interaction of irrigant-endosequence root repair material. J. Biomed. Mater. Res. B Appl. Biomater. 2020, 108, 3383–3392. [Google Scholar] [CrossRef]
- Thomas, A.R.; Mani, R.; Reddy, T.V.; Ravichandran, A.; Sivakumar, M.; Krishnakumar, S. Evaluation of the Antibacterial Efficiency of a Combination of 1% Alexidine and Sodium Hypochlorite on Enterococcus faecalis Biofilm Models: An In Vitro Study. J. Contemp. Dent. Pract. 2019, 20, 1090–1094. [Google Scholar] [CrossRef] [PubMed]
- Siddique, R.; Nivedhitha, M.S.; Jacob, B. Quantitative analysis for detection of toxic elements in various irrigants, their combination (precipitate), and para-chloroaniline: An inductively coupled plasma mass spectrometry study. J. Conserv. Dent. 2019, 22, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Žižka, R.; Šedý, J.; Gregor, L.; Voborná, I. Discoloration after Regenerative Endodontic Procedures: A Critical Review. Iran. Endod. J. 2018, 13, 278–284. [Google Scholar] [CrossRef]
- Ravinanthanan, M.; Hegde, M.N.; Shetty, V.; Kumari, S. Cytotoxicity Evaluation of Combination Irrigant Regimens with MTAD on Two Different Cell Lines. Contemp. Clin. Dent. 2018, 9, 255–259. [Google Scholar] [CrossRef]
- Piperidou, M.; Sodhi, R.N.S.; Kolosowski, K.P.; Basrani, B.R. Effects of Final Irrigation with SmearOFF on the Surface of Dentin Using Surface Analytical Methods. J. Endod. 2018, 44, 1714–1719. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.; Agarwal, P.; Jain, S.; Seal, M.; Adlakha, T. Alexidine versus chlorhexidine for endodontic irrigation with sodium hypochlorite. Eur. J. Dent. 2018, 12, 398–402. [Google Scholar] [CrossRef]
- Irmak, Ö.; Orhan, E.O.; Görgün, K.; Yaman, B.C. Nuclear magnetic resonance spectroscopy and infrared spectroscopy analysis of precipitate formed after mixing sodium hypochlorite and QMix 2in1. PLoS ONE 2018, 13, e0202081. [Google Scholar] [CrossRef]
- Gonzalez, C.; Forner, L.; Llena, C.; Lozano, A. Temperature changes in 2% chlorhexidine gluconate using two activation methods with different intensity levels. J. Clin. Exp. Dent. 2018, 10, e458–e461. [Google Scholar] [CrossRef]
- Campbell, S.T.; Goodnough, L.H.; Bennett, C.G.; Giori, N.J. Antiseptics Commonly Used in Total Joint Arthroplasty Interact and May Form Toxic Products. J. Arthroplasty 2018, 33, 844–846. [Google Scholar] [CrossRef]
- Thaha, K.A.; Varma, R.L.; Nair, M.G.; Sam Joseph, V.G.; Krishnan, U. Interaction between Octenidine-based Solution and Sodium Hypochlorite: A Mass Spectroscopy, Proton Nuclear Magnetic Resonance, and Scanning Electron Microscopy-based Observational Study. J. Endod. 2017, 43, 135–140. [Google Scholar] [CrossRef]
- Surender, L.R.; Shikha, A.; Swathi, A.; Manaswini, C.; Habeeb, A.; Prabha, S.S. Alexidine: A Safer and an Effective Root Canal Irrigant than Chlorhexidine. J. Clin. Diagn. Res. 2017, 11, ZC18–ZC21. [Google Scholar] [CrossRef]
- Guneser, M.B.; Dincer, A.N.; Arslan, D. Comparison of Conventional Syringe, CanalBrush, EndoActivator, Photon-Induced Photoacoustic Streaming, and Manual Instrumentation in Removing Orange-Brown Precipitate: An In Vitro Study. Photomed. Laser Surg. 2017, 35, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Vouzara, T.; Koulaouzidou, E.; Ziouti, F.; Economides, N. Combined and independent cytotoxicity of sodium hypochlorite, ethylenediaminetetraacetic acid and chlorhexidine. Int. Endod. J. 2016, 49, 764–773. [Google Scholar] [CrossRef]
- Patil, P.; Aminoshariae, A.; Harding, J.; Montagnese, T.A.; Mickel, A. Determination of mutagenicity of the precipitate formed by sodium hypochlorite and chlorhexidine using the Ames test. Aust. Endod. J. 2016, 42, 16–21. [Google Scholar] [CrossRef]
- Orhan, E.O.; Irmak, Ö.; Hür, D.; Yaman, B.C.; Karabucak, B. Does Para-chloroaniline Really Form after Mixing Sodium Hypochlorite and Chlorhexidine? J. Endod. 2016, 42, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, Z.; Giardino, L.; Palazzi, F.; Asgary, S. Agonistic and Antagonistic Interactions between Chlorhexidine and Other Endodontic Agents: A Critical Review. Iran. Endod. J. 2015, 10, 1–5. [Google Scholar] [PubMed]
- Metri, M.; Hegde, S.; Dinesh, K.; Indiresha, H.N.; Nagaraj, S.; Bhandi, S.H. Comparative Evaluation of Two Final Irrigation Techniques for the Removal of Precipitate Formed by the Interaction between Sodium Hypochlorite and Chlorhexidine. J. Contemp. Dent. Pract. 2015, 16, 850–853. [Google Scholar] [CrossRef] [PubMed]
- Magro, M.G.; Kuga, M.C.; Aranda-Garcia, A.J.; Victorino, K.R.; Chávez-Andrade, G.M.; Faria, G.; Keine, K.C.; Só, M.V. Effectiveness of several solutions to prevent the formation of precipitate due to the interaction between sodium hypochlorite and chlorhexidine and its effect on bond strength of an epoxy-based sealer. Int. Endod. J. 2015, 48, 478–483. [Google Scholar] [CrossRef]
- Arslan, H.; Uygun, A.D.; Keskin, A.; Karatas, E.; Seçkin, F.; Yıldırım, A. Evaluation of orange-brown precipitate formed in root canals after irrigation with chlorhexidine and QMix and spectroscopic analysis of precipitates produced by a mixture of chlorhexidine/NaOCl and QMix/NaOCl. Int. Endod. J. 2015, 48, 1199–1203. [Google Scholar] [CrossRef]
- Kolosowski, K.P.; Sodhi, R.N.; Kishen, A.; Basrani, B.R. Qualitative analysis of precipitate formation on the surface and in the tubules of dentin irrigated with sodium hypochlorite and a final rinse of chlorhexidine or QMiX. J. Endod. 2014, 40, 2036–2040. [Google Scholar] [CrossRef]
- Homayouni, H.; Majd, N.M.; Zohrehei, H.; Mosavari, B.; Adel, M.; Dajmar, R.; Homayouni, A. The Effect of Root Canal Irrigation with Combination of Sodium Hypo-chlorite and Chlorhexidine Gluconate on the Sealing Ability of Obturation Materials. Open Dent. J. 2014, 8, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.M.; Kuga, M.C.; Regina Victorino, K.; Vazquez-Garcia, F.A.; Aranda-Garcia, A.J.; Faria-Junior, N.B.; Faria, G.; Luis Shinohara, A. Evaluation of the interaction between sodium hypochlorite and several formulations containing chlorhexidine and its effect on the radicular dentin—SEM and push-out bond strength analysis. Microsc. Res. Tech. 2014, 77, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Cintra, L.T.; Watanabe, S.; Samuel, R.O.; da Silva Facundo, A.C.; de Azevedo Queiroz, I.O.; Dezan-Júnior, E.; Gomes-Filho, J.E. The use of NaOCl in combination with CHX produces cytotoxic product. Clin. Oral Investig. 2014, 18, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Arslan, H.; Gok, T.; Saygili, G.; Altintop, H.; Akcay, M.; Capar, I.D. Evaluation of effectiveness of various irrigating solutions on removal of calcium hydroxide mixed with 2% chlorhexidine gel and detection of orange-brown precipitate after removal. J. Endod. 2014, 40, 1820–1823. [Google Scholar] [CrossRef]
- Souza, M.; Cecchin, D.; Barbizam, J.V.; Almeida, J.F.; Zaia, A.A.; Gomes, B.P.; Ferraz, C.C. Evaluation of the colour change in enamel and dentine promoted by the interaction between 2% chlorhexidine and auxiliary chemical solutions. Aust. Endod. J. 2013, 39, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.; Bolla, N.; Sarath, R.K.; Ram, C.H. Assessment of precipitate formation on interaction of irrigants used in different combinations: An in vitro study. Indian J. Dent. Res. 2013, 24, 451–455. [Google Scholar] [CrossRef]
- Rossi-Fedele, G.; Doğramacı, E.J.; Steier, L.; de Figueiredo, J.A. Interaction between chlorhexidine-impregnated gutta-percha points and several chlorine-containing endodontic irrigating solutions. Int. Endod. J. 2013, 46, 675–680. [Google Scholar] [CrossRef]
- Prado, M.; Santos Júnior, H.M.; Rezende, C.M.; Pinto, A.C.; Faria, R.B.; Simão, R.A.; Gomes, B.P. Interactions between irrigants commonly used in endodontic practice: A chemical analysis. J. Endod. 2013, 39, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Pasich, E.; Bialecka, A.; Marcinkiewicz, J. Efficacy of taurine haloamines and chlorhexidine against selected oral microbiome species. Med. Dosw. Mikrobiol. 2013, 65, 187–196. [Google Scholar]
- Gupta, H.; Kandaswamy, D.; Manchanda, S.K.; Shourie, S. Evaluation of the sealing ability of two sealers after using chlorhexidine as a final irrigant: An in vitro study. J. Conserv. Dent. 2013, 16, 75–78. [Google Scholar] [CrossRef]
- Vilanova, W.V.; Carvalho-Junior, J.R.; Alfredo, E.; Sousa-Neto, M.D.; Silva-Sousa, Y.T. Effect of intracanal irrigants on the bond strength of epoxy resin-based and methacrylate resin-based sealers to root canal walls. Int. Endod. J. 2012, 45, 42–48. [Google Scholar] [CrossRef]
- Rossi-Fedele, G.; Doğramaci, E.J.; Guastalli, A.R.; Steier, L.; de Figueiredo, J.A. Antagonistic interactions between sodium hypochlorite, chlorhexidine, EDTA, and citric acid. J. Endod. 2012, 38, 426–431. [Google Scholar] [CrossRef]
- Kim, H.S.; Zhu, Q.; Baek, S.H.; Jung, I.Y.; Son, W.J.; Chang, S.W.; Lee, W.; Gu, Y.; Lee, Y.; Hong, S.T.; et al. Chemical interaction of alexidine and sodium hypochlorite. J. Endod. 2012, 38, 112–116. [Google Scholar] [CrossRef]
- Gasic, J.; Popovic, J.; Zivkovic, S.; Petrovic, A.; Barac, R.; Nikolic, M. Ultrastructural analysis of the root canal walls after simultaneous irrigation of different sodium hypochlorite concentration and 0.2% chlorhexidine gluconate. Microsc. Res. Tech. 2012, 75, 1099–1103. [Google Scholar] [CrossRef]
- Prado, M.; de Assis, D.F.; Gomes, B.P.; Simão, R.A. Effect of disinfectant solutions on the surface free energy and wettability of filling material. J. Endod. 2011, 37, 980–982. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, J.B.; Sem, D.S. An in vitro spectroscopic analysis to determine the chemical composition of the precipitate formed by mixing sodium hypochlorite and chlorhexidine. J. Endod. 2011, 37, 983–988. [Google Scholar] [CrossRef] [PubMed]
- De Assis, D.F.; Prado, M.; Simão, R.A. Evaluation of the interaction between endodontic sealers and dentin treated with different irrigant solutions. J. Endod. 2011, 37, 1550–1552. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.E.; Sem, D.S. An in vitro spectroscopic analysis to determine whether para-chloroaniline is produced from mixing sodium hypochlorite and chlorhexidine. J. Endod. 2010, 36, 315–317. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Sudhakaran, S. Evaluation and prevention of the precipitate formed on interaction between sodium hypochlorite and chlorhexidine. J. Endod. 2010, 36, 1154–1157. [Google Scholar] [CrossRef]
- Basrani, B.R.; Manek, S.; Mathers, D.; Fillery, E.; Sodhi, R.N. Determination of 4-chloroaniline and its derivatives formed in the interaction of sodium hypochlorite and chlorhexidine by using gas chromatography. J. Endod. 2010, 36, 312–314. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Abbott, P.V. The properties and applications of chlorhexidine in endodontics. Int. Endod. J. 2009, 42, 288–302. [Google Scholar] [CrossRef]
- Basrani, B.R.; Manek, S.; Fillery, E. Using diazotization to characterize the effect of heat or sodium hypochlorite on 2.0% chlorhexidine. J. Endod. 2009, 35, 1296–1299. [Google Scholar] [CrossRef]
- Kuruvilla, J.R.; Kamath, M.P. Antimicrobial activity of 2.5% sodium hypochlorite and 0.2% chlorhexidine gluconate separately and combined, as endodontic irrigants. J. Endod. 1998, 24, 472–476. [Google Scholar] [CrossRef]
- Marchesan, M.A.; Pasternak Junior, B.; Afonso, M.M.; Sousa-Neto, M.D.; Paschoalato, C. Chemical analysis of the flocculate formed by the association of sodium hypochlorite and chlorhexidine. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, e103–e105. [Google Scholar] [CrossRef] [PubMed]
- Calt, S.; Serper, A. Time-dependent effects of EDTA on dentin structures. J. Endod. 2002, 28, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Woo Chang, S.; Baek, S.H.; Han, S.H.; Lee, Y.; Zhu, Q.; Kum, K.Y. Antimicrobial effect of alexidine and chlorhexidine against Enterococcus faecalis infection. Int. J. Oral Sci. 2013, 5, 26–31. [Google Scholar] [CrossRef]
- Cobankara, F.K.; Ozkan, H.B.; Terlemez, A. Comparison of organic tissue dissolution capacities of sodium hypochlorite and chlorine dioxide. J. Endod. 2010, 36, 272–274. [Google Scholar] [CrossRef] [PubMed]
- Herczegh, A.; Ghidan, A.; Friedreich, D.; Gyurkovics, M.; Bendo, Z.; Lohinai, Z. Effectiveness of a high purity chlorine dioxide solution in eliminating intracanal Enterococcus faecalis biofilm. Acta Microbiol. Immunol. Hung. 2013, 60, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Nishikiori, R.; Nomura, Y.; Sawajiri, M.; Masuki, K.; Hirata, I.; Okazaki, M. Influence of chlorine dioxide on cell death and cell cycle of human gingival fibroblasts. J. Dent. 2008, 36, 993–998. [Google Scholar] [CrossRef]
- Fleming, C.H.; Litaker, M.S.; Alley, L.W.; Eleazer, P.D. Comparison of classic endodontic techniques versus contemporary techniques on endodontic treatment success. J. Endod. 2010, 36, 414–418. [Google Scholar] [CrossRef]
- Friedman, S.; Mor, C. The success of endodontic therapy—Healing and functionality. J. Calif. Dent. Assoc. 2004, 32, 493–503. [Google Scholar] [PubMed]
- Regan, J.D.; Fleury, A.A. Irrigants in non-surgical endodontic treatment. J. Ir. Dent. Assoc. 2006, 52, 84–92. [Google Scholar]
- Gilbert, P.; Moore, L.E. Cationic antiseptics: Diversity of action under a common epithet. J. Appl. Microbiol. 2005, 99, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, S.R.; Hirsch, S.; Hiergeist, A.; Kirschneck, C.; Muehler, D.; Hiller, K.A.; Maisch, T.; Al-Ahmad, A.; Gessner, A.; Buchalla, W.; et al. Limited antimicrobial efficacy of oral care antiseptics in microcosm biofilms and phenotypic adaptation of bacteria upon repeated exposure. Clin. Oral Investig. 2021, 25, 2939–2950. [Google Scholar] [CrossRef]
- Yesilsoy, C.; Whitaker, E.; Cleveland, D.; Phillips, E.; Trope, M. Antimicrobial and toxic effects of established and potential root canal irrigants. J. Endod. 1995, 21, 513–515. [Google Scholar] [CrossRef]
- Kandaswamy, D.; Venkateshbabu, N.; Gogulnath, D.; Kindo, A.J. Dentinal tubule disinfection with 2% chlorhexidine gel, propolis, morinda citrifolia juice, 2% povidone iodine, and calcium hydroxide. Int. Endod. J. 2010, 43, 419–423. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
|
|
| Author | Title | Study Aim | Type |
|---|---|---|---|
| Bueso et al., 2022 [34] | Comparative evaluation of intermediate solutions in prevention of brown precipitate formed from sodium hypochlorite and chlorhexidine gluconate | To evaluate intermediate treatments between sodium hypochlorite and chlorhexidine gluconate irrigations for the prevention of a toxic brown precipitate in root canal therapy. | Laboratory study |
| Jeong et al., 2021 [35] | Assessment of the cytotoxic effects and chemical composition of the insoluble precipitate formed from sodium hypochlorite and chlorhexidine gluconate | To investigate (1) the cytotoxic potential of the brown precipitate (BP) formed with sodium hypochlorite (NaOCl) and chlorhexidine gluconate (CHX), using both a small animal model of Caenorhabditis elegans (C. elegans) and cultured human gingival fibroblasts; (2) the chemical composition of BP using Time-of-Flight Secondary Ion Mass Spectrometry (ToF-SIMS). | Laboratory study |
| Czopik et al., 2021 [36] | Insight into the Reaction of Alexidine with Sodium Hypochlorite: A Potential Error in Endodontic Treatment | The aim of this study was to identify detected chemical compounds formed in the reaction of ALX and NaOCl with the ultra-high-performance liquid chromatography–mass spectrophotometry (UHPLC-MS) method and assess whether precipitates and PCA are formed in this reaction. | Laboratory study |
| Alberto et al., 2021 [37] | Does sodium thiosulphate avoid the formation of the brown-coloured precipitate as an intermediate irrigant between NaOCl and chlorhexidine? | This study evaluated the efficacy of sodium thiosulphate (ST) as an intermediate irrigant between sodium hypochlorite (NaOCl) and chlorhexidine (CHX) to avoid the formation of the brown-coloured precipitate. | Laboratory study |
| Khatib et al., 2020 [33] | Decoding the Perplexing Mystery of Para-Chloroaniline Formation: A Systematic Review | The purpose of this systematic review is to evaluate the relationship between PCA and brown precipitate. | Systematic review |
| Keles et al., 2020 [32] | Effect of various solutions on the removal of orange-brown precipitate formed by interaction of sodium hypochlorite and chlorhexidine with or without ultrasonic activation | The aim of this in vitro study was to investigate the possible interactions between photon-induced photoacoustic streaming (PIPS™)-activated oxidizing agents and 2% chlorhexidine digluconate. | Laboratory study |
| Buyukozer Ozkan et al., 2020 [38] | Proton Nuclear Magnetic Resonance Spectroscopy Analysis of Mixtures of Chlorhexidine with Different Oxidizing Agents Activated by Photon-Induced Photoacoustic Streaming for Root Canal Irrigation | The aim of the study was to assess the depth of sealer penetration into dentinal tubules following different final rinses and indirectly evaluate precipitation of irrigating solutions. | Laboratory study |
| Abusteit, 2020 [39] | Evaluation of resin sealer penetration of dentin following different final rinses for endodontic irrigation using confocal laser scanning microscopy | This study aimed to evaluate the characterization of chemical interaction of root canal irrigants on the surface of EndoSequence root repair materials using spectroscopy analysis. | Laboratory study |
| Abu Zeid et al., 2020 [40] | Morphological and chemical analysis of surface interaction of irrigant-endosequence root repair material | This study aimed to evaluate the characterization of chemical interaction of root canal irrigants on the surface of EndoSequence root repair materials using spectroscopy analysis. | Laboratory study |
| Thomas et al., 2019 [41] | Evaluation of the Antibacterial Efficiency of a Combination of 1% Alexidine and Sodium Hypochlorite on Enterococcus faecalis Biofilm Models: An In Vitro Study | The aim of the study was to assess the antibacterial efficiency of a combination of 1% alexidine (ALX) and 5.25% sodium hypochlorite (NaOCl) against E. faecalis biofilm using a confocal scanning electron microscopy. | Laboratory study |
| Siddique et al., 2019b [16] | Qualitative and quantitative analysis of precipitate formation following interaction of chlorhexidine with sodium hypochlorite, neem, and tulsi | This study aims to evaluate the precipitate formed on combination of different irrigants, weigh the amount of precipitate formed and to analyze the precipitate for PCA. | Laboratory study |
| Siddique et al., 2019a [42] | Quantitative analysis for detection of toxic elements in various irrigants, their combination (precipitate), and para-chloroaniline: An inductively coupled plasma mass spectrometry study | The aim of this study was to evaluate the precipitate formed on combination of different irrigants, weigh the amount of precipitate formed, and to analyze 35 different metal elements in each irrigant, precipitate formed as well as in PCA. | Laboratory study |
| Žižka et al., 2018 [43] | Discoloration after Regenerative Endodontic Procedures: A Critical Review | This review presents a critical view on current knowledge of discoloration sources, its treatment and possible preventive modalities. | review |
| Ravinanthanan et al., 2018 [44] | Cytotoxicity Evaluation of Combination Irrigant Regimens with MTAD on Two Different Cell Lines | The aim of this study was to evaluate the cytotoxicity of combination regimens on target and nontarget cell lines by trypan blue assay. | Laboratory study |
| Piperidou et al., 2018 [45] | Effects of Final Irrigation with SmearOFF on the Surface of Dentin Using Surface Analytical Methods | This study examined the chemical interaction of SmearOFF with sodium hypochlorite (NaOCl) on the dentin surface, specifically the formation of precipitate and/or parachloroaniline (PCA). | Laboratory study |
| Jain et al., 2018 [46] | Alexidine versus chlorhexidine for endodontic irrigation with sodium hypochlorite | The objective of this study was to chemically evaluate precipitate formation on irrigation by different concentrations of chlorhexidine (CHX) and alexidine (ALX) with sodium hypochlorite (NaOCl). | Laboratory study |
| Irmak et al., 2018 [47] | Nuclear magnetic resonance spectroscopy and infrared spectroscopy analysis of precipitate formed after mixing sodium hypochlorite and QMix 2 in 1 | This study assessed whether para-chloroaniline (PCA) is formed after mixing NaOCl with Qmix. | Laboratory study |
| Gonzalez et al., 2018 [48] | Temperature changes in 2% chlorhexidine gluconate using two activation methods with different intensity levels | …the objective is to establish the influence of ultrasonic and sonic activation, with the use of different intensities, upon the temperature of chlorhexidine gluconate (CHX). | Laboratory study |
| Chhabra et al., 2018 [15] | Efficacy of various solutions in preventing orange-brown precipitate formed during alternate use of sodium hypochlorite and chlorhexidine: An In vitro study | The study evaluated the effectiveness of three Intermediate endodontic irrigating solutions in eliminating the residual sodium hypochlorite (NaOCl). | Laboratory study |
| Campbell et al., 2018 [49] | Antiseptics Commonly Used in Total Joint Arthroplasty Interact and May Form Toxic Products | Our clinical experience is that chlorhexidine (CHX) and Dakin’s solution (NaOCl) interact and form a precipitate. The purpose of this study is to determine whether this reaction could be replicated in a laboratory setting, and to determine if other commonly used antiseptics also visibly react when mixed. | Laboratory study |
| Wright et al., 2017 [7] | Alkaline Sodium Hypochlorite Irrigant and Its Chemical Interactions | Of particular interest is the interaction between sodium hypochlorite and the chelators EDTA, citric acid and etidronate and between sodium hypochlorite and the antimicrobials chlorhexidine, alexidine, MTAD and octenisept. | review |
| Thaha et al., 2017 [50] | Interaction between Octenidine-based Solution and Sodium Hypochlorite: A Mass Spectroscopy, Proton Nuclear Magnetic Resonance, and Scanning Electron Microscopy-based Observational Study | The aim of this study was first to Identify the precipitate formed on the interaction between OCT and NaOCl and secondly to compare its effect on dentinal tubules with that of precipitate formed on combining chlorhexidine (CHX) and NaOCl. | Laboratory study |
| Surrender et al., 2017 [51] | Alexidine: A Safer and an Effective Root Canal Irrigant than Chlorhexidine | AIM: To compare antimicrobial activity of different concentrations of ALX with CHX individually and when combined with NaOCl against E. faecalis strains. | Laboratory study |
| Nocca et al., 2017 [14] | Chromographic Analysis and Cytotoxic Effects of Chlorhexidine and Sodium Hypochlorite Reaction Mixtures | This study aimed to investigate the stability of PCA in the presence of NaOCl and to examine the in vitro cytotoxic effects of CHX/NaOCl reaction mixtures. | Laboratory study |
| Guneser et al., 2017 [52] | Comparison of Conventional Syringe, CanalBrush, EndoActivator, Photon-Induced Photoacoustic Streaming, and Manual Instrumentation in Removing Orange-Brown Precipitate: An In Vitro Study | The aim of this In vitro study was to compare the various techniques for removing precipitate formed after irrigation with sodium hypochlorite (NaOCl) and chlorhexidine (CHX). | Laboratory study |
| Vouzara et al., 2016 [53] | Combined and independent cytotoxicity of sodium hypochlorite, ethylenediaminetetraacetic acid and chlorhexidine | AIM: To evaluate the capacity of commonly used root canal irrigants to induce cytotoxic effects, when applied singly or in combination | Laboratory study |
| Patil et al., 2016 [54] | Determination of mutagenicity of the precipitate formed by sodium hypochlorite and chlorhexidine using the Ames test | The aim of this study was to determine the direct mutagenic potential of any precipitate formed by combining sodium hypochlorite (NaOCl) and chlorhexidine (CHX). | Laboratory study |
| Orhan et al., 2016 [55] | Does Para-chloroaniline Really Form after Mixing Sodium Hypochlorite and Chlorhexidine? | Purpose of this study was to determine whether PCA is formed through the reaction of mixing NaOCl and CHX. | Laboratory study |
| Mohammadi et al., 2015 [56] | Agonistic and Antagonistic Interactions between Chlorhexidine and Other Endodontic Agents: A Critical Review | The aim of this investigation was to review the agonistic and antagonistic interactions between chlorhexidine (CHX) and other irrigants and medicaments. | review |
| Metri et al., 2015 [57] | Comparative Evaluation of Two Final Irrigation Techniques for the Removal of Precipitate Formed by the Interaction between Sodium Hypochlorite and Chlorhexidine | AIM: To evaluate the effectiveness of two final irrigation techniques for the removal of precipitate formed by the interaction between sodium hypochlorite (NaOCl) and chlorhexidine (CHX). | Laboratory study |
| Magro et al., 2015 [58] | Effectiveness of several solutions to prevent the formation of precipitate due to the interaction between sodium hypochlorite and chlorhexidine and its effect on bond strength of an epoxy-based sealer | AIM: To evaluate the effectiveness of isopropyl alcohol, saline or distilled water to prevent the precipitate formed between sodium hypochlorite (NaOCl) and chlorhexidine (CHX) and its effect on the bond strength of an epoxy-based sealer in radicular dentine. | Laboratory study |
| Bernardi & Teixeira, 2015 [28] | The properties of chlorhexidine and undesired effects of its use in endodontics | The purpose of this article was to review the literature on the properties of chlorhexidine (CHX) and the adverse effects that may occur from its use in endodontics. | review |
| Arslan et al., 2015 [59] | Evaluation of orange-brown precipitate formed in root canals after irrigation with chlorhexidine and QMix and spectroscopic analysis of precipitates produced by a mixture of chlorhexidine/NaOCl and Qmix/NaOCl | AIM: To compare chlorhexidine and Qmix™ in terms of orange-brown precipitate generation in root canals and (ii) to analyse the precipitate produced by mixing chlorhexidine and Qmix(™) with NaOCl to determine whether para-chloroaniline was produced. | Laboratory study |
| Kolosowski et al., 2014 [60] | Qualitative analysis of precipitate formation on the surface and in the tubules of dentin irrigated with sodium hypochlorite and a final rinse of chlorhexidine or QMiX | The aim of this study was to qualitatively assess the formation of precipitate and PCA on the surface and in the tubules of dentin irrigated with NaOCl, followed either by EDTA, NaOCl, and CHX or by saline and QMiX. | Laboratory study |
| Homayouni et al., 2014 [61] | The Effect of Root Canal Irrigation with Combination of Sodium Hypo-chlorite and Chlorhexidine Gluconate on the Sealing Ability of Obturation Materials | The aim of this study was to evaluate the effect of the precipitate that was formed by combining Sodium Hypochlorite (NaOCl) and Chlorhexidine Gluconate (CHX) on the sealing ability of root canal obturation materials. | Laboratory study |
| Magro et al., 2014 [62] | Evaluation of the interaction between sodium hypochlorite and several formulations containing chlorhexidine and its effect on the radicular dentin—SEM and push-out bond strength analysis | The aim of the current study was to evaluate the presence of debris and smear layer after endodontic irrigation with different formulations of 2% chlorhexidine gluconate (CHX) and its effects on the push-out bond strength of an epoxy-based sealer on the radicular dentin. | Laboratory study |
| Cintra et al., 2014 [63] | The use of NaOCl in combination with CHX produces cytotoxic product | The aim of this study was to evaluate the tissue response to implanted polyethylene tubes filled with PPT-soaked fibrin sponge. | Laboratory study |
| Arslan et al., 2014 [64] | Evaluation of effectiveness of various irrigating solutions on removal of calcium hydroxide mixed with 2% chlorhexidine gel and detection of orange-brown precipitate after removal | The aims of the present study were to evaluate the effect of various irrigating solutions on the removal of calcium hydroxide mixed with 2% chlorhexidine gel from an artificial groove created in a root canal and the generation of orange-brown precipitate in the remaining calcium hydroxide mixed with 2% chlorhexidine gel after irrigation with the various irrigating solutions. | Laboratory study |
| Souza et al., 2013 [65] | Evaluation of the colour change in enamel and dentine promoted by the interaction between 2% chlorhexidine and auxiliary chemical solutions | AIM: To evaluate the colour change in enamel and dentine, promoted by interaction of 2% chlorhexidine gluconate (CHX) with 5.25% sodium hypochlorite (NaOCl) and 17% ethylenediaminetetraacetic acid (EDTA). | Laboratory study |
| Shenoy et al., 2013 [66] | Assessment of precipitate formation on interaction of irrigants used in different combinations: an in vitro study | AIM: To evaluate the combination of various irrigants whether it forms the precipitate and also to quantify the amount of precipitate formed. | Laboratory study |
| Rossi-Fedele et al., 2013 [67] | Interaction between chlorhexidine-impregnated gutta-percha points and several chlorine-containing endodontic irrigating solutions | AIM: To evaluate if the immersion of chlorhexidine-impregnated gutta-percha points in chlorine-containing endodontic irrigants causes colour changes and precipitate formation. | Laboratory study |
| Prado et al., 2013 [68] | Interactions between irrigants commonly used in endodontic practice: a chemical analysis | The aim of this work was to characterize the by-products formed in the associations between the most commonly used irrigants in endodontic practice. | Laboratory study |
| Pasich et al., 2013 [69] | Efficacy of taurine haloamines and chlorhexidine against selected oral microbiome species | In this in vitro study we have compared antimicrobial activity of CHX with that of taurine chloramine (TauC1) and taurine bromamine (TauBr). | Laboratory study |
| Gupta et al., 2013 [70] | Evaluation of the sealing ability of two sealers after using chlorhexidine as a final irrigant: An in vitro study | The aim of this study was to evaluate the effect of the precipitate formed by using sodium hypochlorite and chlorhexidine as a root canal irrigant on the sealing ability of different root canal sealers. | Laboratory study |
| Gomes et al., 2013 [6] | Chlorhexidine in endodontics | The aim of this paper is to review CHX’s general use in the medical field and in dentistry. | review |
| Vilanova et al., 2012 [71] | Effect of intracanal irrigants on the bond strength of epoxy resin-based and methacrylate resin-based sealers to root canal walls | AIM: To assess the bond strength of Epiphany and AH Plus sealers to root canal walls using a push-out test after use of several endodontic irrigants. | Laboratory study |
| Rossi-Fedele et al., 2012 [72] | Antagonistic interactions between sodium hypochlorite, chlorhexidine, EDTA, and citric acid | The aim of this investigation was to review the antagonistic interactions occurring when sodium hypochlorite (NaOCl), chlorhexidine (CHX), EDTA, and citric acid (CA) are used together during endodontic treatment. | review |
| Mortenson et al., 2012 [13] | The effect of using an alternative irrigant between sodium hypochlorite and chlorhexidine to prevent the formation of para-chloroaniline within the root canal system | AIM: To determine if the formation of para-chloroaniline (PCA) can be avoided by using an alternative irrigant following sodium hypochlorite but before chlorhexidine. | Laboratory study |
| Kim, 2012 [31] | Precipitate from a combination of sodium hypochlorite and chlorhexidine | …Chlorhexidine can form a precipitate when used in combination with NaOCl during intra-canal irrigation. What is the adverse effect of this precipitate and how can I reduce the chance of precipitation? | short communication |
| Kim et al., 2012 [73] | Chemical interaction of alexidine and sodium hypochlorite | This study determined by electrospray ionization mass spectrometry (ESI-MS) and scanning electron microscopy (SEM) whether the chemical interaction between ALX and NaOCl results in PCA or precipitates. | Laboratory study |
| Gasic et al., 2012 [74] | Ultrastructural analysis of the root canal walls after simultaneous irrigation of different sodium hypochlorite concentration and 0.2% chlorhexidine gluconate | AIM: To determine whether sodium hypochlorite (NaOCl) with 0.2% chlorhexidine gluconate (CHX) leads to colour change and precipitate formation, and to ultrastructurally analyse the dentine surface after simultaneous irrigation with 0.5% NaOCl and 0.2% CHX. | Laboratory study |
| Prado et al., 2011 [75] | Effect of disinfectant solutions on the surface free energy and wettability of filling material | The aims of this study were to evaluate the surface free energy of GP and Res cones after disinfection procedures and to investigate the wettability of endodontic sealers in contact with these surfaces. | Laboratory study |
| Nowicki & Sem, 2011 [76] | An in vitro spectroscopic analysis to determine the chemical composition of the precipitate formed by mixing sodium hypochlorite and chlorhexidine | The purpose of this in vitro study was to determine the chemical composition of the precipitate formed by mixing sodium hypochlorite (NaOCl) and chlorhexidine (CHX) and the relative molecular weight of the components. | Laboratory study |
| de Assis et al., 2011 [77] | Evaluation of the interaction between endodontic sealers and dentin treated with different irrigant solutions | The aim of this study was to investigate the wettability of endodontic sealers in contact with dentin treated with 5.25% sodium hypochlorite (NaOCl) and 2% chlorhexidine (CHX) in the presence or absence of smear layer. | Laboratory study |
| Thomas & Sem, 2010 [78] | An in vitro spectroscopic analysis to determine whether para-chloroaniline is produced from mixing sodium hypochlorite and chlorhexidine | The purpose of this in vitro study was to determine whether para-chloroaniline (PCA) is formed through the reaction of mixing sodium hypochlorite (NaOCl) and chlorhexidine (CHX). | Laboratory study |
| Krishnamurthy & Sudhakaran, 2010 [79] | Evaluation and prevention of the precipitate formed on interaction between sodium hypochlorite and chlorhexidine | The purpose of this study was (1) to evaluate maximum thickness the and chemical composition of the precipitate formed between sodium hypochlorite (NaOCl) and chlorhexidine (CHX) and (2) to evaluate effectiveness of absolute alcohol to remove residual NaOCl and thereby prevent the formation of the precipitate. | Laboratory study |
| Basrani et al., 2010 [80] | Determination of 4-chloroaniline and its derivatives formed in the interaction of sodium hypochlorite and chlorhexidine by using gas chromatography | The aim of this study was to further identify the precipitate by using gas chromatography-mass spectrometry (GC-MS). | Laboratory study |
| Akisue et al., 2010 [12] | Effect of the combination of sodium hypochlorite and chlorhexidine on dentinal permeability and scanning electron microscopy precipitate observation | This study compared the combined use of sodium hypochlorite (NaOCl) and chlorhexidine (CXH) with citric acid and CXH on dentinal permeability and precipitate formation. | Laboratory study |
| Mohammadi & Abbott, 2009 [81] | The properties and applications of chlorhexidine in endodontics | The purpose of this paper is to review the structure and mechanism of action of CHX, its antibacterial and antifungal activity, its effect on biofilm, its substantivity (residual antibacterial activity), its tissue solvent ability, its interaction with calcium hydroxide and sodium hypochlorite, its anticollagenolytic activity, its effect on coronal and apical leakage of bacteria, its toxicity and allergenicity and the modulating effect of dentine and root canal components on its antimicrobial activity. | review |
| Basrani et al., 2009 [82] | Using diazotization to characterize the effect of heat or sodium hypochlorite on 2.0% chlorhexidine | The aim of the present study was to use a diazotization technique to confirm the presence of an aromatic amine (such as PCA) in the NaOCl/CHX precipitate and also in the 2.0% CHX at different temperatures (37 degrees C and 45 degrees C). | Laboratory study |
| Bui et al., 2008 [30] | Evaluation of the interaction between sodium hypochlorite and chlorhexidine gluconate and its effect on root dentin | The aim of this study was to evaluate the effect of irrigating root canals with a combination of NaOCl and CHX on root dentin and dentinal tubules… | Laboratory study |
| Basrani et al., 2007 [11] | Interaction between sodium hypochlorite and chlorhexidine gluconate | The aim of this study was to determine the minimum concentration of NaOCl required to form a precipitate with 2.0% CHX. | Laboratory study |
| Zehnder, 2006 [5] | Root canal irrigants | In this review article, the specifics of the pulpal microenvironment and the resulting requirements for irrigating solutions are spelled out. | review |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drews, D.-J.; Nguyen, A.D.; Diederich, A.; Gernhardt, C.R. The Interaction of Two Widely Used Endodontic Irrigants, Chlorhexidine and Sodium Hypochlorite, and Its Impact on the Disinfection Protocol during Root Canal Treatment. Antibiotics 2023, 12, 589. https://doi.org/10.3390/antibiotics12030589
Drews D-J, Nguyen AD, Diederich A, Gernhardt CR. The Interaction of Two Widely Used Endodontic Irrigants, Chlorhexidine and Sodium Hypochlorite, and Its Impact on the Disinfection Protocol during Root Canal Treatment. Antibiotics. 2023; 12(3):589. https://doi.org/10.3390/antibiotics12030589
Chicago/Turabian StyleDrews, Dirk-Joachim, Anh Duc Nguyen, Antje Diederich, and Christian Ralf Gernhardt. 2023. "The Interaction of Two Widely Used Endodontic Irrigants, Chlorhexidine and Sodium Hypochlorite, and Its Impact on the Disinfection Protocol during Root Canal Treatment" Antibiotics 12, no. 3: 589. https://doi.org/10.3390/antibiotics12030589
APA StyleDrews, D.-J., Nguyen, A. D., Diederich, A., & Gernhardt, C. R. (2023). The Interaction of Two Widely Used Endodontic Irrigants, Chlorhexidine and Sodium Hypochlorite, and Its Impact on the Disinfection Protocol during Root Canal Treatment. Antibiotics, 12(3), 589. https://doi.org/10.3390/antibiotics12030589