
Comparing the Outcomes of Ceftaroline plus Vancomycin or Daptomycin Combination Therapy versus Vancomycin or Daptomycin Monotherapy in Adults with Methicillin-Resistant Staphylococcus aureus Bacteremia—A Meta-Analysis

Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Included Trials
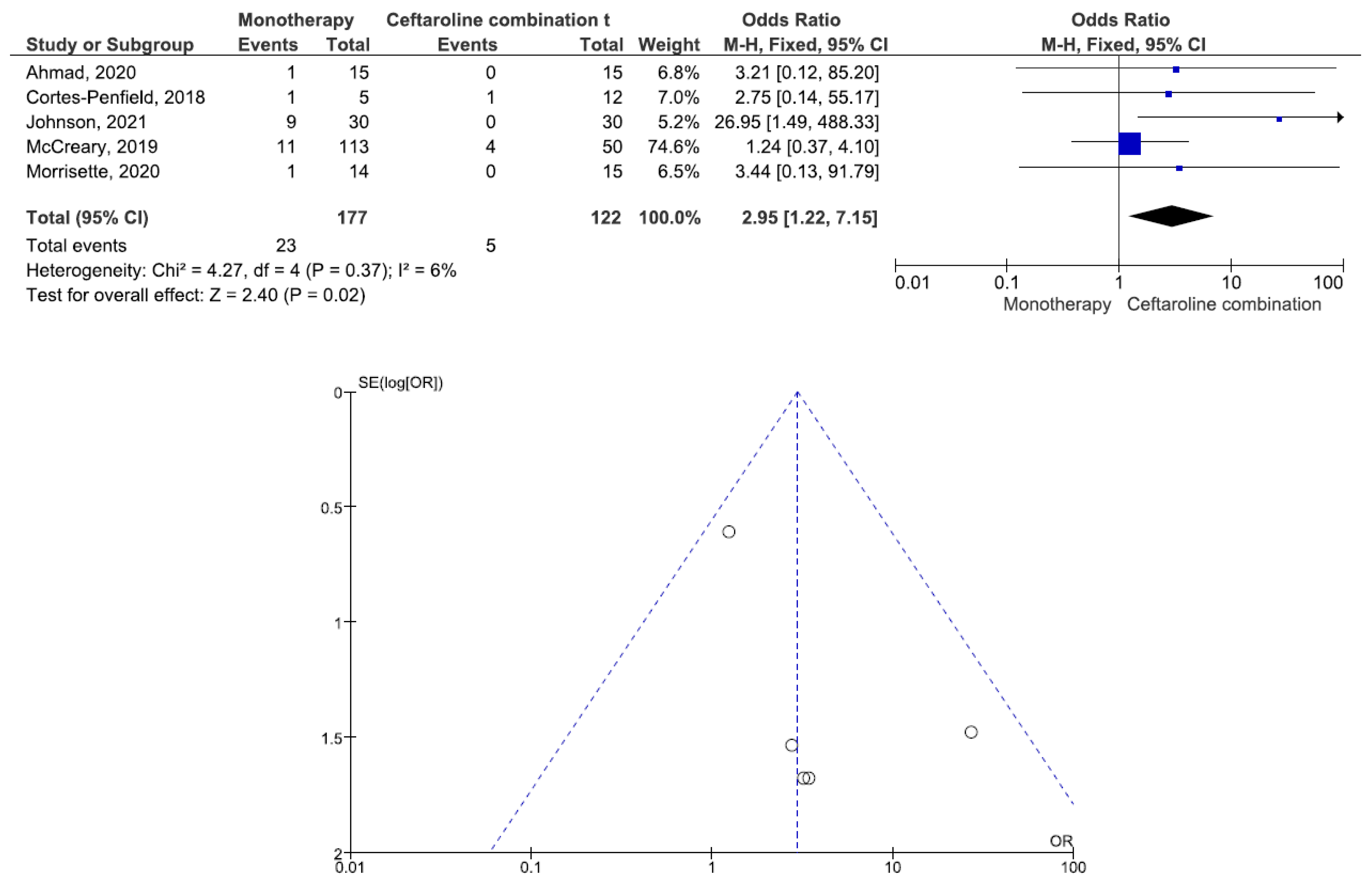
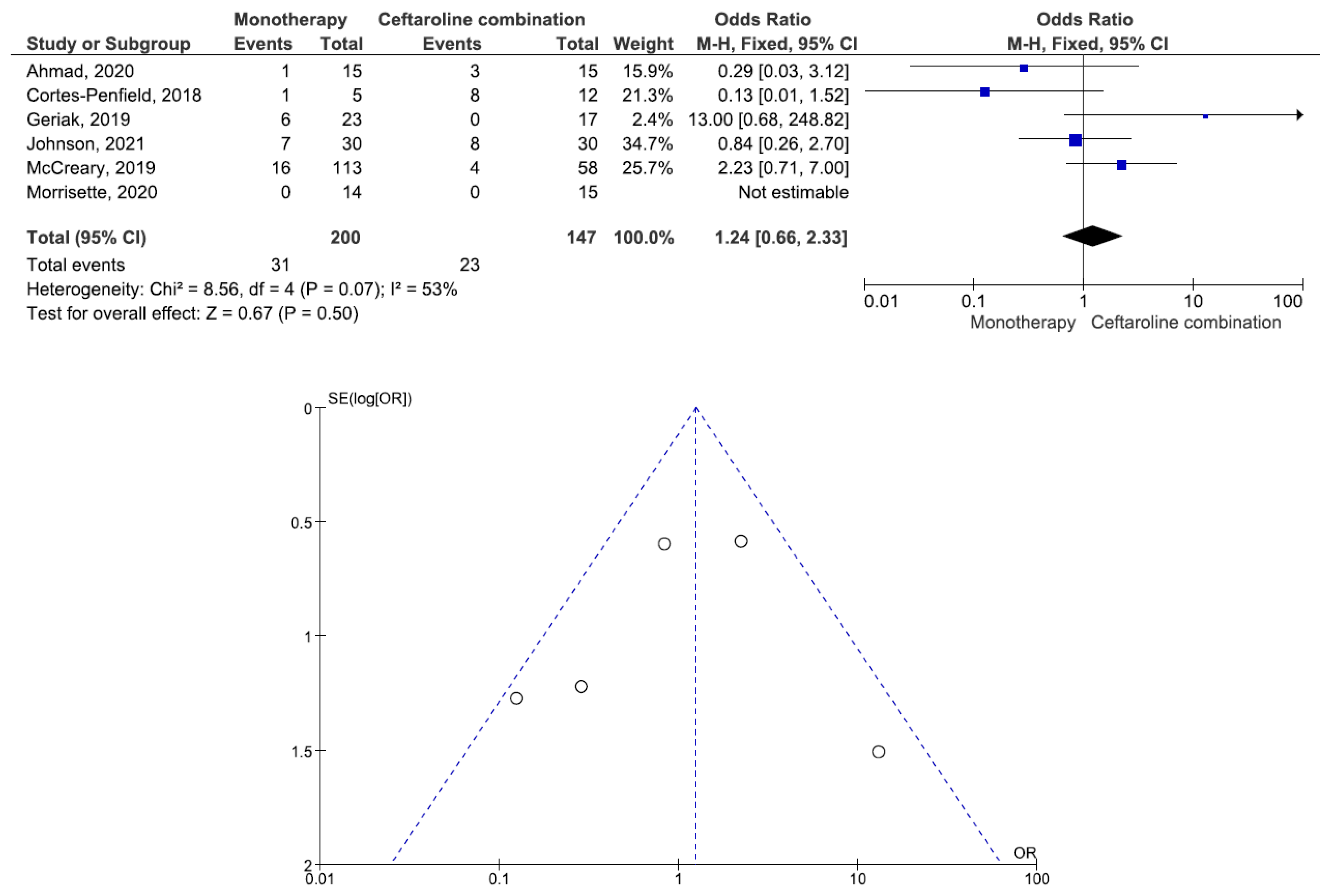
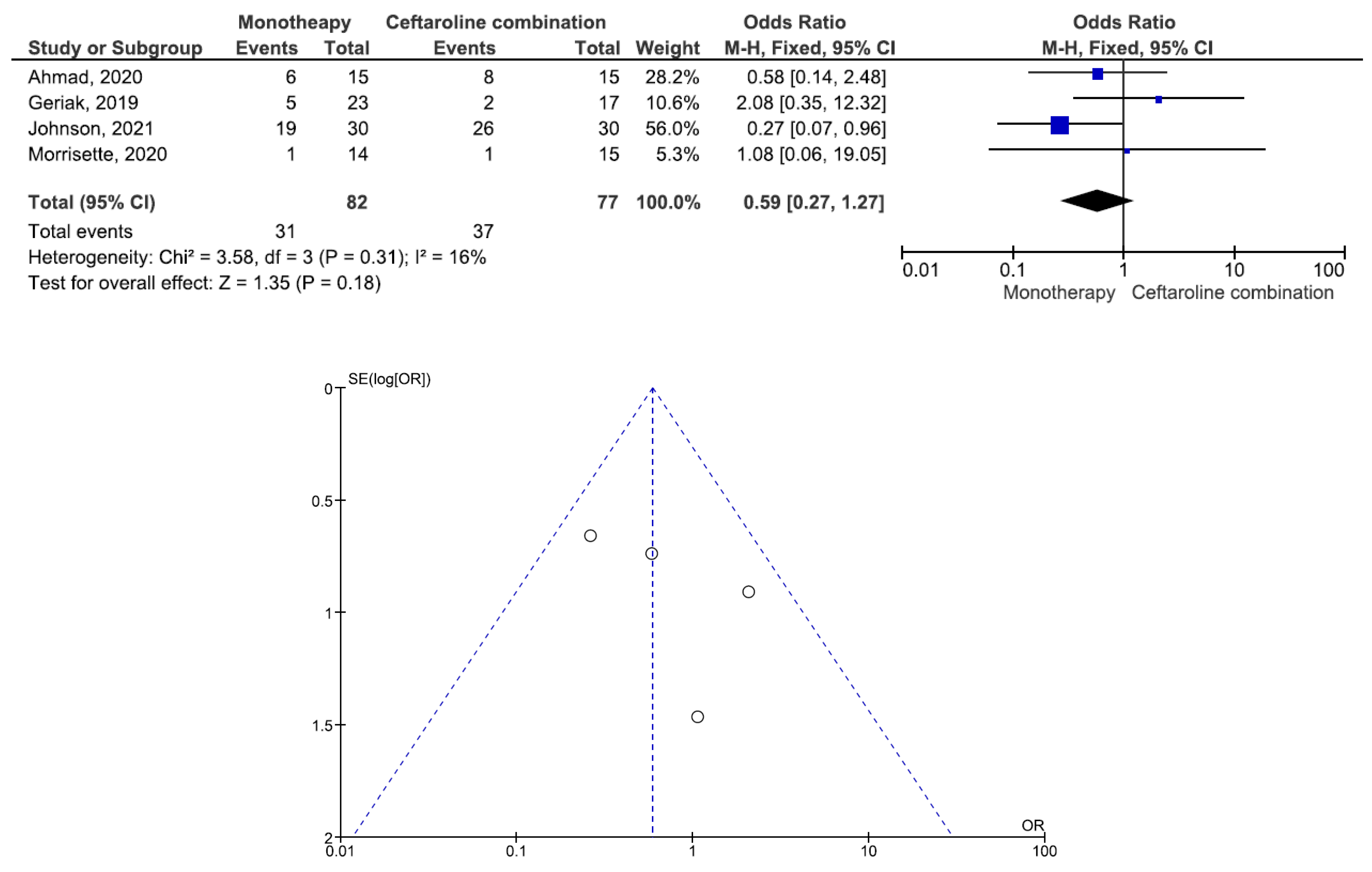
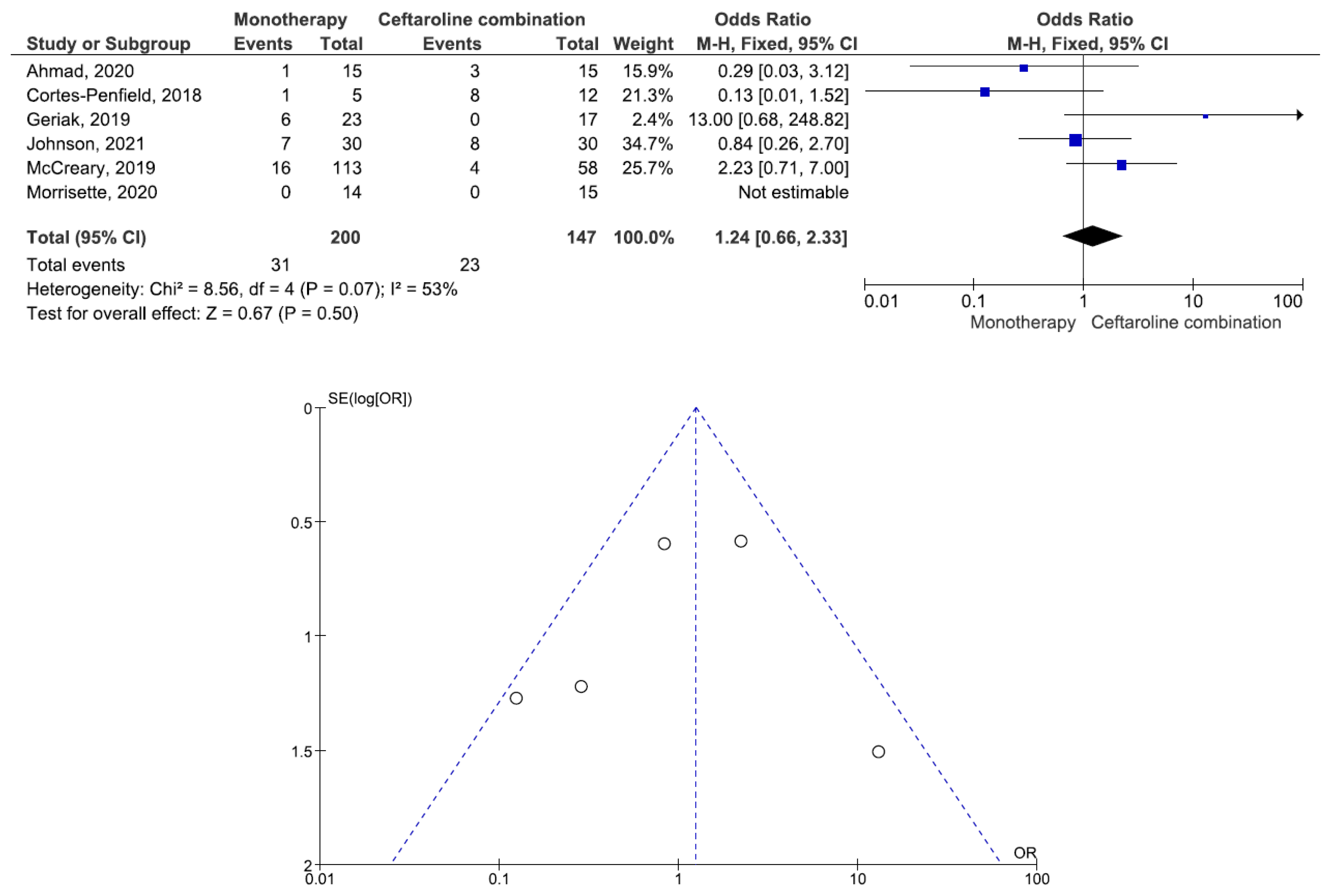
2.2. Efficacy and Safety Outcomes
3. Methods
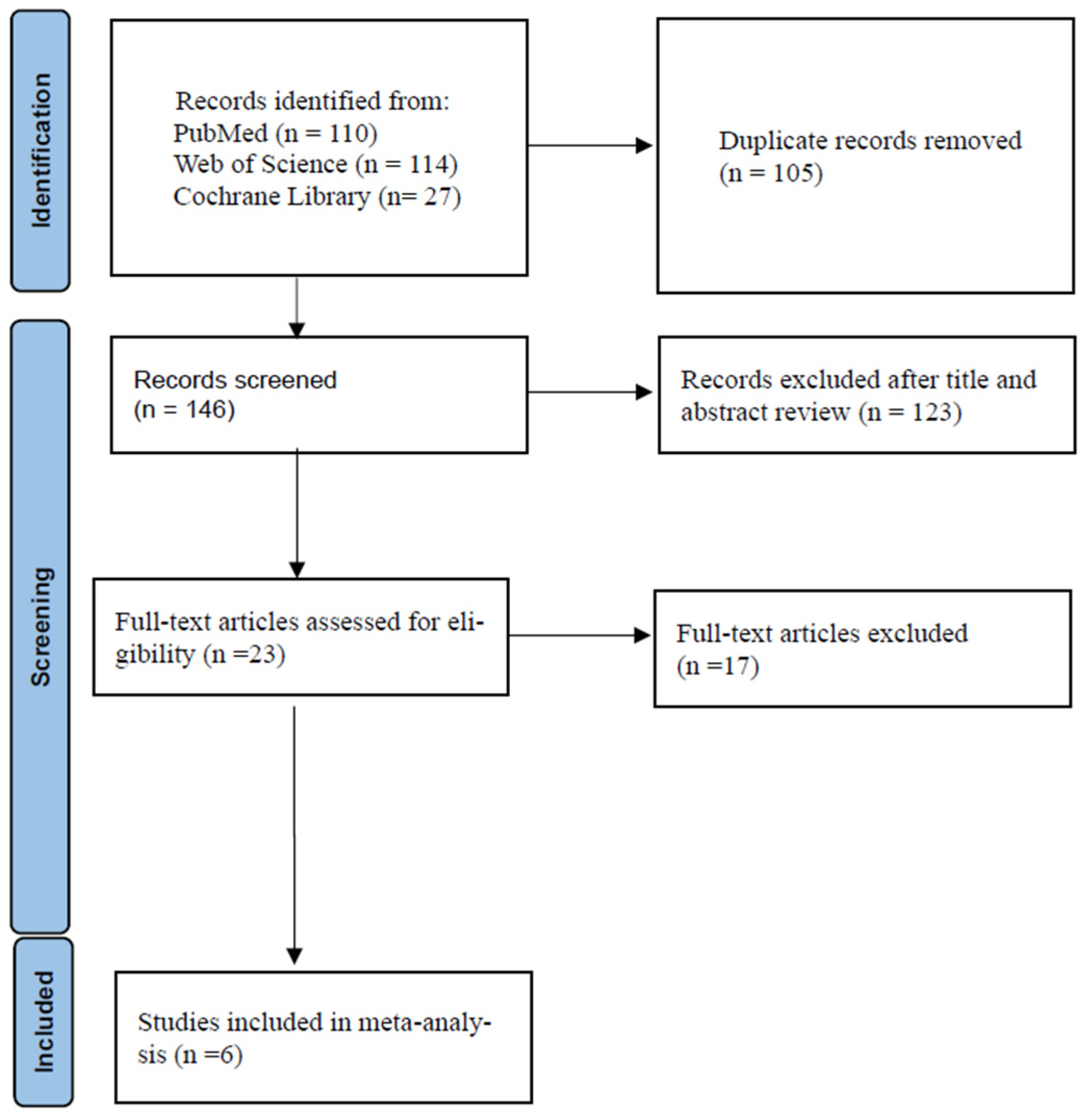
3.1. Data Search Strategy
3.2. Study Selection and Data Extraction
3.3. Inclusion and Exclusion Criteria
3.4. Definitions and Outcomes
3.5. Quality Assessment and Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Hal, S.J.; Jensen, S.O.; Vaska, V.L.; Espedido, B.A.; Paterson, D.L.; Gosbell, I.B. Predictors of mortality in Staphylococcus aureus bacteremia. Clin. Microbiol. Rev. 2012, 25, 362–386. [Google Scholar] [CrossRef] [PubMed]
- Naber, C.K. Staphylococcus aureus bacteremia: Epidemiology, pathophysiology, and management strategies. Clin. Infect. Dis. 2009, 48, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, C.; Huang, J.; Jin, N.; Noskin, G.A.; Zembower, T.R.; Bolon, M. Persistent Staphylococcus aureus bacteremia: An analysis of risk factors and outcomes. Arch. Intern. Med. 2007, 167, 1861–1867. [Google Scholar] [CrossRef]
- Forstner, C.; Dungl, C.; Tobudic, S.; Mitteregger, D.; Lagler, H.; Burgmann, H. Predictors of clinical and microbiological treatment failure in patients with methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia: A retrospective cohort study in a region with low MRSA prevalence. Clin. Microbiol. Infect. 2013, 19, E291–E297. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.H.; Liao, W.H.; Lai, C.C.; Liao, C.H.; Tan, C.K.; Wang, C.Y.; Huang, Y.T.; Hsueh, P.R. Risk factors for mortality in patients with persistent methicillin-resistant Staphylococcus aureus bacteraemia in a tertiary care hospital in Taiwan. J. Antimicrob. Chemother. 2010, 65, 1792–1798. [Google Scholar] [CrossRef]
- Lodise, T.P.; Graves, J.; Evans, A.; Graffunder, E.; Helmecke, M.; Lomaestro, B.M.; Stellrecht, K. Relationship between vancomycin MIC and failure among patients with methicillin-resistant Staphylococcus aureus bacteremia treated with vancomycin. Antimicrob. Agents Chemother. 2008, 52, 3315–3320. [Google Scholar] [CrossRef]
- Yoon, Y.K.; Kim, J.Y.; Park, D.W.; Sohn, J.W.; Kim, M.J. Predictors of persistent methicillin-resistant Staphylococcus aureus bacteraemia in patients treated with vancomycin. J. Antimicrob. Chemother. 2010, 65, 1015–1018. [Google Scholar] [CrossRef]
- Gould, I.M. Treatment of bacteraemia: Meticillin-resistant Staphylococcus aureus (MRSA) to vancomycin-resistant S. aureus (VRSA). Int. J. Antimicrob. Agents 2013, 42 (Suppl. S1), S17–S21. [Google Scholar] [CrossRef]
- Sharma, M.; Riederer, K.; Chase, P.; Khatib, R. High rate of decreasing daptomycin susceptibility during the treatment of persistent Staphylococcus aureus bacte¬remia. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 27, 433–437. [Google Scholar] [CrossRef]
- Kelley, P.G.; Gao, W.; Ward, P.B.; Howden, B.P. Daptomycin non-susceptibility in vancomycin- intermediate Staphylococcus aureus (VISA) and heterogeneous- VISA (hVISA): Implications for therapy after vancomycin treatment failure. J. Antimicrob. Chemother. 2011, 66, 1057–1060. [Google Scholar] [CrossRef]
- Gasch, O.; Camoez, M.; Domínguez, M.A.; Padilla, B.; Pintado, V.; Almirante, B.; Martín, C.; López-Medrano, F.; de Gopegui, E.R.; Blanco, J.R.; et al. Emergence of resistance to daptomycin in a cohort of patients with methicillin-resistant Staphylococcus aureus persistent bacteraemia treated with daptomycin. J. Antimicrob. Chemother. 2014, 69, 568–571. [Google Scholar] [CrossRef]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef] [PubMed]
- Farrell, D.J.; Castanheira, M.; Mendes, R.E.; Sader, H.S.; Jones, R.N. In vitro activity of ceftaroline against multidrug-resistant Staphylococcus aureus and Streptococcus pneumoniae: A review of published studies and the AWARE Surveillance Program (2008–2010). Clin. Infect. Dis. 2012, 55 (Suppl. S3), S206–S214. [Google Scholar] [CrossRef] [PubMed]
- Laudano, J.B. Ceftaroline fosamil: A new broad-spectrum cephalosporin. J. Antimicrob Chemother. 2011, 66 (Suppl. S3), iii11–iii18. [Google Scholar] [CrossRef] [PubMed]
- Moisan, H.; Pruneau, M.; Malouin, F. Binding of ceftaroline to penicillin-binding proteins of Staphylococcus aureus and Streptococcus pneumoniae. J. Antimicrob Chemother. 2010, 65, 713–716. [Google Scholar] [CrossRef]
- De Lencastre, H.; Oliveira, D.; Tomasz, A. Antibiotic resistant Staphylococcus aureus: A paradigm of adaptive power. Curr. Opin. Microbiol. 2007, 10, 428–435. [Google Scholar] [CrossRef]
- Kosowska-Shick, K.; McGhee, P.L.; Appelbaum, P.C. Affinity of ceftaroline and other β-lactams for penicillin-binding proteins from Staphylococcus aureus and Streptococcus pneumoniae. Antimicrob. Agents Chemother. 2010, 54, 1670–1677. [Google Scholar] [CrossRef] [PubMed]
- File, T.M.J.r.; Wilcox, M.H.; Stein, G.E. Summary of ceftaroline fosamil clinical trial studies and clinical safety. Clin. Infect. Dis. 2012, 55 (Suppl. S3), S173–S180. [Google Scholar] [CrossRef]
- Cosimi, R.A.; Beik, N.; Kubiak, D.W.; Johnson, J.A. Ceftaroline for severe methicillin-resistant Staphylococcus aureus infections: A systematic review. Open Forum Infect. Dis. 2017, 4, ofx084. [Google Scholar] [CrossRef]
- Casapao, A.M.; Davis, S.L.; Barr, V.O.; Klinker, K.P.; Goff, D.A.; Barber, K.E.; Kaye, K.S.; Mynatt, R.P.; Molloy, L.M.; Pogue, J.M.; et al. Large retrospective evaluation of the effectiveness and safety of ceftaroline fosamil therapy. Antimicrob. Agents Chemother. 2014, 58, 2541–2546. [Google Scholar] [CrossRef]
- Zasowski, E.J.; Trinh, T.D.; Claeys, K.C.; Casapao, A.M.; Sabagha, N.; Lagnf, A.M.; Klinker, K.P.; Davis, S.L.; Rybak, M.J. Multicenter observational study of ceftaroline fosamil for methicillin-resistant Staphylococcus aureus bloodstream infections. Antimicrob. Agents Chemother. 2017, 61, e02015–e02016. [Google Scholar] [CrossRef] [PubMed]
- Werth, B.J.; Sakoulas, G.; Rose, W.E.; Pogliano, J.; Tewhey, R.; Rybak, M.J. Ceftaroline increases membrane binding and enhances the activity of daptomycin against daptomycin-nonsusceptible vancomycin-intermediate Staphylococcus aureus in a pharmacokinetic/pharmacodynamic model. Antimicrob. Agents Chemother. 2013, 57, 66–67. [Google Scholar] [CrossRef] [PubMed]
- Zasowski, E.J.; Trinh, T.D.; Claeys, K.C.; Lagnf, A.M.; Bhatia, S.; Klinker, K.P.; Veve, M.P.; Estrada, S.J.; Johns, S.T.; Sawyer, A.J.; et al. Multicenter cohort study of ceftaroline versus daptomycin for treatment of methicillin-resistant Staphylococcus aureus bloodstream infection. Open Forum. Infect. Dis. 2021, 9, ofab606. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.S.; Sud, A.; O’Sullivan, M.V.N.; Robinson, J.O.; Ferguson, P.E.; Foo, H.; van Hal, S.J.; Ralph, A.P.; Howden, B.P.; Binks, P.M.; et al. Combination of vancomycin and beta-lactam therapy for methicillin-resistant Staphylococcus aureus bacteremia: A pilot multicenter randomized controlled trial. Clin. Infect. Dis. 2016, 62, 173–180. [Google Scholar] [CrossRef]
- Sakoulas, G.; Moise, P.A.; Casapao, A.M.; Nonejuie, P.; Olson, J.; Okumura, C.Y.; Rybak, M.J.; Kullar, R.; Dhand, A.; Rose, W.E.; et al. Antimicrobial salvage therapy for persistent staphylococcal bacteremia using daptomycin plus ceftaroline. Clin. Ther. 2014, 36, 1317–1333. [Google Scholar] [CrossRef]
- Dhand, A.; Sakoulas, G. Daptomycin in combination with other antibiotics for the treatment of complicated methicillin-resistant Staphylococcus aureus bacteremia. Clin. Ther. 2014, 36, 1303–1316. [Google Scholar] [CrossRef]
- Jorgensen, S.C.J.; Zasowski, E.J.; Trinh, T.D.; Lagnf, A.M.; Bhatia, S.; Sabagha, N.; Abdul-Mutakabbir, J.C.; Alosaimy, S.; Mynatt, R.P.; Davis, S.L.; et al. Daptomycin plus beta-lactam combination therapy for methicillin-resistant Staphylococcus aureus bloodstream infections: A retrospective, comparative cohort study. Clin. Infect. Dis. 2019, 20, 1–10. [Google Scholar] [CrossRef]
- Barber, K.E.; Werth, B.J.; Rybak, M.J. The combination of ceftaroline plus daptomycin allows for therapeutic de-escalation and daptomycin sparing against MRSA. J. Antimicrob. Chemother. 2015, 70, 505–509. [Google Scholar] [CrossRef]
- Cortes-Penfield, N.; Oliver, N.T.; Hunter, A.; Rodriguez-Barradas, M. Daptomycin and combination daptomycin-ceftaroline as salvage therapy for persistent methicillin-resistant Staphylococcus aureus bacteremia. Infect. Dis. 2018, 50, 643–647. [Google Scholar] [CrossRef]
- Geriak, M.; Haddad, F.; Rizvi, K.; Rose, W.; Kullar, R.; LaPlante, K.; Yu, M.; Vasina, L.; Ouellette, K.; Zervos, M.; et al. Clinical data on daptomycin plus ceftaroline versus standard of care monotherapy in the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother. 2019, 63, e02483-18. [Google Scholar] [CrossRef]
- McCreary, E.K.; Kullar, R.; Geriak, M.; Zasowski, E.J.; Rizvi, K.; Schulz, L.T.; Ouellette, K.; Vasina, L.; Haddad, F.; Rybak, M.J.; et al. Multicenter cohort of patients with methicillin-resistant Staphylococcus aureus bacteremia receiving daptomycin plus ceftaroline compared with other MRSA treatments. Open Forum. Infect. Dis. 2019, 7, ofz538. [Google Scholar] [CrossRef] [PubMed]
- Morrisette, T.; Lagnf, A.M.; Alosaimy, S.; Rybak, M.J. A comparison of daptomycin alone and in combination with ceftaroline fosamil for methicillin-resistant Staphylococcus aureus bacteremia complicated by septic pulmonary emboli. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2199–2203. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, O.; Crawford, T.N.; Myint, T. Comparing the outcomes of ceftaroline plus vancomycin or daptomycin combination therapy versus monotherapy in adults with complicated and prolonged methicillin-resistant Staphylococcus aureus bacteremia initially treated with supplemental ceftaroline. Infect. Dis. Ther. 2020, 9, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.M.; Molina, K.C.; Miller, M.A.; Kiser, T.H.; Huang, M.; Mueller, S.W. Combination ceftaroline and daptomycin salvage therapy for complicated methicillin-resistant Staphylococcus aureus bacteraemia compared with standard of care. Int. J. Antimicrob. Agents 2021, 57, 106310. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Chen, I.; Yang, Y. Doripenem in the Treatment of Patients with Nosocomial Pneumonia: A Meta-Analysis. J. Clin. Med. 2022, 11, 4014. [Google Scholar] [CrossRef]
- Ye, C.; Wang, Z.; Hu, Y.; Deng, C.; Liao, L.; Sun, L.; Wang, C. Systematic review and meta-analysis of the efficacy and safety of vancomycin combined with β-lactam antibiotics in the treatment of methicillin-resistant Staphylococcus aureus bloodstream infections. J. Glob. Antimicrob. Resist. 2020, 23, 303–310. [Google Scholar] [CrossRef]
- Wang, C.; Ye, C.; Liao, L.; Wang, Z.; Hu, Y.; Deng, C.; Liu, L. Adjuvant β-lactam therapy combined with vancomycin or daptomycin for methicillin-resistant Staphylococcus aureus bacteremia: A systematic review and meta-analysis. Antimicrob. Agents Chemother. 2020, 64, e01377-20. [Google Scholar] [CrossRef]
- Kale-Pradhan, P.B.; Giuliano, C.; Jongekrijg, A.; Rybak, M.J. Combination of vancomycin or daptomycin and beta-lactam antibiotics: A meta-analysis. Pharmacotherapy 2020, 40, 648–658. [Google Scholar] [CrossRef]
- Yi, Y.H.; Wang, J.L.; Yin, W.J.; Xu, W.H. Vancomycin or daptomycin Plus a β-lactam versus vancomycin or daptomycin alone for methicillin-resistant Staphylococcus aureus bloodstream infections: A systematic review and meta-analysis. Microb. Drug Resist. 2021, 27, 1044–1056. [Google Scholar] [CrossRef]
- Lodise, T.P.; Drusano, G.L.; Zasowski, E.; Dihmess, A.; Lazariu, V.; Cosler, L.; McNutt, L.A. Vancomycin exposure in patients with methicillin-resistant Staphylococcus aureus bloodstream infections: How much is enough? Clin. Infect. Dis. 2014, 59, 666–675. [Google Scholar] [CrossRef]
- Casapao, A.M.; Jacobs, D.M.; Bowers, D.R.; Beyda, N.D.; Dilworth, T.J. Early administration of adjuvant blactam therapy in combination with vancomycin among patients with methicillin-resistant Staphylococcus aureus bloodstream infection: A retrospective, multicenter analysis. Pharmacotherapy 2017, 37, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, R.; Morata, L.; Boeing, C.; Subirana, I.; Seifert, H.; Rieg, S.; Kern, W.V.; Kim, H.B.; Kim, E.S.; Liao, C.H.; et al. Defining persistent Staphylococcus aureus bacteraemia: Secondary analysis of a prospective cohort study. Lancet Infect. Dis. 2020, 20, 1409–1417. [Google Scholar] [CrossRef]
- Minejima, E.; Mai, N.; Bui, N.; Mert, M.; Mack, W.J.; She, R.C.; Nieberg, P.; Spellberg, B.; Wong-Beringer, A. Defining the Breakpoint Duration of Staphylococcus aureus Bacteremia Predictive of Poor Outcomes. Clin. Infect. Dis. 2020, 70, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Souli, M.; Ruffin, F.; Choi, S.H.; Park, L.P.; Gao, S.; Lent, N.C.; Sharma-Kuinkel, B.K.; Thaden, J.T.; Maskarinec, S.A.; Wanda, L.; et al. Changing characteristics of Staphylococcus aureus bacteremia: Results from a 21-Year, prospective, longitudinal study. Clin. Infect. Dis. 2019, 69, 1868–1877. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Region | Study Type | Initial or Salvage Therapy | Primary Infection Site | Drug Dosage | Duration of Bacteremia |
|---|---|---|---|---|---|---|
| Cortes-Penfield N, 2018 [29] | USA | RET | Salvage | Multiple | DAP: 5.7–13.8 mg/kg/day CPT: no data | MON: 12.0 days COM: 15.2 days |
| Geriak M, 2019 [30] | USA | RCT | Initial | Multiple | DAP: 6–8 mg/kg/day CPT: 600 mg q8h | MON: 3 days COM: 3 days |
| McCreary EK, 2019 [31] | USA | RET | Initial and salvage | Multiple | DAP: 8.2 mg/kg/day CPT: 600 mg q8h | MON: 4.8 days COM: 3.3 days |
| Morrisette T, 2020 [32] | USA | RET | Salvage | Multiple (Most IE) | DAP: 8.4–9.9 mg/kg/day CPT: 600 mg q8h | MON: 6.7 days COM: 7.6 days |
| Ahmad O, 2020 [33] | USA | RET | Salvage | IE, brain abscess, OMS | DAP: 8–10 mg/kg/day VAN:15–20 mg/kg, q12h-q8h CPT: 600 mg q12h-q8h | MON: 6.0 days COM: 6.0 days |
| Johnson TM, 2021 [34] | USA | RET | Salvage | Multiple | DAP: 100 mg/kg/day CPT: 600 mg q8h | MON: 5.0 days COM: 9.0 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.; Chen, I.; Lin, L. Comparing the Outcomes of Ceftaroline plus Vancomycin or Daptomycin Combination Therapy versus Vancomycin or Daptomycin Monotherapy in Adults with Methicillin-Resistant Staphylococcus aureus Bacteremia—A Meta-Analysis. Antibiotics 2022, 11, 1104. https://doi.org/10.3390/antibiotics11081104
Huang C, Chen I, Lin L. Comparing the Outcomes of Ceftaroline plus Vancomycin or Daptomycin Combination Therapy versus Vancomycin or Daptomycin Monotherapy in Adults with Methicillin-Resistant Staphylococcus aureus Bacteremia—A Meta-Analysis. Antibiotics. 2022; 11(8):1104. https://doi.org/10.3390/antibiotics11081104
Chicago/Turabian StyleHuang, Chienhsiu, Ihung Chen, and Lichen Lin. 2022. "Comparing the Outcomes of Ceftaroline plus Vancomycin or Daptomycin Combination Therapy versus Vancomycin or Daptomycin Monotherapy in Adults with Methicillin-Resistant Staphylococcus aureus Bacteremia—A Meta-Analysis" Antibiotics 11, no. 8: 1104. https://doi.org/10.3390/antibiotics11081104
APA StyleHuang, C., Chen, I., & Lin, L. (2022). Comparing the Outcomes of Ceftaroline plus Vancomycin or Daptomycin Combination Therapy versus Vancomycin or Daptomycin Monotherapy in Adults with Methicillin-Resistant Staphylococcus aureus Bacteremia—A Meta-Analysis. Antibiotics, 11(8), 1104. https://doi.org/10.3390/antibiotics11081104