
Diagnostic Value of CRP and Serum WBC Count during Septic Two-Stage Revision of Total Hip Arthroplasties

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Research Workflow
2.2. Treatment Protocol
2.3. Laboratory Parameters
2.4. Statistical Analyses
3. Results
3.1. Collective
3.2. Treatment Response
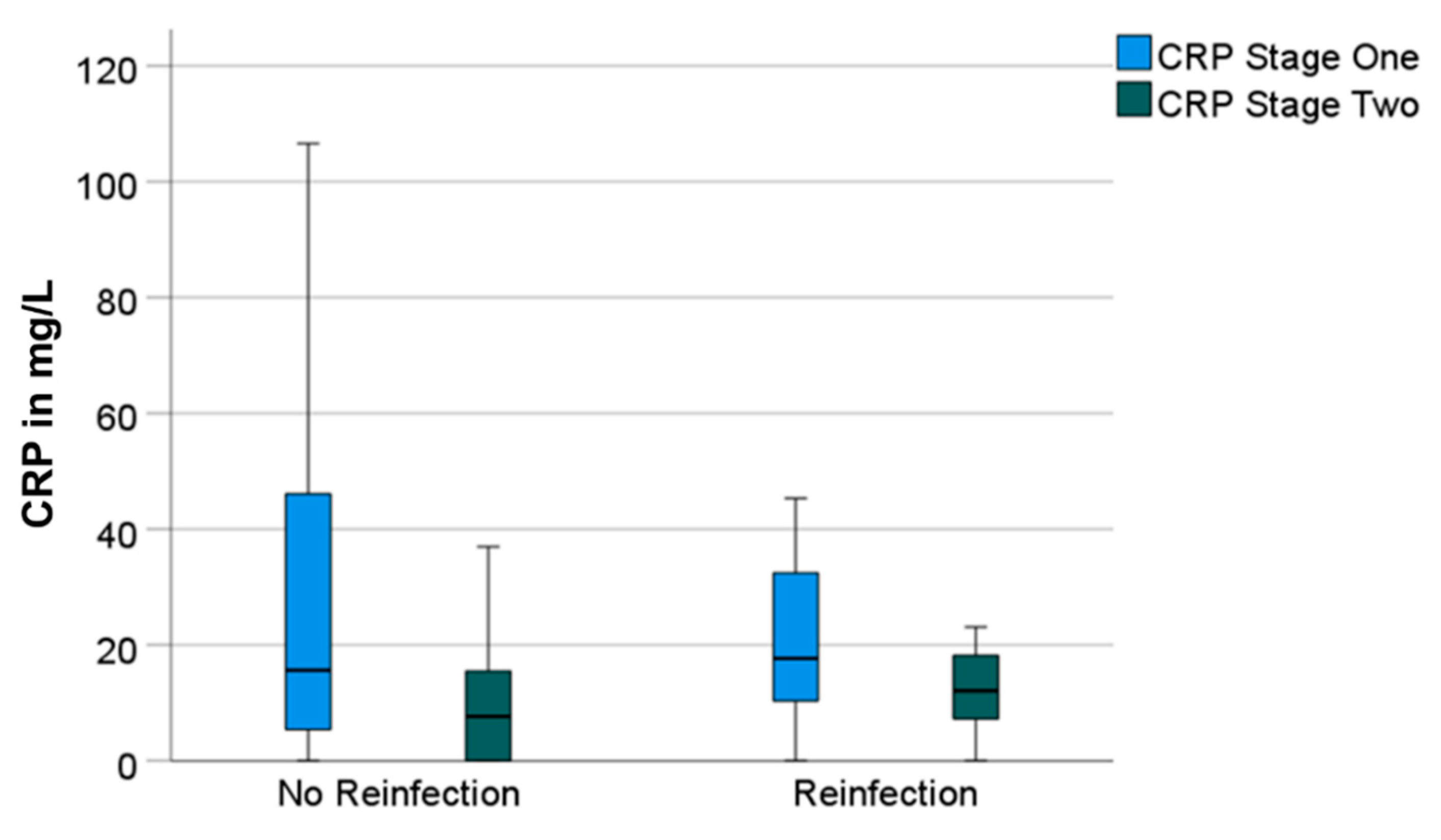
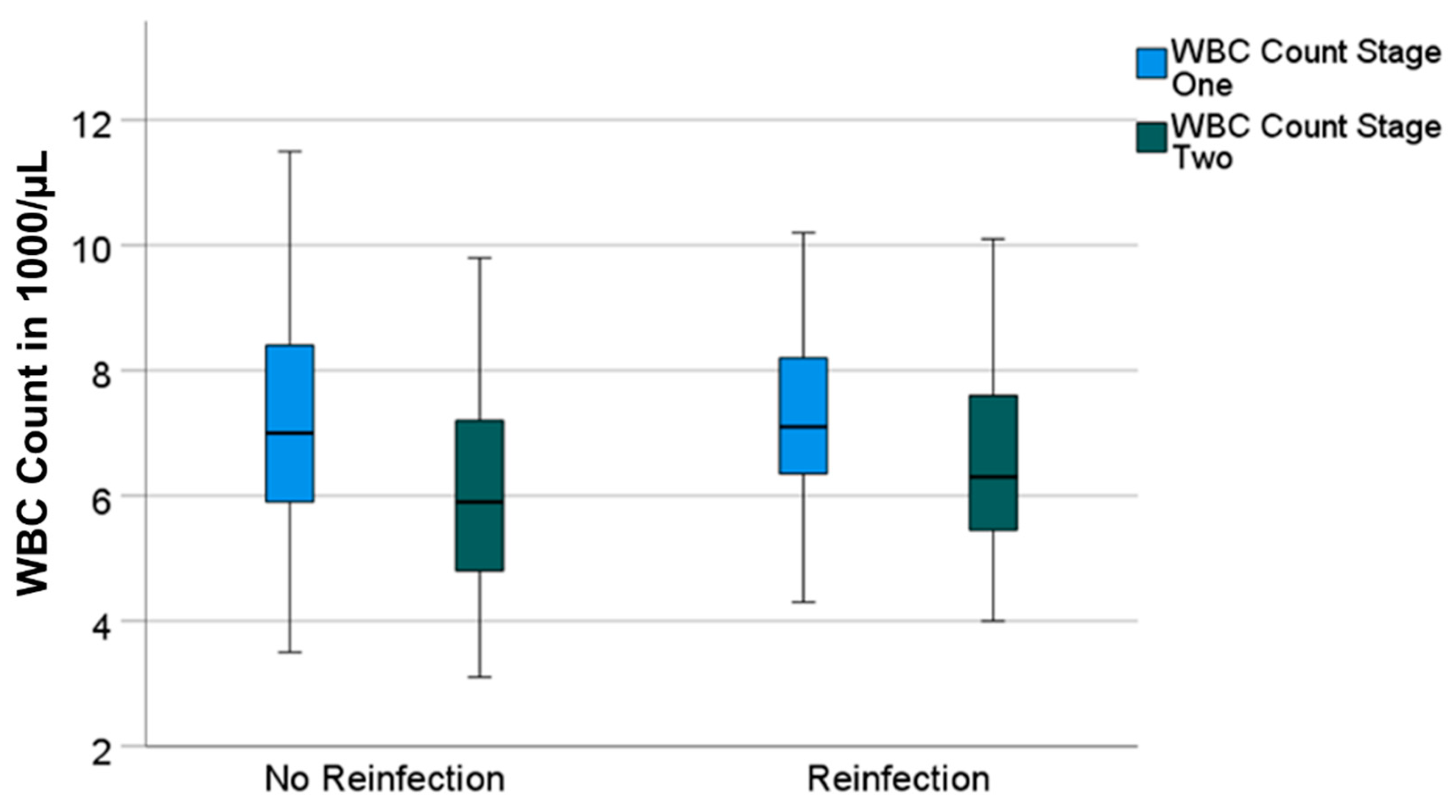
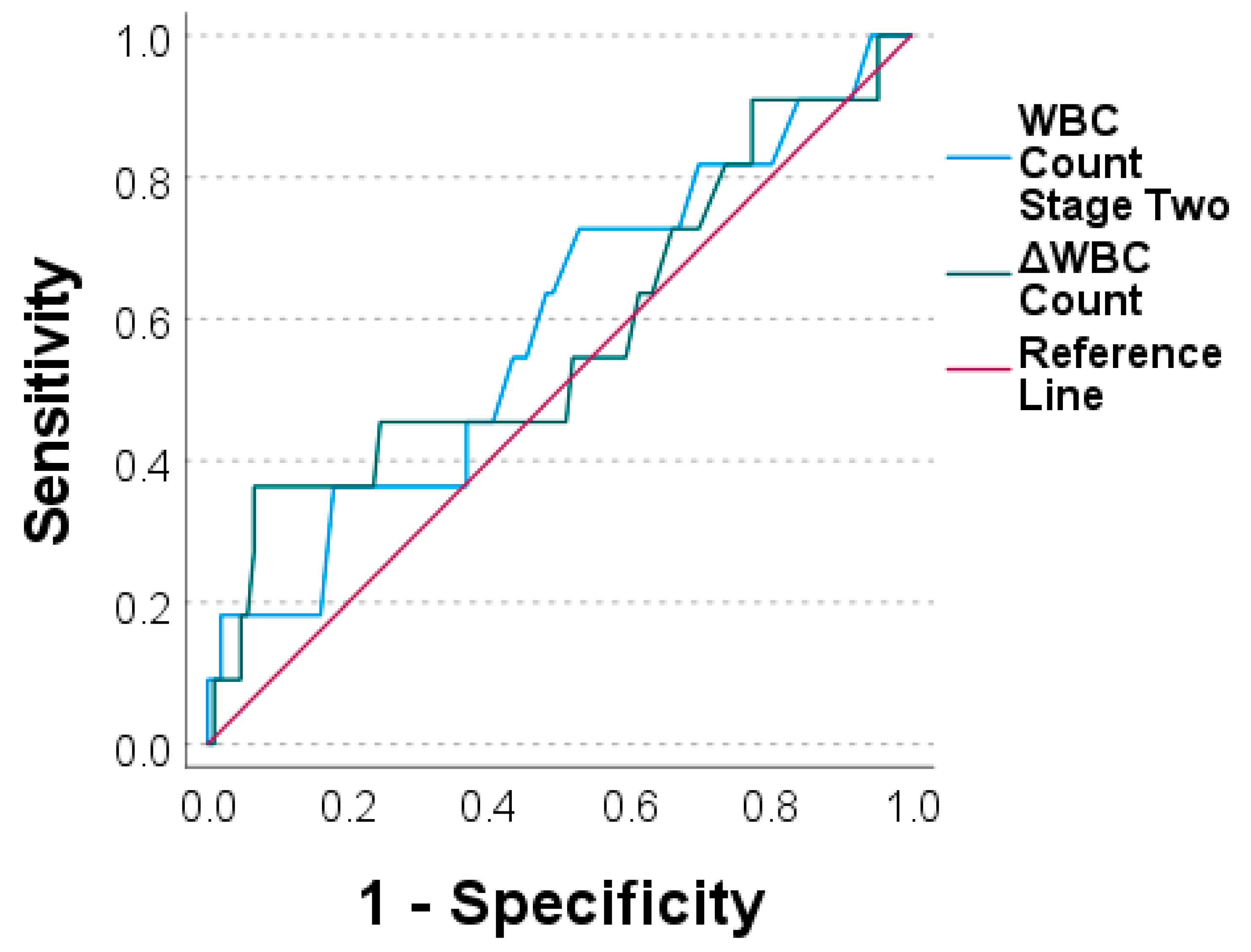
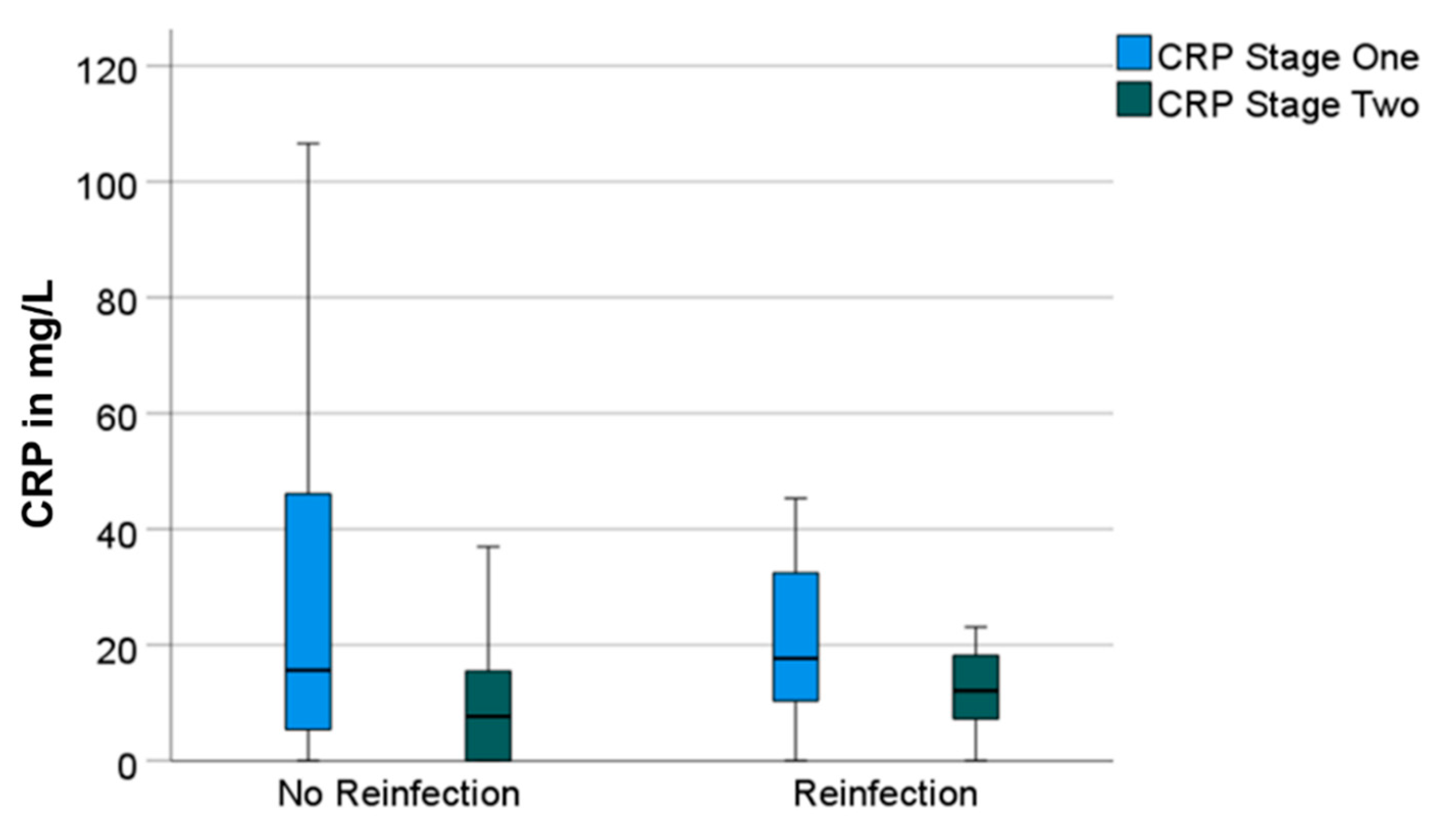
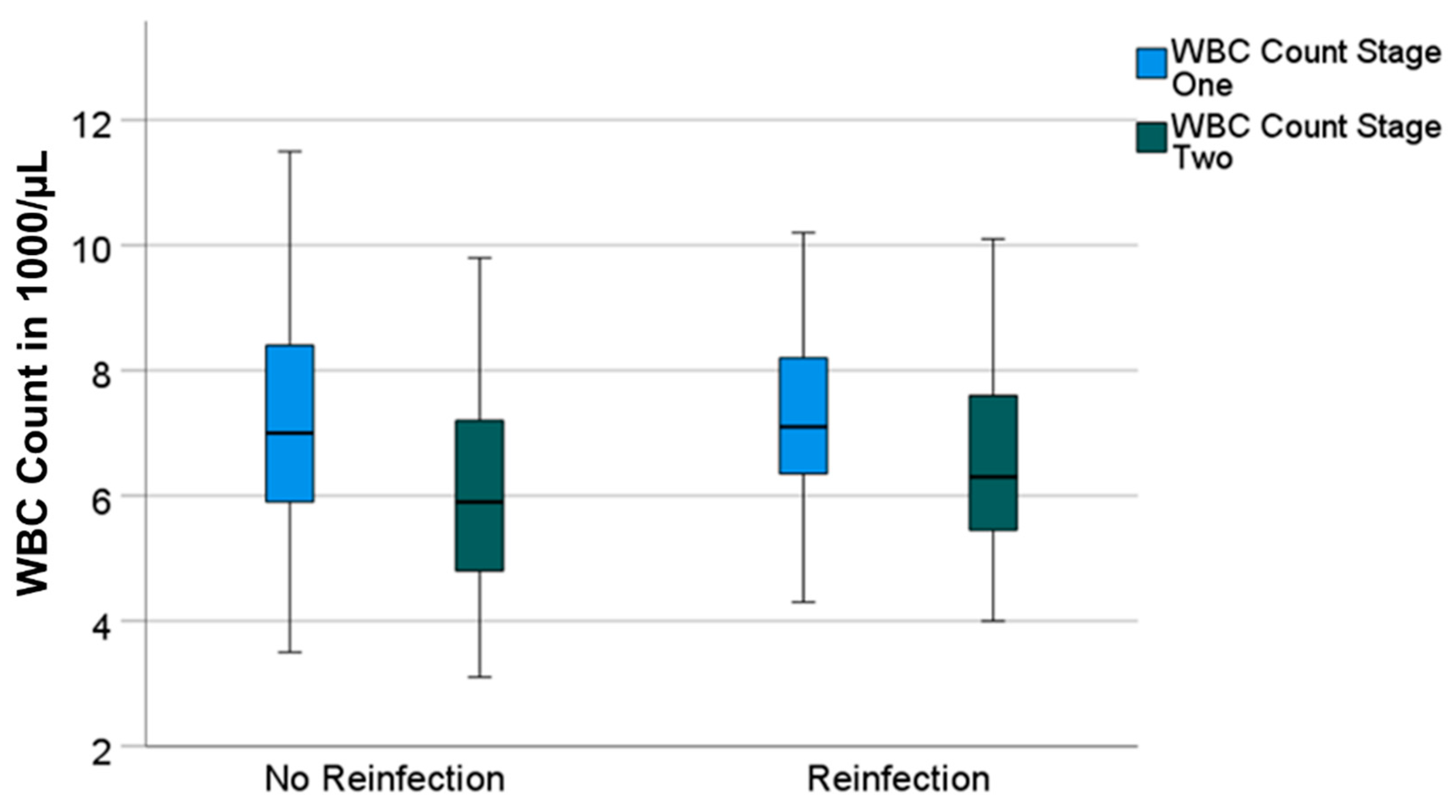
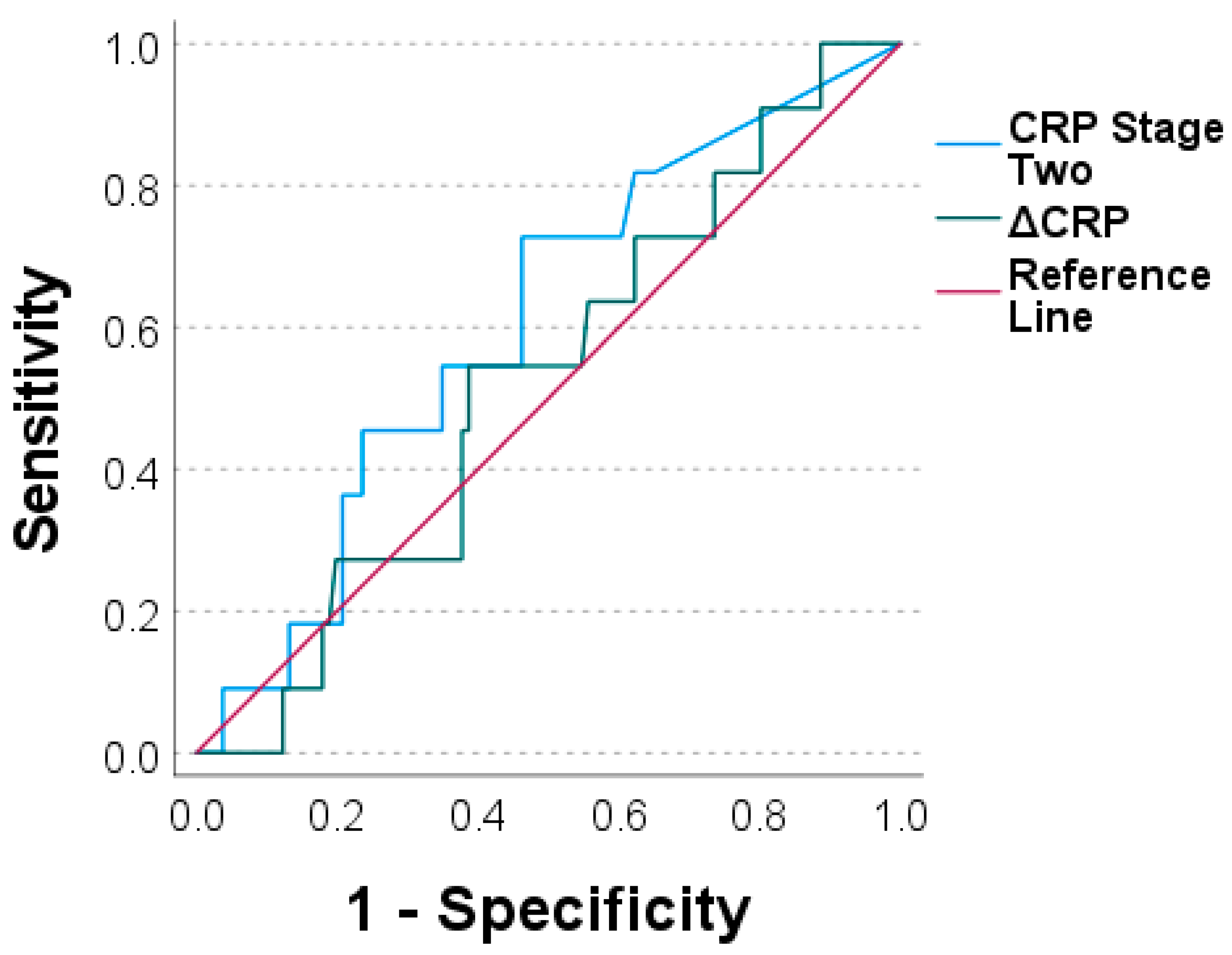
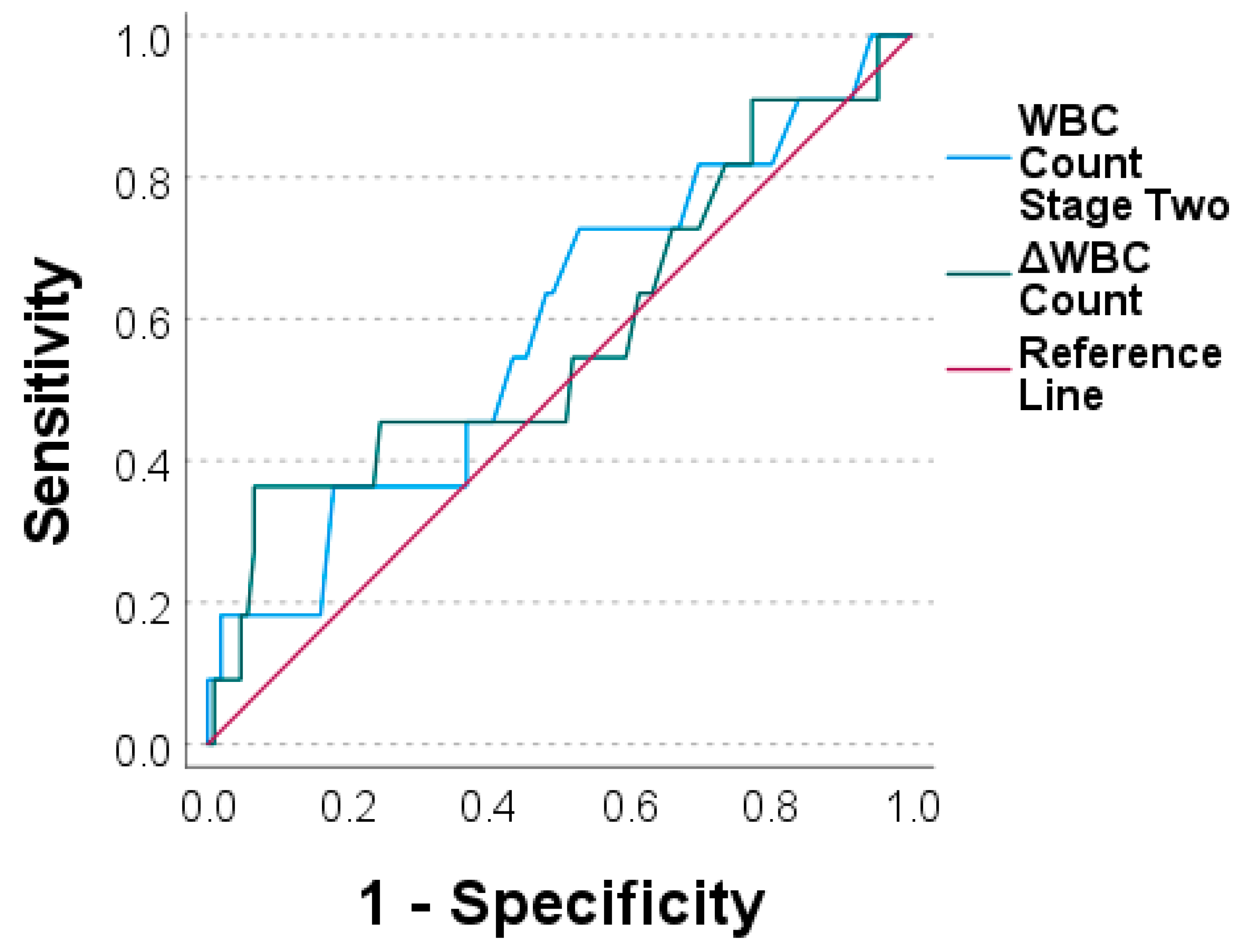
3.3. Diagnostic Value and Determination of Optimal Threshold
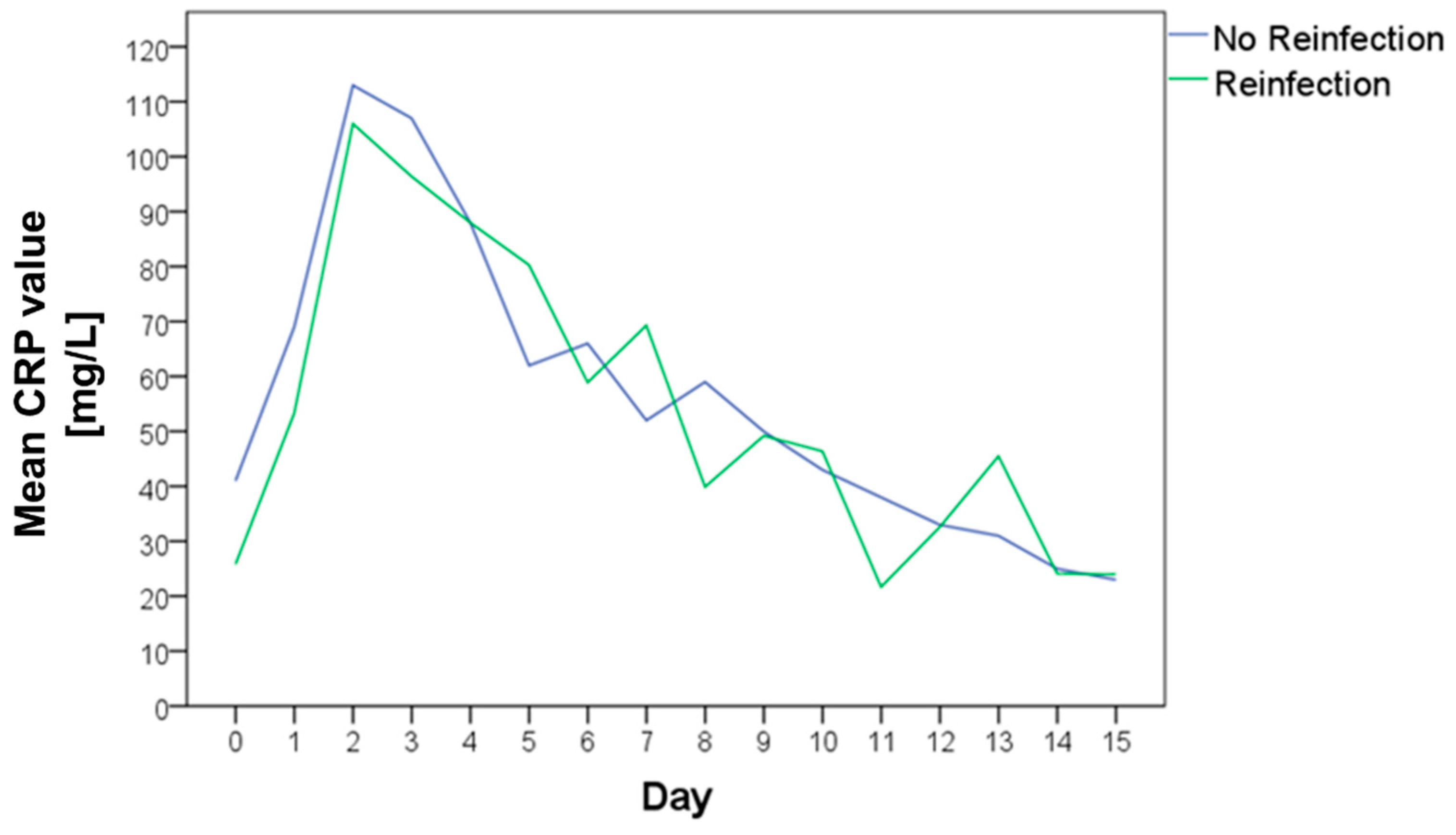
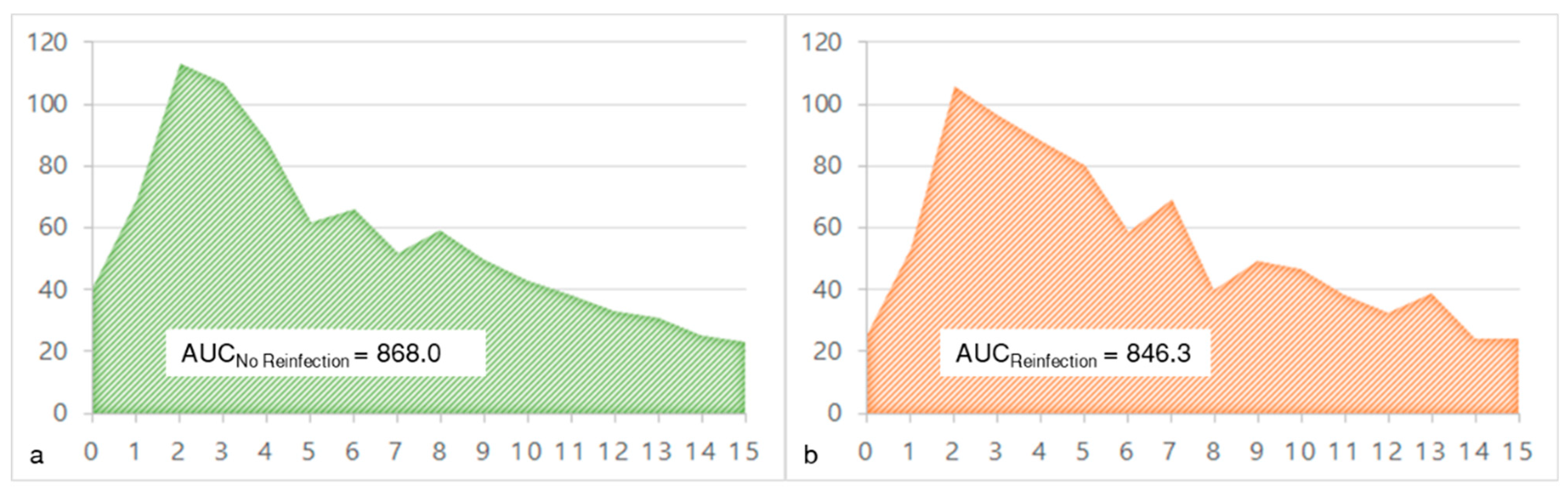
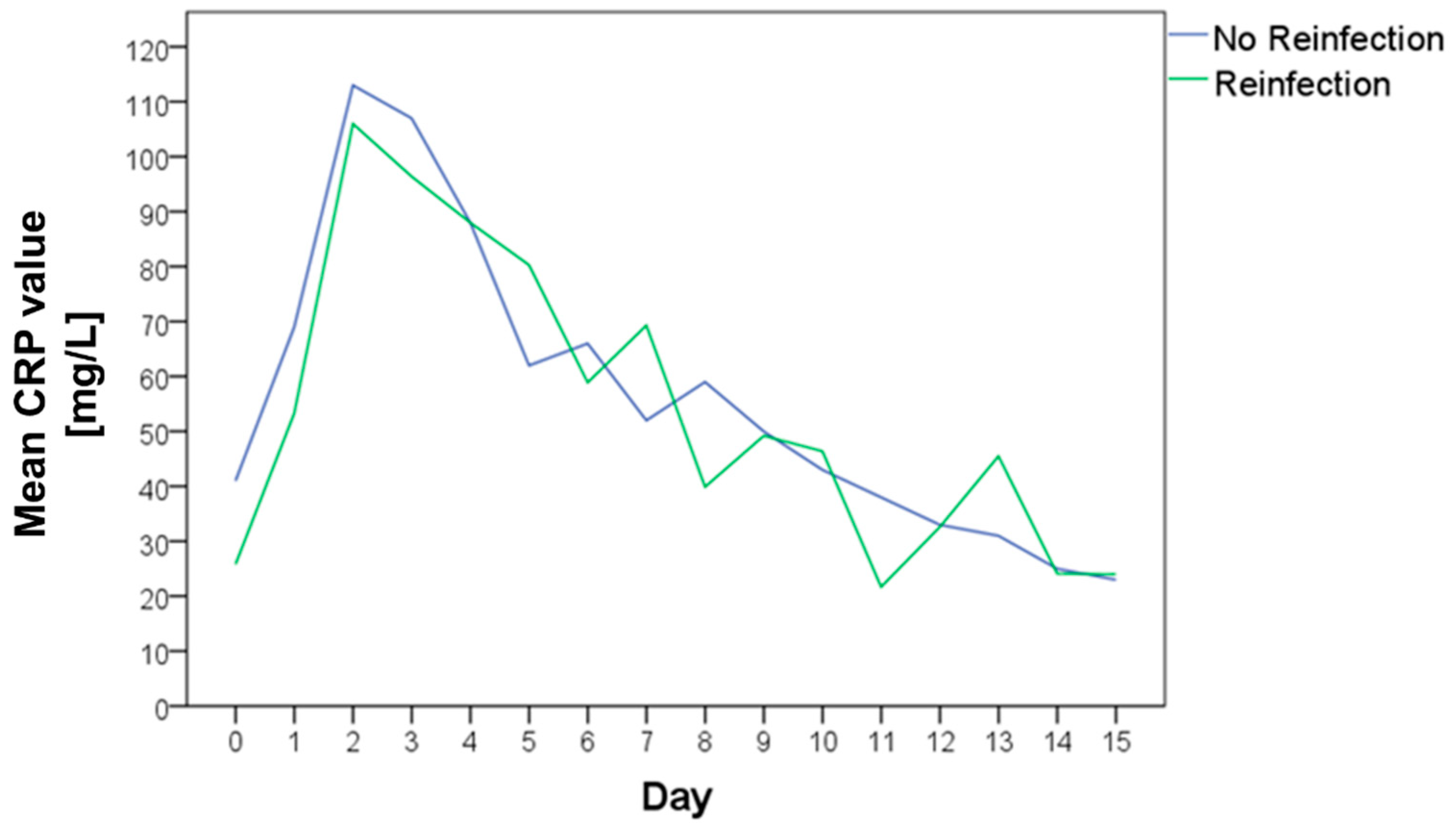
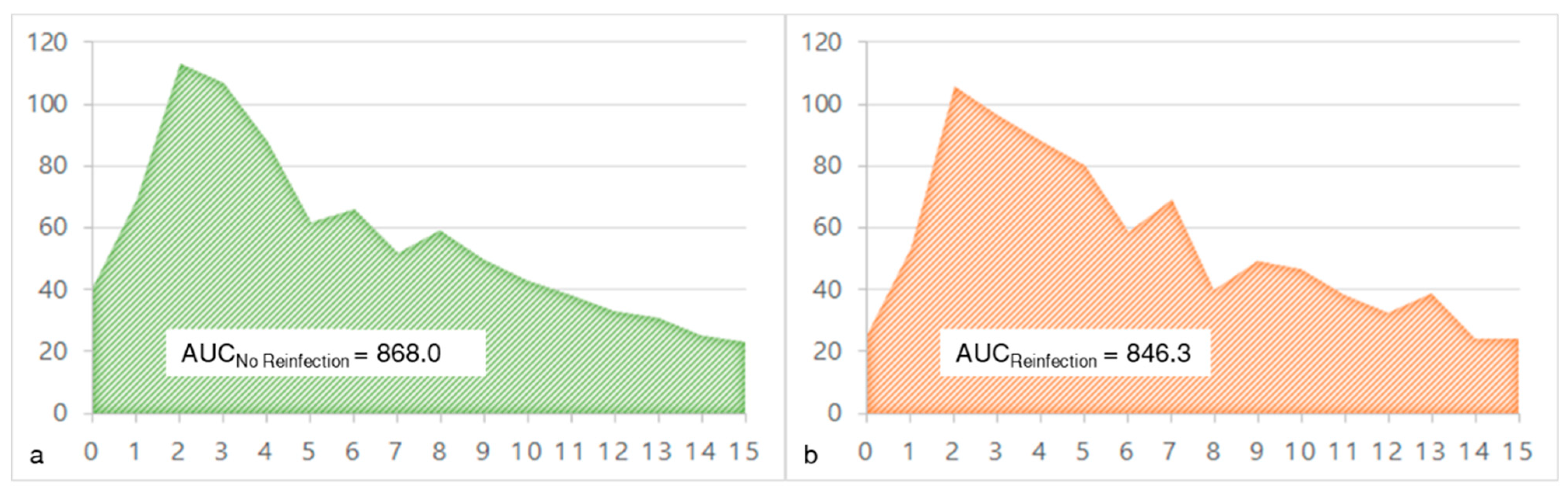
3.4. CRP Course in the Interim Phase
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamagni, T. Epidemiology and burden of prosthetic joint infections. J. Antimicrob. Chemother. 2014, 69 (Suppl. S1), i5–i10. [Google Scholar] [CrossRef] [PubMed]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Garvin, K.L.; Hanssen, A.D. Infection after total hip arthroplasty. Past, present, and future. J. Bone Joint Surg. Am. 1995, 77, 1576–1588. [Google Scholar] [CrossRef] [PubMed]
- Fink, B. Revision of late periprosthetic infections of total hip endoprostheses: Pros and cons of different concepts. Int. J. Med. Sci. 2009, 6, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Cui, Q.; Mihalko, W.M.; Shields, J.S.; Ries, M.; Saleh, K.J. Antibiotic-impregnated cement spacers for the treatment of infection associated with total hip or knee arthroplasty. J. Bone Joint Surg. Am. 2007, 89, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.S.; Kelly, M.A.; Hanssen, A.D.; Barrack, R.L. Technique and timing of two-stage exchange for infection in TKA. Clin. Orthop. Relat. Res. 2007, 464, 164–178. [Google Scholar] [CrossRef]
- Garvin, K.L.; Evans, B.G.; Salvati, E.A.; Brause, B.D. Palacos gentamicin for the treatment of deep periprosthetic hip infections. Clin. Orthop. Relat. Res. 1994, 298, 97–105. [Google Scholar] [CrossRef]
- Fink, B.; Grossmann, A.; Fuerst, M.; Schafer, P.; Frommelt, L. Two-stage cementless revision of infected hip endoprostheses. Clin. Orthop. Relat. Res. 2009, 467, 1848–1858. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, J.R.; Callaway, G.H.; Salvati, E.A.; Pellicci, P.M.; Brause, B.D. Treatment of the infected total hip arthroplasty with a two-stage reimplantation protocol. Clin. Orthop. Relat. Res. 1994, 301, 205–212. [Google Scholar] [CrossRef]
- Mederake, M.; Hofmann, U.K.; Fink, B. New Technique for Custom-Made Spacers in Septic Two-Stage Revision of Total Hip Arthroplasties. Antibiotics 2021, 10, 1073. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Ni, M.; Li, H.; Li, X.; Chai, W.; Zhou, Y.; Hao, L.; Chen, J. The proper timing of second-stage revision in treating periprosthetic knee infection: Reliable indicators and risk factors. J. Orthop. Surg. Res. 2018, 13, 214. [Google Scholar] [CrossRef] [PubMed]
- Kusuma, S.K.; Ward, J.; Jacofsky, M.; Sporer, S.M.; Della Valle, C.J. What is the role of serological testing between stages of two-stage reconstruction of the infected prosthetic knee? Clin. Orthop. Relat. Res. 2011, 469, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Stambough, J.B.; Curtin, B.M.; Odum, S.M.; Cross, M.B.; Martin, J.R.; Fehring, T.K. Does Change in ESR and CRP Guide the Timing of Two-stage Arthroplasty Reimplantation? Clin. Orthop. Relat. Res. 2019, 477, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Fu, J.; Chai, W.; Hao, L.B.; Zhou, Y.G.; Xu, C.; Chen, J.Y. Changes in serum markers failed to predict persistent infection after two-stage exchange arthroplasty. J. Orthop. Surg. Res. 2020, 15, 382. [Google Scholar] [CrossRef]
- Muhlhofer, H.M.L.; Knebel, C.; Pohlig, F.; Feihl, S.; Harrasser, N.; Schauwecker, J.; von Eisenhart-Rothe, R. Synovial aspiration and serological testing in two-stage revision arthroplasty for prosthetic joint infection: Evaluation before reconstruction with a mean follow-up of twenty seven months. Int. Orthop. 2018, 42, 265–271. [Google Scholar] [CrossRef]
- Shukla, S.K.; Ward, J.P.; Jacofsky, M.C.; Sporer, S.M.; Paprosky, W.G.; Della Valle, C.J. Perioperative testing for persistent sepsis following resection arthroplasty of the hip for periprosthetic infection. J. Arthroplast. 2010, 25, 87–91. [Google Scholar] [CrossRef]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetic joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314. [Google Scholar] [CrossRef]
- Fink, B.; Rechtenbach, A.; Buchner, H.; Vogt, S.; Hahn, M. Articulating spacers used in two-stage revision of infected hip and knee prostheses abrade with time. Clin. Orthop. Relat. Res. 2011, 469, 1095–1102. [Google Scholar] [CrossRef]
- Fink, B.; Oremek, D. The Transfemoral Approach for Removal of Well-Fixed Femoral Stems in 2-Stage Septic Hip Revision. J. Arthroplast. 2016, 31, 1065–1071. [Google Scholar] [CrossRef]
- Fink, B.; Vogt, S.; Reinsch, M.; Buchner, H. Sufficient release of antibiotic by a spacer 6 weeks after implantation in two-stage revision of infected hip prostheses. Clin. Orthop. Relat. Res. 2011, 469, 3141–3147. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success after treatment of periprosthetic joint infection: A Delphi-based international multidisciplinary consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.E.; Bachmann, L.M.; Jaeschke, R. A readers' guide to the interpretation of diagnostic test properties: Clinical example of sepsis. Intensive Care Med 2003, 29, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Cao, J.; Zhang, Y.; Ding, W.; Shen, Y. Risk factors for periprosthetic joint infection following primary total hip or knee arthroplasty: A meta-analysis. Int. Wound J. 2017, 14, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Jamsen, E.; Nevalainen, P.; Eskelinen, A.; Huotari, K.; Kalliovalkama, J.; Moilanen, T. Obesity, diabetes, and preoperative hyperglycemia as predictors of periprosthetic joint infection: A single-center analysis of 7181 primary hip and knee replacements for osteoarthritis. J. Bone Joint Surg. Am. 2012, 94, e101. [Google Scholar] [CrossRef] [PubMed]
- Eka, A.; Chen, A.F. Patient-related medical risk factors for periprosthetic joint infection of the hip and knee. Ann. Transl. Med. 2015, 3, 233. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.Y.; Lin, Y.C.; Chang, C.H.; Chen, S.Y.; Lu, T.W.; Lee, S.H. Trend of serum C-reactive protein is associated with treatment outcome of hip Periprosthetic joint infection undergoing two-stage exchange arthroplasty: A case control study. BMC Musculoskelet Disord. 2021, 22, 1007. [Google Scholar] [CrossRef]
- Agrawal, P.; Pandey, A.; Sompura, S.; Pursnani, M.L. Role of blood Creactive protein levels in upper urinary tract infection and lower urinary tract infection in adult patients (>16 years). J. Assoc. Physicians India 2013, 61, 462–463. [Google Scholar]
- Meisner, M.; Adina, H.; Schmidt, J. Correlation of procalcitonin and C-reactive protein to inflammation, complications, and outcome during the intensive care unit course of multiple-trauma patients. Crit. Care 2006, 10, R1. [Google Scholar] [CrossRef]
- Kasapis, C.; Thompson, P.D. The effects of physical activity on serum C-reactive protein and inflammatory markers: A systematic review. J. Am. Coll. Cardiol. 2005, 45, 1563–1569. [Google Scholar] [CrossRef]
- Melbye, H.; Hvidsten, D.; Holm, A.; Nordbo, S.A.; Brox, J. The course of C-reactive protein response in untreated upper respiratory tract infection. Br. J. Gen. Pract. 2004, 54, 653–658. [Google Scholar] [PubMed]
- Aronson, D.; Bartha, P.; Zinder, O.; Kerner, A.; Markiewicz, W.; Avizohar, O.; Brook, G.J.; Levy, Y. Obesity is the major determinant of elevated C-reactive protein in subjects with the metabolic syndrome. Int. J. Obes. Relat. Metab. Disord 2004, 28, 674–679. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reinfection Free | Reinfection | p-Value | |
|---|---|---|---|
| CRP stage one in mg/L (median/range) | 16 (0–357) | 18 (0–115) | 0.793 |
| CRP stage two in mg/L (median/range) | 8 (0–89) | 12 (0–41) | 0.249 |
| ΔCRP (stage two–stage one) in mg/L (median/range) | −11 (−338–79) | −5 (−74–14) | 0.794 |
| WBC count stage one in 1000/µL (median/range) | 7.0 (3.5–16.2) | 7.1 (4.3–11) | 0.848 |
| WBC count stage two in 1000/µL (median/range) | 5.9 (3.1–12.3) | 6.3 (4–12.5) | 0.350 |
| ΔWBC count (stage two–stage one) in 1000/µL (median/range) | −1.0 (−8.7–6.3) | −1.1 (−4.4–4.5) | 0.390 |
| Calculated Threshold Value | Sensitivity | Specificity | |
|---|---|---|---|
| CRP stage two | 8.1 mg/L | 0.727 | 0.538 |
| ΔCRP | −5.1 mg/L | 0.545 | 0.613 |
| WBC count stage two | 5800/µL | 0.727 | 0.472 |
| ΔWBC count | 1150/µL | 0.364 | 0.934 |
| No Reinfection | Reinfection | p-Value | |
|---|---|---|---|
| Preoperatively | 41 ± 64 | 26 ± 34 | 0.913 |
| Day 1 | 69 ± 57 | 53 ± 32 | 0.520 |
| Day 2 | 114 ± 67 | 106 ± 35 | 0.769 |
| Day 3 | 109 ± 54 | 96 ± 27 | 0.692 |
| Day 4 | 88 ± 52 | n.a. | - |
| Day 5 | 62 ± 39 | 80 ± 35 | 0.201 |
| Day 6 | 66 ± 51 | 59 ± 25 | 0.864 |
| Day 7 | 53 ± 44 | 69 ± 46 | 0.311 |
| Day 8 | 58 ± 51 | 40 ± 30 | 0.706 |
| Day 9 | 50 ± 36 | n.a. | - |
| Day 10 | 43 ± 33 | 46 ± 18 | 0.519 |
| Day 11 | 38 ± 26 | 38 ± 22 | 0.769 |
| Day 12 | 33 ± 17 | 33 ± 23 | 0.930 |
| Day 13 | 32 ± 20 | n.a. | - |
| Day 14 | 25 ± 25 | n.a. | - |
| Day 14–21 | 23 ± 24 | 24 ± 8 | 0.436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mederake, M.; Hofmann, U.K.; Benda, S.; Schuster, P.; Fink, B. Diagnostic Value of CRP and Serum WBC Count during Septic Two-Stage Revision of Total Hip Arthroplasties. Antibiotics 2022, 11, 1098. https://doi.org/10.3390/antibiotics11081098
Mederake M, Hofmann UK, Benda S, Schuster P, Fink B. Diagnostic Value of CRP and Serum WBC Count during Septic Two-Stage Revision of Total Hip Arthroplasties. Antibiotics. 2022; 11(8):1098. https://doi.org/10.3390/antibiotics11081098
Chicago/Turabian StyleMederake, Moritz, Ulf K. Hofmann, Sebastian Benda, Philipp Schuster, and Bernd Fink. 2022. "Diagnostic Value of CRP and Serum WBC Count during Septic Two-Stage Revision of Total Hip Arthroplasties" Antibiotics 11, no. 8: 1098. https://doi.org/10.3390/antibiotics11081098
APA StyleMederake, M., Hofmann, U. K., Benda, S., Schuster, P., & Fink, B. (2022). Diagnostic Value of CRP and Serum WBC Count during Septic Two-Stage Revision of Total Hip Arthroplasties. Antibiotics, 11(8), 1098. https://doi.org/10.3390/antibiotics11081098