
Impact of the SARS-CoV-2 Virus Pandemic on Patients with Bronchiectasis: A Multicenter Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
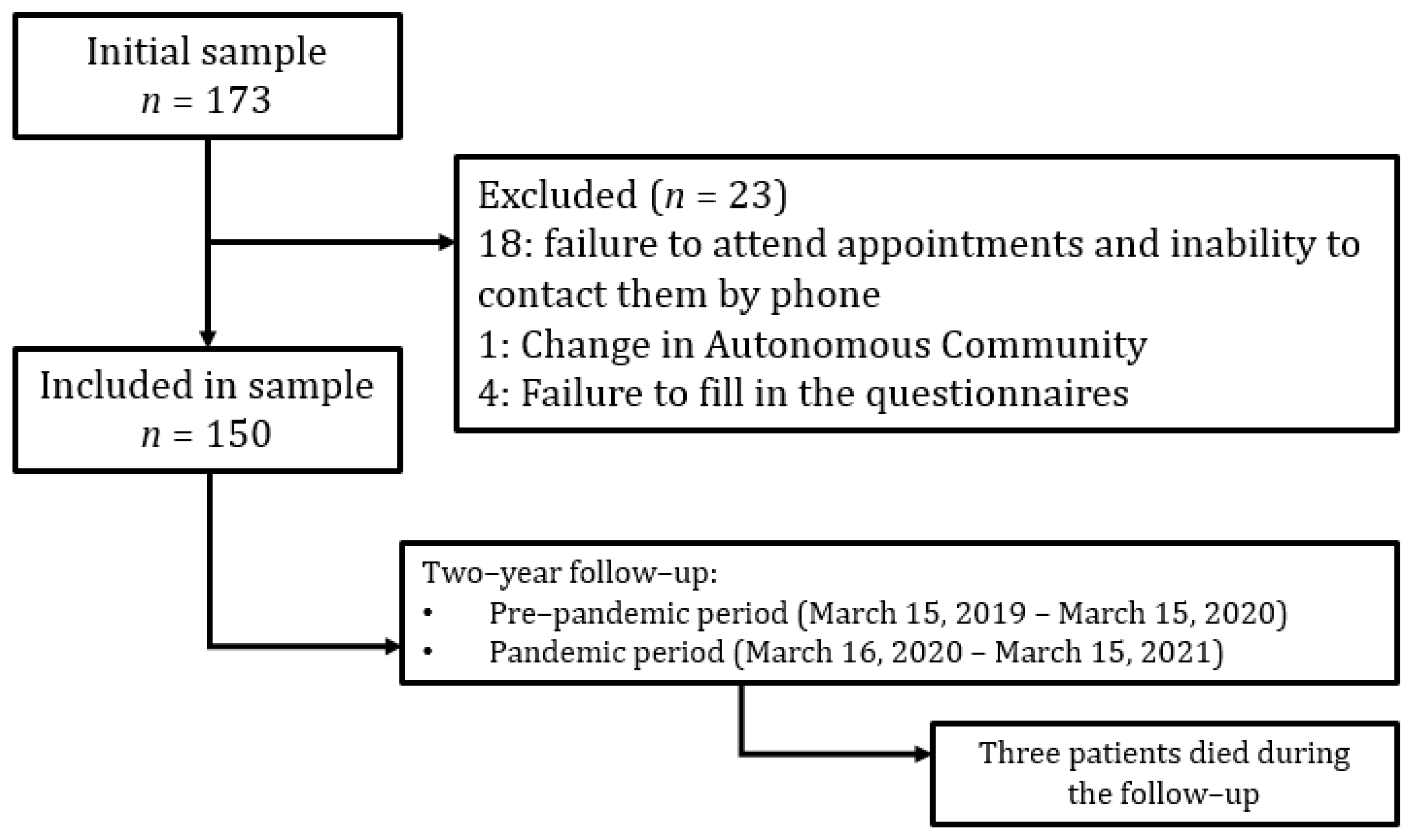
2.1. Study Design
2.2. Criteria for Inclusion and Exclusion
2.3. Follow-Up
2.4. Analyzed Variables
2.4.1. Baseline Variables
2.4.2. Variables Compared between the Pre-Pandemic and Pandemic Periods
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Patients
3.2. Comparison between the Pre-Pandemic and Pandemic Periods
3.2.1. Exacerbations
3.2.2. Microbiological Aspects
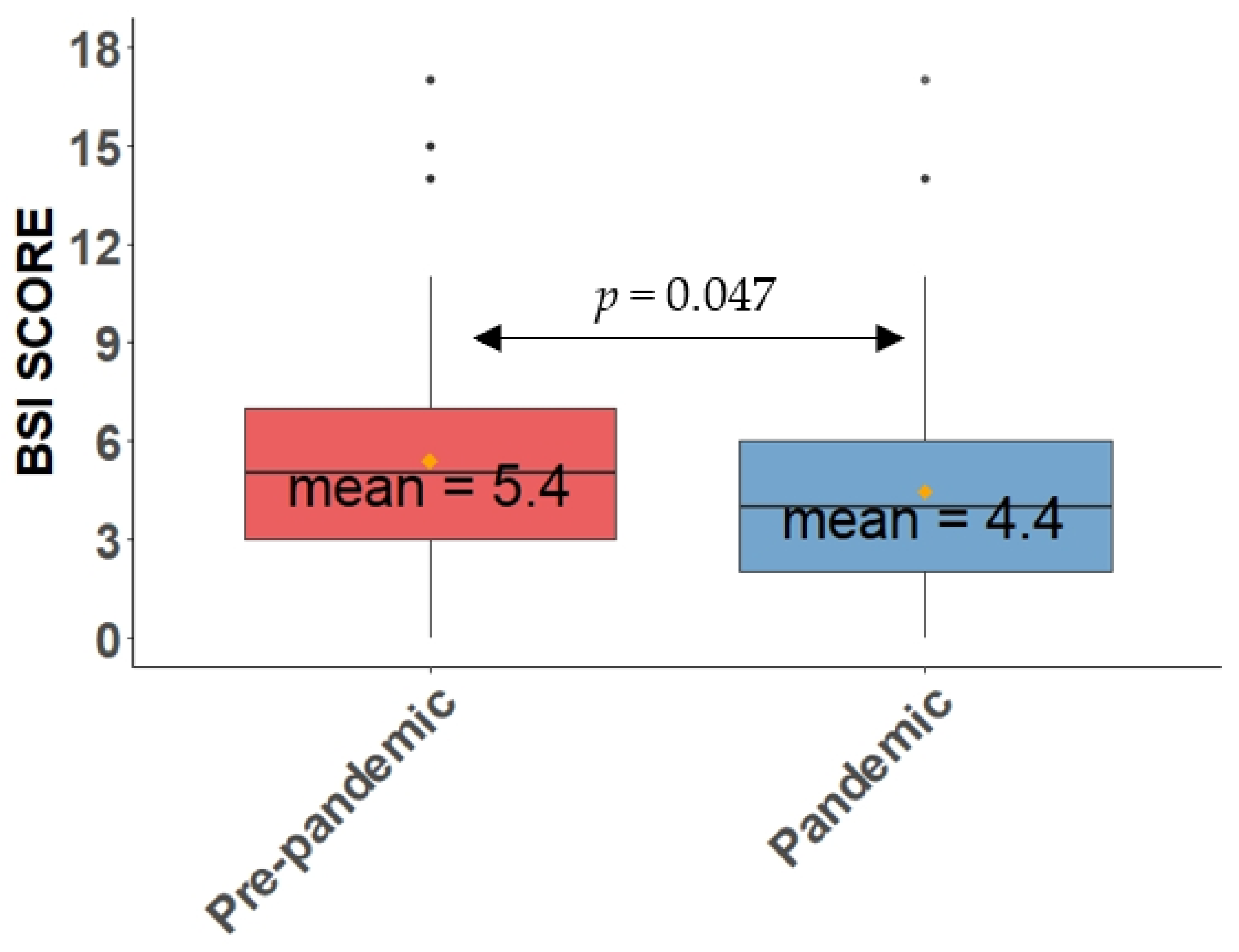
3.2.3. Severity Scores
3.2.4. Quality of Life and Psychomorbidity
3.2.5. Clinical, Functional, Analytical, and Therapeutic Aspects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torres, A.; Arguimbau, M.; Bermejo-Martín, J.; Campo, R.; Ceccato, A.; Fernandez-Barat, L.; Ferrer, R.; Jarillo, N.; Lorente-Balanza, J.; Menéndez, R.; et al. CIBERESUCICOVID: A strategic project for a better understanding and clinical management of COVID-19 in critical patients. Arch Bronconeumol. 2021, 57, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Golpe, R.; Blanco, N.; Castro-Añón, O.; Corredoira, J.; García-Pais, M.J.; Pérez-de-Llano, L.A.; Rabuñal, R.; Romay, E.; Suárez, R. Factors Associated to Hospital Admission in a Care Protocol in COVID-19. Arch Bronconeumol. 2020, 56, 676–677. [Google Scholar] [CrossRef] [PubMed]
- López-Reyes, R.; Oscullo, G.; Jiménez, D.; Cano, I.; García-Ortega, A. Thrombotic Risk and Covid-19: Review of Current Evidence for a Better Diagnostic and Therapeutic Approach. Arch. Bronconeumol. 2021, 57, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Tabernero Huguet, E.; Urrutia Gajarte, A.; Ruiz Iturriaga, L.A.; Serrano Fernandez, L.; Marina Malanda, N.; Iriberri Pascual, M.; Zalacain Jorge, R. Pulmonary Function in Early Follow-up of patients with COVID-19 Pneumonia. Arch. Bronconeumol. 2021, 57, 75–76. [Google Scholar] [CrossRef]
- Posso, M.; Comas, M.; Román, M.; Domingo, L.; Louro, J.; González, C.; Sala, M.; Anglès, A.; Cirera, I.; Cots, F.; et al. Comorbidities and Mortality in Patients With COVID-19 Aged 60 Years and Older in a University Hospital in Spain. Arch. Bronconeumol. 2020, 56, 756–758. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Candal-Pedreira, C.; Fernández-Villar, A.; López-Campos, J.L.; Ruano-Ravina, A. Prognostic Scales of COVID-19 Morbidity and Mortality: Necessary but also Reliable. Arch. Bronconeumol. 2021, 57, 62–63. [Google Scholar] [CrossRef]
- Ahn, D.G.; Shin, H.J.; Kim, M.H.; Lee, S.; Kim, H.S.; Myoung, J.; Kim, B.T.; Kim, S.J. Current Status of Epidemiology, Diagnosis, Therapeutics, and Vaccines for Novel Coronavirus Disease 2019 (COVID-19). J. Microbiol. Biotechnol. 2020, 30, 313–324. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr 2020, 109, 1088–1095. [Google Scholar] [CrossRef]
- Ríos-Barnés, M.; Lanaspa, M.; Noguera-Julian, A.; Baleta, L.; De Sevilla, M.F.; Ferri, D.; Götzens, J.; Jordan, I.; Lecina, L.; Monfort, L.; et al. The Spectrum of COVID-19 Disease in Adolescents. Arch. Bronconeumol. 2021, 57, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Chavasse, R.; Almario, A.; Christopher, A.; Kappos, A.; Shankar, A. The Indirect Impact of COVID-19 on Children With Asthma. Arch. Bronconeumol. 2020, 56, 768–769. [Google Scholar] [CrossRef]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 And Novel Therapeutics Against Coronavirus (COVID-19). In StatPearls [Internet]; StatPearls: Treasure Island, FL, USA, 12 May 2022. [Google Scholar]
- Gülsen, A.; König, I.R.; Jappe, U.; Drömann, D. Effect of comorbid pulmonary disease on the severity of COVID-19: A systematic review and meta-analysis. Respirology 2021, 26, 552–565. [Google Scholar] [CrossRef] [PubMed]
- Burgos Rincón, F.; Martínez Llorens, J.; Cordovilla Pérez, R. Impact of the COVID-19 Pandemic on Lung Function Laboratories: Considerations for “Today” and the “Day After”. Arch. Bronconeumol. 2020, 56, 611–612. [Google Scholar] [CrossRef] [PubMed]
- Alkhathami, M.G.; Advani, S.M.; Abalkhail, A.A.; Alkhathami, F.M.; Alshehri, M.K.; Albeashy, E.E.; Alsalamah, J.A. Prevalence and mortality of lung comorbidities among patients with COVID-19: A systematic review and meta-analysis. Lung India 2021, 38, S31–S40. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo Alonso, J.L.; Rodríguez González-Moro, J.M. Pneumology in the Days of COVID-19. Arch. Bronconeumol. 2020, 56, 1–2. [Google Scholar] [CrossRef]
- Tiotiu, A. Impact of COVID-19 on the Most Frequent Middle and Lower Obstructive Airway Diseases/Syndromes in Adult Population. Arch. Bronconeumol. 2021, 57, 7–8. [Google Scholar] [CrossRef]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef]
- Alcázar-Navarrete, B.; Molina París, J.; Martín Sánchez, F.J. Management and Follow up of Respiratory Patients in the Post-COVID-19 Era: Are We Ready Yet? Arch. Bronconeumol. 2020, 56, 685–686. [Google Scholar] [CrossRef]
- Isea de la Viña, J.; Mayol, J.; Ortega, A.L.; Alcázar Navarrete, B. Lung Cancer Patients on the Waiting List in the Midst of the COVID-19 Crisis: What Do We Do Now? Arch. Bronconeumol. 2020, 56, 602–604. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Vogelmeier, C.F.; Agusti, A.A. COPD & COVID-19. Arch. Bronconeumol. 2021, 57, 162–164. [Google Scholar] [CrossRef] [PubMed]
- de la Rosa Carrillo, D.; Athanazio, R.; Girón Moreno, R.M.; Máiz Carro, L.; Olveira, C.; de Gracia, J.; Vendrell, M.; Prados Sánchez, C.; Gramblicka, G.; Corso Pereira, M.; et al. The annual prognostic ability of FACED and E-FACED scores to predict mortality in patients with bronchiectasis. ERJ Open Res. 2018, 4, 00139-2017. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.H.; Guan, W.J.; Xu, G.; Lin, Z.Y.; Tang, Y.; Lin, Z.M.; Gao, Y.; Li, H.M.; Zhong, N.S.; Zhang, G.J.; et al. The role of viral infection in pulmonary exacerbations of bronchiectasis in adults: A prospective study. Chest 2015, 147, 1635–1643. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Mendes, R.G.; Alghamdi, S.M.; Miravitlles, M.; Mandal, S.; Hurst, J.R. Reduction in hospitalised COPD exacerbations during COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0255659. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.Y.; Conceicao, E.P.; Wee, L.E.; Sim, X.Y.J.; Venkatachalam, I. COVID-19 public health measures: A reduction in hospital admissions for COPD exacerbations. Thorax 2021, 76, 512–513. [Google Scholar] [CrossRef] [PubMed]
- Koutsakos, M.; Wheatley, A.K.; Laurie, K.; Kent, S.J.; Rockman, S. Influenza lineage extinction during the COVID-19 pandemic? Nat. Rev. Microbiol. 2021, 19, 741–742. [Google Scholar] [CrossRef]
- de la Rosa, D.; Martínez-Garcia, M.A.; Olveira, C.; Girón, R.; Máiz, L.; Prados, C. Annual direct medical costs of bronchiectasis treatment: Impact of severity, exacerbations, chronic bronchial colonization and chronic obstructive pulmonary disease coexistence. Chron. Respir. Dis. 2016, 13, 361–371. [Google Scholar] [CrossRef]
- Hernández, C.; Abreu, J.; Jiménez, A.; Fernández, R.; Martín, C. Pulmonary function and quality of life in relation to bronchial colonization in adults with bronchiectasis not caused by cystic fibrosis. Med. Clin. 2002, 118, 130–134. [Google Scholar] [CrossRef]
- Crichton, M.L.; Shoemark, A.; Chalmers, J.D. The Impact of the COVID-19 Pandemic on Exacerbations and Symptoms in Bronchiectasis: A Prospective Study. Am. J. Respir. Crit Care Med. 2021, 204, 857–859. [Google Scholar] [CrossRef]
- Martinez-García, M.A.; Villa, C.; Dobarganes, Y.; Girón, R.; Maíz, L.; García-Clemente, M.; Sibila, O.; Golpe, R.; Rodríguez, J.; Barreiro, E.; et al. RIBRON: The spanish Online Bronchiectasis Registry. Characterization of the First 1912 Patients. Arch. Bronconeumol. 2021, 57, 28–35. [Google Scholar] [CrossRef]
- Martínez-García, M.; Máiz, L.; Olveira, C.; Girón, R.M.; de la Rosa, D.; Blanco, M.; Cantón, R.; Vendrell, M.; Polverino, E.; de Gracia, J.; et al. Spanish Guidelines on Treatment of Bronchiectasis in Adults. Arch. Bronconeumol. 2018, 54, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Webb, W.R.; Müller, N.L.; Naidich, D.P.; Ovid Technologies, I. High-Resolution CT of the Lung, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Aliberti, S.; Goeminne, P.C.; O’Donnell, A.E.; Aksamit, T.R.; Al-Jahdali, H.; Barker, A.F.; Blasi, F.; Boersma, W.G.; Crichton, M.L.; De Soyza, A.; et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: International consensus recommendations. Lancet Respir. Med. 2022, 10, 298–306. [Google Scholar] [CrossRef]
- Ministerio de la Presidencia Relaciones con las Cortes y Memoria Democrática. Gobierno de España. Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la crisis sanitaria ocasionada por el COVID-19. Boletín Oficial del Estado. 2020, 67, 25390–25400. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- McDonnell, M.J.; Aliberti, S.; Goeminne, P.C.; Restrepo, M.I.; Finch, S.; Pesci, A.; Dupont, L.J.; Fardon, T.C.; Wilson, R.; Loebinger, M.R.; et al. Comorbidities and the risk of mortality in patients with bronchiectasis: An international multicentre cohort study. Lancet Respir. Med. 2016, 4, 969–979. [Google Scholar] [CrossRef]
- Murray, M.P.; Pentland, J.L.; Turnbull, K.; MacQuarrie, S.; Hill, A.T. Sputum colour: A useful clinical tool in non-cystic fibrosis bronchiectasis. Eur Respir. J. 2009, 34, 361–364. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef]
- Martínez-García, M.; de Gracia, J.; Vendrell Relat, M.; Girón, R.M.; Máiz Carro, L.; de la Rosa Carrillo, D.; Olveira, C. Multidimensional approach to non-cystic fibrosis bronchiectasis: The FACED score. Eur Respir. J. 2014, 43, 1357–1367. [Google Scholar] [CrossRef]
- McDonnell, M.J.; Aliberti, S.; Goeminne, P.C.; Dimakou, K.; Zucchetti, S.C.; Davidson, J.; Ward, C.; Laffey, J.G.; Finch, S.; Pesci, A.; et al. Multidimensional severity assessment in bronchiectasis: An analysis of seven European cohorts. Thorax 2016, 71, 1110–1118. [Google Scholar] [CrossRef]
- Olveira, C.; Olveira, G.; Espildora, F.; Girón, R.M.; Vendrell, M.; Dorado, A.; Martínez-García, M. Mediterranean diet is associated on symptoms of depression and anxiety in patients with bronchiectasis. Gen. Hosp. Psychiatry 2014, 36, 277–283. [Google Scholar] [CrossRef]
- De la Rosa Carrillo, D.; Olveira, C.; García-Clemente, M.; Girón-Moreno, R.M.; Nieto-Royo, R.; Navarro-Rolon, A.; Prados-Sánchez, C.; Sibila, O.; Martínez-García, M. COPD Assessment Test in Bronchiectasis: Minimum Clinically Important Difference and Psychometric Validation: A Prospective Study. Chest 2020, 157, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Colomo, N.; Olveira, C.; Hernández-Pedrosa, J.; Bergero, T.; Fábrega-Ruz, J.; Porras, N.; Girón, M.V.; de Rota, L.F.; Olveira, G. Validity of Self-rating Screening Scales for the Diagnosis of Depression and Anxiety in Adult Patients With Bronchiectasis. Arch. Bronconeumol. 2021, 57, 179–185. [Google Scholar] [CrossRef]
- Hill, A.T.; Haworth, C.S.; Aliberti, S.; Barker, A.; Blasi, F.; Boersma, W.; Chalmers, J.D.; De Soyza, A.; Dimakou, K.; Elborn, J.S.; et al. Pulmonary exacerbation in adults with bronchiectasis: A consensus definition for clinical research. Eur Respir. J. 2017, 49, 1700051. [Google Scholar] [CrossRef] [PubMed]
- Gleckman, R.; DeVita, J.; Hibert, D.; Pelletier, C.; Martin, R. Sputum gram stain assessment in community-acquired bacteremic pneumonia. J. Clin. Microbiol. 1988, 26, 846–849. [Google Scholar] [CrossRef] [PubMed]
- de la Rosa Carrillo, D.; López-Campos, J.L.; Alcázar Navarrete, B.; Calle Rubio, M.; Cantón Moreno, R.; García-Rivero, J.L.; Máiz Carro, L.; Olveira Fuster, C.; Martínez-García, M.; Documento, C.A.d.; et al. Consensus Document on the Diagnosis and Treatment of Chronic Bronchial Infection in Chronic Obstructive Pulmonary Disease. Arch. Bronconeumol. 2020, 56, 651–664. [Google Scholar] [CrossRef]
- Chen, C.L.; Huang, Y.; Yuan, J.J.; Li, H.M.; Han, X.R.; Martinez-Garcia, M.A.; de la Rosa-Carrillo, D.; Chen, R.C.; Guan, W.J.; Zhong, N.S. The Roles of Bacteria and Viruses in Bronchiectasis Exacerbation: A Prospective Study. Arch. Bronconeumol. 2020, 56, 621–629. [Google Scholar] [CrossRef]
- Martinez-Garcia, M.; Athanazio, R.; Gramblicka, G.; Corso, M.; Cavalcanti Lundgren, F.; Fernandes de Figueiredo, M.; Arancibia, F.; Rached, S.; Girón, R.; Máiz Carro, L.; et al. Prognostic Value of Frequent Exacerbations in Bronchiectasis: The Relationship With Disease Severity. Arch. Bronconeumol. 2019, 55, 81–87. [Google Scholar] [CrossRef]
- Martinez-García, M.A. Infection and exacerbations in bronchiectasis: More questions than answers. Eur Respir. J. 2018, 51, 1702497. [Google Scholar] [CrossRef]
- Monsó, E. Look at the wood and not at the tree: The Microbiome in Chronic Obstructive Lung Disease and Cystic Fibrosis. Arch. Bronconeumol. 2020, 56, 5–6. [Google Scholar] [CrossRef]
- Wilson, R.; Aksamit, T.; Aliberti, S.; De Soyza, A.; Elborn, J.S.; Goeminne, P.; Hill, A.T.; Menendez, R.; Polverino, E. Challenges in managing Pseudomonas aeruginosa in non-cystic fibrosis bronchiectasis. Respir. Med. 2016, 117, 179–189. [Google Scholar] [CrossRef]
- Aliberti, S.; Lonni, S.; Dore, S.; McDonnell, M.J.; Goeminne, P.C.; Dimakou, K.; Fardon, T.C.; Rutherford, R.; Pesci, A.; Restrepo, M.I.; et al. Clinical phenotypes in adult patients with bronchiectasis. Eur Respir. J. 2016, 47, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Finch, S.; McDonnell, M.J.; Abo-Leyah, H.; Aliberti, S.; Chalmers, J.D. A Comprehensive Analysis of the Impact of Pseudomonas aeruginosa Colonization on Prognosis in Adult Bronchiectasis. Ann. Am. Thorac Soc. 2015, 12, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Martinez-García, M.A.; Oscullo, G.; Posadas, T.; Zaldivar, E.; Villa, C.; Dobarganes, Y.; Girón, R.; Olveira, C.; Maíz, L.; García-Clemente, M.; et al. Pseudomonas aeruginosa and lung function decline in patients with bronchiectasis. Clin. Microbiol. Infect. 2021, 27, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Gender
| (76.7%) (23.3%) |
| Age, years | 61.3 ± 16.1 |
| BMI (kg/m2) | 25.3 ± 4.6 |
Smoking
| 93 (62%) 14 (9.3%) 43 (28.17%) |
| Packs-per-year index | 12.6 ± 17.7 |
| Age at diagnosis of BE, years | 50 ± 19.5 |
Etiology
| 74 (49.3%) 17 (11.4%) 13 (8.7%) 10 (6.7%) 9 (6%) 6 (4%) 5 (3.3%) 3 (2%) 3 (2%) 2 (1.3%) 2 (1.3%) 2 (1.3%) 1 (0.7%) 3 (2%) |
Number of pulmonary lobes affected
| 28 (18.7%) 56 (37.3%) 19 (12.7%) 47 (31.4%) |
Distribution
| 48 (32%) 102 (68%) |
| Cystic bronchiectasis | 15 (10%) |
| Charlson Index | 2.9 ± 1.9 |
| BACI Index | 1.66 ± 2.16 |
| FACED | 1.6 ± 1.4 |
| E-FACED | 1.8 ± 1.5 |
| BSI | 5.4 ± 3.6 |
| FEV1 (mL) FEV11 (%) FEV1/FVC | 1861.8 ± 726.5 75.6 ± 25 79.2 ± 17.5 |
| Exacerbations Number of oral antibiotic courses Number of intravenous antibiotic courses Days of oral antibiotic therapy Days of oral intravenous therapy | 1 (1–2) 1 (1–2) 0 (0–0) 14 (6–23.25) 0 (0–0) |
| Pre-Pandemic | Pandemic | p Value | |
|---|---|---|---|
| Courses of oral antibiotic therapy | 1 (1–2) | 0 (0–1) | <0.0001 |
| Courses of intravenous antibiotic therapy | 0 (0–0) | 0 (0–0) | <0.0001 |
Days of oral antibiotic therapy
| 14 (6–23,25) 16.9 ± 16 | 0 (0–14) 7.3 ± 12.5 | <0.0001 <0.001 |
Severe exacerbations
| 0 (0–0) 1.96 ± 5.44 | 0 (0–0) 0.83 ± 3.64 | <0.0001 p = 0.009 |
| Pre-Pandemic n (%) | Pandemic n (%) | p Value | |
|---|---|---|---|
| % patients with at least 1 valid sputum sample | 75.3% | 46.7% | 0.001 |
| Percentage of sputum samples positive for PPM | 58% | 44.7% | 0.012 |
| Percentage of sputum samples positive for PA | 23.3% | 13.3% | 0.013 |
| Percentage of sputum samples positive for HI | 21.3% | 14% | 0.042 |
| Percentage of sputum samples positive for SA | 6% | 8.7% | 0.672 |
| Pre-Pandemic Period | Pandemic Period | p Value | |
|---|---|---|---|
| FACED (m ± SD) | 1.6 ± 1.4 | 1.41 ± 1.4 | 0.065 |
| E-FACED (m ± SD) | 1.8 ± 1.5 | 1.43 ± 1.43 | 0.030 |
| BSI (m ± SD) | 5.4 ± 3.6 | 4.4 ± 3.3 | 0.047 |
| CAT (m ± SD) >10 points | 12.8 ± 7.59 56% | 11.8 ± 6.47 52.7% | 0.519 0.812 |
| HADS-A (m ± SD) >11 points | 6.47 ± 4.54 13.3% | 5.49 ± 4 8% | 0.084 0.059 |
| HADS-D (m ± SD) >11 points | 4.78 ± 4.1 8% | 4.54 ± 3.73 2.7% | 0.877 0.011 |
| Pre-Pandemic | Pandemic | p Value | |
|---|---|---|---|
Dyspnea mMRC n (%)
| 80 (54.1%) 42 (28.4%) 19 (12.8%) 7 (4.7%) 0 (0%) | 77 (52%) 44 (29.7%) 24 (16.2%) 3 (2%) 0 (0%) | 0.515 |
Expectoration n (%)
| 112 (75.7%) 36 (24.3%) | 114 (77%) 34 (23%) | 0.891 0.872 |
Lung function (m ± SD)
| 80.4 (22.5) 73.7 ± 24.3 81.1 ± 17.3 | 78.4 (19) 72.8 ± 21.6 83.4 ± 19.6 | 0.785 0.610 0.713 |
Analytical parameters (m ± SD)
| 7070.4 ± 1722 55.8 ± 10.3 2.89 ± 2.2 0.35 ± 0.74 14.75 ± 12.5 4.17 ± 0.45 | 7139.8 ± 2043 56.4 ± 11.4 2.89 ± 3.07 0.44 ± 0.89 13.14 ± 12.6 4.2 ± 0.46 | 0.657 0.453 0.966 0.112 0.564 0.819 |
Treatment in stable phase (%)
| 47.3% 15% 58% 26% 52% 8.2% 1.4% 3.4% 0.7% 24.3% 21% 23% 2.7% | 45.3% 18% 57% 29% 53% 9.5% 2% 6.1% 2.7% 26.3% 22.3% 20.3% 4.7% | 0.699 0.546 0.901 0.739 0.934 0.645 0.766 0.332 0.211 0.867 0.876 0.624 0.423 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Vergara, A.; Girón Moreno, R.M.; Olveira, C.; Victoria Girón, M.; Peláez, A.; Ancochea, J.; Oscullo, G.; Martínez-García, M.Á. Impact of the SARS-CoV-2 Virus Pandemic on Patients with Bronchiectasis: A Multicenter Study. Antibiotics 2022, 11, 1096. https://doi.org/10.3390/antibiotics11081096
Martínez-Vergara A, Girón Moreno RM, Olveira C, Victoria Girón M, Peláez A, Ancochea J, Oscullo G, Martínez-García MÁ. Impact of the SARS-CoV-2 Virus Pandemic on Patients with Bronchiectasis: A Multicenter Study. Antibiotics. 2022; 11(8):1096. https://doi.org/10.3390/antibiotics11081096
Chicago/Turabian StyleMartínez-Vergara, Adrián, Rosa Mª Girón Moreno, Casilda Olveira, María Victoria Girón, Adrián Peláez, Julio Ancochea, Grace Oscullo, and Miguel Ángel Martínez-García. 2022. "Impact of the SARS-CoV-2 Virus Pandemic on Patients with Bronchiectasis: A Multicenter Study" Antibiotics 11, no. 8: 1096. https://doi.org/10.3390/antibiotics11081096
APA StyleMartínez-Vergara, A., Girón Moreno, R. M., Olveira, C., Victoria Girón, M., Peláez, A., Ancochea, J., Oscullo, G., & Martínez-García, M. Á. (2022). Impact of the SARS-CoV-2 Virus Pandemic on Patients with Bronchiectasis: A Multicenter Study. Antibiotics, 11(8), 1096. https://doi.org/10.3390/antibiotics11081096