
Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh

 ,
,  , , , , , , ,
, , , , , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Drug Sellers and Their Perspectives on Antibiotics Sales
2.2. Characteristics of the Customers Attending the Participating Pharmacies
2.3. Purchase of Antimicrobials including Antibiotics
2.4. Most Frequently Purchased Antibiotics
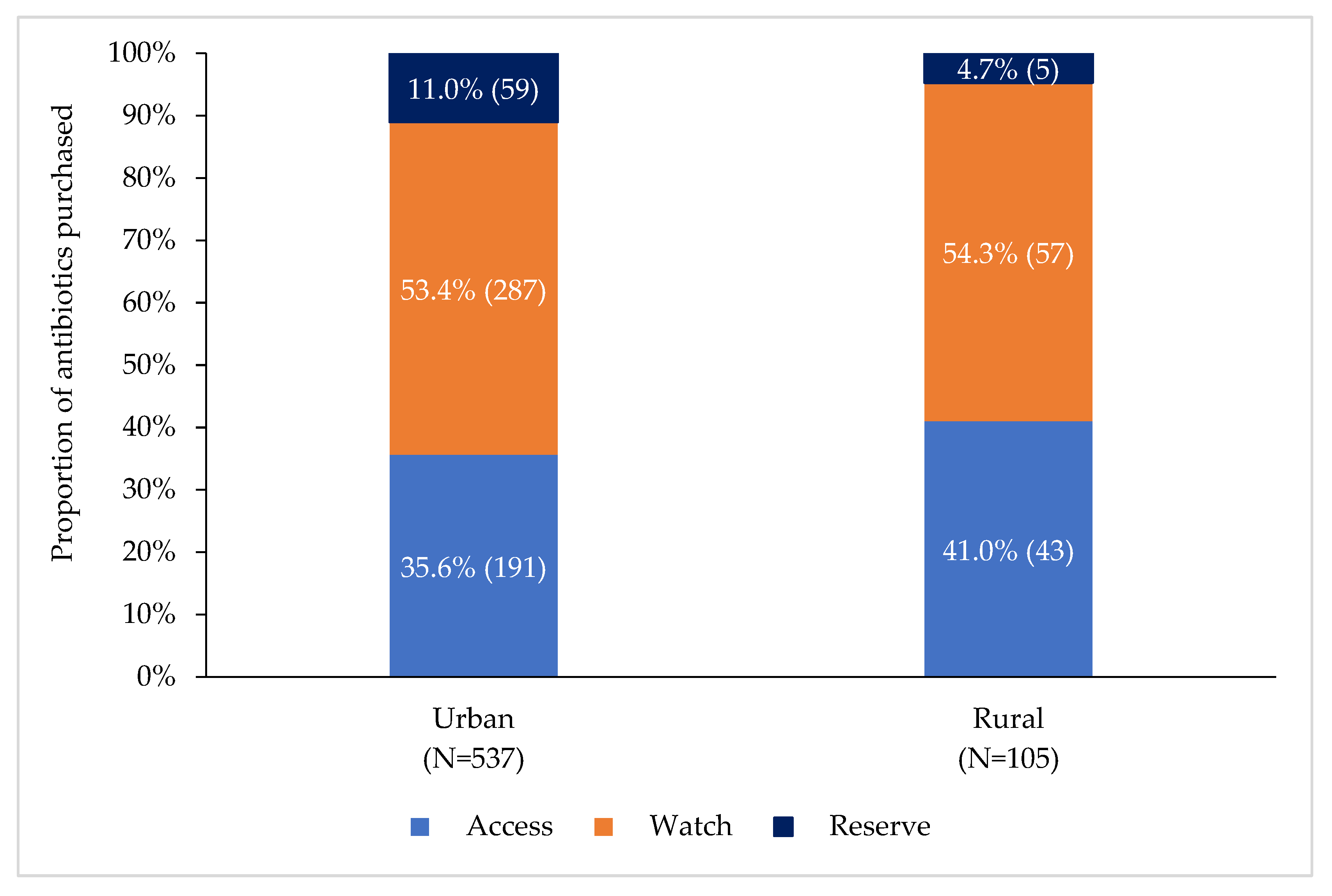
2.5. Antibiotics Purchased According to the WHO AWaRe Classification
3. Discussion
4. Materials and Methods
4.1. Study Sites and Study Population
4.2. Selection of Participants
4.2.1. Drug Seller
4.2.2. Customers
4.3. Data Collection
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Antimicrobial Resistance. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 16 October 2021).
- Mendelson, M.; Røttingen, J.-A.; Gopinathan, U.; Hamer, D.H.; Wertheim, H.; Basnyat, B.; Butler, C.; Tomson, G.; Balasegaram, M. Maximising access to achieve appropriate human antimicrobial use in low-income and middle-income countries. Lancet 2016, 387, 188–198. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 30 January 2021).
- Tula, M.; Iyoha, O.; Iruolaje, F. Antibiotic resistance: Challenges and prospect for therapy in developing countries. J. Pharm. Res. Int. 2015, 8, 1–16. [Google Scholar] [CrossRef]
- Ilić, K.; Jakovljević, E.; Škodrić-Trifunović, V. Social-economic factors and irrational antibiotic use as reasons for antibiotic resistance of bacteria causing common childhood infections in primary healthcare. Eur. J. Pediatr. 2012, 171, 767–777. [Google Scholar] [CrossRef]
- World Health Organization. New Report Calls for Urgent Action to Avert Antimicrobial Resistance Crisis. 2019. Available online: https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed on 17 October 2021).
- World Health Organization, No Time to Wait: Securing the Future from Drug-Resistant Infections. 2019. Available online: https://www.who.int/publications/i/item/no-time-to-wait-securing-the-future-from-drug-resistant-infections (accessed on 17 October 2021).
- World Health Organization, WHO Global Strategy for Containment of Antimicrobial Resistance. 2001. World Health Organization. Available online: https://www.who.int/drugresistance/WHO_Global_Strategy_English.pdf (accessed on 17 October 2021).
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2016. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 1 November 2020).
- Smith, F. The quality of private pharmacy services in low and middle-income countries: A systematic review. Pharm. World Sci. 2009, 31, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 18. [Google Scholar] [CrossRef]
- Kalungia, A.; Godman, B. Implications of non-prescription antibiotic sales in China. Lancet Infect. Dis. 2019, 19, 1272–1273. [Google Scholar] [CrossRef] [Green Version]
- Sakeena, M.; Bennett, A.A.; McLachlan, A.J. Non-prescription sales of antimicrobial agents at community pharmacies in developing countries: A systematic review. Int. J. Antimicrob. Agents 2018, 52, 771–782. [Google Scholar] [CrossRef]
- Auta, A.; Hadi, M.A.; Oga, E.; Adewuyi, E.O.; Abdu-Aguye, S.N.; Adeloye, D.; Strickland-Hodge, B.; Morgan, D.J. Global access to antibiotics without prescription in community pharmacies: A systematic review and meta-analysis. J. Infect. 2019, 78, 8–18. [Google Scholar] [CrossRef]
- World Health Organization, WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation. 2018. Available online: https://www.who.int/publications/i/item/who-report-on-surveillance-of-antibiotic-consumption (accessed on 20 October 2021).
- Samir, N.; Hassan, M.; Biswas, M.; Al Jubayer, A.; Chowdhury, F.; Akhtar, Z.; Lingam, R.; Banu, S.; Homaira, N. Antibiotic Use for Febrile Illness among Under-5 Children in Bangladesh: A Nationally Representative Sample Survey. Antibiotics 2021, 10, 1153. [Google Scholar] [CrossRef]
- Ministry of Health and Family Welfare, G.o.t.P.s.R.o.B. The National Drug Policy 2005. 2005. Available online: https://www.who.int/docs/default-source/searo/hsd/edm/nmp-ban-2005-goweb-ok.pdf?sfvrsn=101bc39d_2 (accessed on 20 October 2021).
- Ahmed, S.M.; Hossain, M.A.; Chowdhury, M.R. Informal sector providers in Bangladesh: How equipped are they to provide rational health care? Health Policy Plan. 2009, 24, 467–478. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization, WHO Releases the 2019 AWaRe Classification Antibiotics. 2019. Available online: https://www.who.int/news/item/01-10-2019-who-releases-the-2019-aware-classification-antibiotics (accessed on 20 October 2021).
- World Health Organization. WHO Access, Watch, Reserve (AWaRe) Classification of Antibiotics for Evaluation and Monitoring of Use. 2021. Available online: https://www.who.int/publications/i/item/2021-aware-classification (accessed on 24 December 2021).
- Ministry of Health and Family Welfare (MoHFW), G.o.B. National Action Plan: Antimicrobial Resistance Containment in Bangladesh 2017–2022. Available online: https://www.who.int/publications/m/item/bangladesh-antimicrobial-resistance-containment-in-bangladesh-2017-2022 (accessed on 20 November 2021).
- Orubu, E.S.F.; Zaman, M.H.; Rahman, M.T.; Wirtz, V.J. Veterinary antimicrobial resistance containment in Bangladesh: Evaluating the national action plan and scoping the evidence on implementation. J. Glob. Antimicrob. Resist. 2020, 21, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Hoque, R.; Ahmed, S.M.; Naher, N.; Islam, M.A.; Rousham, E.K.; Islam, B.Z.; Hassan, S. Tackling antimicrobial resistance in Bangladesh: A scoping review of policy and practice in human, animal and environment sectors. PLoS ONE 2020, 15, e0227947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paper, I.D. Antimicrobial Resistance: National Action Plans. 2018. Available online: https://www.who.int/antimicrobial-resistance/interagency-coordination-group/IACG_AMR_National_Action_Plans_110618.pdf (accessed on 22 November 2021).
- SIAPS, Baseline Study of Private Drug Shops in Bangladesh: Findings and Recommendations. 2015. Management Sciences for Health Arlington, VA, USA. Available online: https://siapsprogram.org/wp-content/uploads/2015/12/15-226-SIAPS-BD-Study_final-Revised-Report_10-Sept.-2015.-FINAL.pdf (accessed on 22 November 2021).
- Shill, M.C.; Das, A.K. Medication practices in Bangladesh-roles of pharmacists at current circumstances. Int. J. Pharm. Pharm. Sci. 2011, 3, 5–8. [Google Scholar]
- Biswas, M.; Roy, M.N.; Manik, M.I.; Hossain, M.S.; Tapu, S.M.; Moniruzzaman, M.; Sultana, S. Self medicated antibiotics in Bangladesh: A cross-sectional health survey conducted in the Rajshahi City. BMC Public Health 2014, 14, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Haque, M.U.; Kumar, A.; Barik, S.; Islam, M.A.U. Prevalence, practice and irrationality of self-medicated antibiotics among people in northern and southern region of Bangladesh. Int. J. Res. Pharm. Biosci. 2017, 4, 17–24. [Google Scholar]
- Sujan, M.A. ANTIBIOTICS USE, SALE: Who Needs PRESCRIPTION?, in The Daily Star. 2020. Available online: https://www.thedailystar.net/frontpage/antibiotics-use-and-sale-in-bangladesh-without-prescription-continues-1853359 (accessed on 22 December 2021).
- Orubu, E.S.F.; Samad, M.A.; Rahman, M.T.; Zaman, M.H.; Wirtz, V.J. Mapping the Antimicrobial Supply Chain in Bangladesh: A Scoping-Review-Based Ecological Assessment Approach. Glob. Health Sci. Pract. 2021, 9, 532–547. [Google Scholar] [CrossRef]
- Mah-E-Muneer, S.; Hassan, M.Z.; Biswas, M.A.A.J.; Rahman, F.; Akhtar, Z.; Das, P.; Islam, M.A.; Chowdhury, F. Use of Antimicrobials among Suspected COVID-19 Patients at Selected Hospitals, Bangladesh: Findings from the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 738. [Google Scholar] [CrossRef]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–2015: An analysis of pharmaceutical sales data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Bansal, A.; Sharma, R.; Prakash, R. Adoption of the World Health Organization access, watch reserve index to evaluate and monitor the use of antibiotics at a tertiary care hospital in India. Perspect. Clin. Res. 2021. [Google Scholar]
- Aljadeeah, S.; Wirtz, V.J.; Nagel, E. Outpatient antibiotic dispensing for the population with government health insurance in Syria in 2018–2019. Antibiotics 2020, 9, 570. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, Z.; Rashid, M.; Ahmed, M.; Islam, M.; Chowdhury, S.; Khan, Z.; Hassan, M.; Islam, K.; Parveen, S.; Debnath, N.; et al. Antibiotics Use and Its Knowledge in the Community: A Mobile Phone Survey during the COVID-19 Pandemic in Bangladesh. Antibiotics 2021, 10, 1052. [Google Scholar] [CrossRef] [PubMed]
- Nepal, A.; Hendrie, D.; Robinson, S.; Selvey, L.A. Survey of the pattern of antibiotic dispensing in private pharmacies in Nepal. BMJ Open 2019, 9, e032422. [Google Scholar] [CrossRef]
- World Health Organization and Access Watch Reserve (AWaRe). AWaRe Policy Brief. Available online: https://pubmed.ncbi.nlm.nih.gov/31601603/ (accessed on 11 November 2021).
- Chowdhury, P. An Overview of the Pharmaceutical Sector in Bangladesh. Dhaka: BRAC EPL Stock Brokerage LTD. 2010. Available online: https://studylib.net/doc/8899923/an-overview-of-the-pharmaceutical-sector-in-bangladesh (accessed on 21 October 2021).
- Das, P.; Martin, D.; Banu, S.; Rahman, M.; Chisti, M.; Friedman, M. Antibiotic use of patients having acute febrile illness prior to their hospital attendance in Bangladesh. Int. J. Infect. Dis. 2020, 101, 93. [Google Scholar] [CrossRef]
- Lucas, P.J.; Uddin, M.R.; Khisa, N.; Akter, S.S.; Unicomb, L.; Nahar, P.; Islam, M.A.; Nizame, F.A.; Rousham, E.K. Pathways to antibiotics in Bangladesh: A qualitative study investigating how and when households access medicine including antibiotics for humans or animals when they are ill. PLoS ONE 2019, 14, e0225270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biswas, M.; Roy, D.N.; Tajmim, A.; Rajib, S.S.; Hossain, M.; Farzana, F.; Yasmen, N. Prescription antibiotics for outpatients in Bangladesh: A cross-sectional health survey conducted in three cities. Ann. Clin. Microbiol. Antimicrob. 2014, 13, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cars, O.; Nordberg, P. Antibiotic resistance–The faceless threat. Int. J. Risk Saf. Med. 2005, 17, 103–110. [Google Scholar]
- Chuc, N.T.K.; Hoa, N.P.; Hoa, N.Q.; Nguyen, N.T.T.; Loan, H.T.; Toan, T.K.; Phuc, H.D.; Horby, P.; Van Yen, N.; Van Kinh, N.; et al. Antibiotic sales in rural and urban pharmacies in northern Vietnam: An observational study. BMC Pharmacol. Toxicol. 2014, 15, 1–10. [Google Scholar]
- Chang, J.; Ye, D.; Lv, B.; Jiang, M.; Zhu, S.; Yan, K.; Tian, Y.; Fang, Y. Sale of antibiotics without a prescription at community pharmacies in urban China: A multicentre cross-sectional survey. J. Antimicrob. Chemother. 2017, 72, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Shet, A.; Sundaresan, S.; Forsberg, B.C. Pharmacy-based dispensing of antimicrobial agents without prescription in India: Appropriateness and cost burden in the private sector. Antimicrob. Resist. Infect. Control 2015, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.; Xu, S.; Zhu, S.; Li, Z.; Yu, J.; Zhang, Y.; Zu, J.; Fang, Y.; Ross-Degnan, D. Assessment of non-prescription antibiotic dispensing at community pharmacies in China with simulated clients: A mixed cross-sectional and longitudinal study. Lancet Infect. Dis. 2019, 19, 1345–1354. [Google Scholar] [CrossRef]
- Do, N.T.; Vu, H.T.; Nguyen, C.T.; Punpuing, S.; Khan, W.A.; Gyapong, M.; Asante, K.P.; Munguambe, K.; Gómez-Olivé, F.X.; John-Langba, J.; et al. Community-based antibiotic access and use in six low-income and middle-income countries: A mixed-method approach. Lancet Glob. Health 2021, 9, e610–e619. [Google Scholar] [CrossRef]
- Batista, A.D.; ARodrigues, D.; Figueiras, A.; Zapata-Cachafeiro, M.; Roque, F.; Herdeiro, M.T. Antibiotic Dispensation without a Prescription Worldwide: A Systematic Review. Antibiotics 2020, 9, 786. [Google Scholar] [CrossRef]
- Darj, E.; Newaz, M.S.; Zaman, M.H. Pharmacists’ perception of their challenges at work, focusing on antimicrobial resistance: A qualitative study from Bangladesh. Glob. Health Action 2019, 12 (Suppl. 1), 1735126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matin, M.A.; Khan, W.A.; Karim, M.M.; Ahmed, S.; John-Langba, J.; Sankoh, O.A.; Gyapong, M.; Kinsman, J.; Wertheim, H. What influences antibiotic sales in rural Bangladesh? A drug dispensers’ perspective. J. Pharm. Policy Pract. 2020, 13, 1–12. [Google Scholar] [CrossRef]
- Chowdhury, F.; Sturm-Ramirez, K.; Al Mamun, A.; Iuliano, A.D.; Chisti, M.J.; Ahmed, M.; Bhuiyan, M.U.; Hossain, K.; Haider, M.S.; Aziz, S.A.; et al. Effectiveness of an educational intervention to improve antibiotic dispensing practices for acute respiratory illness among drug sellers in pharmacies, a pilot study in Bangladesh. BMC Health Serv. Res. 2018, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, F.; Sturm-Ramirez, K.; Mamun, A.A.; Iuliano, A.D.; Bhuiyan, M.U.; Chisti, M.J.; Ahmed, M.; Haider, S.; Rahman, M.; Azziz-Baumgartner, E. Factors driving customers to seek health care from pharmacies for acute respiratory illness and treatment recommendations from drug sellers in Dhaka city, Bangladesh. Patient Prefer. Adherence 2017, 11, 479. [Google Scholar] [CrossRef] [Green Version]
- Bergman, U.; Popa, C.; Tomson, Y.; Wettermark, B.; Einarson, T.R.; Aberg, H.; Sjoqvist, F. Drug utilization 90%—A simple method for assessing the quality of drug prescribing. Eur. J. Clin. Pharmacol. 1998, 54, 113–118. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Drug Sellers Characteristics | n = 128 |
|---|---|
| n(%) | |
| Age in years (mean ± SD *) | 36.8 ± 10 |
| Male | 128 (100.0) |
| Education level (years of schooling) | |
| 6–10 | 22 (17.2) |
| 11–12 | 45 (35.2) |
| 13–16 | 51 (39.8) |
| 16+ | 10 (7.8) |
| Pharmacy certificate registration course completed | 61 (47.7) |
| Working experience at pharmacy in years, median, (IQR **) | 10 (6-20) |
| Awareness of government policy on antibiotics sale | 116 (90.6) |
| Could correctly state government directives on antibiotics sale | 97 (75.8) |
| Pharmacy license shown by drug seller | 98 (76.6) |
| Customers’ Characteristics | n = 2686 n (%) |
| Median age in years, (IQR **) | 38 (29–50) |
| Male | 2118(78.9) |
| Female | 568 (21.1) |
| Education level (years of schooling) | |
| No formal education | 351 (13.1) |
| 1–5 | 540 (20.1) |
| 6–10 | 929 (34.9) |
| 11–12 | 386 (14.4) |
| 13–16 | 365 (13.6) |
| 16+ | 115 (4.3) |
| Medicine purchased for | |
| Customer himself/ herself | 1391 (51.8) |
| Family member | 1260 (46.9) |
| Others | 35 (1.3) |
| Medicine purchased with the advice from | |
| Physician | 883 (32.9) |
| Drug seller | 663 (24.7) |
| Own-decision/self-medication | 422 (15.7) |
| Others (family members, friends and traditional healers) | 718 (26.7) |
| Antibiotics purchased with the advice from (n = 580) | |
| Physician | 276 (47.6) |
| Drug seller | 172 (29.7) |
| Own-decision/self-medication | 22 (3.8) |
| Others (family members, friends and traditional healers) | 110 (19.0) |
| Antimicrobial Purchased | Customers | Purchased with Prescription | Purchased without Prescription | p-Value |
|---|---|---|---|---|
| n = 2686 | n = 883 | n = 1803 | ||
| n (%) | n (%) | n (%) | ||
| Antimicrobial | 679 (25.3) | 314 (35.6) | 365 (20.2) | <0.001 |
| Antibiotics* | 580 (21.6) | 276 (31.3) | 304 (16.9) | <0.001 |
| Number of antibiotics bought | ||||
| One antibiotic | 523 (90.2) | 241 (87.3) | 282 (92.8) | 0.066 |
| Two antibiotics | 52 (9.0) | 31 (11.2) | 21 (6.9) | |
| Three antibiotics | 5 (0.9) | 4 (1.4) | 1 (0.3) | |
| Antiparasitic | 91 (3.4) | 36 (4.1) | 55 (3.1) | 0.167 |
| Antifungal | 7 (0.3) | 2 (0.2) | 5 (0.3) | |
| Antiviral | 1 (0.04) | 0 (0) | 1 (0.1) | |
| Other than antimicrobial drugs bought | 2007 (74.7) | 569 (63.8) | 1,438 (79.8) | <0.001 |
| Number | Generic Name of Antibiotics | WHO AWaRE Classification | Antibiotics * | With Prescription | Without Prescription | p-Value |
|---|---|---|---|---|---|---|
| n = 642 | n = 315 | n = 327 | ||||
| n (%) | n (%) | n (%) | ||||
| Drug Utilization 90% (DU90%) 1–15 | 588 (91.6%) | 283 (89.8%) | 305 (93.3%) | |||
| 1 | Cefixime | Watch | 109 (18.8) | 61 (22.1) | 48 (15.8) | 0.052 |
| 2 | Azithromycin | Watch | 97 (16.7) | 40 (14.5) | 57 (18.8) | 0.17 |
| 3 | Metronidazole | Access | 82 (14.1) | 34 (12.3) | 48 (15.8) | 0.231 |
| 4 | Ciprofloxacin | Watch | 55 (9.5) | 27 (9.8) | 28 (9.2) | 0.814 |
| 5 | Cefuroxime | Watch | 48 (8.3) | 34 (12.3) | 14 (4.6) | 0.001 |
| 6 | Flucloxacillin | Access | 42 (7.2) | 19 (6.9) | 23 (7.6) | 0.752 |
| 7 | Amoxicillin | Access | 35 (5.5) | 6 (2.2) | 29 (9.5) | <0.001 |
| 8 | Linezolid | Reserve | 19 (3.3) | 6 (2.2) | 13 (4.3) | 0.155 |
| 9 | Polymyxin B | Reserve | 18 (3.1) | 12 (4.4) | 6 (1.8) | 0.1 |
| 10 | Cefradine | Access | 18 (3.1) | 6 (2.2) | 12 (3.7) | 0.219 |
| 11 | Levofloxacin | Watch | 15 (2.6) | 8 (2.9) | 7 (2.3) | 0.652 |
| 12 | Faropenem | Reserve | 15 (2.6) | 9 (3.3) | 6 (1.8) | 0.329 |
| 13 | Doxycycline | Access | 13 (2.2) | 5 (1.8) | 8 (2.6) | 0.505 |
| 14 | Amoxycillin + Clavulanic acid | Access | 12 (2.1) | 10 (3.6) | 2 (0.7) | 0.012 |
| 15 | Phenoxymethylpenicillin | Access | 10 (1.7) | 6 (2.2) | 4 (1.3) | 0.428 |
| Others 16–35 | 54 (8.40%) | 32 (10.20%) | 22 (6.70%) | |||
| 16 | Chloramphenicol | Access | 8 (1.4) | 3 (1.1) | 5 (1.6) | 0.565 |
| 17 | Colistin | Reserve | 8 (1.4) | 5 (1.8) | 3 (0.9) | 0.395 |
| 18 | Gentamicin | Access | 6 (0.9) | 3 (1.1) | 3 (0.9) | 0.905 |
| 19 | Ceftriaxone | Watch | 4 (0.7) | 3 (1.1) | 1 (0.3) | 0.271 |
| 20 | Tedizolid | Reserve | 4 (0.7) | 4 (1.5) | 0 (0) | 0.035 |
| 21 | Sulfamethoxazole + Trimethoprim | Access | 3 (0.5) | 0 (0) | 3 (0.9) | 0.098 |
| 22 | Cefaclor | Watch | 3 (0.5) | 2 (0.7) | 1 (0.3) | 0.507 |
| 23 | Clarithromycin | Watch | 3 (0.5) | 2 (0.7) | 1 (0.3) | 0.507 |
| 24 | Tetracycline | Access | 2 (0.3) | 0 (0) | 2 (0.7) | 0.177 |
| 25 | Erythromycin | Watch | 2 (0.3) | 1 (0.4) | 1 (0.3) | 0.945 |
| 26 | Meropenem | Watch | 2 (0.3) | 0 (0) | 2 (0.7) | 0.177 |
| 27 | Cefalexin | Access | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 28 | Chloramphenicol + Dexamethasone phosphate | Access | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 29 | Clindamycin | Access | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 30 | Cefotaxime | Watch | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 31 | Cefpodoxime | Watch | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 32 | Cefpodoxime Proxetil | Watch | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 33 | Ceftazidime | Watch | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 34 | Neomycin sulfate | Watch | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| 35 | Streptomycin | Watch | 1 (0.2) | 1 (0.4) | 0 (0) | 0.294 |
| Total | 642 (100%) | 315 (100%) | 327 (100%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.A.; Akhtar, Z.; Hassan, M.Z.; Chowdhury, S.; Rashid, M.M.; Aleem, M.A.; Ghosh, P.K.; Mah-E-Muneer, S.; Parveen, S.; Ahmmed, M.K.; et al. Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh. Antibiotics 2022, 11, 247. https://doi.org/10.3390/antibiotics11020247
Islam MA, Akhtar Z, Hassan MZ, Chowdhury S, Rashid MM, Aleem MA, Ghosh PK, Mah-E-Muneer S, Parveen S, Ahmmed MK, et al. Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh. Antibiotics. 2022; 11(2):247. https://doi.org/10.3390/antibiotics11020247
Chicago/Turabian StyleIslam, Md. Ariful, Zubair Akhtar, Md. Zakiul Hassan, Sukanta Chowdhury, Md. Mahbubur Rashid, Mohammad Abdul Aleem, Probir Kumar Ghosh, Syeda Mah-E-Muneer, Shahana Parveen, Md. Kaousar Ahmmed, and et al. 2022. "Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh" Antibiotics 11, no. 2: 247. https://doi.org/10.3390/antibiotics11020247
APA StyleIslam, M. A., Akhtar, Z., Hassan, M. Z., Chowdhury, S., Rashid, M. M., Aleem, M. A., Ghosh, P. K., Mah-E-Muneer, S., Parveen, S., Ahmmed, M. K., Ahmed, M. S., Basher, A. K., Palit, A., Biswas, M. A. A. J., Khan, Z., Islam, K., Debnath, N., Rahman, M., & Chowdhury, F. (2022). Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh. Antibiotics, 11(2), 247. https://doi.org/10.3390/antibiotics11020247