
Resident-Related Factors Influencing Antibiotic Treatment Decisions for Urinary Tract Infections in Dutch Nursing Homes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Outcome Measures
2.3. In- and Exclusion Criteria
2.4. Handling Missing Data
2.5. Data Analysis
3. Results
3.1. Baseline Characteristics
3.1.1. Nursing Home Residents
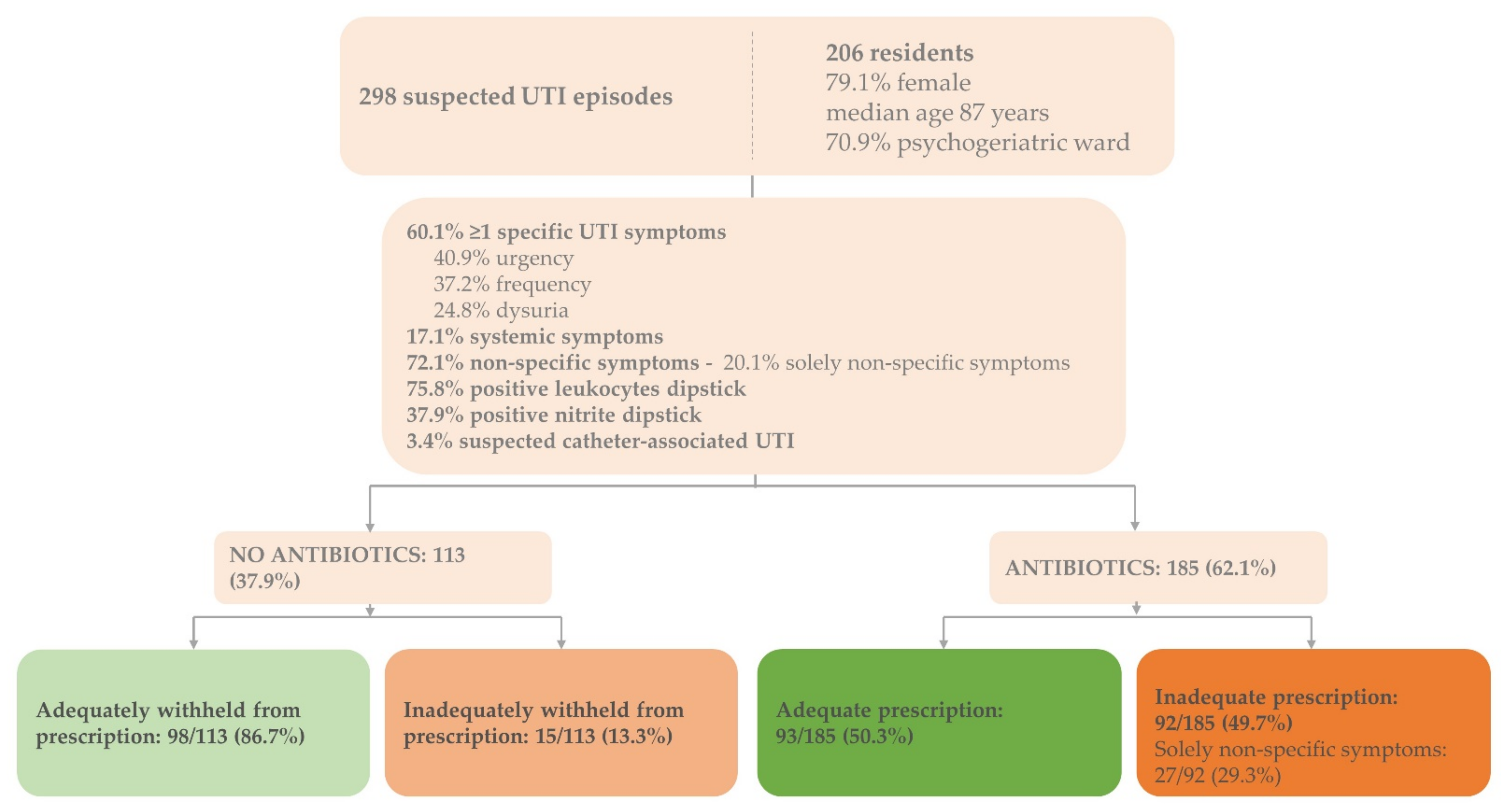
3.1.2. Suspected UTI Episodes
3.1.3. Uropathogens
3.2. Characteristics of Treated versus Untreated Suspected UTI Episodes
3.2.1. Signs and Symptoms
3.2.2. Urine Dipstick Results
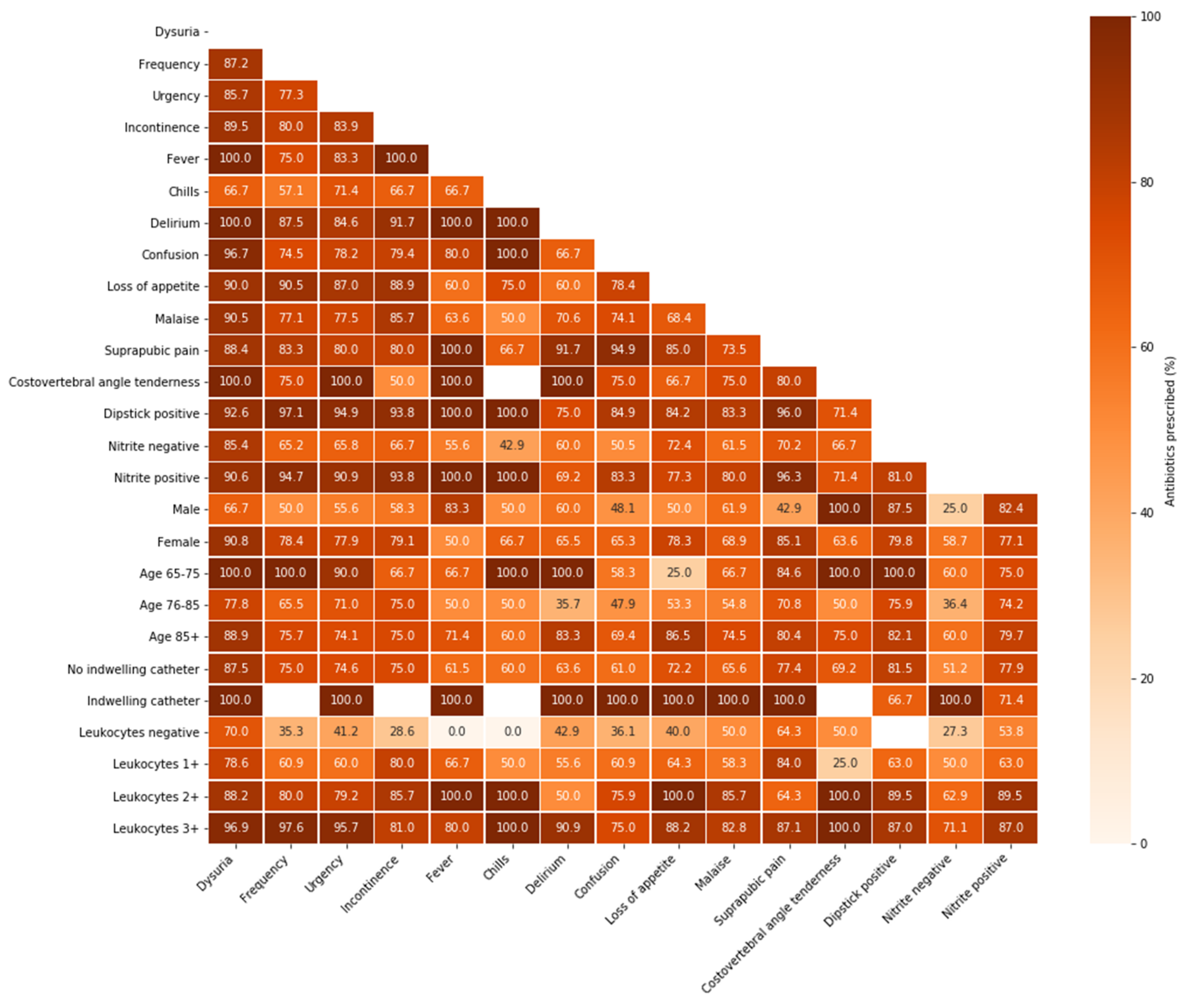
3.3. Prescription Proportions in Resident-Related Factor Combinations
3.4. Adequate Treatment Decisions
3.4.1. Adequate Antibiotic Agents
3.4.2. Adequate Antibiotic Agents Based on Susceptibility Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pulia, M.; Kern, M.; Schwei, R.J.; Shah, M.N.; Sampene, E.; Crnich, C.J. Comparing appropriateness of antibiotics for nursing home residents by setting of prescription initiation: A cross-sectional analysis. Antimicrob. Resist. Infect. Control 2018, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, H.; Iversen, B.; Aavitsland, P. Prevalence of nosocomial infections in hospitals in Norway, 2002 and 2003. J. Hosp. Infect. 2005, 60, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Engelhart, S.; Hanses-Derendorf, L.; Exner, M.; Kramer, M. Prospective surveillance for healthcare-associated infections in German nursing home residents. J. Hosp. Infect. 2005, 60, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Van Buul, L.W.; van der Steen, J.; Veenhuizen, R.; Achterberg, W.; Schellevis, F.G.; Essink, R.T.; van Benthem, B.H.; Natsch, S.; Hertogh, C.M. Antibiotic Use and Resistance in Long Term Care Facilities. J. Am. Med Dir. Assoc. 2012, 13, 568.e1–568.e13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Buul, L.W.; Veenhuizen, R.B.; Achterberg, W.P.; Schellevis, F.G.; Essink, R.T.G.M.; de Greeff, S.C.; Natsch, S.; van der Steen, J.T.; Hertogh, C.M.P.M. Antibiotic Prescribing in Dutch Nursing Homes: How Appropriate Is It? J. Am. Med. Dir. Assoc. 2015, 16, 229–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemoine, L.; Dupont, C.; Capron, A.; Cerf, E.; Yilmaz, M.; Verloop, D.; Blanckaert, K.; Senneville, E.; Alfandari, S. Prospective evaluation of the management of urinary tract infections in 134 French nursing homes. Med. Mal. Infect. 2018, 48, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Daneman, N.; Bronskill, S.E.; Gruneir, A.; Newman, A.M.; Fischer, H.D.; Rochon, P.A.; Anderson, G.M.; Bell, C.M. Variability in Antibiotic Use Across Nursing Homes and the Risk of Antibiotic-Related Adverse Outcomes for Individual Residents. JAMA Intern. Med. 2015, 175, 1331–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voicu, M.; Popescu, F.; Florescu, D.; Rogoveanu, I.; Turcu-Stiolica, A.; Gheonea, D.; Iovanescu, V.; Iordache, S.; Cazacu, S.; Ungureanu, B. Clostridioides difficile Infection among Cirrhotic Patients with Variceal Bleeding. Antibiotics 2021, 10, 731. [Google Scholar] [CrossRef]
- Van der Donk, C.; Schols, J.; Driessen, C.; Hagenouw, R.; Meulendijks, A.; Stobberingh, E. Prevalence and Spread of Multidrug Resistant Escherichia coli Isolates Among Nursing Home Residents in the Southern Part of The Netherlands. J. Am. Med. Dir. Assoc. 2013, 14, 199–203. [Google Scholar] [CrossRef]
- Nicolle, L.E.; Gupta, K.; Bradley, S.F.; Colgan, R.; DeMuri, G.P.; Drekonja, D.; Eckert, O.L.; Geerlings, E.S.; Köves, B.; Hooton, T.M.; et al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2019, 68, 1611–1615. [Google Scholar] [CrossRef]
- Nicolle, L.E. Urinary Tract Infections in the Older Adult. Clin. Geriatr. Med. 2016, 32, 523–538. [Google Scholar] [CrossRef]
- Agata, E.D.; Loeb, M.B.; Mitchell, S.L. Challenges in Assessing Nursing Home Residents with Advanced Dementia for Suspected Urinary Tract Infections. J. Am. Geriatr. Soc. 2013, 61, 62–66. [Google Scholar] [CrossRef]
- Nicolle, L.E.; Yoshikawa, T.T. Urinary Tract Infection in Long-Term-Care Facility Residents. Clin. Infect. Dis. 2000, 31, 757–761. [Google Scholar] [CrossRef]
- Nace, D.A.; Perera, S.K.; Hanlon, J.T.; Saracco, S.; Anderson, G.; Schweon, S.J.; Klein-Fedyshin, M.; Wessel, C.B.; Mulligan, M.; Drinka, P.J.; et al. The Improving Outcomes of UTI Management in Long-Term Care Project (IOU) Consensus Guidelines for the Diagnosis of Uncomplicated Cystitis in Nursing Home Residents. J. Am. Med. Dir. Assoc. 2018, 19, 765–769.e3. [Google Scholar] [CrossRef]
- Van Buul, L.W.; Vreeken, H.L.; Bradley, S.F.; Crnich, C.J.; Drinka, P.J.; Geerlings, S.E.; Jump, R.L.; Mody, L.; Mylotte, J.J.; Loeb, M.; et al. The Development of a Decision Tool for the Empiric Treatment of Suspected Urinary Tract Infection in Frail Older Adults: A Delphi Consensus Procedure. J. Am. Med. Dir. Assoc. 2018, 19, 757–764. [Google Scholar] [CrossRef]
- Sommer-Larsen, S.; Arnold, S.; Holm, A.; Olesen, J.A.; Cordoba, G. Quality of the Diagnostic Process, Treatment Decision, and Predictors for Antibiotic Use in General Practice for Nursing Home Residents with Suspected Urinary Tract Infection. Antibiotics 2021, 10, 316. [Google Scholar] [CrossRef]
- Richtlijn Urineweginfecties Bij Kwetsbare Ouderen, Dutch National Guideline Urinary Tract Infection in Frail Older Adults: Verenso. 2018. Available online: https://www.verenso.nl/richtlijnen-en-praktijkvoering/richtlijnendatabase/urineweginfecties (accessed on 7 July 2021).
- Loeb, M.; Bentley, D.W.; Bradley, S.; Crossley, K.; Garibaldi, R.; Gantz, N.; McGeer, A.; Muder, R.R.; Mylotte, J.; Nicolle, L.E.; et al. Development of Minimum Criteria for the Initiation of Antibiotics in Residents of Long-Term–Care Facilities: Results of a Consensus Conference. Infect. Control Hosp. Epidemiol. 2001, 22, 120–124. [Google Scholar] [CrossRef]
- Rutten, J.J.S.; Van Buul, L.W.; Smalbrugge, M.; Geerlings, S.E.; Gerritsen, D.L.; Natsch, S.; Sloane, P.D.; Veenhuizen, R.B.; Van Der Wouden, J.C.; Hertogh, C.M.P.M. Antibiotic prescribing and non-prescribing in nursing home residents with signs and symptoms ascribed to urinary tract infection (ANNA): Study protocol for a cluster randomized controlled trial. BMC Geriatr. 2020, 20, 341. [Google Scholar] [CrossRef]
- Kistler, C.E.; Beeber, A.S.; Zimmerman, S.; Ward, K.; Farel, C.; Chrzan, K.; Wretman, C.J.; Boynton, M.H.; Pignone, M.; Sloane, P.D. Nursing Home Clinicians’ Decision to Prescribe Antibiotics for a Suspected Urinary Tract Infection: Findings From a Discrete Choice Experiment. J. Am. Med. Dir. Assoc. 2020, 21, 675–682.e1. [Google Scholar] [CrossRef] [Green Version]
- Van Buul, L.W.; van der Steen, J.T.; Doncker, S.M.; Achterberg, W.P.; Schellevis, F.G.; Veenhuizen, R.B.; Hertogh, C.M. Factors influencing antibiotic prescribing in long-term care facilities: A qualitative in-depth study. BMC Geriatr. 2014, 14, 136. [Google Scholar] [CrossRef] [Green Version]
- Kuil, S.D.; Hidad, S.; Fischer, J.C.; Harting, J.; Hertogh, C.M.; Prins, J.M.; van Leth, F.; de Jong, M.D.; Schneeberger, C. Sensitivity of point-of-care testing C reactive protein and procalcitonin to diagnose urinary tract infections in Dutch nursing homes: PROGRESS study protocol. BMJ Open 2019, 9, e031269. [Google Scholar] [CrossRef] [Green Version]
- Richtlijn Urineweginfecties, Dutch Guideline Urinary Tract Infections: Nederlandse Vereniging van Verpleeghuisartsen (NVVA), Verenso. 2006. Available online: https://www.verenso.nl/_asset/_public/Richtlijnen_kwaliteit/richtlijnen/database/Richtlijn-UWI-06-def.pdf (accessed on 7 July 2021).
- Kistler, C.E.; Zimmerman, S.; Scales, K.; Ward, K.; Weber, D.; Reed, D.; McClester, M.; Sloane, P.D. The Antibiotic Prescribing Pathway for Presumed Urinary Tract Infections in Nursing Home Residents. J. Am. Geriatr. Soc. 2017, 65, 1719–1725. [Google Scholar] [CrossRef]
- Phillips, C.D.; Adepoju, O.; Stone, N.; Moudouni, D.K.M.; Nwaiwu, O.; Zhao, H.; Frentzel, E.; Mehr, D.; Garfinkel, S. Asymptomatic bacteriuria, antibiotic use, and suspected urinary tract infections in four nursing homes. BMC Geriatr. 2012, 12, 73. [Google Scholar] [CrossRef] [Green Version]
- Pinder, R.J.; Berry, D.; Sallis, A.; Chadborn, T. Antibiotic Prescribing and Behaviour Change in Healthcare Settings: Literature Review and Behavioural Analysis; Department of Health & Public Health England: London, UK, 2015. [Google Scholar]
- Naughton, B.J.; Mylotte, J.M.; Ramadan, F.; Karuza, J.; Priore, R.L. Antibiotic Use, Hospital Admissions, and Mortality Before and After Implementing Guidelines for Nursing Home-acquired Pneumonia. J. Am. Geriatr. Soc. 2001, 49, 1020–1024. [Google Scholar] [CrossRef]
- Beeber, A.S.; Kistler, C.E.; Zimmerman, S.; Dictus, C.; Ward, K.; Farel, C.; Chrzan, K.; Wretman, C.J.; Boyton-Hansen, M.; Pignone, M.; et al. Nurse Decision-making for Suspected Urinary Tract Infections in Nursing Homes: Potential Targets to Reduce Antibiotic Overuse. J. Am. Med. Dir. Assoc. 2021, 22, 156–163. [Google Scholar] [CrossRef]
- Latour, K.; De Lepeleire, J.; Jans, B.; Buntinx, F.; Catry, B. Diagnosis, prevention and control of urinary tract infections: A survey of routine practices in Belgian nursing homes. J. Infect. Prev. 2020, 21, 182–188. [Google Scholar] [CrossRef]
- Salem-Schatz, S.; Griswold, P.; Kandel, R.; Benjamin-Bothwell, S.; DeMaria, A., Jr.; McElroy, N.; Bolstorf, B.; McHale, E.; Doron, S. A Statewide Program to Improve Management of Suspected Urinary Tract Infection in Long-Term Care. J. Am. Geriatr. Soc. 2019, 68, 62–69. [Google Scholar] [CrossRef]
- Valmadrid, L.C.; Schwei, R.J.; Maginot, E.; Pulia, M.S. The impact of health care provider relationships and communication dynamics on urinary tract infection management and antibiotic utilization for long-term care facility residents treated in the emergency department: A qualitative study. Am. J. Infect. Control. 2020, 49, 198–205. [Google Scholar] [CrossRef]
- Arnold, S.H.; Jensen, J.N.; Kousgaard, M.B.; Siersma, V.; Bjerrum, L.; Holm, A. Reducing Antibiotic Prescriptions for Urinary Tract Infection in Nursing Homes Using a Complex Tailored Intervention Targeting Nursing Home Staff: Protocol for a Cluster Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e17710. [Google Scholar] [CrossRef]
- Brown, K.A.; Daneman, N.; Schwartz, K.L.; Langford, B.; McGeer, A.; Quirk, J.; Diong, C.; Garber, G. The Urine-culturing Cascade: Variation in Nursing Home Urine Culturing and Association with Antibiotic Use and Clostridiodes difficile Infection. Clin. Infect. Dis. 2019, 70, 1620–1627. [Google Scholar] [CrossRef]
- Juthani-Mehta, M.; Tinetti, M.; Perrelli, E.; Towle, V.; Quagliarello, V. Role of Dipstick Testing in the Evaluation of Urinary Tract Infection in Nursing Home Residents. Infect. Control. Hosp. Epidemiol. 2007, 28, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Kuil, S.D.; Hidad, S.; Fischer, J.C.; Harting, J.; Hertogh, C.M.P.M.; Prins, J.M.; De Jong, M.D.; Van Leth, F.; Schneeberger, C. Sensitivity of C-Reactive Protein and Procalcitonin Measured by Point-of-Care Tests to Diagnose Urinary Tract Infections in Nursing Home Residents: A Cross-Sectional Study. Clin. Infect. Dis. 2020, 73, e3867–e3875. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.O.G.; Varillas, S.F.I.; Pastor, H.J.B.; Mitma, Y.L.; Canales, D.H.; Chero, P.A.W.; Gutierrez, C.; Cunza, S.S. Immunological and biochemical response of older adults with urinary tract infection to uropathogenic Esherichia coli virulence factors. Rev. Peru. De Med. Exp. Y Salud Pública 2020, 37, 527–531. [Google Scholar] [CrossRef]
- Haasum, Y.; Fastbom, J.; Johnell, K. Different patterns in use of antibiotics for lower urinary tract infection in institutionalized and home-dwelling elderly: A register-based study. Eur. J. Clin. Pharmacol. 2012, 69, 665–671. [Google Scholar] [CrossRef] [PubMed]
- NHG-Standaard Urineweginfecties, Dutch College of General Practitioners Guideline Urinary Tract Infections: Nederlands Huisartsen Genootschap (NHG). 2020. Available online: https://richtlijnen.nhg.org/standaarden/urineweginfecties (accessed on 7 July 2021).
- Nitrofurantoin: Rationale for the EUCAST Clinical Breakpoints, Version 1; European Committee on Antimicrobial Susceptibility Testing (EUCAST). 2010. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Rationale_documents/Nitrofurantoin_rationale_1.0.pdf (accessed on 26 December 2021).
- Das, R.; Perrelli, E.; Towle, V.; Van Ness, P.H.; Juthani-Mehta, M. Antimicrobial Susceptibility of Bacteria Isolated from Urine Samples Obtained from Nursing Home Residents. Infect. Control. Hosp. Epidemiol. 2009, 30, 1116–1119. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Resident-Related Factor | Antibiotic Prescription (n = 185) | RR [95% CI] | |
|---|---|---|---|
| Gender | Female vs. Male | 65.4% (n = 161)/46.2% (n = 24) | 1.4 [1.04–1.93] |
| Indwelling catheter | Yes vs. No | 80.0% (n = 8)/61.3% (n = 174) | 1.3 [0.95–1.80] |
| Specific UTI symptoms | Dysuria Yes vs. No Urgency Yes vs. No Frequency Yes vs. No Urinary incontinence Yes vs. No Urethral discharge Yes vs. No | 87.8% (n = 65)/49.5% (n = 93) 74.6% (n = 91)/49.3% (n = 71) 74.8% (n = 83)/50.0% (n = 78) 74.5% (n = 41)/57.7% (n = 127) 42.9% (n = 3)/61.9% (n = 159) | 1.8 [1.50–2.10] 1.5 [1.24–1.84] 1.5 [1.24–1.81] 1.3 [1.07–1.56] 0.7 [0.29–1.64] |
| Systemic symptoms | Fever Yes vs. No Chills Yes vs. No Delirium Yes vs. No | 64.3% (n = 9)/60.7% (n = 164) 60.0% (n = 6)/61.7% (n = 174) 64.7% (n = 22)/61.8% (n = 144) | 1.1 [0.71–1.58] 1.0 [0.58–1.63] 1.0 [0.80–1.37] |
| Additional symptoms | Costovertebral angle tenderness Yes vs. No Suprapubic pain Yes vs. No | 69.2% (n = 9)/61.7% (n = 153) 78.4% (n = 69)/51.1% (n = 94) | 1.1 [0.77–1.63] 1.5 [1.28–1.84] |
| Non-specific symptoms | Confusion vs. No confusion Loss of appetite Yes vs. No Malaise Yes vs. No | 62.6% (n = 107)/62.4% (n = 73) 73.2% (n = 41)/57.5% (n = 130) 67.4% (n = 64) 58.2% (n = 110) | 1.0 [0.84–1.20] 1.3 [1.05–1.55] 1.2 [0.96–1.39] |
| Solely non-specific symptoms | 45.0% (n = 27) | ||
| Leukocytes | Positive * vs. Negative | 69.9% (n = 158)/33.3% (n = 19) | 2.1 [1.44–3.06] |
Positive * leukocytes
| 54.8% (n = 40) 72.2% (n = 39) 79.8% (n = 79) | ||
| Nitrite | Positive vs. Negative | 77.9% (n = 88)/52.4% (n = 89) | 1.5 [1.25–1.77] |
| Nitrite & leukocytes | Positive | 81.0% (n = 81) | 1.5 [1.31–1.83] |
| Nitrite & leukocytes | Negative | 27.3% (n = 12) | 0.4 [0.24–0.65] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolodziej, L.M.; Kuil, S.D.; de Jong, M.D.; Schneeberger, C. Resident-Related Factors Influencing Antibiotic Treatment Decisions for Urinary Tract Infections in Dutch Nursing Homes. Antibiotics 2022, 11, 140. https://doi.org/10.3390/antibiotics11020140
Kolodziej LM, Kuil SD, de Jong MD, Schneeberger C. Resident-Related Factors Influencing Antibiotic Treatment Decisions for Urinary Tract Infections in Dutch Nursing Homes. Antibiotics. 2022; 11(2):140. https://doi.org/10.3390/antibiotics11020140
Chicago/Turabian StyleKolodziej, Lisa Marie, Sacha Daniëlle Kuil, Menno Douwe de Jong, and Caroline Schneeberger. 2022. "Resident-Related Factors Influencing Antibiotic Treatment Decisions for Urinary Tract Infections in Dutch Nursing Homes" Antibiotics 11, no. 2: 140. https://doi.org/10.3390/antibiotics11020140
APA StyleKolodziej, L. M., Kuil, S. D., de Jong, M. D., & Schneeberger, C. (2022). Resident-Related Factors Influencing Antibiotic Treatment Decisions for Urinary Tract Infections in Dutch Nursing Homes. Antibiotics, 11(2), 140. https://doi.org/10.3390/antibiotics11020140