
Prognostic Value of Procalcitonin and C-Reactive Protein in 1608 Critically Ill Patients with Severe Influenza Pneumonia

 ,
,  , , , , , , , and
, , , , , , , and 
Abstract
1. Introduction
2. Results
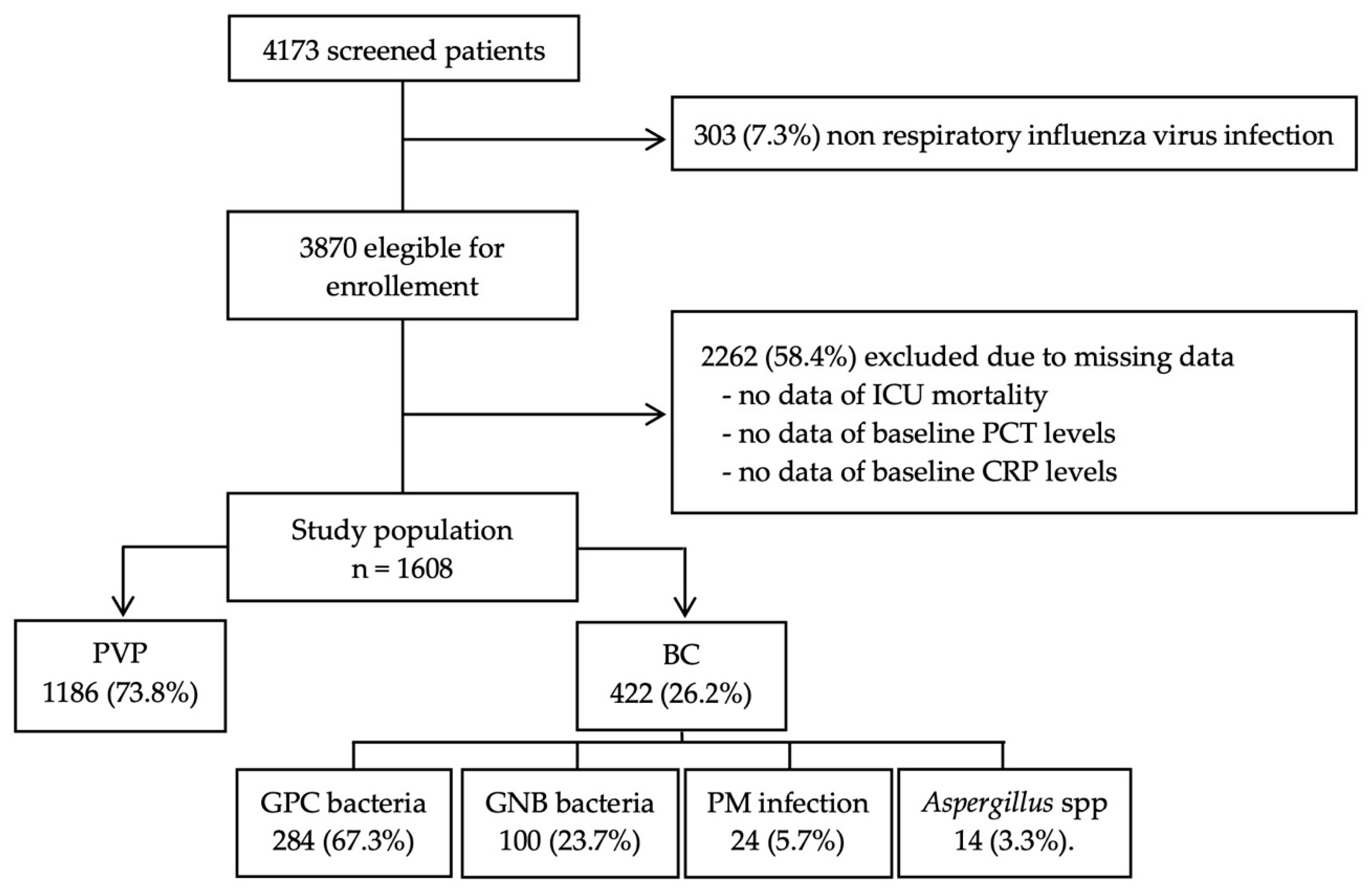
2.1. Comparison Between Patients with and Without Bacterial Co-Infection
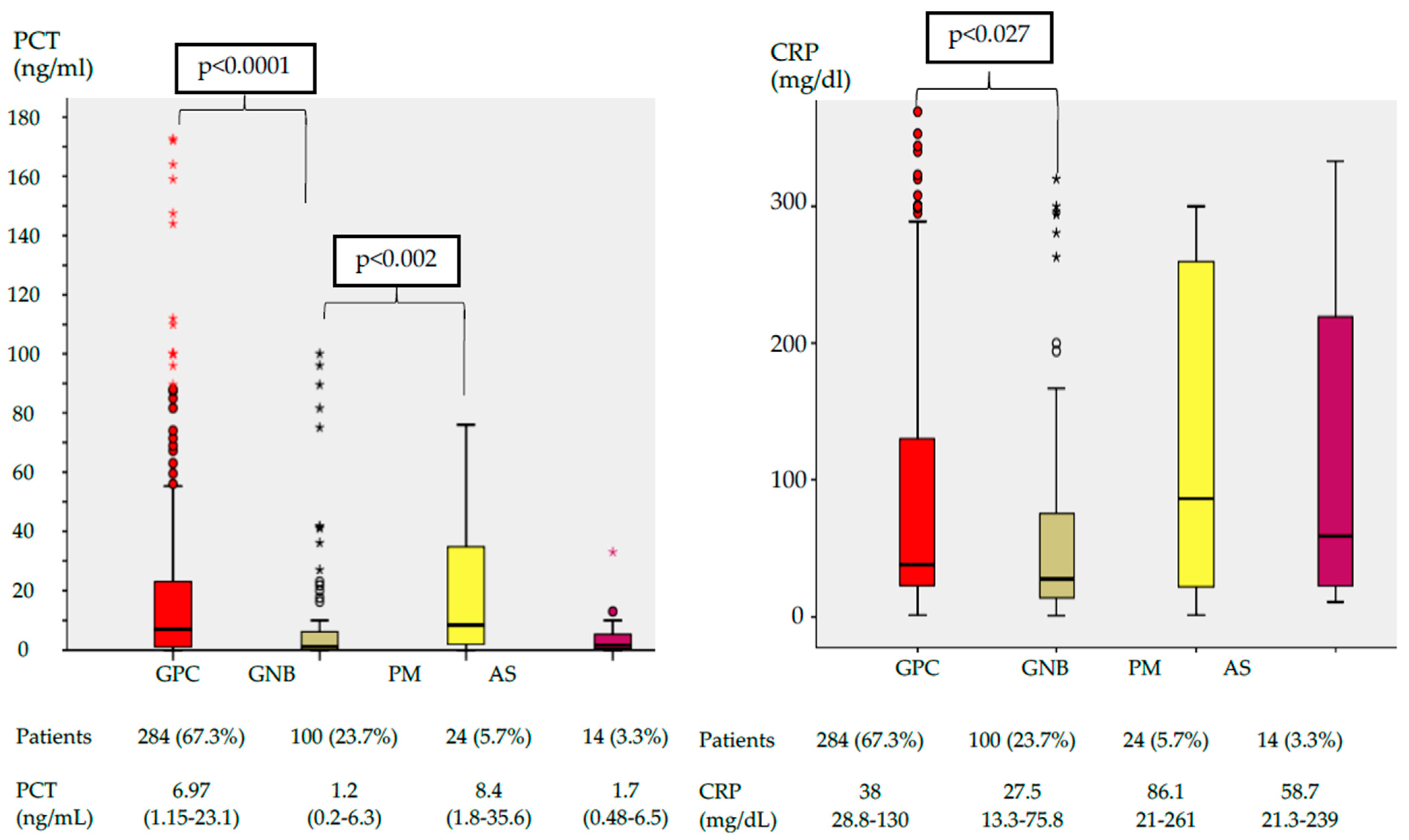
2.2. Performance of PCT or CRP as Predictors of the Microorganism Responsible of Bacterial Co-Infection
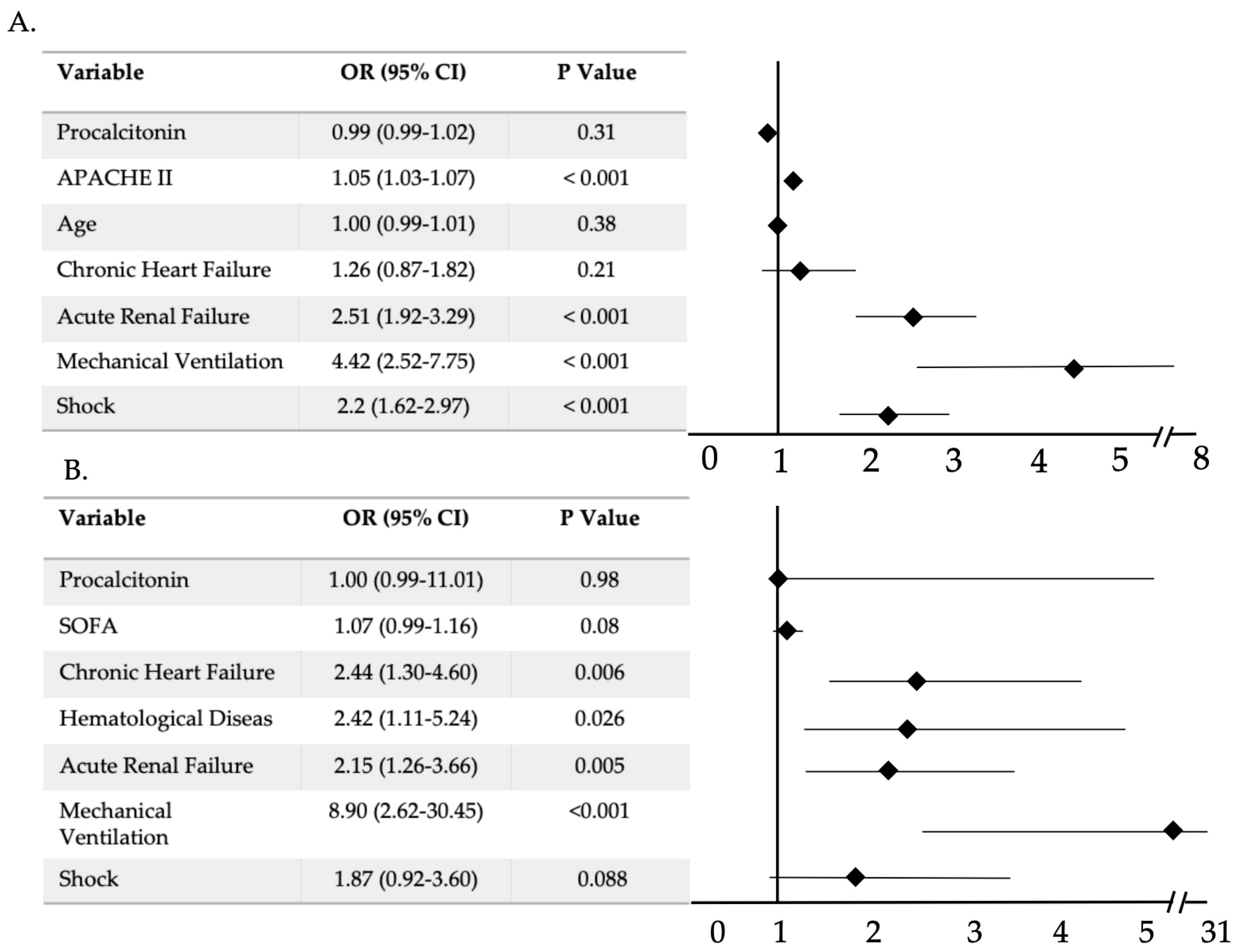
2.3. Mortality Analysis
3. Materials and Methods
3.1. Study Design
3.2. Data Collection and Laboratory Diagnostics
3.3. Study Definitions
3.4. Endpoints
3.5. Statistical Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vincent, J.-L.; Rello, J.; Marshall, J.K.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International Study of the Prevalence and Outcomes of Infection in Intensive Care Units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef]
- Phua, J.; Ngerng, W.J.; See, K.C.; Tay, C.K.; Kiong, T.; Lim, H.F.; Chew, M.Y.; Yip, H.S.; Tan, A.; Khalizah, H.J.; et al. Characteristics and outcomes of culture-negative versus culture-positive severe sepsis. Crit. Care 2013, 17, R202. [Google Scholar] [CrossRef]
- Schuetz, P.; Christ-Crain, M.; Müller, B. Biomarkers to improve diagnostic and prognostic accuracy in systemic infections. Curr. Opin. Crit. Care 2007, 13, 578–585. [Google Scholar] [CrossRef]
- Cho, S.Y.; Choi, J.H. Biomarkers of Sepsis. Infect. Chemother. 2014, 46, 1–12. [Google Scholar] [CrossRef]
- Müller, B.; Harbarth, S.; Stolz, D.; Bingisser, R.; Mueller, C.; Leuppi, J.; Nusbaumer, C.; Tamm, M.; Christ-Crain, M. Diagnostic and prognostic accuracy of clinical and laboratory parameters in community-acquired pneumonia. BMC Infect. Dis. 2007, 7, 10. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Müller, B. Biomarkers in respiratory tract infections: Diagnostic guides to antibiotic prescription, prognostic markers and mediators. Eur. Respir. J. 2007, 30, 556–573. [Google Scholar] [CrossRef]
- Bréchot, N.; Hékimian, G.; Chastre, J.; Luyt, C.-E. Procalcitonin to guide antibiotic therapy in the ICU. Int. J. Antimicrob. Agents 2015, 46, S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Bouadma, L.; Luyt, C.E.; Tubasch, F.; Cracco, C.; Alvarez, A.; Schwebel, C.; Schortgen, F.; Lasocki, S.; Veber, B.; Dehoux, M.; et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): A multicentre randomised controlled trial. Lancet 2010, 375, 463–474. [Google Scholar] [CrossRef]
- Schuetz, P.; Birkhahn, R.; Sherwin, R.; Jones, A.E.; Singer, A.; Kline, J.A.; Runyon, M.S.; Self, W.H.; Courtney, D.M.; Nowak, R.M.; et al. Serial Procalcitonin Predicts Mortality in Severe Sepsis Patients. Crit. Care Med. 2017, 45, 781–789. [Google Scholar] [CrossRef]
- Seligman, R.; Meisner, M.; Lisboa, T.C.; Hertz, F.T.; Filippin, T.B.; Fachel, J.M.G.; Teixeira, P.J.Z. Decreases in procalcitonin and C-reactive protein are strong predictors of survival in ventilator-associated pneumonia. Crit. Care 2006, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Rüddel, D.O.; Poidinger, B.; Kott, M.; Weiss, M.; Reinhart, K.; Bloos, F. Influence of pathogen and focus of infection on procalcitonin values in sepsis patients with bacteremia or candidemia. Crit. Care 2018, 22, 1–11. [Google Scholar] [CrossRef]
- Brodská, H.; Malíčková, K.; Adámková, V.; Benáková, H.; Šåastná, M.M.; Zima, T. Significantly higher procalcitonin levels could differentiate Gram-negative sepsis from Gram-positive and fungal sepsis. Clin. Exp. Med. 2013, 13, 165–170. [Google Scholar] [CrossRef]
- Rodríguez, A.; álvarez-Rocha, L.; Sirvent, J.M.; Zaragoza, R.; Nieto, M.; Arenzana, A.; Luque, P.; Socías, L.; Martín, M.; Navarro, D.; et al. Recomendaciones del Grupo de Trabajo Enfermedades Infecciosas (GTEI) de la Sociedad Española de Medicina Intensiva, Crítica y Unidades Coronarias (SEMICYUC) y el Grupo de Estudio de Infecciones en el Paciente Crítico (GEIPC) de la Sociedad Espanola de Enf. Med. Intensiva 2012, 36, 103–137. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.Z.J. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, R.; Torres, A.; Aspa, J.; Capelastegui, A.; Prat, C.; Rodríguez de Castro, F. Community-acquired pneumonia. New regulations of the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR). Arch. Bronconeumol. 2010, 46, 543–558. [Google Scholar] [CrossRef]
- Rodríguez, A.; Díaz, E.; Martín-Loeches, I.; Sandiumenge, A.; Canadell, L.; Díaz, J.J.; Figueira, J.C.; Marques, A.; Álvarez-Lerma, F.; Vallés, J.; et al. Impact of early oseltamivir treatment on outcome in critically ill patients with 2009 pandemic influenza A. J. Antimicrob. Chemother. 2011, 66, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Martín-Loeches, I.; Sanchez-Corral, A.; Diaz, E.; Granada, R.M.; Zaragoza, R.; Villavicencio, C.; Albaya, A.; Cerdá, E.; Catalán, R.M.; Luque, P.; et al. Community-acquired respiratory coinfection in critically III patients with pandemic 2009 influenza A(H1N1) virus. Chest 2011, 139, 555–562. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; J Schultz, M.; Vincent, J.L.; Alvarez-Lerma, F.; Bos, L.D.; Solé-Violán, J.; Torres, A.; Rodriguez, A. Increased incidence of co-infection in critically ill patients with influenza. Intensive Care Med. 2017, 43, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Cillóniz, C.; Ewig, S.; Ferrer, M.; Polverino, E.; Gabarrús, A.; Puig de la Bellacasa, J.; Mensa, J.; Torres, A. Community-acquired polymicrobial pneumonia in the intensive care unit: Aetiology and prognosis. Crit. Care 2011, 15. [Google Scholar] [CrossRef] [PubMed]
- Loke, Y.K.; Kwok, C.S.; Niruban, A.; Myint, P.K. Value of severity scales in predicting mortality from community-acquired pneumonia: Systematic review and meta-analysis. Thorax 2010, 65, 884–890. [Google Scholar] [CrossRef]
- Langevin, S.; Pichon, M.; Smith, E.; Morrison, J.; Bent, Z.; Green, R.; Barker, K.; Solberg, O.; Gillet, Y.; Javouhey, E.; et al. Early nasopharyngeal microbial signature associated with severe influenza in children: A retrospective pilot study. J. Gen. Virol. 2017, 98, 2425–2437. [Google Scholar] [CrossRef]
- Karakioulaki, M.; Stolz, D. Biomarkers in Pneumonia—Beyond Procalcitonin. Int. J. Mol. Sci. 2019, 20, 2004. [Google Scholar] [CrossRef] [PubMed]
- Guan, J.; Lin, Z.; Lue, H. Dynamic change of procalcitonin, rather than concentration itself, is predictive of survival in septic shock patients when beyond 10 ng/mL. Shock 2011, 36, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Charles, P.E.; Tinel, C.; Barbar, S.; Aho, S.; Prin, S.; Doise, J.M.; Olsson, N.O.; Blettery, B.; Quenot, J.P. Procalcitonin kinetics within the first days of sepsis: Relationship with the appropriateness of antibiotic therapy and the outcome. Crit. Care 2009, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. Am. J. Respir. Crit. Care Med. 2019, 200, E45–E67. [Google Scholar] [CrossRef] [PubMed]
- Suberviola, B.; Castellanos-Ortega, A.; González-Castro, A.; García-Astudillo, L.A.; Fernández-Miret, B. Valor pronóstico del aclaramiento de procalcitonina, PCR y leucocitos en el shock séptico. Med. Intensiva 2012, 36, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, S.; Heikkinen, M.; Pettilä, V.; Alila, S.; Väisänen, S.; Pulkki, K.; Kolho, E.; Ruokonen, E.; The Finnsepsis Study Group. Predictive value of procalcitonin decrease in patients with severe sepsis: A prospective observational study. Crit. Care 2010, 14, R205. [Google Scholar] [CrossRef]
- Liu, D.; Su, L.; Han, G.; Yan, P.; Xie, L. Prognostic Value of Procalcitonin in Adult Patients with Sepsis: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0129450. [Google Scholar] [CrossRef]
- Liu, D.; Su, L.X.; Guan, W.; Xiao, K.; Xie, L.X. Prognostic value of procalcitonin in pneumonia: A systematic review and meta-analysis. Respirology 2016, 21, 280–288. [Google Scholar] [CrossRef]
- Leli, C.; Ferranti, M.; Moretti, A.; Al Dhahab, Z.S.; Cenci, E.; Mencacci, A. Procalcitonin levels in gram-positive, gram-negative, and fungal bloodstream infections. Dis. Markers 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.-H.; Gao, D.-P.; Zou, P.-F. Comparison of serum PCT and CRP levels in patients infected by different pathogenic microorganisms: A systematic review and meta-analysis. Brazilian J. Med. Biol. Res. 2018, 51, 1–8. [Google Scholar] [CrossRef]
- Porfyridis, I.; Georgiadis, G.; Vogazianos, P.; Mitis, G.; Georgiou, A. C-Reactive Protein, Procalcitonin, Clinical Pulmonary Infection Score, and Pneumonia Severity Scores in Nursing Home Acquired Pneumonia. Respir. Care 2014, 59, 574–581. [Google Scholar] [CrossRef]
- Charles, P.E.; Ladoire, S.; Aho, S.; Quenot, J.P.; Doise, J.M.; Prin, S.; Olsson, N.O.; Blettery, B. Serum procalcitonin elevation in critically ill patients at the onset of bacteremia caused by either gram negative or gram positive bacteria. BMC Infect. Dis. 2008, 8, 38. [Google Scholar] [CrossRef] [PubMed]
- Vanderbeke, L.; Spriet, I.; Breynaert, C. Invasive pulmonary aspergillosis complicating severe influenza: Epidemiology, diagnosis and treatment. Curr. Opin. Infect. Dis. 2018. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall Population n = 1608 | PVP n = 1186 | BC n = 422 | p-Value | |
|---|---|---|---|---|
| Demographic Factors and Severity Scores | ||||
| Age (years) | 56 (45–67) | 55 (44–66) | 60 (48–72) | 0.001 |
| Gender (male) | 960 (59.7) | 697 (58.8) | 263 (62) | 0.24 |
| APACHE II score | 17 (12–22) | 16 (11–21) | 19 (14–25) | 0.001 |
| SOFA score | 6 (4–9) | 6 (4–8) | 7 (4–10) | 0.001 |
| Comorbidity | ||||
| COPD | 328 (20.4) | 77 (6.5) | 31 (7.3) | 0.45 |
| Asthma | 109 (6.8) | 203 (17.1) | 124 (29.4) | 0.001 |
| Chronic Heart Failure | 210 (13.1) | 149 (12.6) | 61 (14.5) | 0.34 |
| Chronic Kidney Disease | 146 (9.1) | 109 (9.2) | 37 (8.8) | 0.77 |
| Hematologic Disease | 138 (8.6) | 100 (8.4) | 38 (9) | 0.73 |
| Pregnancy | 240 (14.9) | 168 (14.2) | 72 (17.1) | 0.16 |
| Obesity a | 135 (8.4) | 407 (34.3) | 23 (5.5) | 0.01 |
| Laboratory Findings | ||||
| PCT (ng/mL) | 0.81 (0.24–4.79) | 0.6 (0.2–2.31) | 4.35 (0.6–19.7) | 0.001 |
| CRP (mg/dL) | 30.2 (14.8–113) | 28.1 (13.3–109) | 36.8 (20.4–118) | 0.001 |
| White Blood Cell Count (109/L) | 7.4 (3.8–12.4) | 7.1 (4–11.6) | 8.3 (2.9–15.2) | 0.06 |
| Complications | ||||
| Acute Kidney Failure | 530 (32.9) | 337 (28.4) | 193 (45.7) | 0.001 |
| CRRT | 215 (13.4) | 140 (11.8) | 75 (17.8) | 0.002 |
| Mechanical Ventilation | 1318 (81.9) | 974 (82.1) | 342 (81) | 0.65 |
| Shock on Admission | 920 (57.1) | 634 (53.5) | 284 (67.3) | 0.001 |
| MODS | 1100 (68.4) | 775 (65.3) | 323 (76.5) | 0.001 |
| Clinical Outcomes | ||||
| MV (days) | 10 (4–19) | 10 (4–19) | 10 (4–18) | 0.85 |
| ICU LOS (days) | 10 (5–20) | 10 (5–21) | 10 (5–19) | 0.73 |
| ICU Mortality | 382 (23.8) | 264 (22.3) | 117 (27.7) | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbonell, R.; Moreno, G.; Martín-Loeches, I.; Gomez-Bertomeu, F.; Sarvisé, C.; Gómez, J.; Bodí, M.; Díaz, E.; Papiol, E.; Trefler, S.; et al. Prognostic Value of Procalcitonin and C-Reactive Protein in 1608 Critically Ill Patients with Severe Influenza Pneumonia. Antibiotics 2021, 10, 350. https://doi.org/10.3390/antibiotics10040350
Carbonell R, Moreno G, Martín-Loeches I, Gomez-Bertomeu F, Sarvisé C, Gómez J, Bodí M, Díaz E, Papiol E, Trefler S, et al. Prognostic Value of Procalcitonin and C-Reactive Protein in 1608 Critically Ill Patients with Severe Influenza Pneumonia. Antibiotics. 2021; 10(4):350. https://doi.org/10.3390/antibiotics10040350
Chicago/Turabian StyleCarbonell, Raquel, Gerard Moreno, Ignacio Martín-Loeches, Frederic Gomez-Bertomeu, Carolina Sarvisé, Josep Gómez, María Bodí, Emili Díaz, Elisabeth Papiol, Sandra Trefler, and et al. 2021. "Prognostic Value of Procalcitonin and C-Reactive Protein in 1608 Critically Ill Patients with Severe Influenza Pneumonia" Antibiotics 10, no. 4: 350. https://doi.org/10.3390/antibiotics10040350
APA StyleCarbonell, R., Moreno, G., Martín-Loeches, I., Gomez-Bertomeu, F., Sarvisé, C., Gómez, J., Bodí, M., Díaz, E., Papiol, E., Trefler, S., Nieto, M., Estella, A., Jiménez Herrera, M., Vidal Cortés, P., Guardiola, J. J., Solé-Violán, J., & Rodríguez, A. (2021). Prognostic Value of Procalcitonin and C-Reactive Protein in 1608 Critically Ill Patients with Severe Influenza Pneumonia. Antibiotics, 10(4), 350. https://doi.org/10.3390/antibiotics10040350