
Predicting the Effects of Carbapenem/Carbapenemase Inhibitor Combinations against KPC-Producing Klebsiella pneumoniae in Time-Kill Experiments: Alternative versus Traditional Approaches to MIC Determination

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. MICs of Imipenem or Doripenem Alone and in the Presence of Relebactam
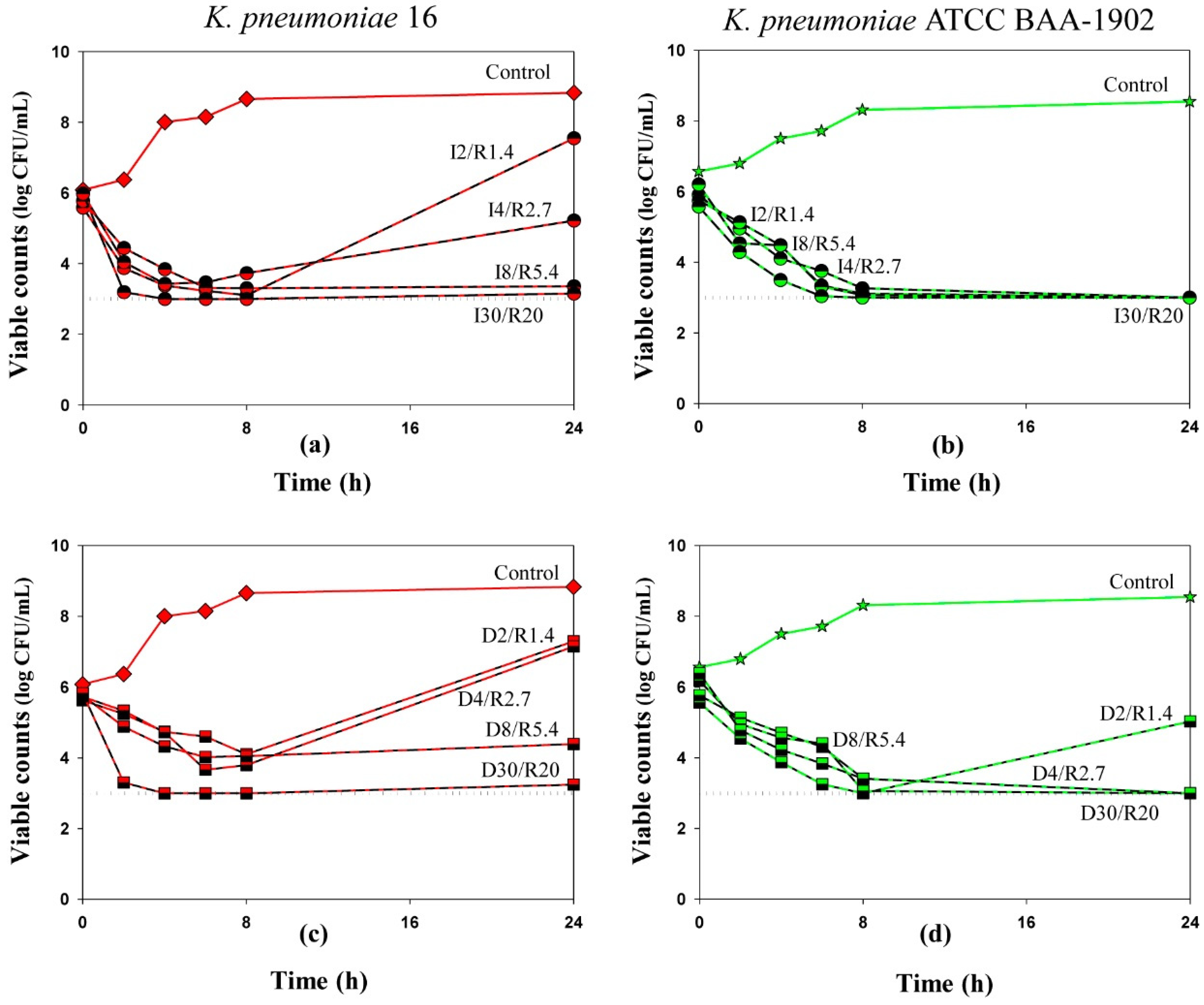
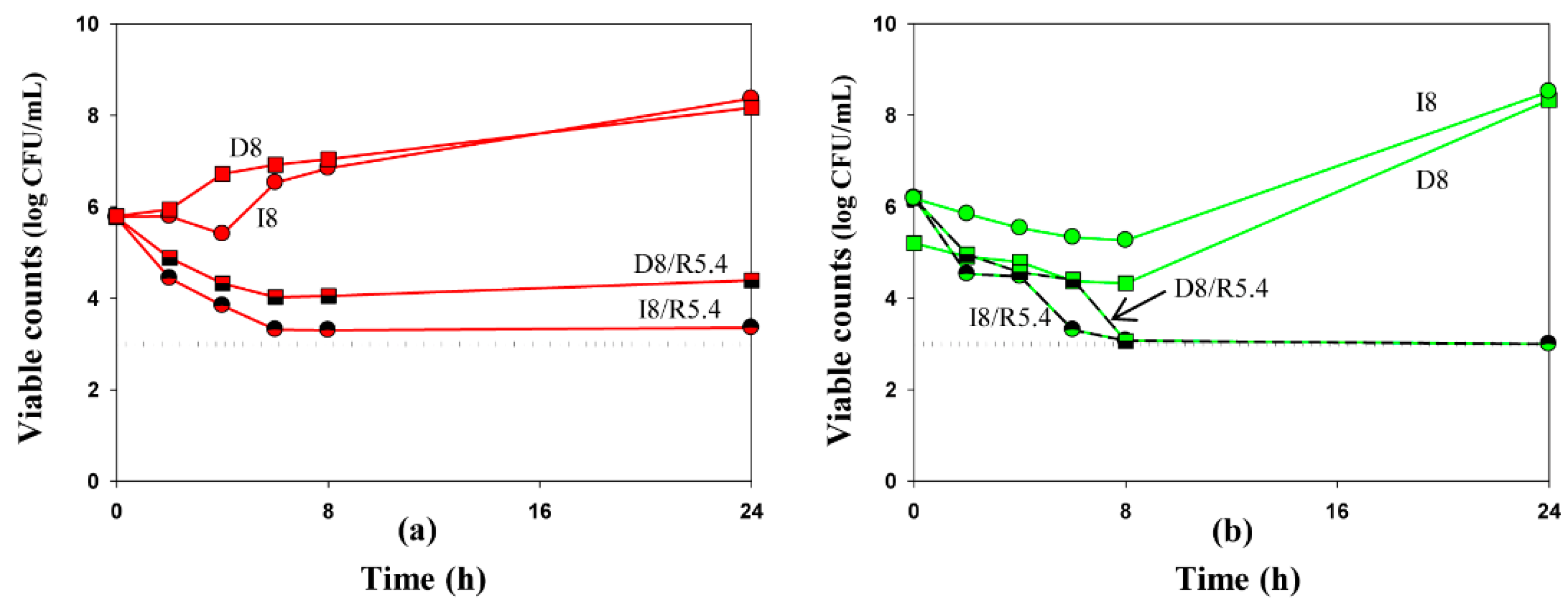
2.2. Time-Kill Experiments with K. Pneumoniae
3. Discussion
4. Materials and Methods
4.1. Antimicrobial Agents and Bacterial Strains
4.2. Susceptibility Testing
4.3. Time-Kill Assay Procedure
4.4. Drug Exposures
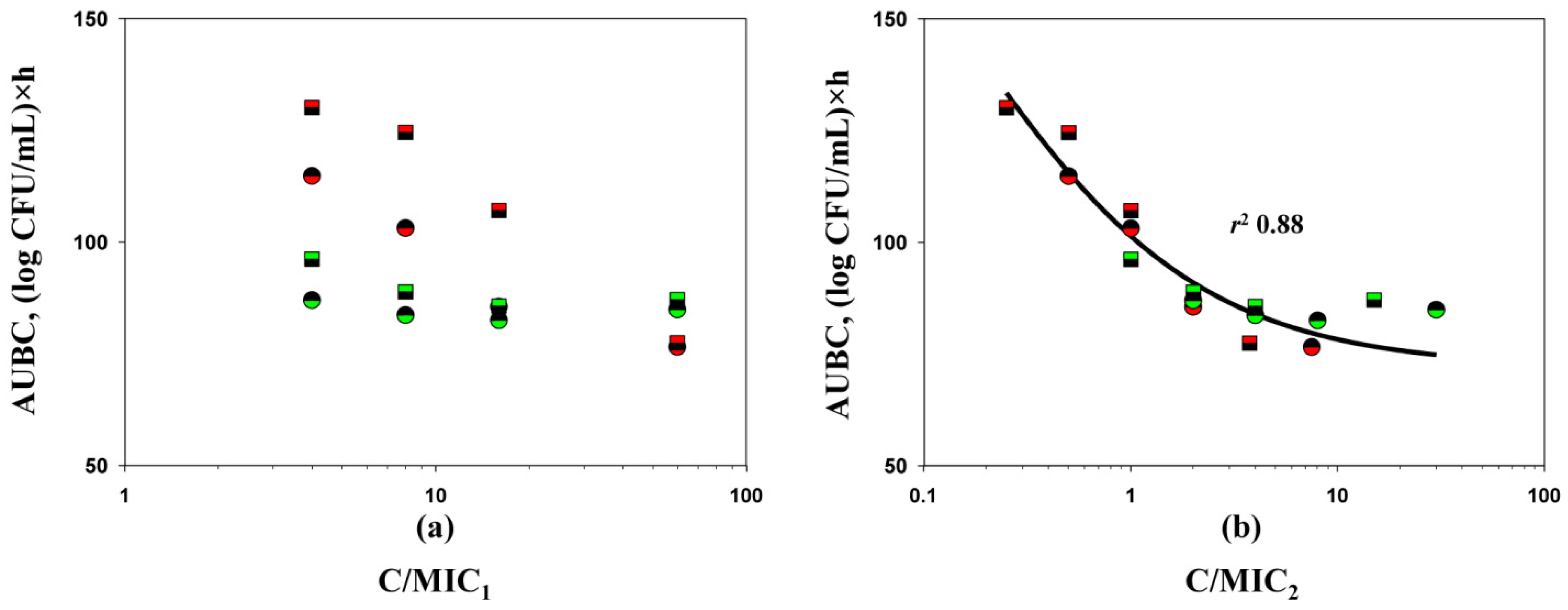
4.5. Quantitation of the Antimicrobial Effect and its Relationships with C/MIC Ratios
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mansour, H.; Ouweini, A.E.L.; Chahine, E.B.; Karaoui, L.R. Imipenem/cilastatin/relebactam: A new carbapenem β-lactamase inhibitor combination. Am. J. Health Syst. Pharm. 2021, 78, 674–683. [Google Scholar] [CrossRef]
- Lapuebla, A.; Abdallah, M.; Olafisoye, O.; Cortes, C.; Urban, C.; Landman, D.; Quale, J. Activity of imipenem with relebactam against Gram-negative pathogens from New York City. Antimicrob. Agents Chemother. 2015, 59, 5029–5031. [Google Scholar] [CrossRef] [Green Version]
- Karlowsky, J.A.; Lob, S.H.; Kazmierczak, K.M.; Young, K.; Motyl, M.R.; Sahm, D.F. In vitro activity of imipenem/relebactam against Enterobacteriaceae and Pseudomonas aeruginosa isolated from intraabdominal and urinary tract infection samples: SMART Surveillance United States 2015-2017. J. Glob. Antimicrob. Resist. 2020, 21, 223–228. [Google Scholar] [CrossRef]
- Smith, J.R.; Rybak, J.M.; Claeys, K.C. Imipenem-cilastatin-relebactam: A novel β-lactam-β-lactamase inhibitor combination for the treatment of multidrug-resistant Gram-negative infections. Pharmacotherapy 2020, 40, 343–356. [Google Scholar] [CrossRef]
- Andrei, S.; Droc, G.; Stefan, G. FDA approved antibacterial drugs: 2018–2019. Discoveries 2019, 31, e102. [Google Scholar] [CrossRef] [PubMed]
- Thakare, R.; Dasgupta, A.; Chopra, S. Imipenem/cilastatin sodium/relebactam fixed combination to treat urinary infections and complicated intra-abdominal bacterial infections. Drugs Today 2020, 56, 241–255. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-antibiotic-treat-hospital-acquired-bacterial-pneumonia-and-ventilator-associated (accessed on 19 November 2021).
- Tooke, C.L.; Hinchliffe, P.; Lang, P.A.; Mulholland, A.J.; Brem, J.; Schofield, C.J.; Spencer, J. Molecular basis of class A β-lactamase inhibition by relebactam. Antimicrob. Agents Chemother. 2019, 63, e00564-19. [Google Scholar] [CrossRef] [Green Version]
- Heo, Y.A. Imipenem/cilastatin/relebactam: A review in Gram-negative bacterial infections. Drugs 2021, 81, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Clinical Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically (M07), 11th ed.; Clinical Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2019. [Google Scholar]
- Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Dovzhenko, S.A.; Kobrin, M.B.; Zinner, S.H.; Firsov, A.A. Predicting effects of antibiotic combinations using MICs determined at pharmacokinetically derived concentration ratios: In vitro model studies with linezolid- and rifampicin-exposed Staphylococcus aureus. J. Chemother. 2017, 5, 267–273. [Google Scholar] [CrossRef]
- Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Zinner, S.H.; Firsov, A.A. Predicting the antistaphylococcal effects of daptomycin-rifampicin combinations in an in vitro dynamic model. J. Antibiot. 2020, 73, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Zinner, S.H.; Firsov, A.A. Verification of a novel approach to predicting effects of antibiotic combinations: In vitro dynamic model study with daptomycin and gentamicin against Staphylococcus aureus. Antibiotics 2020, 9, 538. [Google Scholar] [CrossRef]
- Zinner, S.H.; Alieva, K.N.; Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Firsov, A.A. Anti-mutant efficacy of antibiotic combinations: In vitro model studies with linezolid and daptomycin. J. Antimicrob. Chemother. 2021, 76, 1832–1839. [Google Scholar] [CrossRef]
- Golikova, M.V.; Strukova, E.N.; Alieva, K.N.; Portnoy, Y.A.; Filimonova, A.V.; Zinner, S.H.; Firsov, A.A. A pharmacokinetically-based approach to predict anti-mutant efficacy of combined doripenem and levofloxacin therapy in in vitro model studies with Pseudomonas aeruginosa. In Proceedings of the 31th European Congress of Clinical Microbiology & Infectious Diseases, Abstract No. 833. Online, 9–12 July 2021. [Google Scholar]
- Firsov, A.A.; Saverino, D.; Ruble, M.; Gilbert, D.; Manzano, B.; Medeiros, A.A.; Zinner, S.H. Predictors of effect of ampicillin-sulbactam against TEM-1 β-lactamase-producing Escherichia coli in an in vitro dynamic model: Enzyme activity versus MIC. Antimicrob. Agents Chemother. 1996, 40, 734–738. [Google Scholar] [CrossRef] [Green Version]
- Clinical Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing (M100), 30th ed.; Clinical Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2020. [Google Scholar]
- Keepers, T.R.; Gomez, M.; Celeri, C.; Nichols, W.W.; Krause, K.M. Bactericidal activity, absence of serum effect, and time-kill kinetics of ceftazidime-avibactam against β-lactamase-producing Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2014, 58, 5297–5305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morroni, G.; Bressan, R.; Fioriti, S.; D’Achille, G.; Mingoia, M.; Cirioni, O.; Di Bella, S.; Piazza, A.; Comandatore, F.; Mauri, C.; et al. Antimicrobial activity of aztreonam in combination with old and new β-Lactamase inhibitors against MBL and ESBL co-producing Gram-negative clinical isolates: Possible options for the treatment of complicated infections. Antibiotics 2021, 10, 1341. [Google Scholar] [CrossRef]
- Sy, S.K.; Zhuang, L.; Beaudoin, M.E.; Kircher, P.; Tabosa, M.A.; Cavalcanti, N.C.; Grunwitz, C.; Pieper, S.; Schuck, V.J.; Nichols, W.W.; et al. Potentiation of ceftazidime by avibactam against β-lactam-resistant Pseudomonas aeruginosa in an in vitro infection model. J. Antimicrob. Chemother. 2017, 72, 1109–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero, M.M.; Domene, O.S.; López-Causapé, C.; Luque, S.; Sorlí, L.; Campillo, N.; López, M.I.; Padilla, E.; Prim, N.; Angulo-Brunet, A.; et al. Time-kill evaluation of antibiotic combinations containing ceftazidime-avibactam against extensively drug-resistant Pseudomonas aeruginosa and their potential role against ceftazidime-avibactam-resistant isolates. Microbiol. Spectr. 2021, 9, e0058521. [Google Scholar] [CrossRef]
- Asempa, T.E.; Nicolau, D.P.; Kuti, J.L. In vitro activity of imipenem-relebactam alone or in combination with amikacin or colistin against Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2019, 63, e00997-19. [Google Scholar] [CrossRef] [Green Version]
- Mueller, M.; de la Peña, A.; Derendorf, H. Issues in pharmacokinetics and pharmacodynamics of anti-infective agents: Kill curves versus MIC. Antimicrob. Agents Chemother. 2004, 48, 369–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Zwaluw, K.; de Haan, A.; Pluister, G.N.; Bootsma, H.J.; de Neeling, A.J.; Schouls, L.M. The carbapenem inactivation method (CIM), a simple and low-cost alternative for the Carba NP test to assess phenotypic carbapenemase activity in gram-negative rods. PLoS ONE 2015, 10, e0123690. [Google Scholar] [CrossRef] [Green Version]
- Cirillo, I.; Vaccaro, N.; Turner, K.; Solanki, B.; Natarajan, J.; Redman, R. Pharmacokinetics, safety, and tolerability of doripenem after 0.5-, 1-, and 4-hour infusions in healthy volunteers. J. Clin. Pharmacol. 2009, 49, 798–806. [Google Scholar] [CrossRef] [PubMed]
- Rhee, E.G.; Rizk, M.L.; Calder, N.; Nefliu, M.; Warrington, S.J.; Schwartz, M.S.; Mangin, E.; Boundy, K.; Bhagunde, P.; Colon-Gonzalez, F.; et al. Pharmacokinetics, safety, and tolerability of single and multiple doses of relebactam, a β-lactamase inhibitor, in combination with imipenem and cilastatin in healthy participants. Antimicrob. Agents Chemother. 2018, 62, e00280-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| K. pneumoniae Strain | Imipenem | Imipenem in the Presence of Relebactam | Doripenem | Doripenem in the Presence of Relebactam | ||
|---|---|---|---|---|---|---|
| MIC1 | MIC2 | MIC1 | MIC2 | |||
| 16 | 64 | 0.5 | 4 | 128 | 0.5 | 8 |
| ATCC BAA-1902 | 64 | 0.5 | 1 | 64 | 0.5 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filimonova, A.V.; Golikova, M.V.; Strukova, E.N.; Portnoy, Y.A.; Kuznetsova, A.A.; Zinner, S.H. Predicting the Effects of Carbapenem/Carbapenemase Inhibitor Combinations against KPC-Producing Klebsiella pneumoniae in Time-Kill Experiments: Alternative versus Traditional Approaches to MIC Determination. Antibiotics 2021, 10, 1520. https://doi.org/10.3390/antibiotics10121520
Filimonova AV, Golikova MV, Strukova EN, Portnoy YA, Kuznetsova AA, Zinner SH. Predicting the Effects of Carbapenem/Carbapenemase Inhibitor Combinations against KPC-Producing Klebsiella pneumoniae in Time-Kill Experiments: Alternative versus Traditional Approaches to MIC Determination. Antibiotics. 2021; 10(12):1520. https://doi.org/10.3390/antibiotics10121520
Chicago/Turabian StyleFilimonova, Alla V., Maria V. Golikova, Elena N. Strukova, Yury A. Portnoy, Anastasiya A. Kuznetsova, and Stephen H. Zinner. 2021. "Predicting the Effects of Carbapenem/Carbapenemase Inhibitor Combinations against KPC-Producing Klebsiella pneumoniae in Time-Kill Experiments: Alternative versus Traditional Approaches to MIC Determination" Antibiotics 10, no. 12: 1520. https://doi.org/10.3390/antibiotics10121520
APA StyleFilimonova, A. V., Golikova, M. V., Strukova, E. N., Portnoy, Y. A., Kuznetsova, A. A., & Zinner, S. H. (2021). Predicting the Effects of Carbapenem/Carbapenemase Inhibitor Combinations against KPC-Producing Klebsiella pneumoniae in Time-Kill Experiments: Alternative versus Traditional Approaches to MIC Determination. Antibiotics, 10(12), 1520. https://doi.org/10.3390/antibiotics10121520