Trends in Antibiotic Prescribing in Out-of-Hours Primary Care in England from January 2016 to June 2020 to Understand Behaviours during the First Wave of COVID-19

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Results
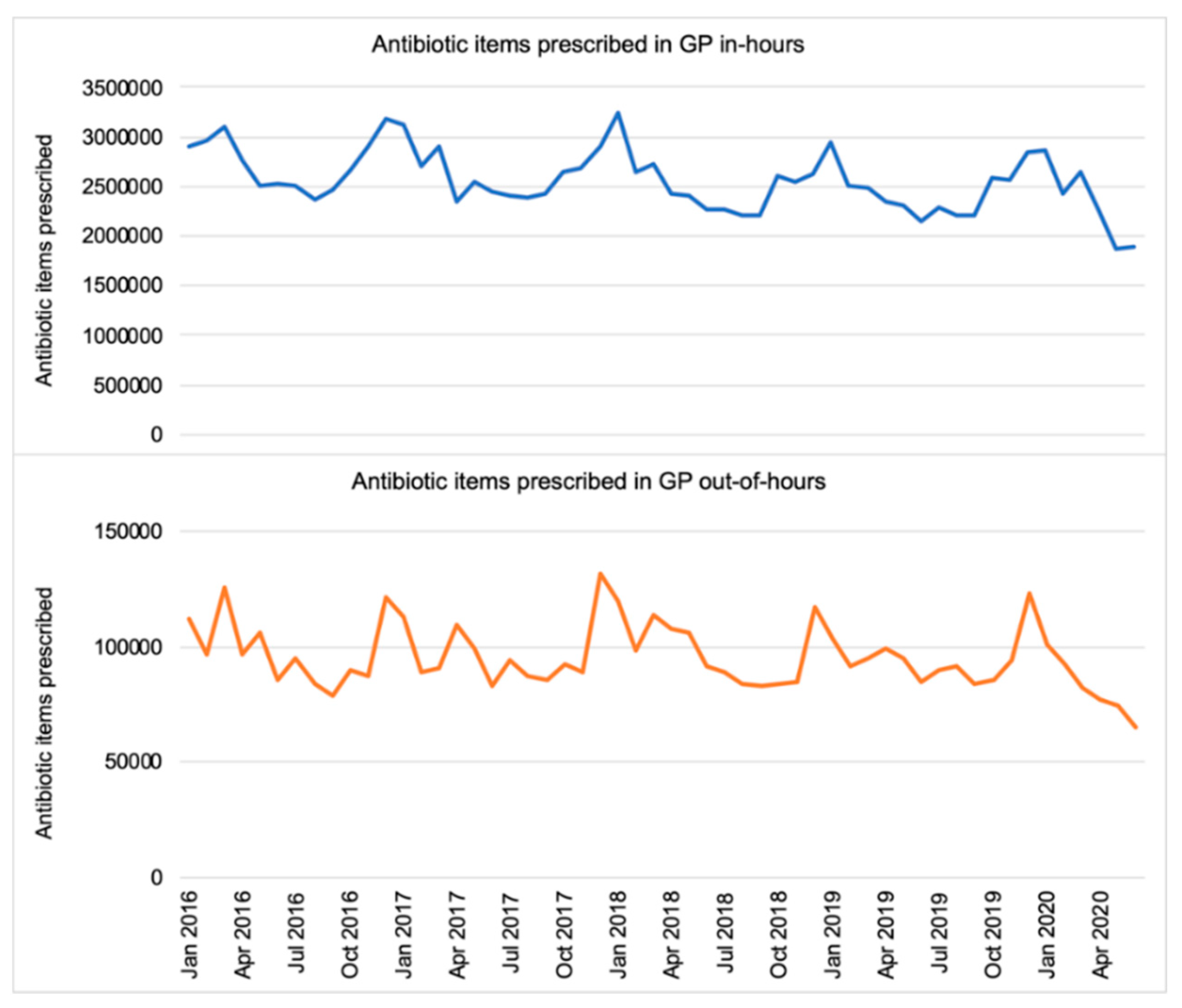
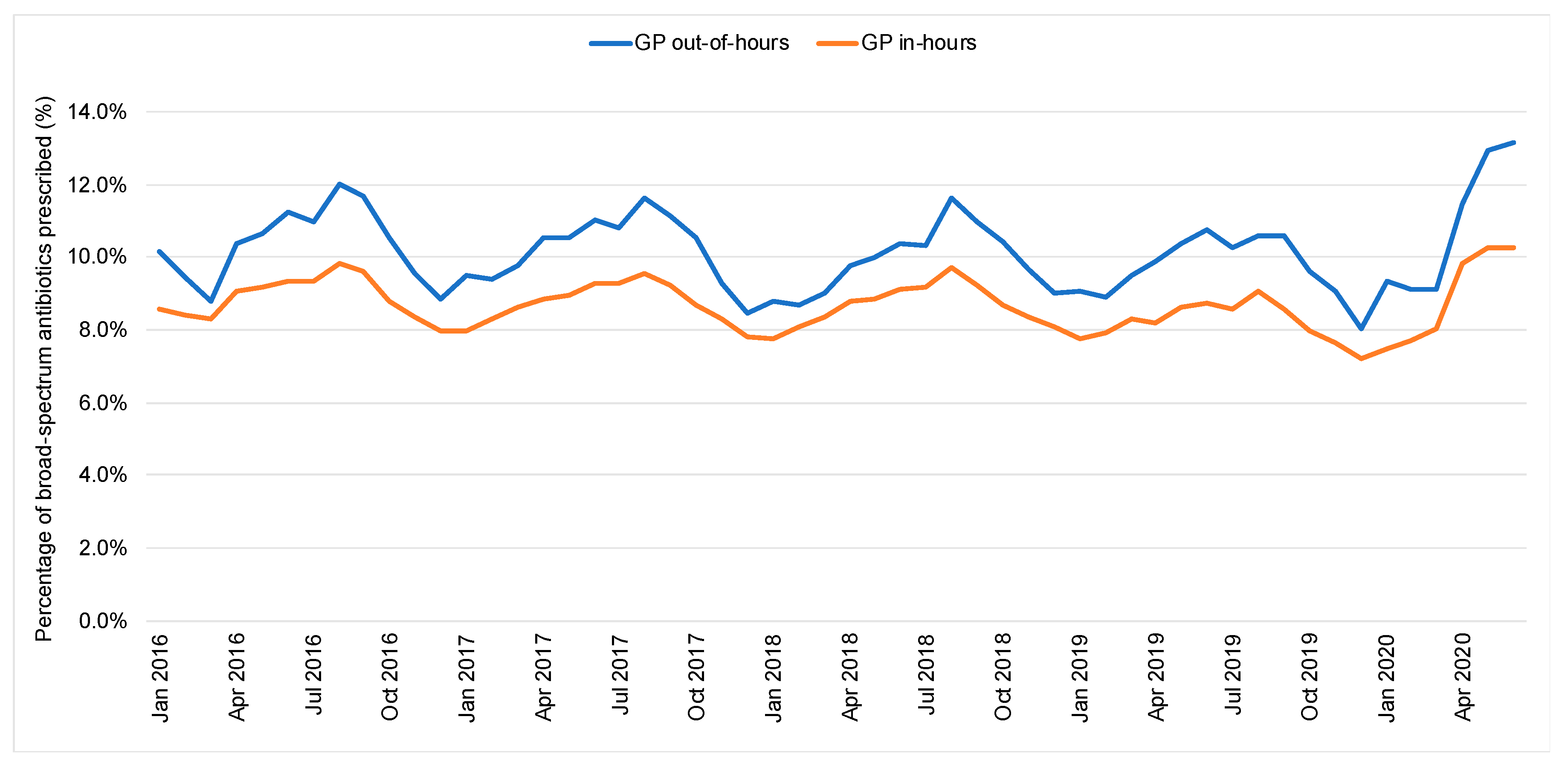
2.1. Antibiotic Prescribing in GP In-Hours and Out-of-Hours
2.2. Respiratory Tract and Chest Infection Antibiotics in Out-of-Hours
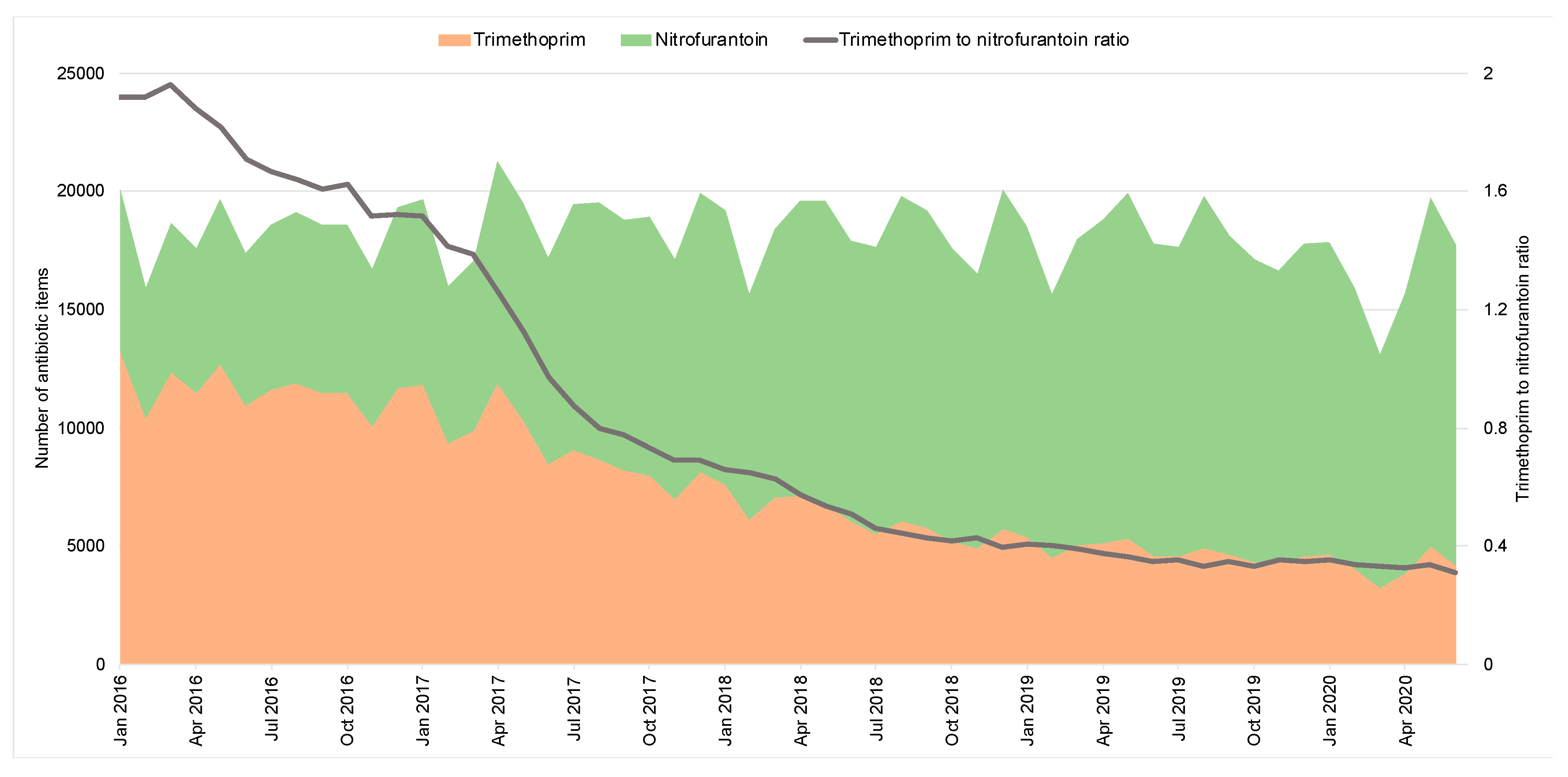
2.3. Urinary Tract Infection Antibiotics in Out-of-Hours
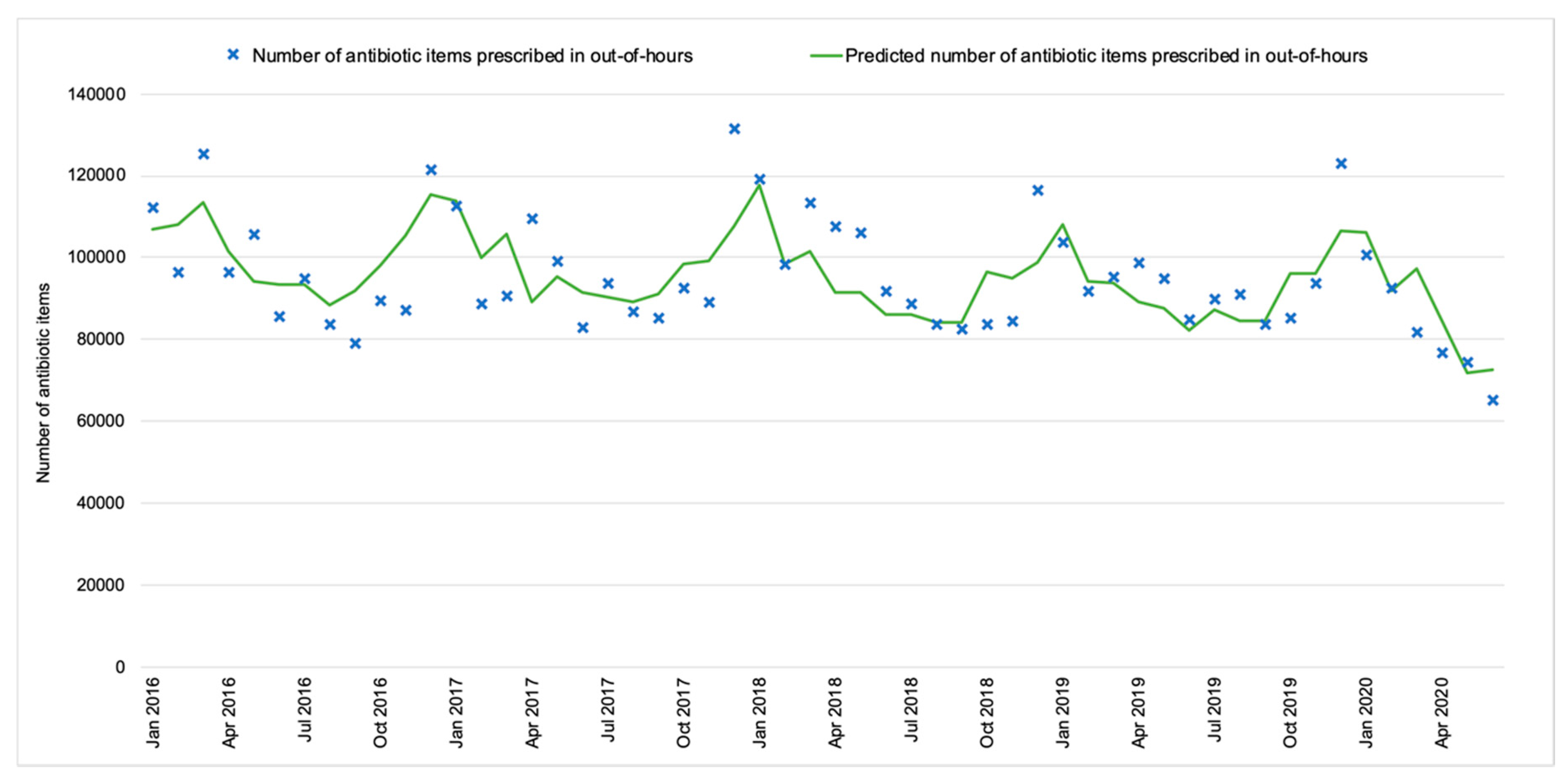
2.4. Out-of-Hours Antibiotic Prescribing in the Context of the COVID-19 Pandemic
3. Discussion
4. Materials and Methods
4.1. Ethical Approval
4.2. Data
4.3. Descriptive and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Monitoring Global Progress on Addressing Antimicrobial Resistance: Analysis Report of the Second Round of Results of AMR Country Self-Assessment Survey; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Department of Health and Social Care. Tackling Antimicrobial Resistance 2019–2024: The UK’s Five-Year National Action Plan; Department of Health and Social Care: London, UK, 2019.
- Smieszek, T.; Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.M.; Hopkins, S.; Sharland, M.; Hay, A.D.; Moore, M.V.; Robotham, J.V. Potential for reducing inappropriate antibiotic prescribing in English primary care. J. Antimicrob. Chemother. 2018, 73, ii36–ii43. [Google Scholar] [CrossRef] [PubMed]
- Mayor, S. Doctors to get real time data to support antibiotic prescribing and reduce resistance. BMJ 2019, 364, l406. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report; PHE Gateway Number: GW-1648; Public Health England: London, UK, 2019.
- Rutter, V.; Kessel, A.; Hopkins, S.; Brown, B.; Brown, N.; Carter, S.; Charlett, A.; Cichowka, A.; Faulding, S.; Gallagher, R.; et al. Antimicrobial stewardship: English Surveillance Programme for Antimicrobial Utilization and Resistance (ESPAUR). J. Antimicrob. Chemother. 2013, 68, 2421–2423. [Google Scholar] [CrossRef]
- National Audit Office. Out-of-Hours GP Services in England; National Audit Office: London, UK, 2014.
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014. Available online: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf (accessed on 20 September 2020).
- NHS. Quality Premium. CCG Outcomes Tools. 2015. Available online: https://www.england.nhs.uk/ccg-out-tool/qual-prem/ (accessed on 20 October 2020).
- Balinskaite, V.; Johnson, A.P.; Holmes, A.; Aylin, P.P. The Impact of a National Antimicrobial Stewardship Program on Antibiotic Prescribing in Primary Care: An Interrupted Time Series Analysis. Clin. Infect. Dis. 2018, 69, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Bou-Antoun, S.; Costelloe, C.; Honeyford, K.; Mazidi, M.; Hayhoe, B.; Holmes, A.; Johnson, A.P.; Aylin, P.P. Age-related decline in antibiotic prescribing for uncomplicated respiratory tract infections in primary care in England following the introduction of a national financial incentive (the Quality Premium) for health commissioners to reduce use of antibiotics in the community: An interrupted time series analysis. J. Antimicrob. Chemother. 2018, 73, 2883–2892. [Google Scholar] [CrossRef] [PubMed]
- Edelstein, M.; Agbebiyi, A.; Ashiru-Oredope, D.; Hopkins, S. Trends and patterns in antibiotic prescribing among out-of-hours primary care providers in England, 2010–14. J. Antimicrob. Chemother. 2017, 72, 3490–3495. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2014; Public Health England: London, UK, 2014.
- Hayward, G.N.; Fisher, R.F.R.; Spence, G.T.; Lasserson, D.S. Increase in antibiotic prescriptions in out-of-hours primary care in contrast to in-hours primary care prescriptions: Service evaluation in a population of 600 000 patients. J. Antimicrob. Chemother. 2016, 71, 2612–2619. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.J.; Halls, A.; Tonkin-Crine, S.; Moore, M.V.; E Latter, S.; Little, P.; Eyles, C.; Postle, K.; Leydon, G.M. General practitioner and nurse prescriber experiences of prescribing antibiotics for respiratory tract infections in UK primary care out-of-hours services (the UNITE study). J. Antimicrob. Chemother. 2018, 73, 795–803. [Google Scholar] [CrossRef] [PubMed]
- NHS England. The NHS Long Term Plan. 2019. Available online: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf (accessed on 20 September 2020).
- NHS Confederation. GPs Set to Diagnose Covid-19 Face to Face in ‘Hot Hubs’. Pulse, 2020. Available online: https://www.pulsetoday.co.uk/news/uncategorised/gps-set-to-diagnose-covid-19-face-to-face-in-hot-hubs/ (accessed on 20 September 2020).
- Maahase, E. Covid-19: Out-of-hours providers are drafted in to manage non-urgent patients in community. BMJ 2020, 368, m959. [Google Scholar] [CrossRef] [PubMed]
- Royal College of General Practitioners. RCGP Survey Provides Snapshot of How GP Care is accessed in Latest Stages of Pandemic; Royal College of General Practitioners: London, UK, 2020. [Google Scholar]
- Royal College of General Practitioners. Around 7 in 10 Patients Now Receive GP Care Remotely in Bid to Keep Patients Safe During Pandemic, Says RCGP. 2020. Available online: https://www.rcgp.org.uk/about-us/news/2020/april/around-7-in-10-patients-now-receive-gp-care-remotely-in-bid-to-keep-patients-safe-during-pandemic.aspx (accessed on 20 October 2020).
- Majeed, A.; Maile, E.J.; Bindman, A.B. The primary care response to COVID-19 in England’s National Health Service. J. R. Soc. Med. 2020, 113, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Debets, V.E.; Verheij, T.J.; Van Der Velden, A. Antibiotic prescribing during office hours and out-of-hours: A comparison of quality and quantity in primary care in the Netherlands. Br. J. Gen. Pract. 2017, 67, e178–e186. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Antibiotic Guidance for Primary Care: For Consultation and Local Adaptation. Management and Treatment of Common Infections. 2014. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/664740/Managing_common_infections_guidance_for_consultation_and_adaptation.pdf (accessed on 20 October 2020).
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing Suspected or Confirmed Pneumonia in Adults in the Community. 2020. Available online: https://www.nice.org.uk/guidance/ng165 (accessed on 20 October 2020).
- Public Health England. GP Out-of-Hours Syndromic Surveillance: Weekly Bulletins for 2020. 2020. Available online: https://www.gov.uk/government/publications/gp-out-of-hours-syndromic-surveillance-weekly-bulletins-for-2020 (accessed on 20 October 2020).
- Rawson, T.M.; Moore, L.S.P.; Castro-Sánchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the potential long-term impact on antimicrobial resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Clinical Commissioning Groups (CCGs). Who commissions NHS Services? 2020. Available online: https://www.england.nhs.uk/commissioning/who-commissions-nhs-services/ccgs/ (accessed on 20 October 2020).
- NHS England. Clinical Commissioning Group Details. 2020. Available online: https://www.england.nhs.uk/ccg-details/ (accessed on 20 October 2020).
- NHS Digital. Practice Level Prescribing Data. 2020. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/practice-level-prescribing-data (accessed on 20 October 2020).
- NHS Business Services Authority. Practice Level Prescribing Data. 2020. Available online: https://www.nhsbsa.nhs.uk/prescription-data/prescribing-data (accessed on 20 October 2020).
- NHS Digital. GP Practices. 2020. Available online: https://digital.nhs.uk/services/organisation-data-service/data-downloads/gp-and-gp-practice-related-data (accessed on 20 September 2020).
- BMJ Publishing Group Ltd.; Royal Pharmaceutical Society. British National Formulary (BNF) 70; BMJ Publishing Group Ltd.: London, UK, September 2015. [Google Scholar]
- Office for National Statistics. Clinical Commissioning Group Population Estimates. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/clinicalcommissioninggroupmidyearpopulationestimates (accessed on 20 October 2020).
- NHS England. Introduction to the Antibiotic Quality Premium. 2015. Available online: https://www.england.nhs.uk/wp-content/uploads/2015/04/02-amr-lon-intro-antimicrobial-prescribing-qp.pdf (accessed on 20 October 2020).
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2016, 46, 348–355. [Google Scholar] [CrossRef] [PubMed]
- UK Government. Prime Minister’s statement on coronavirus (COVID-19): 23 March 2020. 2020. Available online: https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020 (accessed on 20 September 2020).
- Linden, A. ITSA: Stata Module to Perform Interrupted Time Series Analysis for Single and Multiple Groups. Statistical Software Components. 2015. Available online: https://ideas.repec.org/c/boc/bocode/s457793.html (accessed on 20 October 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Prescribed Antibiotic Items | Prescribed Antibiotic Items per 1000 Inhabitants per day | Proportion of Primary Care Volume Prescribed in OOH (%) | ||||
|---|---|---|---|---|---|---|---|
| Primary Care | GP In-Hours | GP Out-of-Hours | Primary Care | GP In-Hours | GP Out-of-Hours | ||
| 2016 | 34,881,080 | 32,844,420 | 1,178,023 | 1.7 | 1.6 | 0.1 | 3.4% |
| 2017 | 33,654,010 | 31,558,849 | 1,163,962 | 1.7 | 1.6 | 0.1 | 3.5% |
| 2018 | 32,362,944 | 30,159,393 | 1,177,075 | 1.6 | 1.5 | 0.1 | 3.6% |
| 2019 | 31,714,925 | 29,429,925 | 1,136,791 | 1.5 | 1.4 | 0.1 | 3.6% |
| 2020 1,2 | 14,855,823 | 13,933,878 | 492,244 | 1.5 | 1.3 | 0.1 | 3.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, N.J.; McLeod, M.; McNulty, C.A.M.; Lecky, D.M.; Holmes, A.H.; Ahmad, R. Trends in Antibiotic Prescribing in Out-of-Hours Primary Care in England from January 2016 to June 2020 to Understand Behaviours during the First Wave of COVID-19. Antibiotics 2021, 10, 32. https://doi.org/10.3390/antibiotics10010032
Zhu NJ, McLeod M, McNulty CAM, Lecky DM, Holmes AH, Ahmad R. Trends in Antibiotic Prescribing in Out-of-Hours Primary Care in England from January 2016 to June 2020 to Understand Behaviours during the First Wave of COVID-19. Antibiotics. 2021; 10(1):32. https://doi.org/10.3390/antibiotics10010032
Chicago/Turabian StyleZhu, Nina J., Monsey McLeod, Cliodna A. M. McNulty, Donna M. Lecky, Alison H. Holmes, and Raheelah Ahmad. 2021. "Trends in Antibiotic Prescribing in Out-of-Hours Primary Care in England from January 2016 to June 2020 to Understand Behaviours during the First Wave of COVID-19" Antibiotics 10, no. 1: 32. https://doi.org/10.3390/antibiotics10010032
APA StyleZhu, N. J., McLeod, M., McNulty, C. A. M., Lecky, D. M., Holmes, A. H., & Ahmad, R. (2021). Trends in Antibiotic Prescribing in Out-of-Hours Primary Care in England from January 2016 to June 2020 to Understand Behaviours during the First Wave of COVID-19. Antibiotics, 10(1), 32. https://doi.org/10.3390/antibiotics10010032