Functionalized GD2 Electrochemical Immunosensor to Diagnose Minimum Residual Disease of Bone Marrow in Neuroblastoma Effectively


 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Materials
2.2. Electrochemical Three-Electrode Fabrication
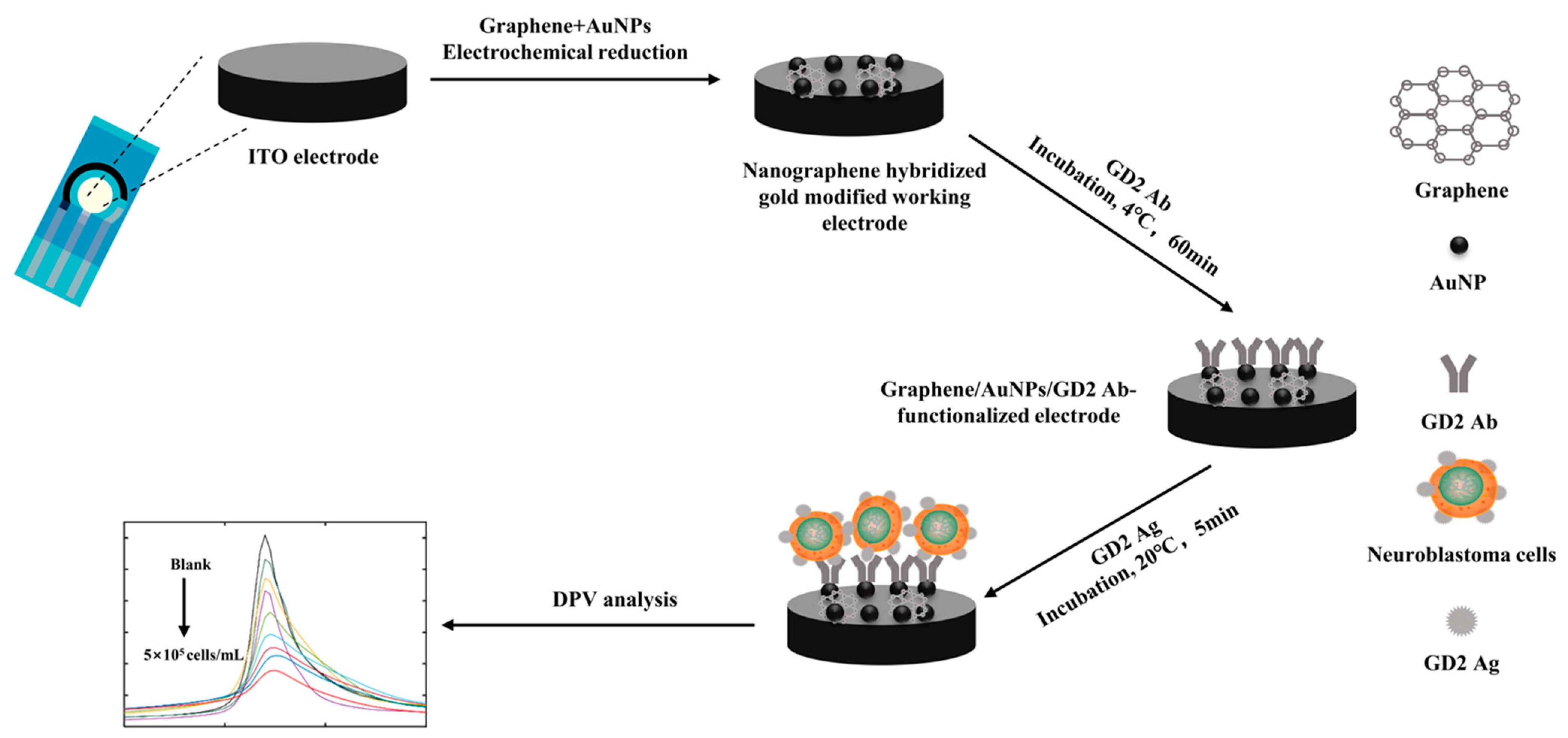
2.3. Graphene/AuNP Modification
2.4. Graphene/AuNP/GD2 Ab-Functionalized Electrode Fabrication
2.5. Cell Culture
2.6. Detection of the Proportion of GD2-Positive Cells in Bone Marrow Samples of Patients with High-Risk NB
2.7. Immunocytochemical Methods for Diagnosis of MRD of Bone Marrow in High-Risk NB
2.8. Flow Cytometry for Diagnosis of MRD of Bone Marrow in High-Risk NB
3. Results and Discussions
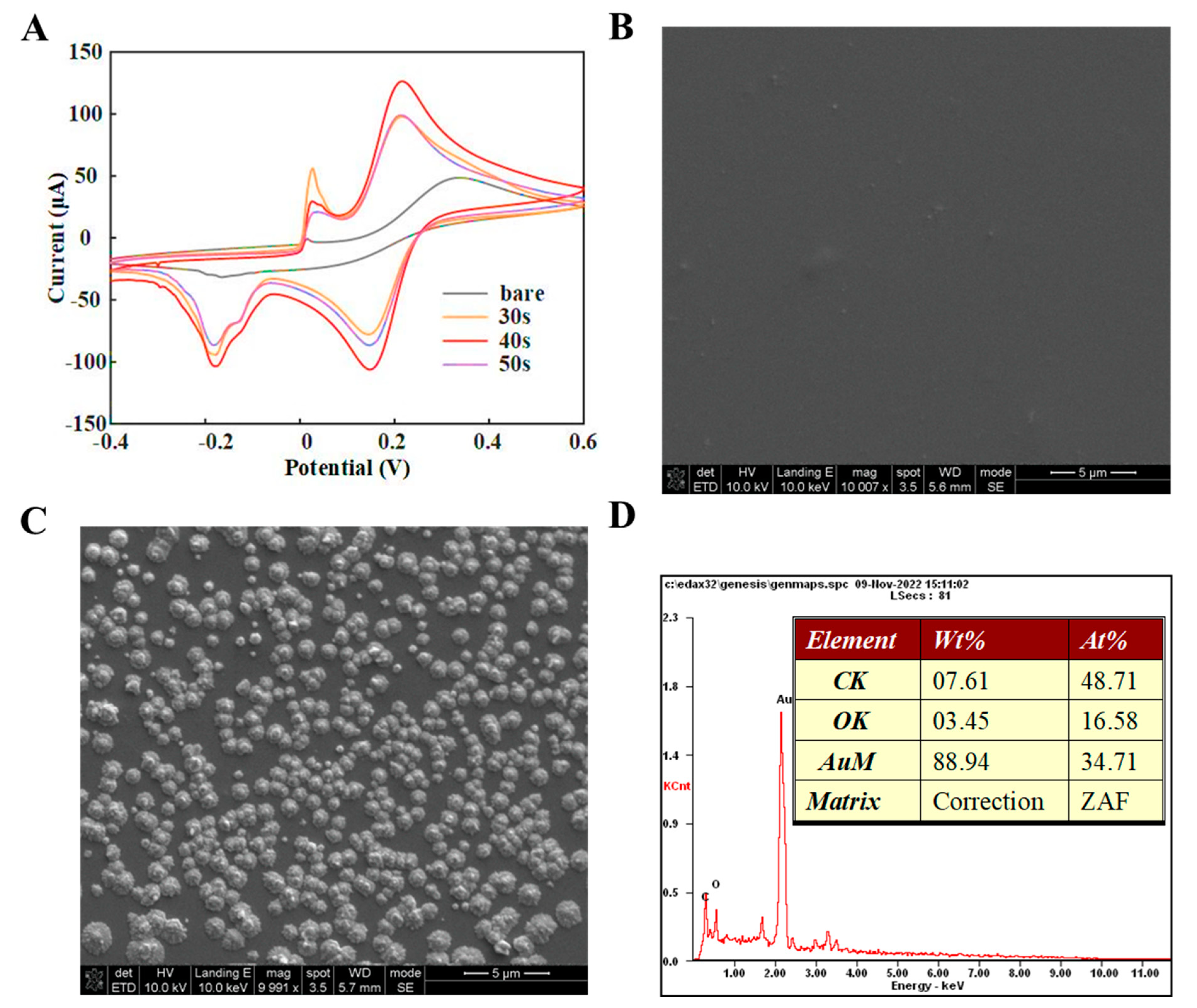
3.1. Graphene/AuNP/GD2 Ab-Functionalized Electrode Characterization
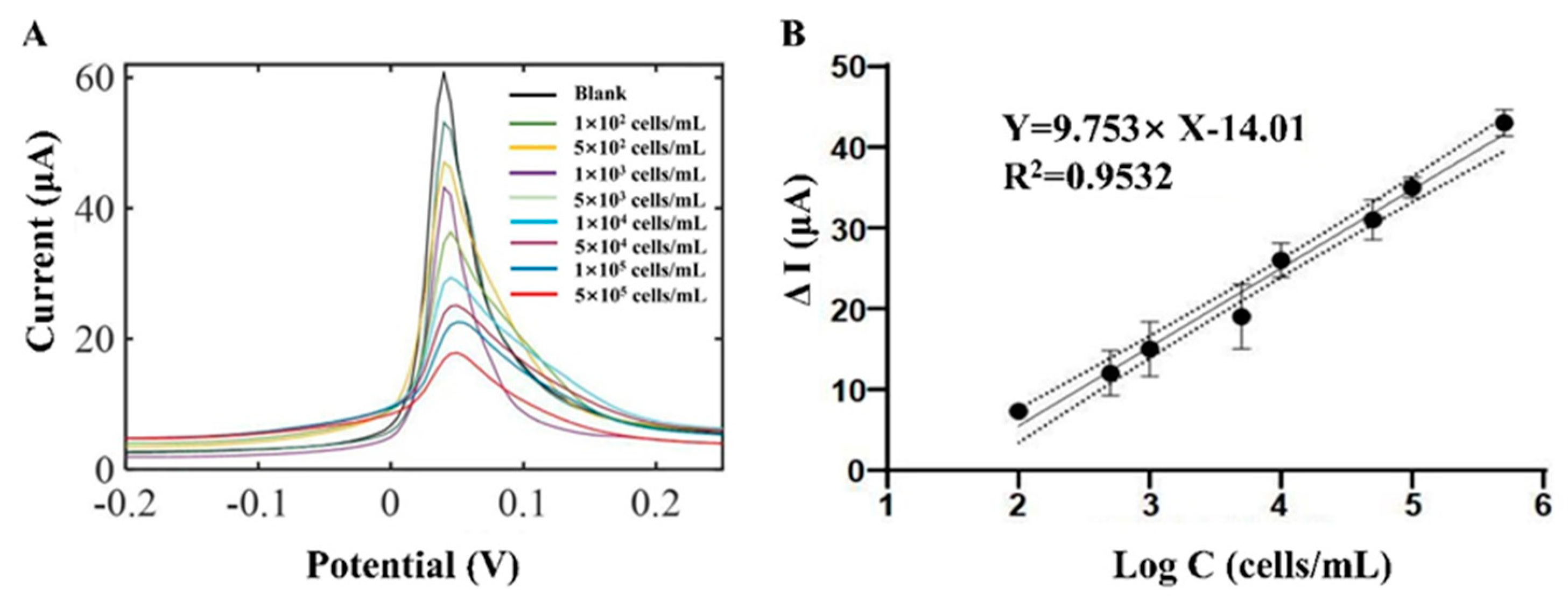
3.2. GD2-Positive Cell Biosensing
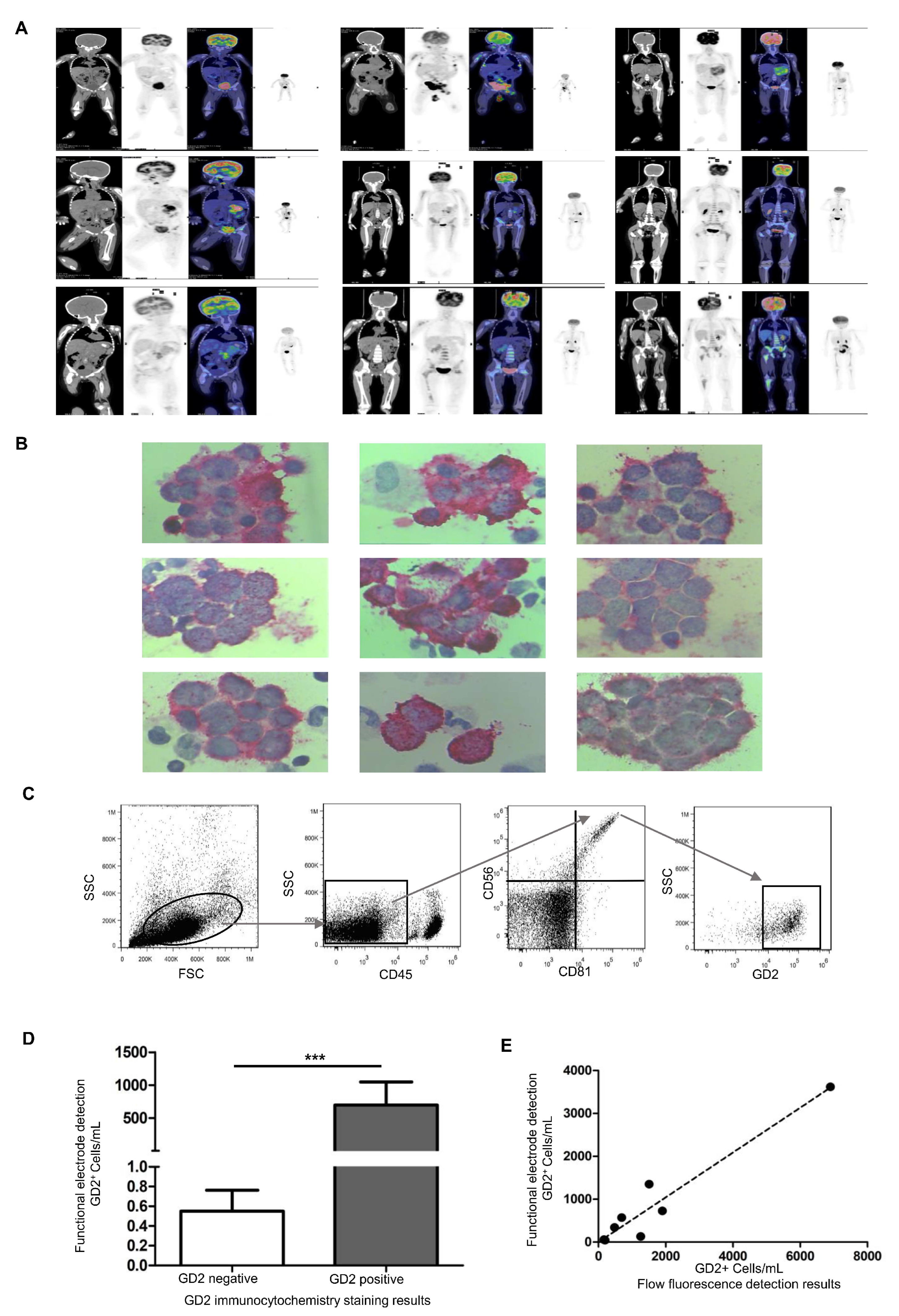
3.3. Bone Marrow Sample Detection in Children with NB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newman, E.A.; Nuchtern, J.G. Recent biologic and genetic advances in neuroblastoma: Implications for diagnostic, risk stratification, and treatment strategies. Semin. Pediatr. Surg. 2016, 25, 257–264. [Google Scholar] [CrossRef]
- Rivera, Z.; Escutia, C.; Madonna, M.B.; Gupta, K.H. Biological Insight and Recent Advancement in the Treatment of Neuroblastoma. Int. J. Mol. Sci. 2023, 24, 8470. [Google Scholar] [CrossRef]
- Gao, J.; Fosbrook, C.; Gibson, J.; Underwood, T.J.; Gray, J.C.; Walters, Z.S. Review: Targeting EZH2 in neuroblastoma. Cancer Treat. Rev. 2023, 119, 102600. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Cotton, M.; Cheung, N.V. Bispecific antibodies for the treatment of neuroblastoma. Pharmacol Ther. 2022, 237, 108241. [Google Scholar] [CrossRef] [PubMed]
- Nader, J.H.; Bourgeois, F.; Bagatell, R.; Moreno, L.; Pearson, A.D.J.; DuBois, S.G. Systematic review of clinical drug development activities for neuroblastoma from 2011 to 2020. Pediatr. Blood. Cancer. 2023, 70, e30106. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.B.; Bae, G.E.; Lee, N.H.; Kim, J.S.; Lee, S.H.; Yoo, K.H.; Sung, K.W.; Koo, H.H. Clinical Significance of Persistent Tumor in Bone Marrow during Treatment of High-risk Neuroblastoma. J. Korean Med. Sci. 2015, 30, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Schramm, A.; Koster, J.; Assenov, Y.; Althoff, K.; Peifer, M.; Mahlow, E.; Odersky, A.; Beisser, D.; Ernst, C.; Henssen, A.G.; et al. Mutational dynamics between primary and relapse neuroblastomas. Nat. Genet. 2015, 47, 872–877. [Google Scholar] [CrossRef]
- Aaltonen, K.; Radke, K.; Adamska, A.; Seger, A.; Manas, A.; Bexell, D. Patient-derived models: Advanced tools for precision medicine in neuroblastoma. Front. Oncol. 2022, 12, 1085270. [Google Scholar] [CrossRef]
- Ceci, A.; Conte, R.; Didio, A.; Landi, A.; Ruggieri, L.; Giannuzzi, V.; Bonifazi, F. Target therapy for high-risk neuroblastoma treatment: Integration of regulatory and scientific tools is needed. Front. Med. 2023, 10, 1113460. [Google Scholar] [CrossRef]
- Bhavsar, S.P. Metastasis in neuroblastoma: The MYCN question. Front. Oncol. 2023, 13, 1196861. [Google Scholar] [CrossRef]
- Cohn, S.L.; Pearson, A.D.; London, W.B.; Monclair, T.; Ambros, P.F.; Brodeur, G.M.; Faldum, A.; Hero, B.; Iehara, T.; Machin, D.; et al. The International Neuroblastoma Risk Group (INRG) classification system: An INRG Task Force report. J. Clin. Oncol. 2009, 27, 289–297. [Google Scholar] [CrossRef]
- Shendy, N.A.M.; Zimmerman, M.W.; Abraham, B.J.; Durbin, A.D. Intrinsic transcriptional heterogeneity in neuroblastoma guides mechanistic and therapeutic insights. Cell Rep. Med. 2022, 3, 100632. [Google Scholar]
- Jacobson, J.C.; Clark, R.A.; Chung, D.H. High-Risk Neuroblastoma: A Surgical Perspective. Children 2023, 10, 388. [Google Scholar] [PubMed]
- Lee, A.C.; Chui, C.H.; Kwok, R.; Lee, K.S.; Fong, C.M.; Wong, W.H. Treatment and outcomes of high-risk neuroblastoma in Southeast Asia: A single-institution experience and review of the literature. Singap. Med. J. 2023, 64, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Streby, K.A.; Parisi, M.T.; Shulkin, B.L.; LaBarre, B.; Bagatell, R.; Diller, L.; Grupp, S.A.; Matthay, K.K.; Voss, S.D.; Yu, A.L.; et al. Impact of diagnostic and end-of-induction Curie scores with tandem high-dose chemotherapy and autologous transplants for metastatic high-risk neuroblastoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2023, 70, e30418. [Google Scholar] [CrossRef]
- Bansal, M.; Gupta, A.; Ding, H.F. MYCN and Metabolic Reprogramming in Neuroblastoma. Cancers 2022, 14, 4113. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, D.; Montemurro, L.; Raieli, S.; Lampis, S.; Pession, A.; Hrelia, P.; Tonelli, R. MYCN Impact on High-Risk Neuroblastoma: From Diagnosis and Prognosis to Targeted Treatment. Cancers 2022, 14, 4421. [Google Scholar]
- Chen, X.T.; Dai, S.Y.; Zhan, Y.; Yang, R.; Chen, D.Q.; Li, Y.; Zhou, E.Q.; Dong, R. Progress of oncolytic virotherapy for neuroblastoma. Front. Pediatr. 2022, 10, 1055729. [Google Scholar]
- Caren, H.; Kryh, H.; Nethander, M.; Sjoberg, R.M.; Trager, C.; Nilsson, S.; Abrahamsson, J.; Kogner, P.; Martinsson, T. High-risk neuroblastoma tumors with 11q-deletion display a poor prognostic, chromosome instability phenotype with later onset. Proc. Natl. Acad. Sci. USA 2010, 107, 4323–4328. [Google Scholar] [CrossRef]
- Cai, J.Y.; Pan, C.; Tang, Y.J.; Chen, J.; Ye, Q.D.; Zhou, M.; Xue, H.; Tang, J.Y. Minimal residual disease is a prognostic marker for neuroblastoma with bone marrow infiltration. Am. J. Clin. Oncol. 2012, 35, 275–278. [Google Scholar] [CrossRef]
- Pathania, A.S.; Prathipati, P.; Murakonda, S.P.; Murakonda, A.B.; Srivastava, A.; Byrareddy, S.N.; Coulter, D.W.; Gupta, S.C.; Challagundla, K.B. Immune checkpoint molecules in neuroblastoma: A clinical perspective. Semin. Cancer Biol. 2022, 86, 247–258. [Google Scholar]
- Bender, H.G.; Irwin, M.S.; Hogarty, M.D.; Castleberry, R.; Maris, J.M.; Kao, P.C.; Zhang, F.F.; Naranjo, A.; Cohn, S.L.; London, W.B. Survival of Patients With Neuroblastoma After Assignment to Reduced Therapy Because of the 12- to 18-Month Change in Age Cutoff in Children’s Oncology Group Risk Stratification. J. Clin. Oncol. 2023, 41, 3149–3159. [Google Scholar] [CrossRef] [PubMed]
- Kobushi, H.; Saida, S.; Umeda, K.; Iwai, A.; Kozuki, K.; Kubota, H.; Tanaka, K.; Obu, S.; Uchihara, Y.; Tasaka, K.; et al. High-dose carboplatin-irinotecan-temozolomide is an effective salvage chemotherapy for relapsed or refractory neuroblastoma. Pediatr. Blood Cancer 2023, 70, e30331. [Google Scholar] [CrossRef] [PubMed]
- Qualman, S.J.; Bowen, J.; Fitzgibbons, P.L.; Cohn, S.L.; Shimada, H.; Cancer Committee CoAP. Protocol for the examination of specimens from patients with neuroblastoma and related neuroblastic tumors. Arch. Pathol. Lab. Med. 2005, 129, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Spix, C.; Pastore, G.; Sankila, R.; Stiller, C.A.; Steliarova-Foucher, E. Neuroblastoma incidence and survival in European children (1978–1997): Report from the Automated Childhood Cancer Information System project. Eur. J. Cancer 2006, 42, 2081–2091. [Google Scholar] [CrossRef]
- Tsubono, Y.; Hisamichi, S. A halt to neuroblastoma screening in Japan. N. Engl. J. Med. 2004, 350, 2010–2011. [Google Scholar] [CrossRef]
- Beiske, K.; Burchill, S.A.; Cheung, I.Y.; Hiyama, E.; Seeger, R.C.; Cohn, S.L.; Pearson, A.D.; Matthay, K.K.; International neuroblastoma Risk Group Task, F. Consensus criteria for sensitive detection of minimal neuroblastoma cells in bone marrow, blood and stem cell preparations by immunocytology and QRT-PCR: Recommendations by the International Neuroblastoma Risk Group Task Force. Br. J. Cancer 2009, 100, 1627–1637. [Google Scholar]
- Cao, S.; Hu, X.; Ren, S.; Wang, Y.; Shao, Y.; Wu, K.; Yang, Z.; Yang, W.; He, G.; Li, X. The biological role and immunotherapy of gangliosides and GD3 synthase in cancers. Front. Cell Dev. Biol. 2023, 11, 1076862. [Google Scholar]
- Schnaar, R.L. Gangliosides as Siglec ligands. Glycoconj. J. 2023, 40, 159–167. [Google Scholar] [CrossRef]
- Molenaar, J.J.; Koster, J.; Zwijnenburg, D.A.; van Sluis, P.; Valentijn, L.J.; van der Ploeg, I.; Hamdi, M.; van Nes, J.; Westerman, B.A.; van Arkel, J.; et al. Sequencing of neuroblastoma identifies chromothripsis and defects in neuritogenesis genes. Nature 2012, 483, 589–593. [Google Scholar] [CrossRef]
- Qiu, B.; Matthay, K.K. Advancing therapy for neuroblastoma. Nat. Rev. Clin. Oncol. 2022, 19, 515–533. [Google Scholar] [PubMed]
- Ambros, P.F.; Ambros, I.M.; Brodeur, G.M.; Haber, M.; Khan, J.; Nakagawara, A.; Schleiermacher, G.; Speleman, F.; Spitz, R.; London, W.B.; et al. International consensus for neuroblastoma molecular diagnostics: Report from the International Neuroblastoma Risk Group (INRG) Biology Committee. Br. J. Cancer 2009, 100, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Burchill, S.A.; Beiske, K.; Shimada, H.; Ambros, P.F.; Seeger, R.; Tytgat, G.A.; Brock, P.R.; Haber, M.; Park, J.R.; Berthold, F. Recommendations for the standardization of bone marrow disease assessment and reporting in children with neuroblastoma on behalf of the International Neuroblastoma Response Criteria Bone Marrow Working Group. Cancer 2017, 123, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Littooij, A.S.; de Keizer, B. Imaging in neuroblastoma. Pediatr. Radiol. 2023, 53, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, K.I.; Treis, D.; Johnsen, J.I. Neuroblastoma Heterogeneity, Plasticity, and Emerging Therapies. Curr. Oncol. Rep. 2022, 24, 1053–1062. [Google Scholar]
- Zanotti, S.; Decaesteker, B.; Vanhauwaert, S.; De Wilde, B.; De Vos, W.H.; Speleman, F. Cellular senescence in neuroblastoma. Br. J. Cancer 2022, 126, 1529–1538. [Google Scholar]
- Li, C.H.; Chan, M.H.; Chang, Y.C.; Hsiao, M. Gold Nanoparticles as a Biosensor for Cancer Biomarker Determination. Molecules 2023, 28, 364. [Google Scholar]
- Bai, X.; Wang, Y.; Song, Z.; Feng, Y.; Chen, Y.; Zhang, D.; Feng, L. The Basic Properties of Gold Nanoparticles and their Applications in Tumor Diagnosis and Treatment. Int. J. Mol. Sci. 2020, 21, 2480. [Google Scholar] [CrossRef]
- Mathaweesansurn, A.; Vittayakorn, N.; Detsri, E. Highly Sensitive and Selective Colorimetric Sensor of Mercury (II) based on Layer-by-Layer Deposition of Gold/Silver Bimetallic Nanoparticles. Molecules 2020, 25, 4443. [Google Scholar] [CrossRef]
- Liu, X.; Wang, Q.; Chen, J.; Chen, X.; Yang, W. Ultrasensitive electrochemiluminescence biosensor for the detection of tumor exosomes based on peptide recognition and luminol-AuNPs@g-C(3)N(4) nanoprobe signal amplification. Talanta 2021, 221, 121379. [Google Scholar] [CrossRef]
- Hu, K.; Cheng, J.; Wang, K.; Zhao, Y.; Liu, Y.; Yang, H.; Zhang, Z. Sensitive electrochemical immunosensor for CYFRA21–1 detection based on AuNPs@MoS(2)@Ti(3)C(2)T(x) composites. Talanta 2022, 238, 122987. [Google Scholar] [CrossRef] [PubMed]
- Okyem, S.; Awotunde, O.; Ogunlusi, T.; Riley, M.B.; Driskell, J.D. Probing the Mechanism of Antibody-Triggered Aggregation of Gold Nanoparticles. Langmuir 2021, 37, 2993–3000. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, S.; Salimi, A.; Hamd-Ghadareh, S.; Fathi, F.; Soleimani, F. A FRET immunosensor for sensitive detection of CA 15–3 tumor marker in human serum sample and breast cancer cells using antibody functionalized luminescent carbon-dots and AuNPs-dendrimer aptamer as donor-acceptor pair. Anal. Biochem. 2018, 557, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Dong, J.; Zhao, Q.; Ying, Y.; Zhang, L.; Zou, J.; Zhao, S.; Wang, J.; Zhao, Y.; Jiang, S. Gold nanoparticle-mediated delivery of paclitaxel and nucleic acids for cancer therapy (Review). Mol. Med. Rep. 2020, 22, 4475–4484. [Google Scholar] [CrossRef] [PubMed]
- Lira, A.L.; Ferreira, R.S.; Torquato, R.J.S.; Zhao, H.; Oliva, M.L.V.; Hassan, S.A.; Schuck, P.; Sousa, A.A. Binding kinetics of ultrasmall gold nanoparticles with proteins. Nanoscale 2018, 10, 3235–3244. [Google Scholar] [CrossRef] [PubMed]
- Mirau, P.A.; Smith, J.E.; Chavez, J.L.; Hagen, J.A.; Kelley-Loughnane, N.; Naik, R. Structured DNA Aptamer Interactions with Gold Nanoparticles. Langmuir 2018, 34, 2139–2146. [Google Scholar] [CrossRef]
- Kalyane, D.; Raval, N.; Maheshwari, R.; Tambe, V.; Kalia, K.; Tekade, R.K. Employment of enhanced permeability and retention effect (EPR): Nanoparticle-based precision tools for targeting of therapeutic and diagnostic agent in cancer. Mater. Sci. Eng. C. Mater. Biol. Appl. 2019, 98, 1252–1276. [Google Scholar]
- Andrade, L.M.; Costa, G.M.J. Insights into Gold Nanoparticles Possibilities for Diagnosis and Treatment of the Head and Neck Upper Aerodigestive Tract Cancers. Cancers 2023, 15, 2080. [Google Scholar]
- Wu, S.; Liu, J.; Tian, Z.; Cai, Y.; Ye, Y.; Yuan, Q.; Liang, C. Highly Dispersed Ultrafine Pt Nanoparticles on Reduced Graphene Oxide Nanosheets: In Situ Sacrificial Template Synthesis and Superior Electrocatalytic Performance for Methanol Oxidation. ACS Appl. Mater. Interfaces 2015, 7, 22935–22940. [Google Scholar] [CrossRef]
- Eswaran, M.; Tsai, P.C.; Wu, M.T.; Ponnusamy, V.K. Novel nano-engineered environmental sensor based on polymelamine/graphitic-carbon nitride nanohybrid material for sensitive and simultaneous monitoring of toxic heavy metals. J. Hazard Mater. 2021, 418, 126267. [Google Scholar] [CrossRef]
- Imanzadeh, H.; Sefid-Sefidehkhan, Y.; Afshary, H.; Afruz, A.; Amiri, M. Nanomaterial-based electrochemical sensors for detection of amino acids. J. Pharm. Biomed. Anal. 2023, 230, 115390. [Google Scholar]
- Pang, Y.H.; Yang, Q.Y.; Jiang, R.; Wang, Y.Y.; Shen, X.F. A stack-up electrochemical device based on metal-organic framework modified carbon paper for ultra-trace lead and cadmium ions detection. Food Chem. 2023, 398, 133822. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Fan, S.; Webb, J.A.; Ma, Y.; Goyette, J.; Chen, X.; Gaus, K.; Tilley, R.D.; Gooding, J.J. Electrochemical fluorescence switching of enhanced green fluorescent protein. Biosens. Bioelectron. 2023, 237, 115467. [Google Scholar]
- Corallo, D.; Dalla Vecchia, M.; Lazic, D.; Taschner-Mandl, S.; Biffi, A.; Aveic, S. The molecular basis of tumor metastasis and current approaches to decode targeted migration-promoting events in pediatric neuroblastoma. Biochem. Pharmacol. 2023, 215, 115696. [Google Scholar]
- Feng, L.; Li, S.; Wang, C.; Yang, J. Current Status and Future Perspective on Molecular Imaging and Treatment of Neuroblastoma. Semin. Nucl. Med. 2023, 53, 517–529. [Google Scholar]
- Larrosa, C.; Mora, J.; Cheung, N.K. Global Impact of Monoclonal Antibodies (mAbs) in Children: A Focus on Anti-GD2. Cancers 2023, 15, 3729. [Google Scholar]
- Sardarabadi, P.; Kojabad, A.A.; Jafari, D.; Liu, C.H. Liquid Biopsy-Based Biosensors for MRD Detection and Treatment Monitoring in Non-Small Cell Lung Cancer (NSCLC). Biosensors 2021, 11, 394. [Google Scholar]
- Wang, L.; Xie, H.; Zhou, X.; Lin, Y.; Qin, Y.; Yang, J.; Zhao, J.; Li, G. An electrochemical biosensor to identify the phenotype of aggressive breast cancer cells. Chem. Commun. 2023, 59, 3890–3893. [Google Scholar] [CrossRef]
- Fan, Y.; Shi, S.; Ma, J.; Guo, Y. A paper-based electrochemical immunosensor with reduced graphene oxide/thionine/gold nanoparticles nanocomposites modification for the detection of cancer antigen 125. Biosens. Bioelectron. 2019, 135, 1–7. [Google Scholar] [CrossRef]
- Liu, S.; Yin, W.; Lin, Y.; Huang, S.; Xue, S.; Sun, G.; Wang, C. Metastasis pattern and prognosis in children with neuroblastoma. World J. Surg. Oncol. 2023, 21, 130. [Google Scholar] [CrossRef]
- Depuydt, P.; Boeva, V.; Hocking, T.D.; Cannoodt, R.; Ambros, I.M.; Ambros, P.F.; Asgharzadeh, S.; Attiyeh, E.F.; Combaret, V.; Defferrari, R.; et al. Genomic Amplifications and Distal 6q Loss. Novel Markers for Poor Survival in High-risk Neuroblastoma Patients. J. Natl. Cancer Inst. 2018, 110, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.; Hu, C.; He, B.; Bai, Y.; He, F.; Li, S.; Tan, C.S. Functionalized GD2 Electrochemical Immunosensor to Diagnose Minimum Residual Disease of Bone Marrow in Neuroblastoma Effectively. Biosensors 2023, 13, 920. https://doi.org/10.3390/bios13100920
Chen C, Hu C, He B, Bai Y, He F, Li S, Tan CS. Functionalized GD2 Electrochemical Immunosensor to Diagnose Minimum Residual Disease of Bone Marrow in Neuroblastoma Effectively. Biosensors. 2023; 13(10):920. https://doi.org/10.3390/bios13100920
Chicago/Turabian StyleChen, Chong, Chang Hu, Baixun He, Yongchang Bai, Feng He, Shuang Li, and Cherie S. Tan. 2023. "Functionalized GD2 Electrochemical Immunosensor to Diagnose Minimum Residual Disease of Bone Marrow in Neuroblastoma Effectively" Biosensors 13, no. 10: 920. https://doi.org/10.3390/bios13100920
APA StyleChen, C., Hu, C., He, B., Bai, Y., He, F., Li, S., & Tan, C. S. (2023). Functionalized GD2 Electrochemical Immunosensor to Diagnose Minimum Residual Disease of Bone Marrow in Neuroblastoma Effectively. Biosensors, 13(10), 920. https://doi.org/10.3390/bios13100920