
Influence of Implant Surface Topography on Primary Stability in a Standardized Osteoporosis Rabbit Model Study


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
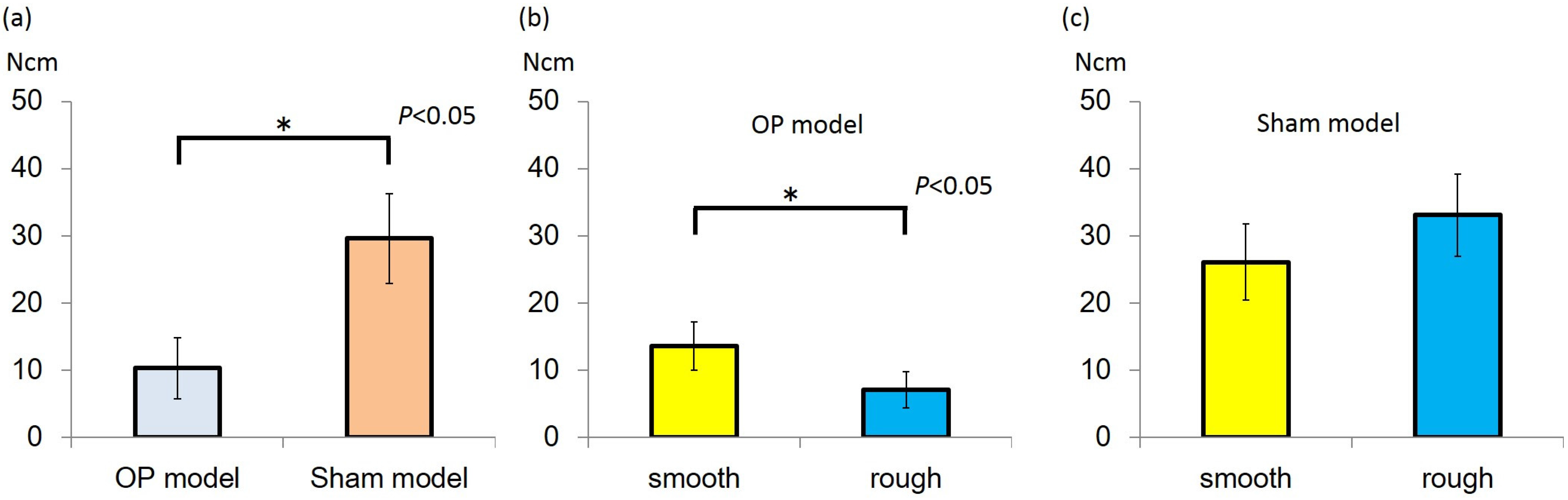
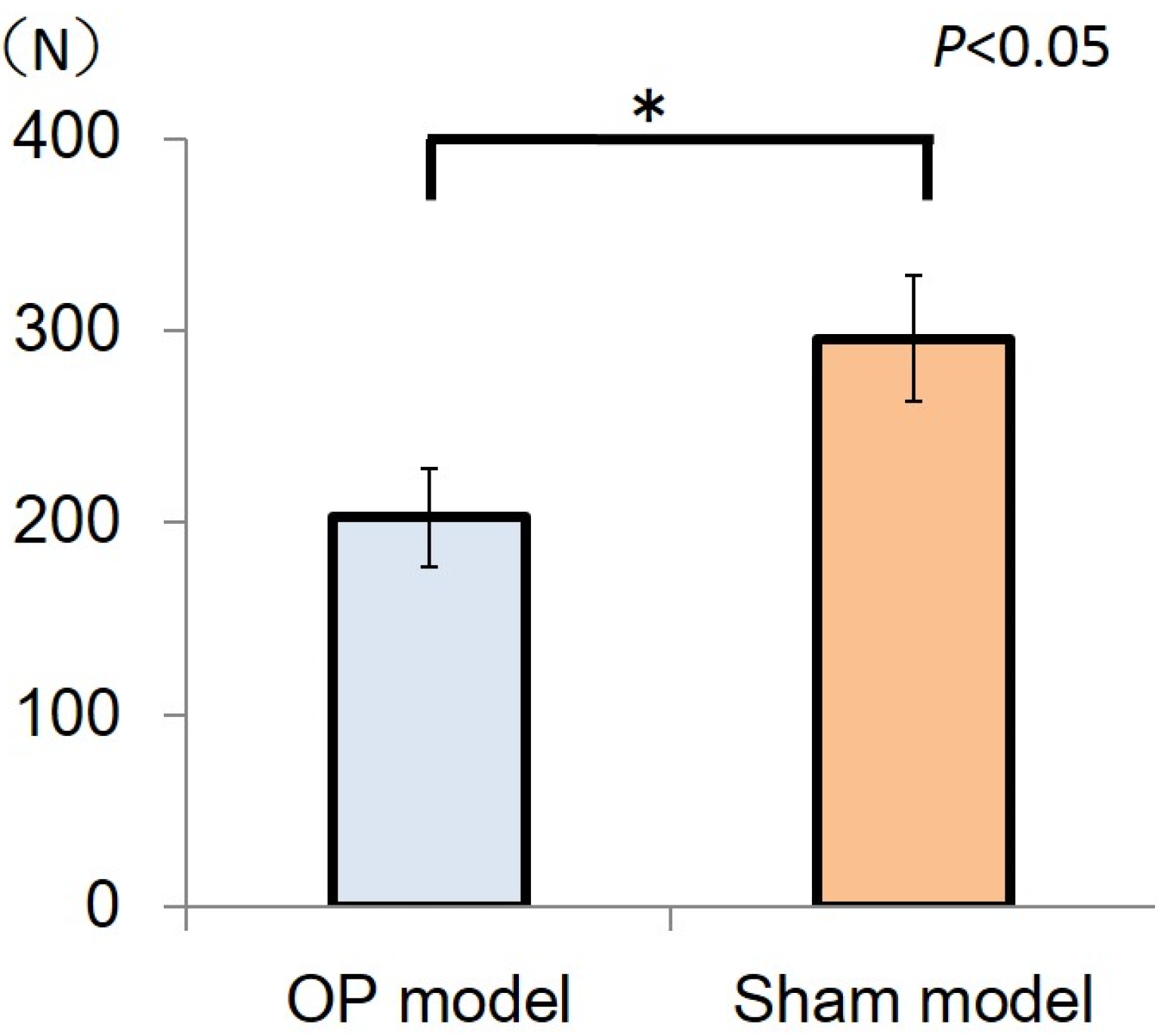
2.1.1. Insertion Torque

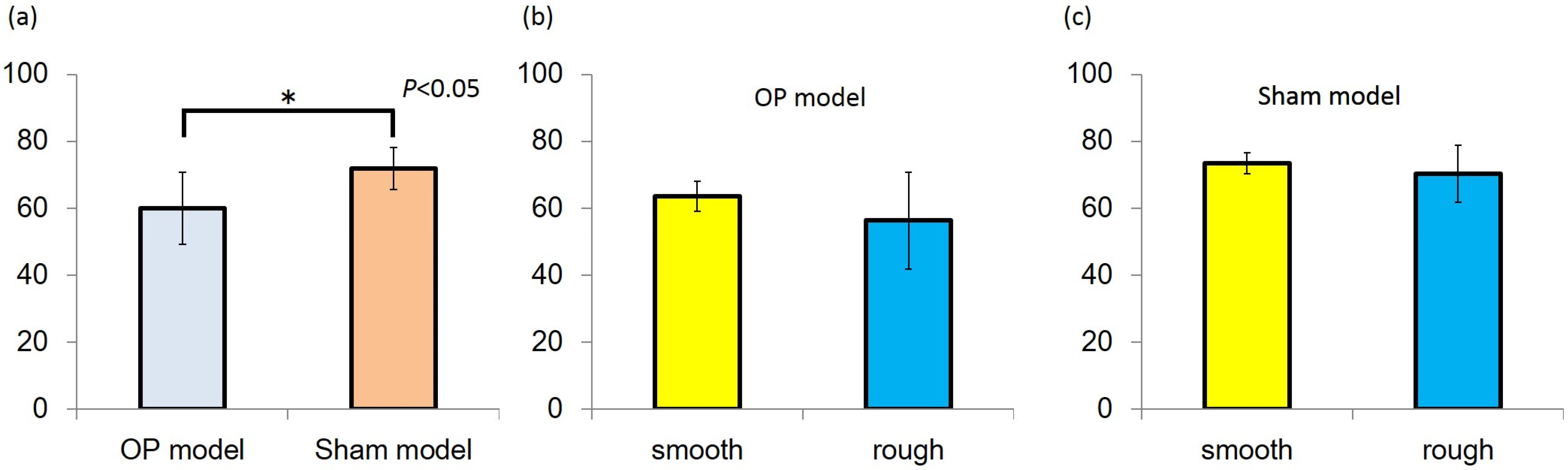
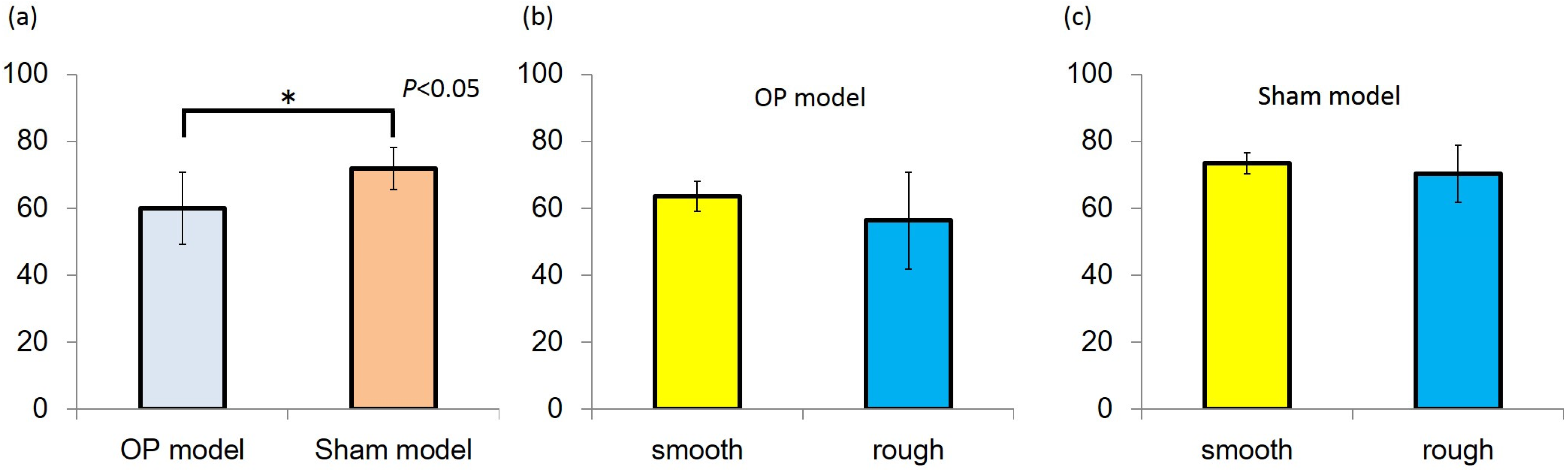
2.1.2. Resonance Frequency Analysis
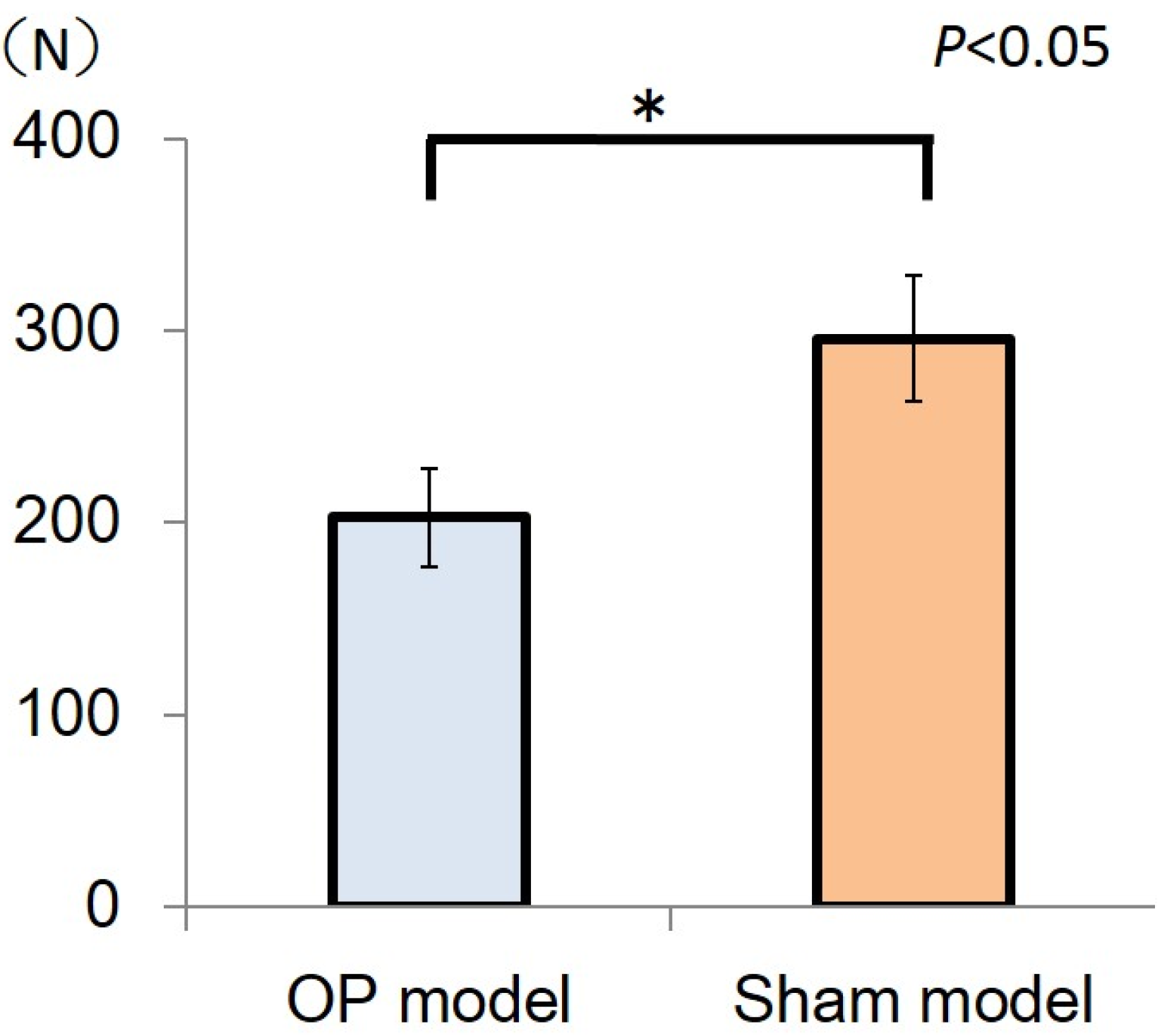
2.1.3. Mechanical Strength of Bone
2.2. Discussion
3. Experimental Section
3.1. Ethics
3.2. Study Design and Animals

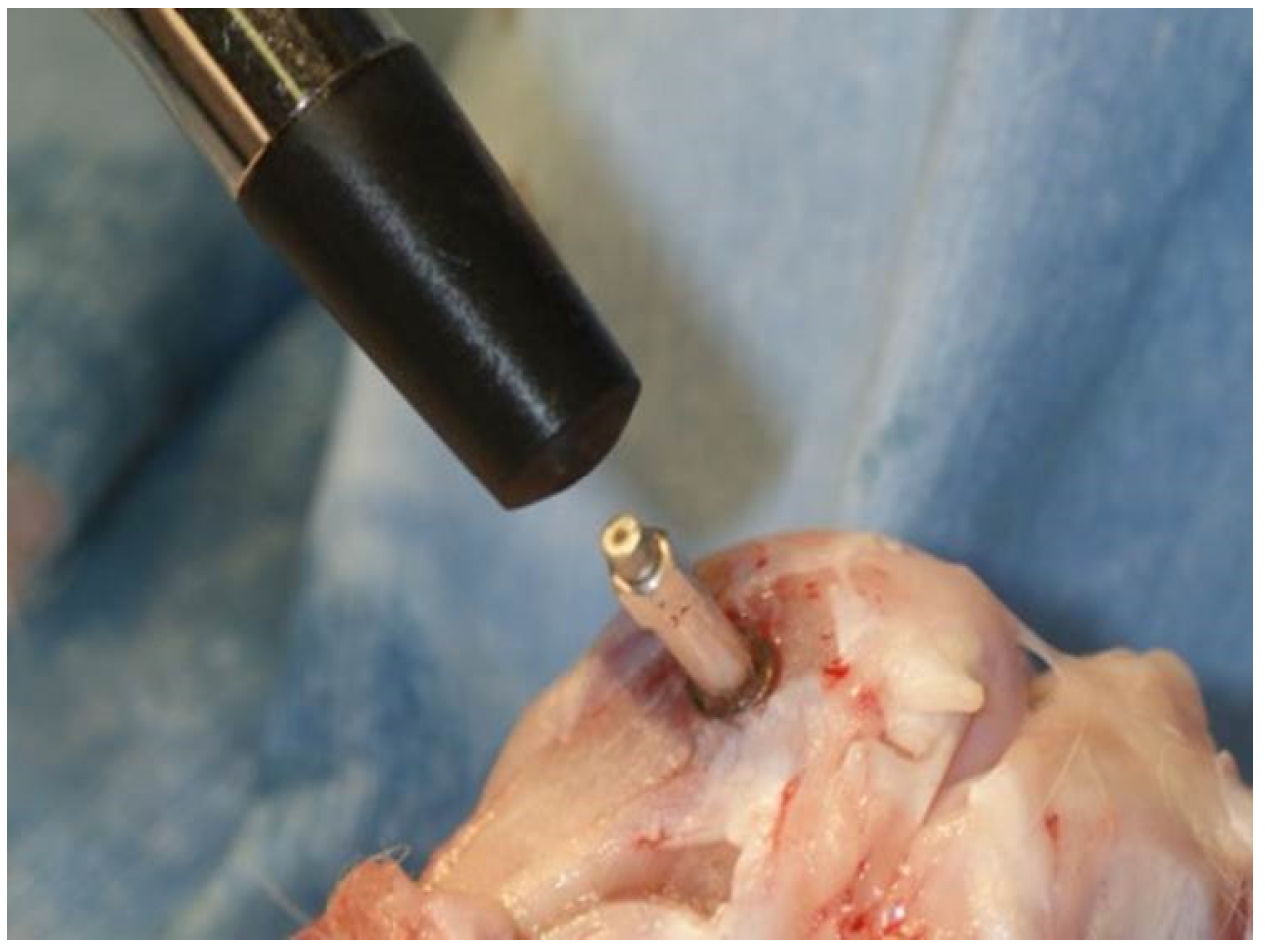
3.3. Measurement of Primary Stability
3.4. Analysis of Mechanical Strength of Bone
3.5. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Östman, P.O.; Hellman, M.; Wendelhag, I.; Sennerby, L. Resonance frequency analysis measurements of implants at placement surgery. Int. J. Prosthodont. 2006, 19, 77–83. [Google Scholar]
- Suito, H.; Tomotake, Y.; Watanabe, M.; Nagao, D.; Ishida, Y.; Ichikawa, T. Survival of immediate implant restoration: A retrospective study through 9-year-observation. J. Prosthodont. Res. 2011, 55, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Johansson, B.; Bäckm, T.; Hirsch, J.M. Cutting torque measurements in conjunction with implant placement in grafted and nongrafted maxillas as an objective evaluation of bone density: a possible method for identifying early implant failures? Clin. Implant Dent. Relat. Res. 2004, 6, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Iezzi, G.; Scarano, A.; Di Stefano, D.; Arosio, P.; Doi, K.; Ricci, L.; Piattelli, A.; Perrotti, V. Correlation between the bone density recorded by a computerized implant motor and by a histomorphometric analysis: A preliminary in vitro study on bovine ribs. Clin. Implant Dent. Relat. Res. 2015, 17, e35–e44. [Google Scholar] [CrossRef] [PubMed]
- Shibli, J.A.; Aguiar, K.C.; Melo, L.; d’Avila, S.; Zenóbio, E.G.; Faveri, M.; Iezzi, G.; Piattelli, A. Histological comparison between implants retrieved from patients with and without osteoporosis. Int. J. Oral Maxillofac. Surg. 2008, 37, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.; Hujoel, P.P.; Becker, B.E.; Willingham, H. Osteoporosis and implant failure: An exploratory case-control study. J. Periodontol. 2000, 71, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Johansson, C.; Lundgren, A.K.; Sul, Y.; Gottlow, J. Experimental studies on oxidezed implants. A histomorphometrical and biomechanical analysis. Appl. Osseointegration Res. 2000, 1, 21–24. [Google Scholar]
- Glauser, R.; Portmann, M.; Ruhstaller, P.; Lundgren, A.K.; Hämmerle, C.; Gottlow, J. Stability measurements of immediately loaded machined and oxidized implants in the posterior maxilla. A comparative clinical study using resonance frequency analysis. Appl. Osseontegration Res. 2001, 2, 27–29. [Google Scholar]
- Turner, R.T.; Maran, A.; Lotinun, S.; Hefferan, T.; Evans, G.L.; Zhang, M.; Sibonga, J.D. Animal models for osteoporosis. Rev. Endocr. Metab. Disord. 2001, 2, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, M.; Scarano, A.; Paolantonio, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Bone response to machined and resorbable blast material titanium implants: an experimental study in rabbits. J. Oral Implantol. 2002, 28, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Castañeda, S.; Largo, R.; Calvo, E.; Rodríguez-Salvanés, F.; Marcos, M.E.; Díaz-Curiel, M.; Herrero-Beaumont, G. Bone mineral measurements of subchondral and trabecular bone in healthy and osteoporotic rabbits. Skeletal Radiol. 2006, 35, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Doi, K.; Kubo, T.; Takeshita, R.; Kajihara, S.; Kato, S.; Kawazoe, Y.; Shiba, T.; Akagawa, Y. Inorganic polyphosphate adsorbed onto hydroxyapatite for guided bone regeneration: An animal study. Dent. Mater. J. 2014, 33, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Jemt, T.; Lekholm, U. Implant treatment in edentulous maxillae: A 5-year follow-up report on patients with different degrees of jaw resorption. Int. J. Oral Maxillofac. Implants 1995, 10, 303–311. [Google Scholar] [PubMed]
- Scarano, A.; Degidi, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Correlation between implant stability quotient and bone-implant contact: A retrospective histological and histomorphometrical study of seven titanium implants retrieved from humans. Clin. Implant Dent. Relat. Res. 2006, 8, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Castañeda, S.; Calvo, E.; Largo, R.; González-González, R.; de la Piedra, C.; Díaz-Curiel, M.; Herrero-Beaumont, G. Characterization of a new experimental model of osteoporosis in rabbits. J. Bone Miner. Metab. 2008, 26, 53–59. [Google Scholar] [CrossRef]
- Almagro, M.I.; Roman-Blas, J.A.; Bellido, M.; Castañeda, S.; Cortez, R.; Herrero-Beaumont, G. PTH [1-34] enhances bone response around titanium implants in a rabbit model of osteoporosis. Clin. Oral Implants Res. 2013, 24, 1027–1034. [Google Scholar] [PubMed]
- Da Cunha, H.A.; Francischone, C.E.; Filho, H.N.; de Oliveira, R.C. A comparison between cutting torque and resonance frequency in the assessment of primary stability and final torque capacity of standard and TiUnite single-tooth implants under immediate loading. Int. J. Oral Maxillofac. Implants 2004, 19, 578–585. [Google Scholar] [PubMed]
- Turkyilmaz, I.; Sennerby, L.; Yilmaz, B.; Bilecenoglu, B.; Ozbek, E.N. Influence of defect depth on resonance frequency analysis and insertion torque values for implants placed in fresh extraction sockets: A human cadaver study. Clin. Implant Dent. Relat. Res. 2009, 11, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Friberg, B.; Sennerby, L.; Linden, B.; Gröndahl, K.; Lekholm, U. Stability measurements of one-stage Brånemark implants during healing in mandibles. A clinical resonance frequency analysis study. Int. J. Oral Maxillofac. Surg. 1999, 28, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawas, B.; Wagner, W.; Grötz, K.A. Insertion torque and resonance frequency analysis of dental implant systems in an animal model with loaded implants. Int. J. Oral Maxillofac. Implants 2006, 21, 726–732. [Google Scholar] [PubMed]
- Degidi, M.; Piattelli, A.; Shibli, J.A.; Perrotti, V.; Iezzi, G. Bone formation around immediately loaded and submerged dental implants with a modified sandblasted and acid-etched surface after 4 and 8 weeks: A human histologic and histomorphometric analysis. Int. J. Oral Maxillofac. Implants 2009, 24, 896–901. [Google Scholar] [PubMed]
- Wennerberg, A.; Albrektsson, T. On implant surfaces: A review of current knowledge and opinions. Int. J. Oral Maxillofac Implants 2010, 25, 63–74. [Google Scholar] [PubMed]
- Doi, K.; Kajihara, S.; Morita, K.; Makihara, Y.; Okada, S.; Akagawa, Y. The influence of fixation in formalin on the measurement of stability of implants using resonance frequency analysis and Periotest M®: A study in a dog. Br. J. Oral Maxillofac. Surg. 2014, 52, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Doi, K.; Oue, H.; Kajihara, S.; Hayashi, K.; Akagawa, Y. Influence of formalin fixation on the implant stability quotient and mechanical characteristics of bone. Br. J. Oral Maxillofac. Surg. 2013, 51, 550–554. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oue, H.; Doi, K.; Oki, Y.; Makihara, Y.; Kubo, T.; Perrotti, V.; Piattelli, A.; Akagawa, Y.; Tsuga, K. Influence of Implant Surface Topography on Primary Stability in a Standardized Osteoporosis Rabbit Model Study. J. Funct. Biomater. 2015, 6, 143-152. https://doi.org/10.3390/jfb6010143
Oue H, Doi K, Oki Y, Makihara Y, Kubo T, Perrotti V, Piattelli A, Akagawa Y, Tsuga K. Influence of Implant Surface Topography on Primary Stability in a Standardized Osteoporosis Rabbit Model Study. Journal of Functional Biomaterials. 2015; 6(1):143-152. https://doi.org/10.3390/jfb6010143
Chicago/Turabian StyleOue, Hiroshi, Kazuya Doi, Yoshifumi Oki, Yusuke Makihara, Takayasu Kubo, Vittoria Perrotti, Adriano Piattelli, Yasumasa Akagawa, and Kazuhiro Tsuga. 2015. "Influence of Implant Surface Topography on Primary Stability in a Standardized Osteoporosis Rabbit Model Study" Journal of Functional Biomaterials 6, no. 1: 143-152. https://doi.org/10.3390/jfb6010143
APA StyleOue, H., Doi, K., Oki, Y., Makihara, Y., Kubo, T., Perrotti, V., Piattelli, A., Akagawa, Y., & Tsuga, K. (2015). Influence of Implant Surface Topography on Primary Stability in a Standardized Osteoporosis Rabbit Model Study. Journal of Functional Biomaterials, 6(1), 143-152. https://doi.org/10.3390/jfb6010143