Survival of Patients Treated with Antibiotics and Immunotherapy for Cancer: A Systematic Review and Meta-Analysis

 , , ,
, , , 

Abstract
1. Introduction
2. Experimental Section
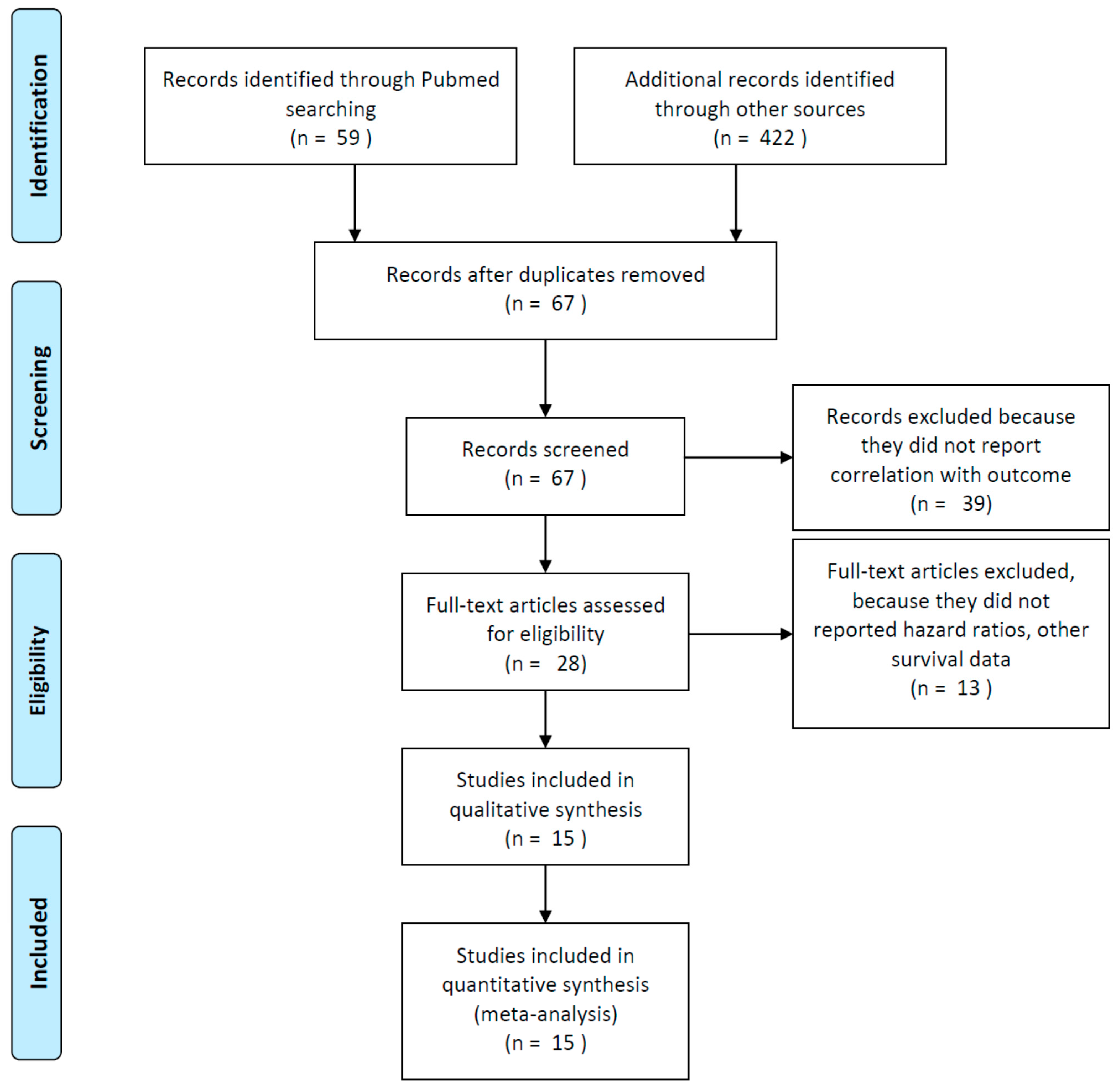
2.1. Search Strategy and Inclusion Criteria
2.2. Data Extraction
2.3. Statistical Analysis
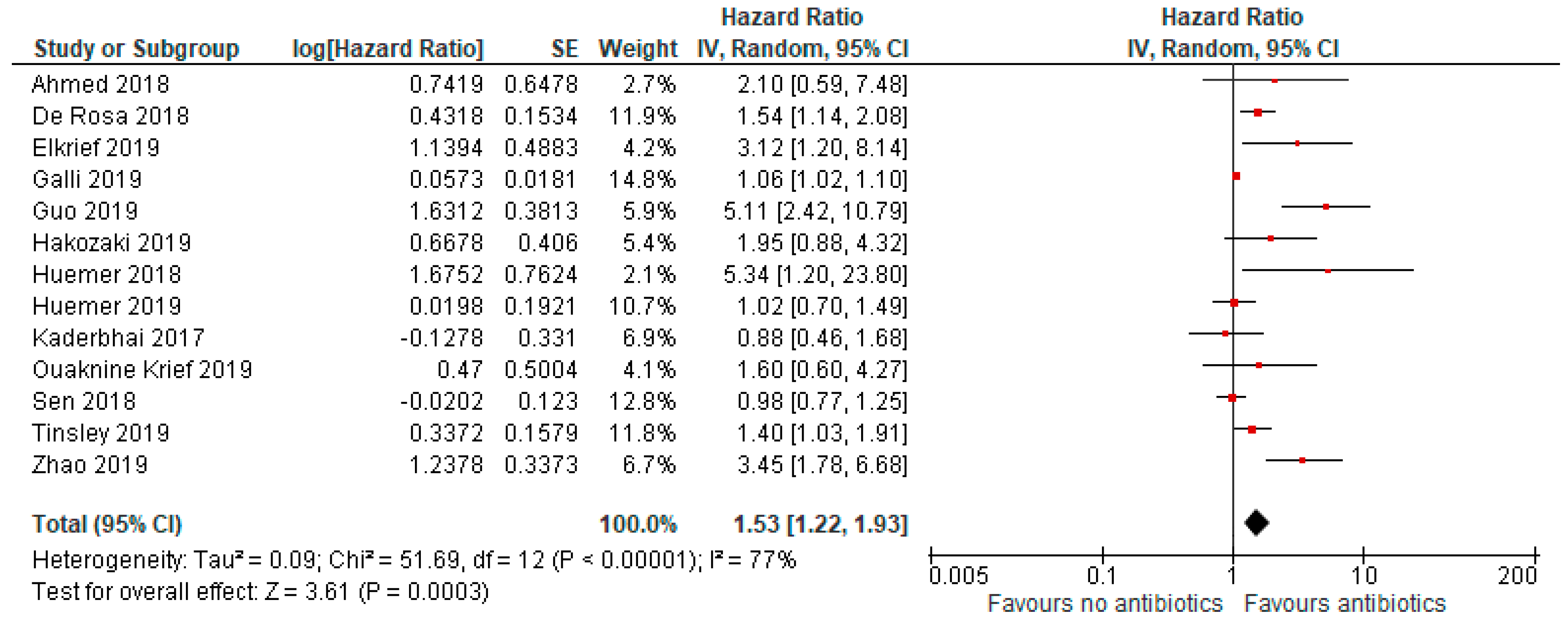
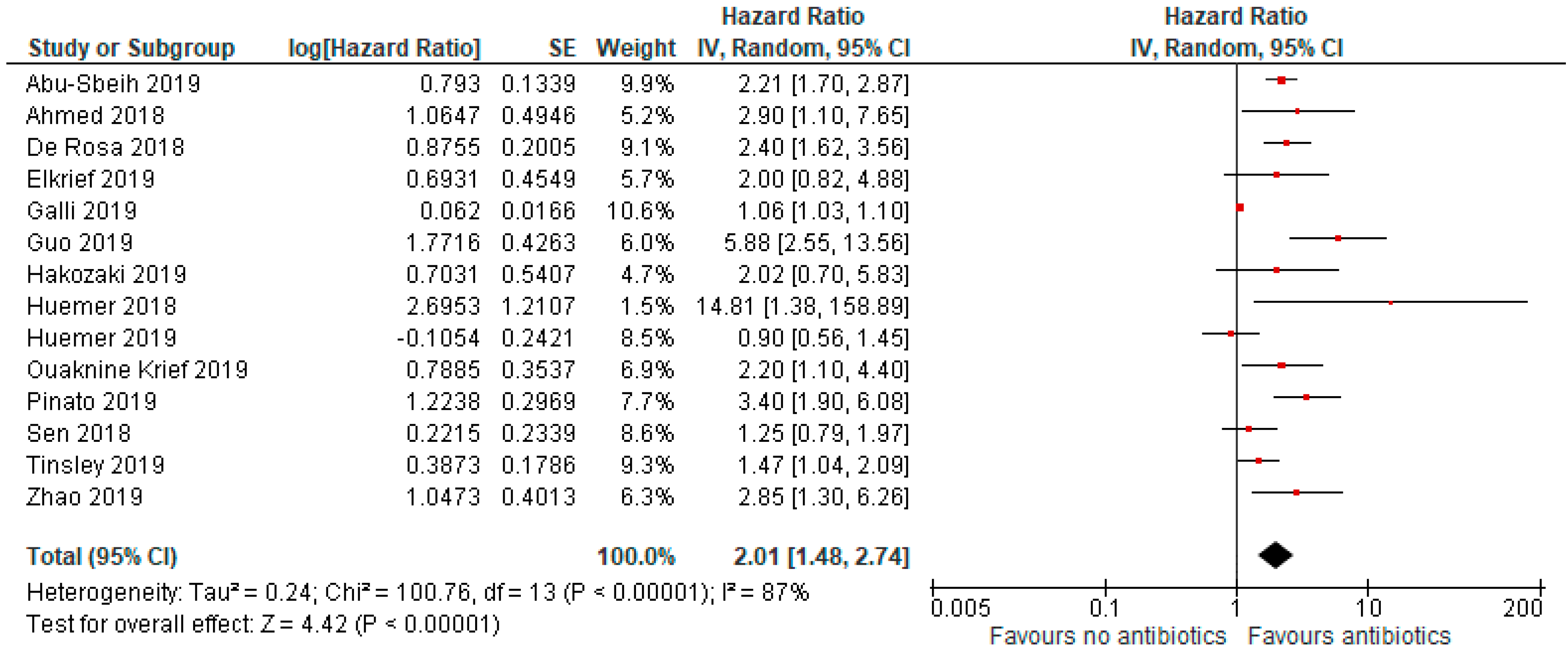
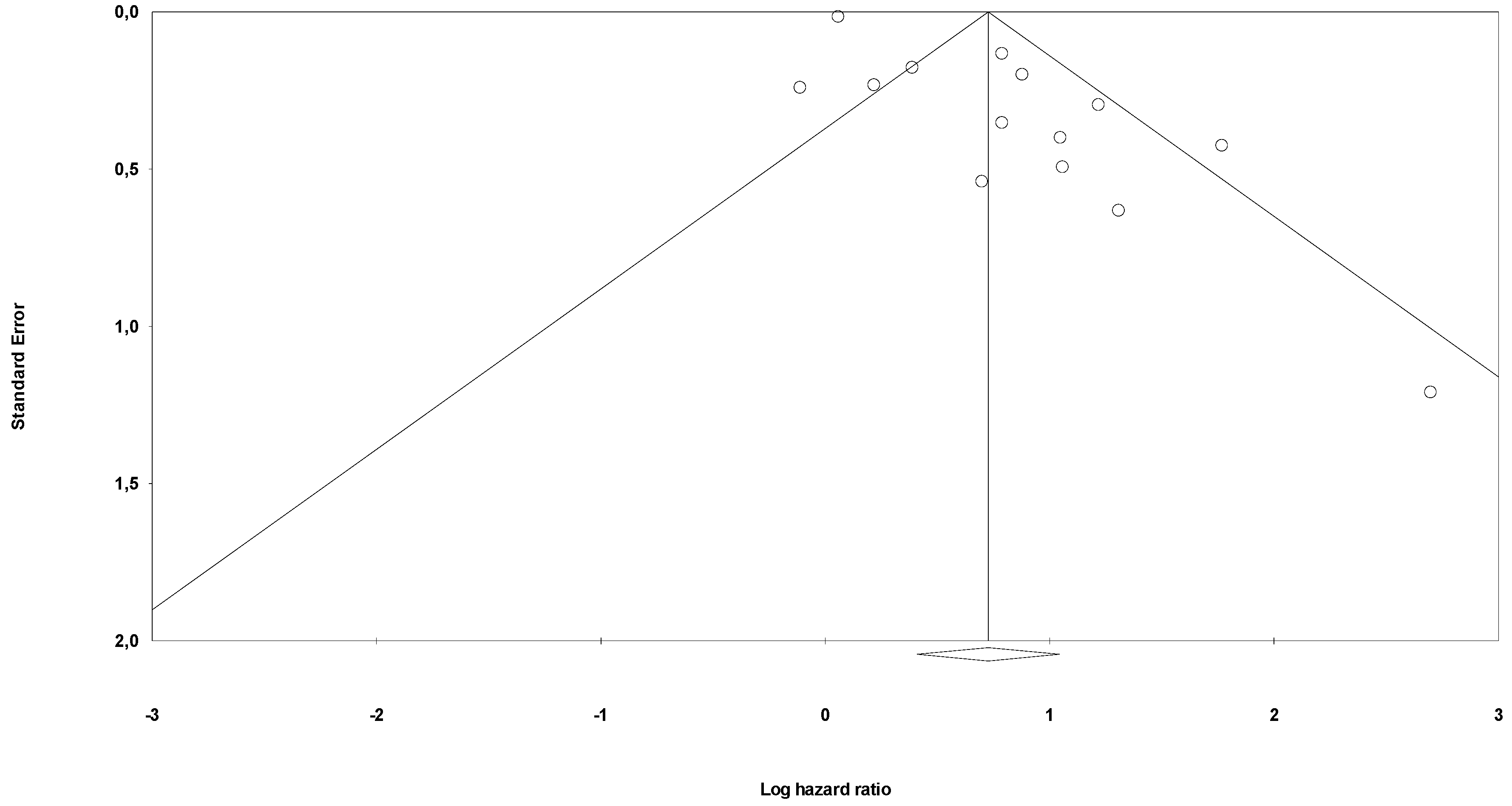
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Gori, S.; Inno, A.; Belluomini, L.; Bocus, P.; Bisoffi, Z.; Russo, A.; Arcaro, G. Gut microbiota and cancer: How gut microbiota modulates activity, efficacy and toxicity of antitumoral therapy. Crit. Rev. Oncol. 2019, 143, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Sivan, A.; Corrales, L.; Hubert, N.; Williams, J.B.; Aquino-Michaels, K.; Earley, Z.M.; Benyamin, F.W.; Lei, Y.M.; Jabri, B.; Alegre, M.-L.; et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 2015, 350, 1084–1089. [Google Scholar] [CrossRef]
- DeRosa, L.; Hellmann, M.; Spaziano, M.; Halpenny, D.; Fidelle, M.; Rizvi, H.; Long, N.; Plodkowski, A.; Arbour, K.; Chaft, J.; et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small-cell lung cancer. Ann. Oncol. 2018, 29, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Galli, G.; Triulzi, T.; Proto, C.; Signorelli, D.; Imbimbo, M.; Poggi, M.; Fucà, G.; Ganzinelli, M.; Vitali, M.; Palmieri, D.; et al. Association between antibiotic-immunotherapy exposure ratio and outcome in metastatic non small cell lung cancer. Lung Cancer 2019, 132, 72–78. [Google Scholar] [CrossRef]
- Tinsley, N.; Zhou, C.; Tan, G.; Rack, S.; Lorigan, P.C.; Blackhall, F.; Krebs, M.; Carter, L.; Thistlethwaite, F.; Graham, D.; et al. Cumulative Antibiotic Use Significantly Decreases Efficacy of Checkpoint Inhibitors in Patients with Advanced Cancer. Oncologist 2019, 25, 55–63. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality if Nonrandomizes Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 29 December 2019).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, U.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Abu-Sbeih, H.; Herrera, L.N.; Tang, T.; Altan, M.; Chaftari, A.-M.; Okhuysen, P.C.; Jenq, R.R.; Wang, Y. Impact of antibiotic therapy on the development and response to treatment of immune checkpoint inhibitor-mediated diarrhea and colitis. J. Immunother. Cancer 2019, 7, 242. [Google Scholar] [CrossRef]
- Ahmed, J.; Kumar, A.; Parikh, K.; Anwar, A.; Knoll, B.M.; Puccio, C.; Chun, H.; Fanucchi, M.; Lim, S.H. Use of broad-spectrum antibiotics impacts outcome in patients treated with immune checkpoint inhibitors. OncoImmunology 2018, 7, e1507670–e1507676. [Google Scholar] [CrossRef]
- Elkrief, A.; El Raichani, L.; Richard, C.; Messaoudene, M.; Belkaid, W.; Malo, J.; Belanger, K.; Miller, W.; Jamal, R.; Letarte, N.; et al. Antibiotics are associated with decreased progression-free survival of advanced melanoma patients treated with immune checkpoint inhibitors. OncoImmunology 2019, 8, e1568812–e1568816. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.-C.; Lin, C.-C.; Lin, C.-Y.; Hsieh, M.-S.; Kuo, H.-Y.; Lien, M.-Y.; Shao, Y.-Y.; Huang, T.-C.; Hsu, C.-H. Neutrophil-to-lymphocyte Ratio and Use of Antibiotics Associated with Prognosis in Esophageal Squamous Cell Carcinoma Patients Receiving Immune Checkpoint Inhibitors. Anticancer Res. 2019, 39, 5675–5682. [Google Scholar] [CrossRef] [PubMed]
- Hakozaki, T.; Okuma, Y.; Omori, M.; Hosomi, Y. Impact of prior antibiotic use on the efficacy of nivolumab for non-small cell lung cancer. Oncol. Lett. 2019, 17, 2946–2952. [Google Scholar] [CrossRef] [PubMed]
- Huemer, F.; Lang, D.; Westphal, T.; Gampenrieder, S.P.; Hutarew, G.; Weiss, L.; Hackl, H.; Lamprecht, B.; Rinnerthaler, G.; Greil, R.; et al. Baseline Absolute Lymphocyte Count and ECOG Performance Score Are Associated with Survival in Advanced Non-Small Cell Lung Cancer Undergoing PD-1/PD-L1 Blockade. J. Clin. Med. 2019, 8, 1014. [Google Scholar] [CrossRef]
- Huemer, F.; Rinnerthaler, G.; Westphal, T.; Hackl, H.; Hutarew, G.; Gampenrieder, S.P.; Weiss, L.; Greil, R. Impact of antibiotic treatment on immune-checkpoint blockade efficacy in advanced non-squamous non-small cell lung cancer. Oncotarget 2018, 9, 16512–16520. [Google Scholar] [CrossRef]
- Kaderbhai, C.; Richard, C.; Fumet, J.D.; Aarnink, A.; Foucher, P.; Coudert, B.; Favier, L.; Lagrange, A.; Limagne, E.; Boidot, R.; et al. Antibiotic Use Does Not Appear to Influence Response to Nivolumab. Anticancer Res. 2017, 37, 3195–3200. [Google Scholar] [CrossRef]
- Krief, J.O.; De Tauriers, P.H.; Duménil, C.; Neveux, N.; Dumoulin, J.; Giraud, V.; Labrune, S.; Tisserand, J.; Julie, C.; Emile, J.-F.; et al. Role of antibiotic use, plasma citrulline and blood microbiome in advanced non-small cell lung cancer patients treated with nivolumab. J. Immunother. Cancer 2019, 7, 176. [Google Scholar] [CrossRef]
- Pinato, D.J.; Howlett, S.; Ottaviani, D.; Urus, H.; Patel, A.; Mineo, T.; Brock, C.; Power, D.; Hatcher, O.; Falconer, A.; et al. Association of Prior Antibiotic Treatment with Survival and Response to Immune Checkpoint Inhibitor Therapy in Patients With Cancer. JAMA Oncol. 2019, 5, 1774. [Google Scholar] [CrossRef]
- Sen, S.; Pestana, R.C.; Hess, K.; Viola, G.; Subbiah, V. Impact of antibiotic use on survival in patients with advanced cancers treated on immune checkpoint inhibitor phase I clinical trials. Ann. Oncol. 2018, 29, 2396–2398. [Google Scholar] [CrossRef]
- Zhao, S.; Gao, G.; Li, W.; Li, X.; Zhao, C.; Jiang, T.; Jia, Y.; He, Y.; Li, A.; Su, C.; et al. Antibiotics are associated with attenuated efficacy of anti-PD-1/PD-L1 therapies in Chinese patients with advanced non-small cell lung cancer. Lung Cancer 2019, 130, 10–17. [Google Scholar] [CrossRef]
- Routy, B.; Le Chatelier, E.; DeRosa, L.; Duong, C.P.; Alou, M.T.; Daillère, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1–based immunotherapy against epithelial tumors. Science 2017, 359, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, V.; Spencer, C.N.; Nezi, L.; Reuben, A.; Andrews, M.C.; Karpinets, T.V.; Prieto, P.A.; Vicente, D.; Hoffman, K.; Wei, S.C.; et al. Gut microbiome modulates response to anti–PD-1 immunotherapy in melanoma patients. Science 2017, 359, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Matson, V.; Fessler, J.; Bao, R.; Chongsuwat, T.; Zha, Y.; Alegre, M.-L.; Luke, J.J.; Gajewski, T.F. The commensal microbiome is associated with anti–PD-1 efficacy in metastatic melanoma patients. Science 2018, 359, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Vétizou, M.; Pitt, J.M.; Daillère, R.; Lepage, P.; Waldschmitt, N.; Flament, C.; Rusakiewicz, S.; Routy, B.; Roberti, M.P.; Duong, C.P.; et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science 2015, 350, 1079–1084. [Google Scholar] [CrossRef]
- Tinsley, N.; Zhou, C.; Villa, S.; Tan, G.; Lorigan, P.C.; Blackhall, F.H.; Elliott, T.; Krebs, M.G.; Carter, L.; Thistlethwaite, F.; et al. Cumulative antibiotic use and efficacy of immune checkpoint inhibitors in patients with advanced cancer. J. Clin. Oncol. 2018, 36, 3010. [Google Scholar] [CrossRef]
- Huang, X.-Z.; Gao, P.; Song, Y.-X.; Xu, Y.; Sun, J.-X.; Chen, X.-W.; Zhao, J.-H.; Wang, Z.-N. Antibiotic use and the efficacy of immune checkpoint inhibitors in cancer patients: A pooled analysis of 2740 cancer patients. OncoImmunology 2019, 8, e1665973. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/ Year | Type of Study | N° Of Patients (Disease) | Treatment Received (%) | Median Age (Years) | Ab% /Timing | Median Duration (Weeks)/n° of AB Courses/pts | Med FUP (mos) | Type of Analysis | Covariates of MVA for OS | Quality (NOS Score) |
|---|---|---|---|---|---|---|---|---|---|---|
| Abu-Sbeih/ 2019 | retrospective | 826 (melanoma n = 347; hematologic n = 116; other n = 363) | anti-PD(L)1 (51.6), anti-CTLA4 (32), combo (16.5) | 62 | 68.9 /before or after start (47.5%), both (52.5%) | NR/NR | NR | MVA | ICI type, Stage IV cancer, IMDC, anaerobic AB use | 6 |
| Ahmed/ 2018 | retrospective | 60 (NSCLC n = 34; other n = 26) | anti-PD1 (81.7), anti-PDL1 (5), ICI + CT (13.3) | 59 | 28 /2w before and/or after start | 1–2 | NR | MVA | broad spectrum AB use, age | 5 |
| Derosa/ 2018 | retrospective | 360 (RCC n = 121, NSCLC n = 239) | RCC: anti-PD(L)1 (88), anti-PD(L)1 + anti-CTLA4 (8), anti-PD(L)1 + BEVA (4) NSCLC: anti-PD(L)1 (86), combo (14) | 64 | 21.5 /1 mos before start | NR/NR | NR | MVA | RCC: ab 30–0 days/no AB IMDC risk, tumour burden NSCLC: ab 30–0 days/no AB, PS, clinical trial Y/N, prior regimens >/<3 | 5 |
| Elkrief/ 2019 | retrospective | 59 (melanoma) * | NIVO/PEMBRO/IPI (100) | 64.5 | 13.5° /1 month before | 0.9/NR | NR | MVA | age, PS, gender, AB use, LDH, BRAF, line of tx, type of ICI | 5 |
| Galli/ 2019 | retrospective | 157 (NSCLC) | anti-PD(L)1 (95.6), anti-CTLA4 o combo (4.4) | 66.7 | 17.2 /during ICI period | 1/NR | 28.6 | MVA | high AB /immunotherapy exposure ratio through entire ICI period | 8 |
| Guo/ 2019 | retrospective | 49 (oesophageal) | anti-PD(L1) alone (61), combo (39) | 56.7 | 43/2 mos before or 1 month after | 1.42/NR | 16.4 | MVA | PS, treatment, n° of metastatic sites, NLR, antibiotic use | 7 |
| Hakozaki/ 2019 | retrospective | 90 (NSCLC) | NIVO (100) | 68 | 14.4/1 month before start | >1 (84.6%)/ | NR | MVA | driver mutations | 6 |
| Huemer/ 2018 | retrospective | 30 (NSCLC) | NIVO (83), PEMBRO (17) | NR | 37/1 month before/after start | NR/NR | NR | MVA | sex, antibiotic use, ICI, EGFR/ALK mutations, line of tx, PDL1 status, immune-related adverse events | 5 |
| Huemer/ 2019 | retrospective | 142 (NSCLC) | NIVO, PEMBRO or ATEZO (100) | 66 | 44/1 months before or after start | NR/NR | 13.3 | UVA | NR | 7 |
| Kaderbhai/ 2017 | retrospective | 74 (NSCLC) | NIVO (100) | 67.5 | 20.3/3 months before or concurrent | 1/NR | NR | UVA (PFS) | NR | 5 |
| Krief/ 2019 | prospective cohort | 72 (NSCLC) | NIVO (100) | 68.8 | 42/2 months before or 1 month after start | 1.35/1.7 | 16.6 | MVA | AB use; KRAS mutations, gemmatimonadaceae on blood microbiome at baseline | 7 |
| Pinato/ 2019 | prospective cohort | 196 (NSCLC n = 118; melanoma n = 38; RCC n = 11; other n = 26) | anti-PD(L)1 (96) | 68 | 29/1 month before or concurrent | NR/NR | NR | MVA | response to ICI, AB 0–30 days before ICI | 6 |
| Sen/ 2018 | retrospective | 172 (NSCLC n = 21; RCC n = 25; melanoma n = 16; sarcoma n = 16; other n = 94) | anti-CTLA4 (61), anti-PD1 (39) | 60 | 33/during and up to 2 mos before | NR/NR | NR | UVA | NR | 5 |
| Tinsley/ 2019 | retrospective | 291 (melanoma n = 179, RCC n = 48, NSCLC n = 69) | NR | 66 | 32/2w before up to 6w after start | NR/NR | NR | MVA | AB use, comorbidities, metastatic sites > 3, PS > 0 | 6 |
| Zhao/ 2019 | retrospective | 109 (NSCLC) | anti-PD1 (52.3), anti-PD1 + CT (30.3), anti-PD1 + antiangiogenic (17.4) | 62 | 18.3/1 mos before or after start | NR/NR | NR | MVA | AB use, PS | 6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrelli, F.; Iaculli, A.; Signorelli, D.; Ghidini, A.; Dottorini, L.; Perego, G.; Ghidini, M.; Zaniboni, A.; Gori, S.; Inno, A. Survival of Patients Treated with Antibiotics and Immunotherapy for Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1458. https://doi.org/10.3390/jcm9051458
Petrelli F, Iaculli A, Signorelli D, Ghidini A, Dottorini L, Perego G, Ghidini M, Zaniboni A, Gori S, Inno A. Survival of Patients Treated with Antibiotics and Immunotherapy for Cancer: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(5):1458. https://doi.org/10.3390/jcm9051458
Chicago/Turabian StylePetrelli, Fausto, Alessandro Iaculli, Diego Signorelli, Antonio Ghidini, Lorenzo Dottorini, Gianluca Perego, Michele Ghidini, Alberto Zaniboni, Stefania Gori, and Alessandro Inno. 2020. "Survival of Patients Treated with Antibiotics and Immunotherapy for Cancer: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 5: 1458. https://doi.org/10.3390/jcm9051458
APA StylePetrelli, F., Iaculli, A., Signorelli, D., Ghidini, A., Dottorini, L., Perego, G., Ghidini, M., Zaniboni, A., Gori, S., & Inno, A. (2020). Survival of Patients Treated with Antibiotics and Immunotherapy for Cancer: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 9(5), 1458. https://doi.org/10.3390/jcm9051458