Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure


Abstract
1. Introduction
2. Patients and Methods
2.1. Study Group
2.2. Nutritional Assessment and Cachexia Detection
2.3. Bioelectrical Impedance Analysis
2.4. Plasma IrisinConcentration
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Sobieszek, G.; Mlak, R.; Skwarek-Dziekanowska, A.; Jurzak-Myśliwy, A.; Homa-Mlak, I.; Małecka-Massalska, T. Electrical Changes in Polish Patients with Chronic Heart Failure: Preliminary Observations. Medicina 2019, 55, 484. [Google Scholar] [CrossRef] [PubMed]
- Ramani, G.V.; Uber, P.A.; Mehra, M.R. Chronic Heart Failure: Contemporary Diagnosis and Management. Mayo Clin. Proc. 2010, 85, 180–195. [Google Scholar] [CrossRef] [PubMed]
- Gřiva, M. Cardiac cachexia-Up-to-date 2015. Cor Vasa 2016, 58. [Google Scholar] [CrossRef]
- Okoshi, M.P.; Capalbo, R.V.; Romeiro, F.G.; Okoshi, K. Cardiac Cachexia: Perspectives for Prevention and Treatment. Arq. Bras. Cardiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Kalkan, A.K.; Cakmak, H.A.; Erturk, M.; Kalkan, K.U.; Uzun, F.; Tasbulak, O.; Diker, V.O.; Aydin, S.; Celik, A. Adropin and Irisin in Patients with Cardiac Cachexia. Arq. Bras. Cardiol. 2018. [Google Scholar] [CrossRef]
- Aydin, S.; Aydin, S. Irisin Concentrations as a Myocardial Biomarker. Biomark. Cardiovasc. Dis. 2016, 489–504. [Google Scholar] [CrossRef]
- Piątek, P.; Fabian-Danielewska, A.; Korabiusz, K. The role of irisin in ischemic heart diesease. J. Educ. Health Sport 2019, 9, 30–35. [Google Scholar] [CrossRef]
- Silvestrini, A.; Bruno, C.; Vergani, E.; Venuti, A.; Favuzzi, A.M.R.; Guidi, F.; Nicolotti, N.; Meucci, E.; Mordente, A.; Mancini, A. Circulating irisin levels in heart failure with preserved or reduced ejection fraction: A pilot study. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- El-Mottaleb, N.A.A.; Galal, H.M.; Maghraby, K.M.E.; Gadallah, A.I. Serum irisin level in myocardial infarction patients with or without heart failure. Can. J. Physiol. Pharmacol. 2019, 97, 932–938. [Google Scholar] [CrossRef]
- Khalil, S.; Mohktar, M.; Ibrahim, F. The Theory and Fundamentals of Bioimpedance Analysis in Clinical Status Monitoring and Diagnosis of Diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef]
- Grundmann, O.; Yoon, S.L.; Williams, J.J. The value of bioelectrical impedance analysis and phase angle in the evaluation of malnutrition and quality of life in cancer patients—A comprehensive review. Eur. J. Clin. Nutr. 2015, 69, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Génot, N.; Mewton, N.; Bresson, D.; Zouaghi, O.; Francois, L.; Delwarde, B.; Kirkorian, G.; Bonnefoy-Cudraz, E. Bioelectrical impedance analysis for heart failure diagnosis in the ED. Am. J. Emerg. Med. 2015, 33, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- The Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 9th ed.; Little, Brown & Co.: Boston, MA, USA, 1994; pp. 253–256. [Google Scholar]
- Evans, W.J.; Morley, J.E.; Argiles, J.; Bales, C.; Baracos, V.; Guttridge, D.; Jatoi, A.; Kalantar-Zadeh, K.; Lochs, H.; Mantovani, G.; et al. Cachexia: A new definition. Clin. Nutr. 2008, 27, 793–799. [Google Scholar] [CrossRef]
- Hsieh, I.C.; Ho, M.Y.; Wen, M.S.; Chen, C.C.; Hsieh, M.J.; Lin, C.P.; Yeh, J.K.; Tsai, M.L.; Yang, C.H.; Wu, V.C.; et al. Serum irisin levels are associated with adverse cardiovascular outcomes in patients with acute myocardial infarction. Int. J. Cardiol. 2018, 261, 12–17. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2012, 14, 803–869. [Google Scholar] [CrossRef]
- Okoshi, M.P.; Romeiro, F.G.; Paiva, S.A.R.; Okoshi, K. Heart Failure-Induced Cachexia. Arq. Bras. Cardiol. 2013. [Google Scholar] [CrossRef]
- Emami, A.; Saitoh, M.; Valentova, M.; Sandek, A.; Evertz, R.; Ebner, N.; Loncar, G.; Springer, J.; Doehner, W.; Lainscak, M.; et al. Comparison of sarcopenia and cachexia in men with chronic heart failure: Results from the Studies Investigating Co-morbidities Aggravating Heart Failure (SICA-HF). Eur. J. Heart Fail. 2018, 20, 1580–1587. [Google Scholar] [CrossRef]
- Di Ieva, A.; Butz, H.; Niamah, M.; Rotondo, F.; De Rosa, S.; Sav, A.; Yousef, G.M.; Kovacs, K.; Cusimano, M.D. MicroRNAs as biomarkers in pituitary tumors. Neurosurgery 2014, 75, 181–189. [Google Scholar] [CrossRef]
- Okugawa, Y.; Yao, L.; Toiyama, Y.; Yamamoto, A.; Shigemori, T.; Yin, C.; Omura, Y.; Ide, S.; Kitajima, T.; Shimura, T.; et al. Prognostic impact of sarcopenia and its correlation with circulating miR-21 in colorectal cancer patients. Oncol. Rep. 2018, 39, 1555–1564. [Google Scholar] [CrossRef]
- De Rosa, S.; Indolfi, C. Circulating microRNAs as Biomarkers in Cardiovascular Diseases. In Circulating microRNAs in Disease Diagnostics and Their Potential Biological Relevance; Experientia, S., Igaz, P., Eds.; Springer: Basel, Switzerland, 2015; Volume 106. [Google Scholar]
- Antunes-Correa, L.M.; Trevizan, P.F.; Bacurau, A.V.N.; Ferreira-Santos, L.; Gomes, J.L.P.; Urias, U.; Oliveira, P.A.; Alves, M.J.N.N.; de Almeida, D.R.; Brum, P.C.; et al. Effects of aerobic and inspiratory training on skeletal muscle microRNA-1 and downstream-associated pathways in patients with heart failure. J. Cachexia Sarcopenia Muscle 2020, 11, 89–102. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Eposito, F.; Carella, C.; Strangio, A.; Ammirati, G.; Sabatino, J.; Abbate, F.G.; Iaconetti, C.; Liguori, V.; Pergola, V.; et al. Transcoronary concentration gradients of circulating microRNAs in heart failure. Eur. J. Heart Fail. 2018, 20, 1000–1010. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factor | Study Group (n = 66) | |
|---|---|---|
| Age (years) | 77 ± 9.0 | |
| Weight (kg) | 77 ± 18.0 | |
| BMI (kg/m2) | 29.75 ± 6.52 | |
| FM (kg) | 26.45 ± 11.14 | |
| FFM (kg) | 50.08 ± 12.45 | |
| Albumin (g/dL) | 3.44 ± 0.59 | |
| Triglycerides (mg/dL) | 119.8 ± 64.0 | |
| Total cholesterol (mg/dL) | 172.1 ± 46.2 | |
| HDL (mg/dL) | 54.66 ± 16.9 | |
| LDL (mg/dL) | 91.80 ± 36.79 | |
| Creatinine (mg/dL) | 1.19 ± 0.53 | |
| Hemoglobin (g/dL) | 12.48 ± 1.93 | |
| CRP (mg/L) † | 4.0 (1.60–17.43) | |
| TNF-α (pg/mL) † | 3.92 (3.22–5.10) | |
| IL-6 (pg/mL) | 5.52 (3.21–8.69) | |
| Irisin (µg/mL) † | 7.12 (5.70–9.99) | |
| Systolic blood pressure (mmHg) | 134 ± 22.0 | |
| Diastolic blood pressure (mmHg) | 76 ± 11.0 | |
| EF% | 45 ± 11.0 | |
| NT-proBNP (pg/mL) † | 2332 (1002–4010) | |
| LVESd (cm) | 4.04 ± 0.83 | |
| LVEDd (cm) | 5.45 ± 0.79 | |
| LAD (cm) | 4.45 ± 0.63 | |
| RVOT (cm) | 3.33 ± 0.37 | |
| TAPSE (cm) | 1.91 ± 0.40 | |
| PASP (mmHg) | 41 ± 11.0 | |
| NYHA | I | 13 (19.7%) |
| II | 21 (31.8%) | |
| III | 21 (31.8%) | |
| IV | 11 (16.7%) | |
| SGA | A | 35 (53%) |
| B | 23 (34.8%) | |
| C | 8 (12.2%) | |
| Diabetes mellitus | 28 (42.4%) | |
| Renal failure | 25 (37.9%) | |
| ACEi treatment | 40 (60.6%) | |
| ARBs treatment | 11 (16.7%) | |
| HRT treatment | 8 (12.1%) | |
| SmokingStatus | smoker | 36 (54.5%) |
| non-smoker | 30 (45.5%) | |
| Cm (nF) † | 1.159 (0.750–1.681) | |
| Pa (o) | 4.09 ± 1.22 | |
| Z200/Z5 | 0.853 (0.830–0.879) | |
| Factor | Cachectic (n = 34) | Non-Cachectic (n = 32) | p | |
|---|---|---|---|---|
| Age (years) | 80 ± 12 | 77 ± 9 | 0.267 | |
| Weight (kg) | 71 ± 17 | 82 ± 17 | 0.010 | |
| BMI (kg/m2) | 28.02 ± 6.22 | 31.64 ± 6.41 | 0.024 | |
| FM (kg) | 23.14 ± 9.32 | 29.92 ± 10.89 | 0.020 | |
| FFM (kg) | 46.61 ± 13.21 | 53.96 ± 10.48 | 0.031 | |
| Albumin (g/dL) | 3.14 ± 0.61 | 3.76 ± 0.36 | <0.001 | |
| Triglycerides (mg/dL) | 118.0 ± 60.6 | 121.9 ± 68.6 | 0.806 | |
| Total cholesterol (mg/dL) | 167.6 ± 52.0 | 177.0 ± 39.0 | 0.417 | |
| HDL (mg/dL) | 49.90 ± 16.72 | 59.88 ± 15.94 | 0.017 | |
| LDL (mg/dL) | 92.26 ± 39.88 | 91.28 ± 33.72 | 0.915 | |
| Hemoglobin (g/dL) | 11.97 ± 1.84 | 13.04 ± 1.89 | 0.025 | |
| CRP (mg/L) † | 10.95 (1.96–26.20) | 3.10 (1.45–4.95) | 0.005 | |
| TNF-α (pg/mL) † | 4.48 (3.49–5.13) | 3.29 (3.07–4.91) | 0.032 | |
| Irisin (µg/mL) † | 7.12 (5.94–9.42) | 7.61 (5.29–10.39) | 0.022 | |
| Systolic blood pressure (mmHg) | 132 ± 22 | 137 ± 22 | 0.409 | |
| Diastolic blood pressure (mmHg) | 75 ± 12 | 76 ± 11 | 0.754 | |
| EF% | 42 ± 13.0 | 48 ± 9.0 | 0.039 | |
| NT-proBNP (pg/mL) † | 3476 (1690–5773) | 1176 (716–2605) | <0.001 | |
| LVESd (cm) | 4.11 ± 0.89 | 3.97 ± 0.80 | 0.514 | |
| LVEDd (cm) | 4.99 ± 0.85 | 5.04 ± 0.71 | 0.833 | |
| LAD (cm) | 4.54 ± 0.72 | 4.36 ± 0.52 | 0.271 | |
| RVOT (cm) | 3.35 ± 0.41 | 3.32 ± 0.32 | 0.704 | |
| TAPSE (cm) | 1.84 ± 0.42 | 1.96 ± 0.37 | 0.180 | |
| PASP (mmHg) | 42.8 ± 12.5 | 39.2 ± 10.0 | 0.208 | |
| NYHA I+II | 13 (38.2%) | 21 (65.6%) | 0.030 | |
| NYHA III+IV | 21 (61.8%) | 11 (34.4%) | ||
| ACEi | Yes | 18 (52.9%) | 22 (68.8%) | 0.216 |
| No | 16 (47.1%) | 10 (31.2%) | ||
| ARBs | Yes | 8 (23.5%) | 3 (9.4%) | 0.188 |
| No | 26 (76.5%) | 29 (90.6%) | ||
| HRT | Yes | 1 (3%) | 7 (21.9%) | 0.025 |
| No | 33 (97%) | 25 (78.1%) | ||
| SGA-A | 9 (26.5%) | 26 (81.3%) | <0.001 | |
| SGA-B+C | 25 (73.5%) | 6 (18.7%) | ||
| Cm (nF) † | 0.860(0.670–1.070) | 1.280 (0.916–1.789) | <0.001 | |
| Pa (o) | 3.60 ± 1.17 | 4.60 ± 1.08 | 0.005 | |
| Z200/Z5 | 0.877(0.840–0.887) | 0.845 (0.823–0.854) | 0.002 | |
| Factor | R [95%CI] | p |
|---|---|---|
| Positive Correlation | ||
| FM | 0.408 [0.155 to 0.681] | 0.020 |
| HDL | 0.318 [0.080 to 0.524] | 0.010 |
| EF% | 0.253 [0.010 to 0.471] | 0.046 |
| Negative Correlation | ||
| Cm | −0.393 [−0.580 to −0.167] | 0.005 |
| CRP | −0.362 [−0.561 to −0.123] | 0.004 |
| LVESd | −0.326 [−0.529 to −0.090] | 0.009 |
| NT-proBNP | −0.320 [−0.532 to −0.080] | 0.010 |
| LVEDd | −0.272 [−0.485 to −0.027] | 0.030 |
| TNF-α | −0.243 [−0.436 to −0.005] | 0.044 |
| Univariate Analysis | ||
| Factor | OR [95%CI] | p |
| Albumin | 33.18 [5.00–220.4] | <0.001 |
| Cm | 10.76 [2.586–44.78] | <0.001 |
| CRP | 1.10 [1.030–1.700] | 0.007 |
| FFM | 1.05 [1.0–1.111] | 0.040 |
| Hemoglobin | 1.328 [1.001–1.751] | 0.030 |
| BMI | 1.11 [1.01–1.210] | 0.025 |
| Body weight | 1.04 [1.008–1.078] | 0.013 |
| Multivariate Analysis | ||
| Factor | OR [95%CI] | p |
| Albumin | 50.48 [2.594–182.39] | 0.009 |
| Cm | 34.49 [4.181–282.54] | 0.007 |
| Irisin | 1.390 [1.07–1.079] | 0.013 |
| Overall model fit p < 0.001 | ||
| Factor | Sensitivity | Specificity | AUC [95%CI] | Cut-Off Value | p |
|---|---|---|---|---|---|
| Albumin | 93.5% | 52.8% | 0.724 [0.582–0.788] | 3.30 | <0.001 |
| CRP | 55.9% | 87.1% | 0.704 [0.577–0.810] | 9.65 | 0.003 |
| Cm | 52.9% | 90.6% | 0.787 [0.669–0.878] | 0.789 | <0.001 |
| Irisin | 64.7% | 46.9% | 0.580 [0.452–0.700] | 8.11 | 0.270 |
| Cm+CRP | 70.6% | 83.9% | 0.855 [0.745–0.930] | - | <0.001 |
| Cm+albumin | 96.8% | 76.5% | 0.917 [0.821–0.971] | - | <0.001 |
| Cm+Irisin | 61.8% | 96.9% | 0.849 [0.740–0.925] | - | <0.001 |
| CRP+albumin | 96.7% | 70.6% | 0.858 [0.748–0.933] | - | <0.001 |
| CRP+Irisin | 58.8% | 90.3% | 0.731 [0.607–0.834] | - | <0.001 |
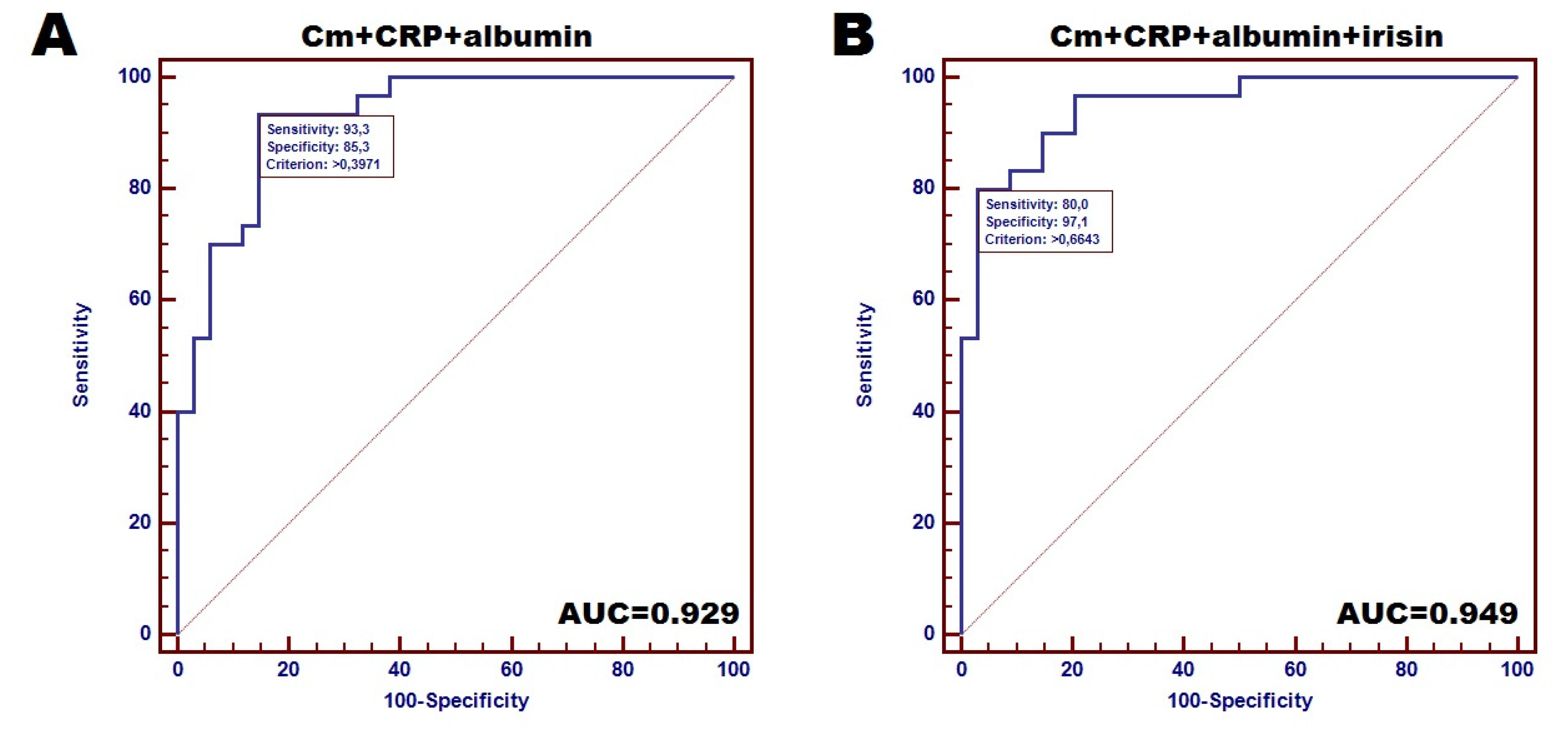
| Cm+albumin+CRP | 93.3% | 85.3% | 0.929 [0.938–0.979] | - | <0.001 |
| 4 markers | 80% | 97.1% | 0.949 [0.863–0.988] | - | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobieszek, G.; Powrózek, T.; Mazurek, M.; Skwarek-Dziekanowska, A.; Małecka-Massalska, T. Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure. J. Clin. Med. 2020, 9, 1021. https://doi.org/10.3390/jcm9041021
Sobieszek G, Powrózek T, Mazurek M, Skwarek-Dziekanowska A, Małecka-Massalska T. Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure. Journal of Clinical Medicine. 2020; 9(4):1021. https://doi.org/10.3390/jcm9041021
Chicago/Turabian StyleSobieszek, Grzegorz, Tomasz Powrózek, Marcin Mazurek, Anna Skwarek-Dziekanowska, and Teresa Małecka-Massalska. 2020. "Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure" Journal of Clinical Medicine 9, no. 4: 1021. https://doi.org/10.3390/jcm9041021
APA StyleSobieszek, G., Powrózek, T., Mazurek, M., Skwarek-Dziekanowska, A., & Małecka-Massalska, T. (2020). Electrical and Hormonal Biomarkers in Cachectic Elderly Women with Chronic Heart Failure. Journal of Clinical Medicine, 9(4), 1021. https://doi.org/10.3390/jcm9041021