Impact of Timely Public Health Measures on Kidney Transplantation in Austria during the SARS-CoV-2 Outbreak—A Nationwide Analysis

 ,
, 
Abstract
1. Introduction
SARS-CoV-2 in Austria
2. Methods
3. Results
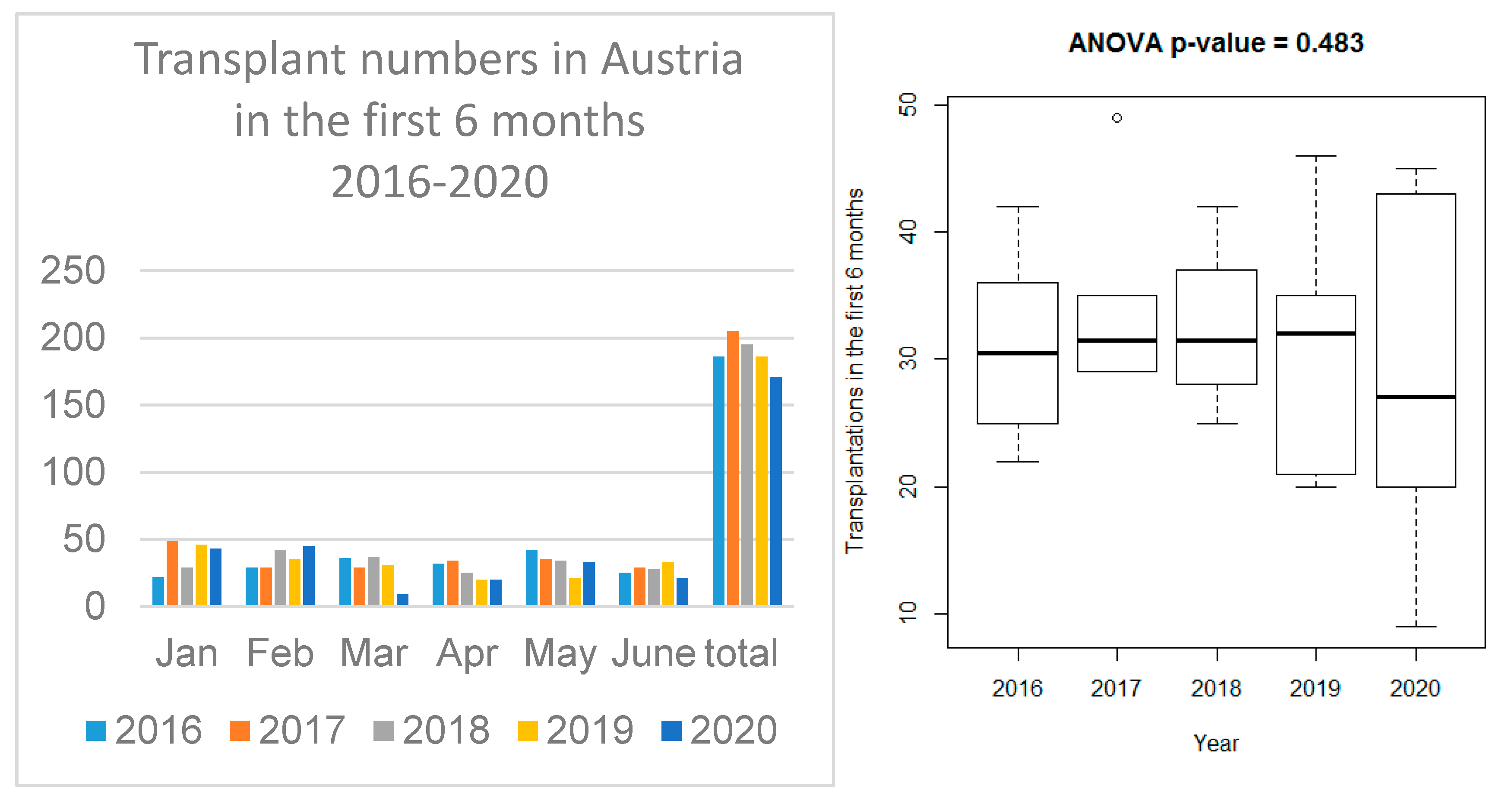
3.1. Transplant Activity in the Four Austrian Transplant Centers
3.2. Deceased Donor Transplantation
3.3. Living Donor Transplantation
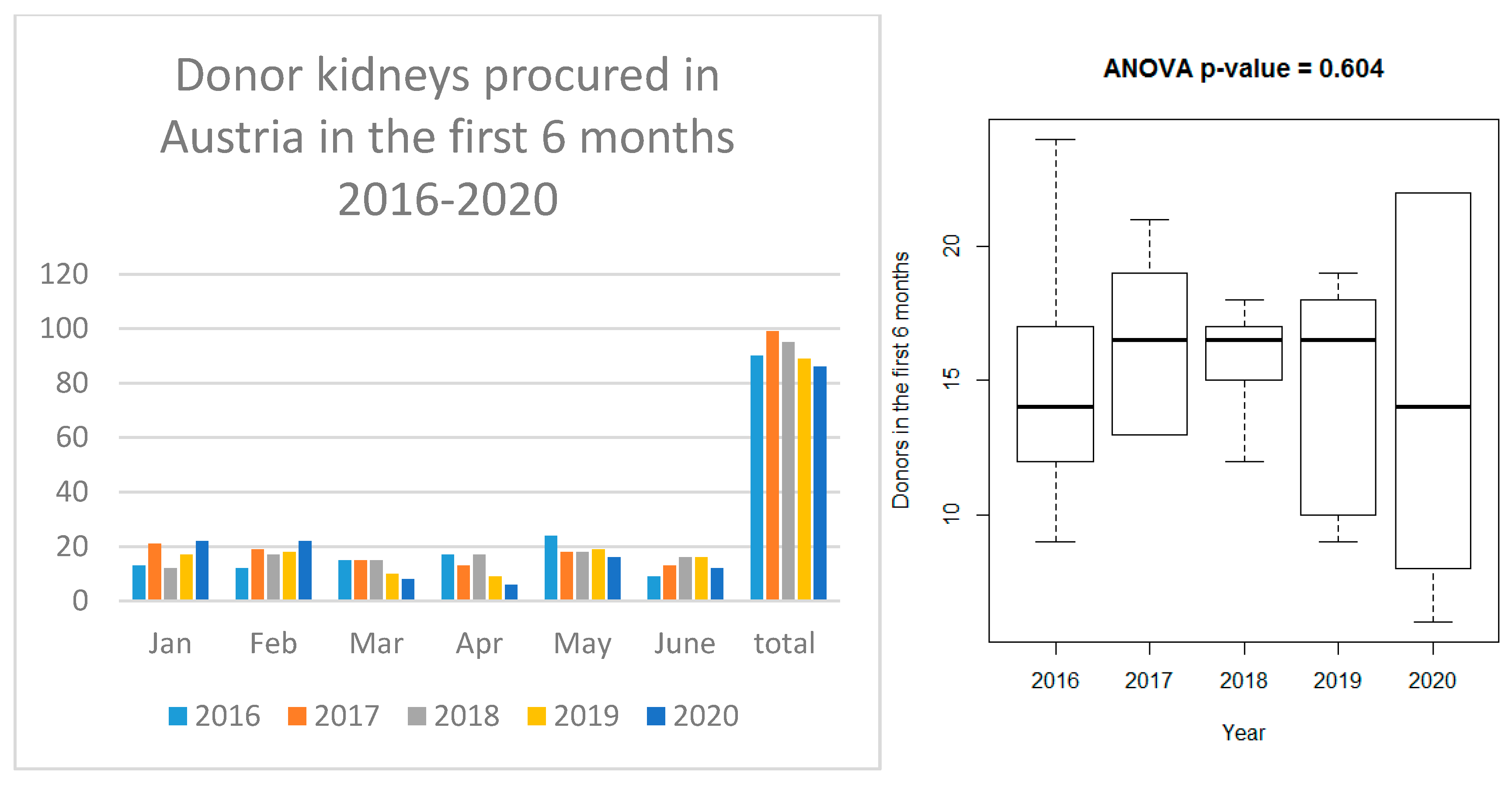
3.4. Organ Procurement
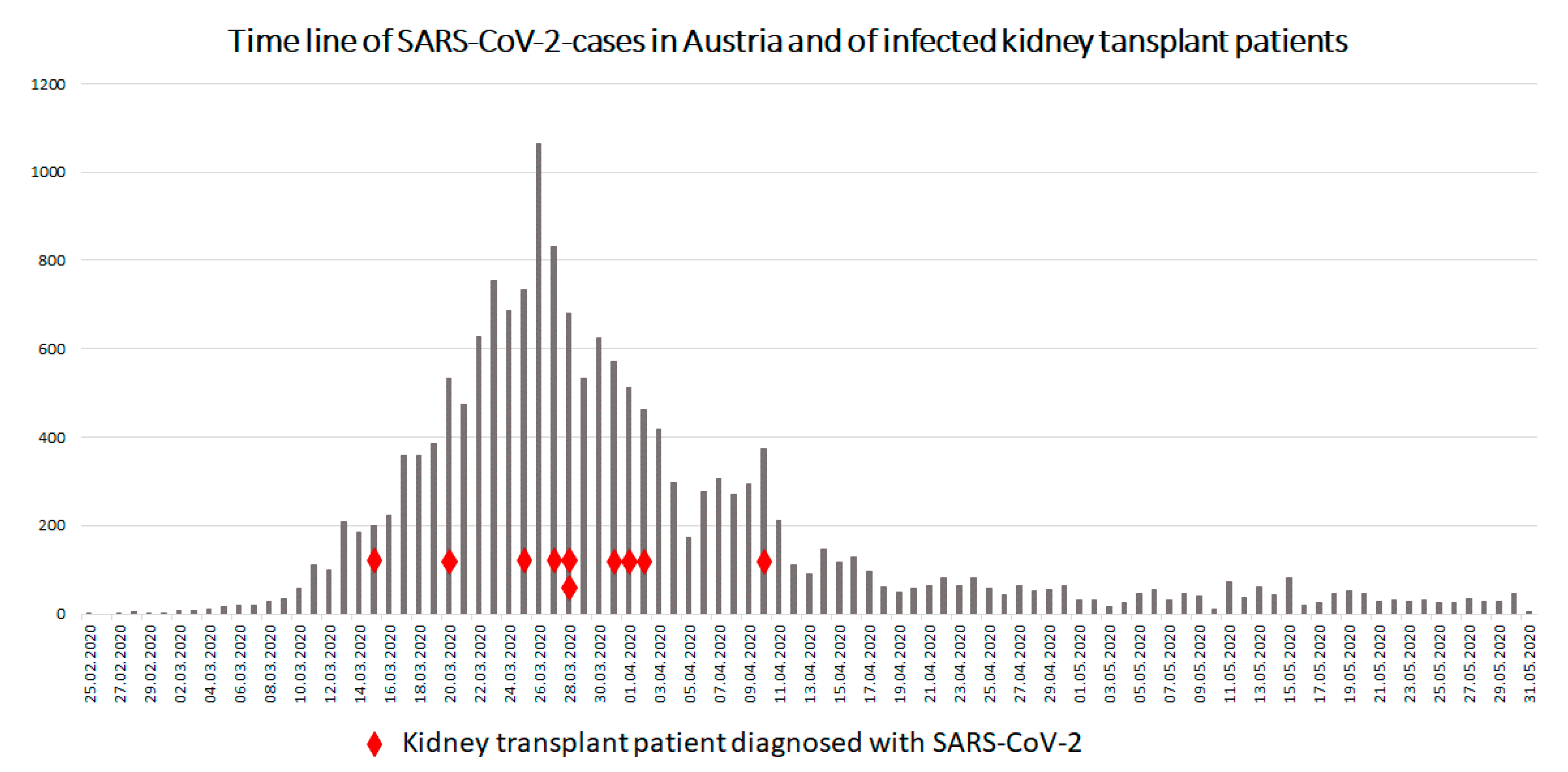
3.5. SARS-CoV-2 Infections in Austrian Transplant Patients
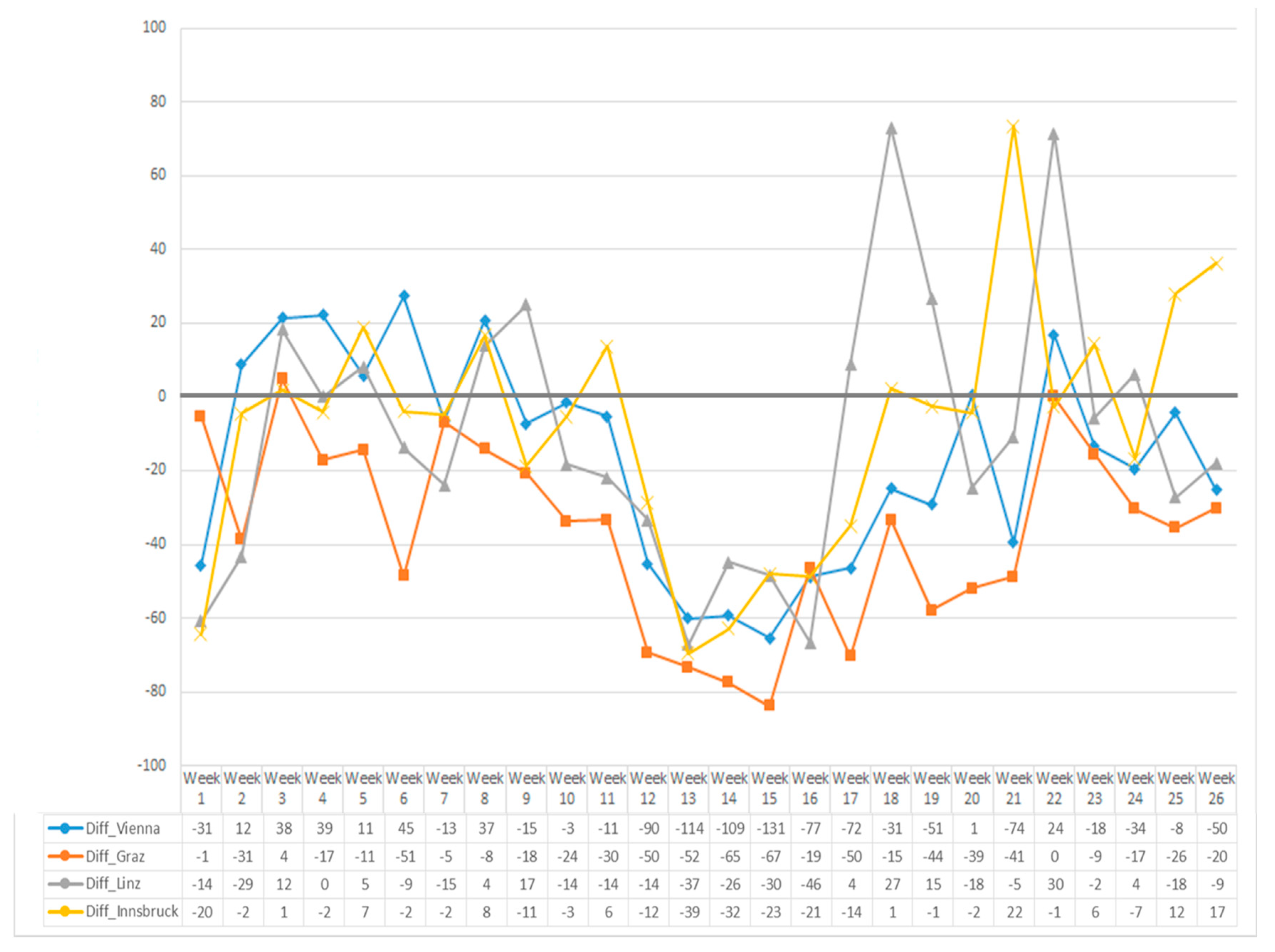
3.6. Post-Transplant Care of Austrian Kidney Recipients
4. Discussion
5. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- Covid-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. Available online: https://coronavirusjhuedu/maphtml (accessed on 12 September 2020).
- Maggiore, U.; Abramowicz, D.; Crespo, M.; Mariat, C.; Mjoen, G.; Peruzzi, L.; Sever, M.S.; Oniscu, G.C.; Hilbrands, L.; Watschinger, B. How should I manage immunosuppression in a kidney transplant patient with COVID-19? An ERA-EDTA DESCARTES expert opinion. Nephrol. Dial. Transpl. 2020, 35, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. Covid-19 and Kidney Transplantation. N. Engl. J. Med. 2020, 382, 2475–2477. [Google Scholar] [CrossRef] [PubMed]
- Alberici, F.; Delbarba, E.; Manenti, C.; Econimo, L.; Valerio, F.; Pola, A.; Maffei, C.; Possenti, S.; Zambetti, N.; Moscato, M.; et al. A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV2 pneumonia. Kidney Int. 2020, 97, 1083–1088. [Google Scholar] [CrossRef]
- Columbia University Kidney Transplant Program Early. Description of Coronavirus 2019 Disease in Kidney Transplant Recipients in New York. J. Am. Soc. Nephrol. JASN 2020, 31, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Hoek, R.A.S.; Manintveld, O.C.; Betjes, M.G.H.; Hellemons, M.E.; Seghers, L.; Van Kampen, J.A.A.; Caliskan, K.; Van De Wetering, J.; Hoogen, M.V.D.; Metselaar, H.J.; et al. COVID-19 in solid organ transplant recipients: A single-center experience. Transpl. Int. 2020. [Google Scholar] [CrossRef] [PubMed]
- Montagud-Marrahi, E.; Cofan, F.; Torregrosa, J.; Cucchiari, D.; Ventura-Aguiar, P.; Revuelta, I.; Bodro, M.; Piñeiro, G.J.; Esforzado, N.; Ugalde, J.; et al. Preliminary data on outcomes of SARS-CoV-2 infection in a Spanish single center cohort of kidney recipients. Am. J. Transpl. 2020, 20, 2958–2959. [Google Scholar] [CrossRef]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.K.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transpl. 2020, 20, 1800–1808. [Google Scholar] [CrossRef]
- Bellini, M.I.; Tortorici, F.; Capogni, M. Kidney transplantation and the lockdown effect. Transpl. Int. 2020, 33, 1142–1143. [Google Scholar] [CrossRef]
- Vistoli, F.; Furian, L.; Maggiore, U.; Caldara, R.; Cantaluppi, V.; Ferraresso, M.; Zaza, G.; Cardillo, M.; Biancofiore, G.; Menichetti, F.; et al. COVID-19 and kidney transplantation: An Italian Survey and Consensus. J. Nephrol. 2020, 33, 667–680. [Google Scholar] [CrossRef] [PubMed]
- Loupy, A.; Aubert, O.; Reese, P.P.; Bastien, O.; Bayer, F.; Jacquelinet, C. Organ procurement and transplantation during the COVID-19 pandemic. Lancet 2020, 395, e95–e96. [Google Scholar] [CrossRef]
- International Registry of Organ Donation and Transplantation. Available online: http://www.irodat.org (accessed on 12 September 2020).
- Gerli, A.G.; Centanni, S.; Miozzo, M.R.; Virchow, J.C.; Sotgiu, G.; Canonica, G.W.; Soriano, J.B. COVID-19 mortality rates in the European Union, Switzerland, and the UK: Effect of timeliness, lockdown rigidity, and population density. Minerva Med. 2020, 111, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Limited TEIU. How well have OECD Countries Responded to the Coronavirus Crisis? A Report by The Economist Intelligence Unit 2020. Available online: https://www.eiu.com/n/campaigns/oecd-countries-responded-to-the-coronavirus-crisis/#mktoForm_anchor (accessed on 12 September 2020).
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-Harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Ritschl, P.V.; Nevermann, N.; Wiering, L.; Wu, H.H.; Moroder, P.; Brandl, A.; Hillebrandt, K.; Tacke, F.; Friedersdorff, F.; Schlomm, T.; et al. Solid organ transplantation programs facing lack of empiric evidence in the COVID-19 pandemic: A By-proxy Society Recommendation Consensus approach. Am. J. Transpl. 2020, 20, 1826–1836. [Google Scholar] [CrossRef]
- Ahn, C.; Amer, H.; Anglicheau, D.; Ascher, N.; Baan, C.; Battsetset, G.; Bat-Ireedui, B.; Berney, T.; Betjes, M.; Bichu, S.; et al. Global Transplantation COVID Report March 2020. Transplantation 2020, 104, 1974–1983. [Google Scholar] [CrossRef]
- Angelico, R.; Trapani, S.; Manzia, T.M.; Lombardini, L.; Tisone, G.; Cardillo, M. The COVID-19 outbreak in Italy: Initial implications for organ transplantation programs. Am. J. Transpl. 2020, 20, 1780–1784. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Chiang, T.P.; Werbel, W.A.; Durand, C.M.; Avery, R.K.; Getsin, S.N.; Jackson, K.R.; Kernodle, A.B.; Rasmussen, S.E.V.P.; Massie, A.B.; et al. Early impact of COVID-19 on transplant center practices and policies in the United States. Am. J. Transpl. 2020, 20, 1809–1818. [Google Scholar] [CrossRef]
- Cacciola, R. Response to “The COVID-19 outbreak in Italy: Initial implications for organ transplantation programs”. Am. J. Transpl. 2020, 20, 1937–1938. [Google Scholar] [CrossRef]
- Moeckli, B.; Peloso, A.; Oldani, G.; Orci, L.A.; Banz, V.; Dutkowski, P.; Toso, C.; Berney, T. The Swiss approach to the COVID-19 outbreak. Am. J. Transpl. 2020, 20, 1935–1936. [Google Scholar] [CrossRef]
- Pinar, U.; Anract, J.; Duquesne, I.; Dariane, C.; Chartier-Kastler, E.; Cussenot, O.; Desgrandchamps, F.; Hermieu, J.-F.; de La Taille, A.; Mejean, A.; et al. Impact of the COVID-19 pandemic on surgical activity within academic urological departments in Paris. Progres en Urologie Journal de l’Association Francaise D’urologie et de la Societe Francaise D’urologie 2020, 30, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, E.; Miñambres, E.; Gutiérrez-Baños, J.L.; Valero, R.; Belmar, L.; Ruiz, J.C. COVID-19-related collapse of transplantation systems: A heterogeneous recovery? Am. J. Transpl. 2020, 10. [Google Scholar] [CrossRef]
- Dominguez-Gil, B.; Coll, E.; Fernández-Ruiz, M.; Corral, E.; Del Río, F.; Zaragoza, R.; Rubio, J.J.; Hernández, D. COVID-19 in Spain: Transplantation in the midst of the pandemic. Am. J. Transpl. 2020, 20, 2593–2598. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Shaw, A.; Lowe, M.; Summers, A.; van Dellen, D.; Augustine, T. The impact of the COVID-19 pandemic on renal transplantation in the UK. Clin. Med. 2020, 20, e82–e86. [Google Scholar] [CrossRef]
- ÖBIG-Transplant: Transplant-Jahresbericht 2018. Gesundheit Österreich GmbH, Wien. 2019. Available online: https://transplant.goeg.at/ (accessed on 12 September 2020).
- Li, Y.; Yang, N.; Li, X.; Wang, J.; Yan, T. Strategies for prevention and control of the 2019 novel coronavirus disease in the department of kidney transplantation. Transpl. Int. 2020. [Google Scholar] [CrossRef]
- Kumar, D.; Manuel, O.; Natori, Y.; Egawa, H.; Grossi, P.; Han, S.; Fernández-Ruiz, M.; Humar, A. COVID-19: A global transplant perspective on successfully navigating a pandemic. Am. J. Transpl. 2020, 20, 1773–1779. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID-19 Relevant Dates in Austria | |
|---|---|
| 25 February | First two cases of SARS-CoV-2 in Innsbruck |
| 27 February | First case of SARS-CoV-2 in Vienna |
| 12 March | First COVID-19-associated death in Austria (at 302 recorded SARS-CoV-2-positive cases) |
| 31 March | Peak (n = 1.110) of concurrently hospitalized COVID-19 patients |
| 3 April | Peak (n = 9.193) of concurrently COVID-19 ill individuals |
| 8 April | Peak (n = 267) of concurrently patients in intensive care (n = 267) |
| 18 April | First day with less than 100 new SARS-CoV-2-positive cases |
| 10 May | Less than 300 patients in hospital care |
| 17 May | Less than 50 patients in intensive care |
| Measures imposed by the Austrian government | |
| 10 March | Temporary ban of indoor events with >100 persons and outdoor events with >500 persons |
| 11 March | Announcement of planned school and university closures (2,3 cases/100,000 population, 206 new cases recorded) |
| 12 March | Universities close |
| 15 March | COVID-19 Law passed (9 cases/100,000 population, 800 cases recorded) |
| 16 March | Shops close (except grocery stores, pharmacies and drugstores) |
| Restaurants allowed to open only until 3 p.m. | |
| Prohibition of visiting public places | |
| 17 March | All bars and restaurants close |
| 18 March | All schools close |
| 20 March | Home office publicly advised for non-essential work |
| 1 April | Compulsory use of face covering/masks over nose/mouth in grocery stores, 1-m distance to be observed |
| 14 April | Compulsory use of face covering/masks over nose and mouth for public transportation and in all shops |
| 15 April | Re-opening of small shops |
| 1 May | Re-opening of larger shops |
| 15 May | Restaurants allowed to open with some restrictions |
| 18 May | Low-graders allowed back to schools |
| 25 May | Stepwise re-opening of schools |
| 29 May | Re-opening of hotels |
| 15 June | Use of face covering/masks over nose and mouth only for public transportation, in pharmacies and healthcare facilities and if 1 m distance is not feasible; restaurants allowed to open until 1 a.m.; easing of travel restrictions for most European countries |
| SARS-CoV-2 Infections in Austrian Transplant Patients | ||
|---|---|---|
| Patient characteristics | Sex (male/female) | 7/3 |
| Mean age (years; range) | 53.1 (35–77) | |
| Ethnicity (Caucasian/Asian) | 9/1 | |
| Reason for SARS-CoV-2 PCR test | Symptoms/screening | 9/1 |
| Transplantation | Type of transplant (deceased/living donation) | 6/3 |
| Time since last kidney transplantation (years; range) | 9.9 (1–20) | |
| Comorbidity | Hypertension | 7 |
| Coronary artery disease | 2 | |
| Diabetes mellitus | 2 | |
| Malignancy | 1 | |
| Obesity | 2 | |
| Symptoms | Fever | 6 |
| Cough | 5 | |
| Dyspnea | 3 | |
| Rhinitis | 1 | |
| Diarrhea | 5 | |
| Myalgia | 1 | |
| Hemodynamic instability | (yes/no) | 1/9 |
| Oxygen saturation | (mean %; range) | 95.5 (88–100) |
| Organ manifestation | Pneumonia | 3 |
| Rise in creatinine | 4 | |
| ECG changes | 1 | |
| No organ manifestation | 4 | |
| Immunosuppressive therapy | Triple/dual | 8/2 |
| Steroid/TAC/MPA | 4 | |
| Steroid/TAC/AZA | 3 | |
| Steroid/mTOR/MPA | 1 | |
| Steroid/TAC | 1 | |
| TAC/MPA | 1 | |
| Recent T-cell-depleting therapy | 0 | |
| Other therapeutics | Renin angiotensin inhibitor therapy | 4 |
| Clinical course | Hospital admission | 8 |
| ICU admission | 2 | |
| Changes of immunosuppression (yes/no) | 5/5 | |
| Antiviral therapy | 1 | |
| Renal replacement therapy | 0 | |
| Days in hospital (mean; range) | 14.1 (5–24) | |
| Outcome | Death/alive | 1/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watschinger, B.; Watschinger, C.; Reindl-Schwaighofer, R.; Meyer, E.L.; Deak, A.T.; Hammer, T.; Eigner, M.; Sprenger-Mähr, H.; Schneeberger, S.; Cejka, D.; et al. Impact of Timely Public Health Measures on Kidney Transplantation in Austria during the SARS-CoV-2 Outbreak—A Nationwide Analysis. J. Clin. Med. 2020, 9, 3465. https://doi.org/10.3390/jcm9113465
Watschinger B, Watschinger C, Reindl-Schwaighofer R, Meyer EL, Deak AT, Hammer T, Eigner M, Sprenger-Mähr H, Schneeberger S, Cejka D, et al. Impact of Timely Public Health Measures on Kidney Transplantation in Austria during the SARS-CoV-2 Outbreak—A Nationwide Analysis. Journal of Clinical Medicine. 2020; 9(11):3465. https://doi.org/10.3390/jcm9113465
Chicago/Turabian StyleWatschinger, Bruno, Clara Watschinger, Roman Reindl-Schwaighofer, Elias L. Meyer, Andras T. Deak, Tamara Hammer, Manfred Eigner, Hannelore Sprenger-Mähr, Stefan Schneeberger, Daniel Cejka, and et al. 2020. "Impact of Timely Public Health Measures on Kidney Transplantation in Austria during the SARS-CoV-2 Outbreak—A Nationwide Analysis" Journal of Clinical Medicine 9, no. 11: 3465. https://doi.org/10.3390/jcm9113465
APA StyleWatschinger, B., Watschinger, C., Reindl-Schwaighofer, R., Meyer, E. L., Deak, A. T., Hammer, T., Eigner, M., Sprenger-Mähr, H., Schneeberger, S., Cejka, D., Mayer, G., Oberbauer, R., Rosenkranz, A. R., & Kerschbaum, J. (2020). Impact of Timely Public Health Measures on Kidney Transplantation in Austria during the SARS-CoV-2 Outbreak—A Nationwide Analysis. Journal of Clinical Medicine, 9(11), 3465. https://doi.org/10.3390/jcm9113465