Prognostic Significance of Tumor Location in T2 Gallbladder Cancer: A Korea Tumor Registry System Biliary Pancreas (KOTUS-BP) Database Analysis

 , , and
, , and
Abstract
1. Introduction
2. Experimental Section
2.1. Patients and Study Design
2.2. Tumor Stage
2.3. Tumor Location
2.4. Operative Procedures
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Surgical Interventions and Postoperative Morbidity and Mortality
3.3. LN Metastasis
3.4. Recurrence
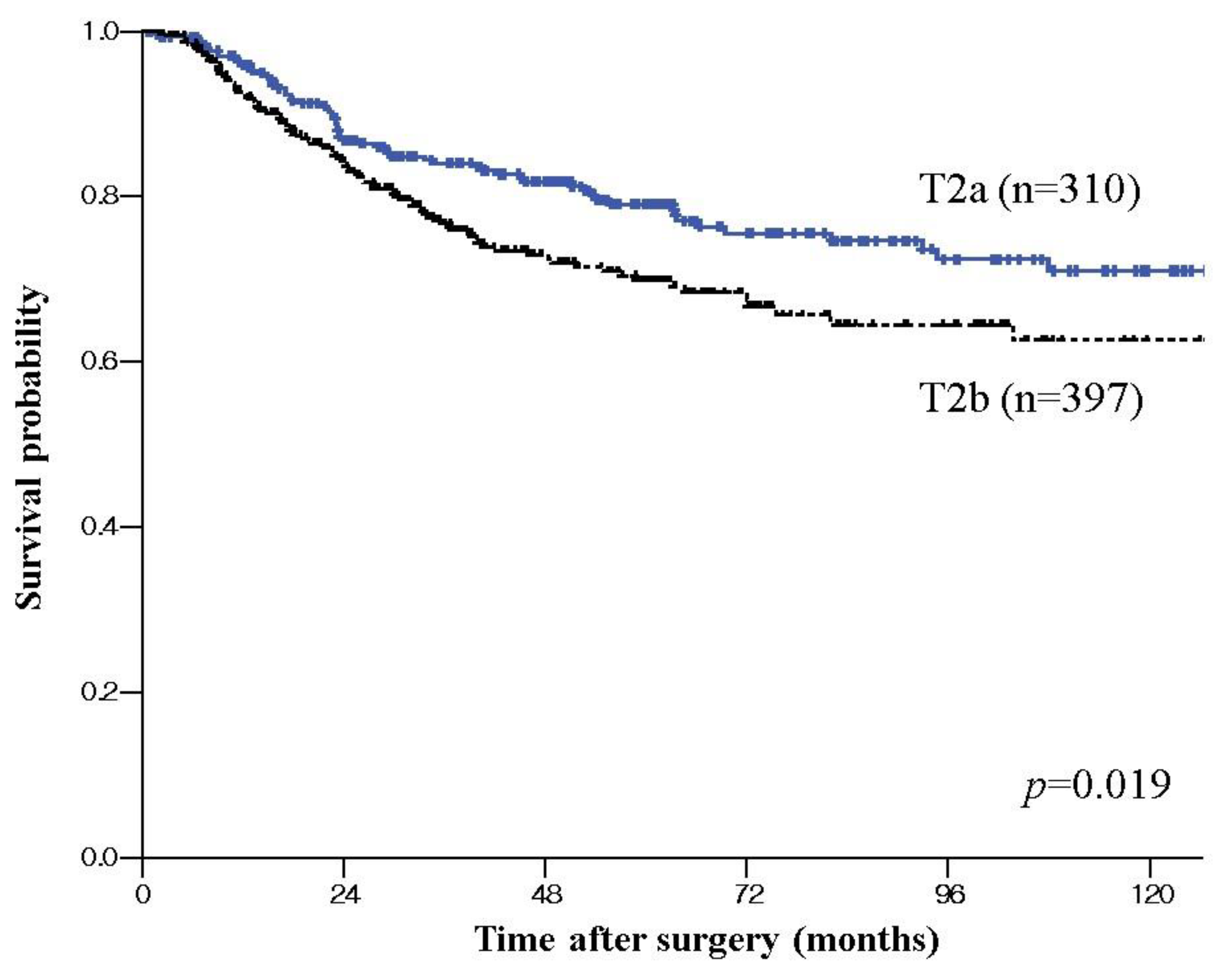
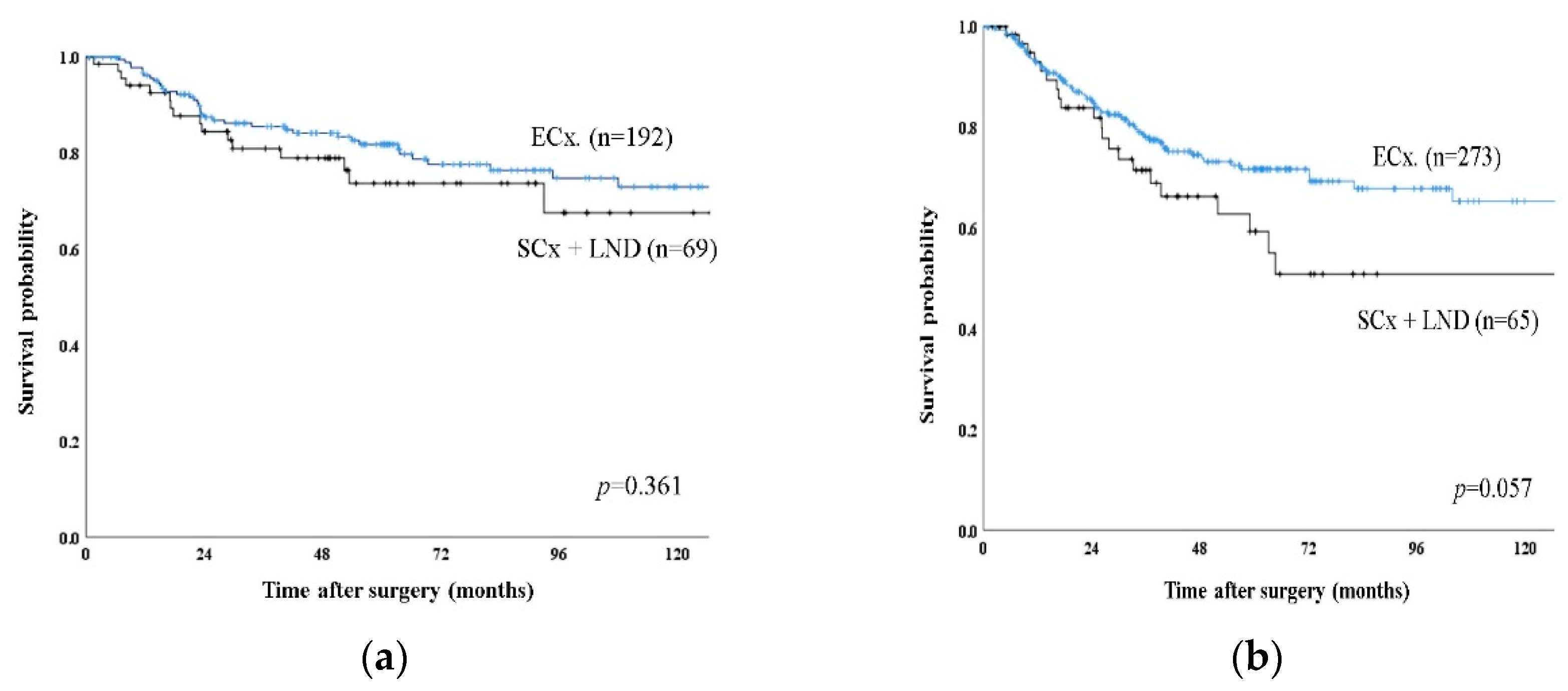
3.5. Long-Term Survival
3.6. Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shindoh, J.; de Aretxabala, X.; Aloia, T.A.; Roa, J.C.; Roa, L.; Zimmitti, G.; Javle, M.; Conrad, C.; Maru, D.M.; Aoki, T.; et al. Tumor location is a strong predictor of tumor progression and survival in T2 gallbladder cancer: An international multicenter study. Ann. Surg. 2015, 261, 733–739. [Google Scholar] [CrossRef]
- Lee, H.; Choi, D.W.; Park, J.Y.; Youn, S.; Kwon, W.; Heo, J.S.; Choi, S.H.; Jang, K.-T. Surgical strategy for T2 gallbladder cancer according to tumor location. Ann. Surg. Oncol. 2015, 22, 2779–2786. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.; Jang, J.Y.; Kang, M.J.; Chang, Y.R.; Shin, Y.C.; Chang, J.; Kim, S.-W. Effects of surgical methods and tumor location on survival and recurrence patterns after curative resection in patients with T2 gallbladder cancer. Gut Liver 2016, 10, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Park, T.J.; Ahn, K.S.; Kim, Y.H.; Kim, T.-S.; Hong, J.H.; Kang, K.J. The optimal surgical resection approach for T2 gallbladder carcinoma: Evaluating the role of surgical extent according to the tumor location. Ann. Surg. Treat. Res. 2018, 94, 135–141. [Google Scholar] [CrossRef]
- Lee, W.; Jeong, C.Y.; Jang, J.Y.; Kim, Y.H.; Roh, Y.H.; Kim, K.W.; Kang, S.H.; Yoon, M.H.; Seo, H.L.; Yun, S.P.; et al. Do hepatic-sided tumors require more extensive resection than peritoneal-sided tumors in patients with T2 gallbladder cancer? Results of a retrospective multicenter study. Surgery 2017, 162, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.K.; Lee, W.; Jang, J.Y.; Kim, H.J.; Kim, J.M.; Kwag, S.J.; Park, J.H.; Kim, J.Y.; Park, T.; Jeong, S.H.; et al. Validation of the oncologic effect of hepatic resection for T2 gallbladder cancer: A retrospective study. World J. Surg. Oncol. 2019, 17, 8. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA, 2017. [Google Scholar]
- Jensen, E.H.; Abraham, A.; Jarosek, S.; Habermann, E.B.; Al-Refaie, W.B.; Vickers, S.A.; Virnig, B.A.; Tuttle, T.M. Lymph node evaluation is associated with improved survival after surgery for early stage gallbladder cancer. Surgery 2009, 146, 706–711, discussion 711–713. [Google Scholar] [CrossRef]
- Downing, S.R.; Cadogan, K.A.; Ortega, G.; Oyetunji, T.A.; Siram, S.M.; Chang, D.C.; Ahuja, N.; Leffall, L.D., Jr.; Frederick, W.A.I. Early-stage gallbladder cancer in the surveillance, epidemiology, and end results database: Effect of extended surgical resection. Arch. Surg. 2011, 146, 734–738. [Google Scholar] [CrossRef]
- Goetze, T.O.; Paolucci, V. The prognostic impact of positive lymph nodes in stages T1 to T3 incidental gallbladder carcinoma: Results of the German Registry. Surg. Endosc. 2012, 26, 1382–1389. [Google Scholar] [CrossRef]
- Shirai, Y.; Wakai, T.; Sakata, J.; Hatakeyama, K. Regional lymphadenectomy for gallbladder cancer: Rational extent, technical details, and patient outcomes. World J. Gastroenterol. 2012, 18, 2775–2783. [Google Scholar] [CrossRef]
- Horiguchi, A.; Miyakawa, S.; Ishihara, S.; Miyazaki, M.; Ohtsuka, M.; Shimizu, H.; Sano, K.; Miura, F.; Ohta, T.; Kayahara, M.; et al. Gallbladder bed resection or hepatectomy of segments 4a and 5 for pT2 gallbladder carcinoma: Analysis of Japanese registration cases by the study group for biliary surgery of the Japanese society of hepato-biliary-pancreatic surgery. J. Hepatobiliary Pancreat. Sci. 2013, 20, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Kambayashi, M. Lymphatic and vascular systems of the gallbladder—with special reference to carcinoma of the gallbladder. Hokkaido Igaku Zasshi 1989, 64, 618–629. [Google Scholar] [PubMed]
- Nagahashi, M.; Shirai, Y.; Wakai, T.; Sakata, J.; Ajioka, Y.; Hatakeyama, K. Perimuscular connective tissue contains more and larger lymphatic vessels than the shallower layers in human gallbladders. World J. Gastroenterol. 2007, 13, 4480–4483. [Google Scholar] [CrossRef] [PubMed]
- Toge, K.; Sakata, J.; Hirose, Y.; Yuza, K.; Ando, T.; Soma, D.; Katada, T.; Miura, K.; Takizawa, K.; Kobayashi, T.; et al. Lymphatic spread of T2 gallbladder carcinoma: Regional lymphadenectomy is required independent of tumor location. Eur. J. Surg. Oncol. 2019, 45, 1446–1452. [Google Scholar] [CrossRef]
- Eckel, F.; Brunner, T.; Jelic, S.; Group, E.G.W. Biliary cancer: ESMO Clincal Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2011, 22, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Wedel, T.; Seidl, H.; Kreis, M.E.; Andresen, V.; Preiss, J.C.; Layer, P.; van der Voort, I. S3 guideline of the German society for digestive and metabolic diseases (DGVS) and the German society for neurogastroenterology and motility (DGNM) to the definition, pathophysiology, diagnosis and treatment of intestinal motility. Z. Gastroenterol. 2011, 49, 374–390. [Google Scholar] [CrossRef] [PubMed]
- Kondo, S.; Takada, T.; Miyazaki, M.; Miyakawa, S.; Tsukada, K.; Nagino, M.; Furuse, J.; Saito, H.; Tsuyuguchi, T.; Yamamoto, M.; et al. Guidelines for the management of biliary tract and ampullary carcinomas: Surgical treatment. J. Hepatobiliary Pancreat. Surg. 2008, 15, 41–54. [Google Scholar] [CrossRef]
- Lee, S.E.; Kim, K.S.; Kim, W.B.; Kim, I.-G.; Nah, Y.W.; Ryu, D.H.; Park, J.S.; Yoon, M.H.; Cho, J.Y.; Hong, T.H.; et al. Practical guidelines for the surgical treatment of gallbladder cancer. J. Korean Med. Sci. 2014, 29, 1333–1340. [Google Scholar] [CrossRef]
- Hezel, A.F.; Noel, M.S.; Allen, J.N.; Abrams, T.A.; Yurgelun, M.; Faris, J.E.; Goyal, L.; Clark, J.W.; Blaszkowsky, L.S.; Murphy, J.E.; et al. Phase II study of gemcitabine, oxaliplatin in combination with panitumumab in KRAS wild-type unresectable or metastatic biliary tract and gallbladder cancer. Br. J. Cancer 2014, 111, 430–436. [Google Scholar] [CrossRef]
- Stein, A.; Arnold, D.; Bridgewater, J.; Goldstein, D.; Jensen, L.H.; Klümpen, H.-J.; Lohse, A.W.; Nashan, B.; Primrose, J.; Schrum, S.; et al. Adjuvant chemotherapy with gemcitabine and cisplatin compared to observation after curative intent resection of cholangiocarcinoma and muscle invasive gallbladder carcinoma (ACTICCA-1 trial)—a randomized, multidisciplinary, multinational phase III trial. BMC Cancer 2015, 15, 564. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Thomas, C.R., Jr.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A phase II intergroup trial of adjuvant capecitabine and gemcitabine followed by radiotherapy and concurrent capecitabine in extrahepatic cholangiocarcinoma and gallbladder carcinoma. J. Clin. Oncol. 2015, 33, 2617–2622. [Google Scholar] [CrossRef] [PubMed]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | T2a (n = 310) | T2b (n = 397) | p-Value |
|---|---|---|---|
| Age (years) | 66 ± 11 | 67 ± 11 | 0.892 |
| Sex (M:F) | 1:1.4 | 1:1.2 | 0.413 |
| Combined Gallstone | 45 (14.5%) | 58 (14.6%) | 0.922 |
| Tumor size (cm) | 2.98 ± 1.83 | 3.39 ± 2.15 | 0.027 |
| Postoperative morbidity | 31 (10.0%) | 57 (14.3%) | 0.107 |
| Lymph node dissection | 261 (84.2%) | 338 (85.1%) | 0.857 |
| Lymph node metastasis | 77 (29.5%) | 128 (37.9%) | 0.032 |
| AJCC 8th N stage | 0.031 | ||
| N0 | 184 (70.5%) | 211 (62.4%) | |
| N1 | 72 (27.6%) | 109 (32.2%) | |
| N2 | 5 (1.9%) | 18 (5.3%) | |
| Histologic differentiation | 0.326 | ||
| Papillary, well differentiation | 116 (37.4%) | 125 (31.5%) | |
| Moderate differentiation | 131 (42.3%) | 193 (48.6%) | |
| Poor differentiation | 45 (14.5%) | 56 (14.1%) | |
| Lymphovascular invasion (yes) | 81 (36.5%) | 105 (36.2%) | 0.948 |
| Perineural invasion (yes) | 42 (19.7%) | 103 (36.9%) | <0.001 |
| Adjuvant chemotherapy (yes) | 65 (24.9%) | 119 (35.2%) | <0.001 |
| Recurrence Site | Total (n = 707) | T2a (n = 310) | T2b (n = 397) | p-Value |
|---|---|---|---|---|
| Total | 201 (28.4%) | 70 (22.6%) | 131 (33.0%) | 0.006 |
| Loco-regional | 56 (29.0%) | 15 (22.7%) | 41 (31.3%) | |
| Liver bed | 8 (14.3%) | 1 (6.7%) | 7 (17.1%) | |
| Common bile duct | 17 (30.4%) | 3 (20.0%) | 14 (34.1%) | |
| Regional lymph node | 23 (41.1%) | 8 (53.3%) | 15 (36.6%) | |
| Systemic | 137 (71.3%) | 51 (77.3%) | 86 (68.7%) | |
| Liver | 52 (38.0%) | 23 (45.1%) | 29 (33.7%) | |
| Lung | 22 (16.1%) | 5 (9.8%) | 17 (19.8%) | |
| Peritoneal seeding | 36 (26.3%) | 15 (29.4%) | 21 (24.4%) | |
| Para-aortic lymph node | 18 (13.1%) | 5 (9.8%) | 13 (15.1%) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Subgroup (n) | MST (mo) | p-Value | HR | 95% CI | p-Value | |
| T stage | pT2a (261) | 52 | 0.02 | 1.340 | 0.919–1.955 | 0.128 |
| pT2b (338) | 37 | |||||
| Lymph node metastasis | Yes (206) | 29 | <0.001 | 3.222 | 1.960–4.489 | <0.001 |
| No (393) | 62 | |||||
| Cellular differentiation | Well (193) | 50 | 0.055 | 1.738 | 0–0.2967 | 0.995 |
| Moderate/poor (379) | 40 | |||||
| Lymphovascular invasion | Yes (186) | 32 | <0.001 | 1.721 | 0.505–5.858 | 0.117 |
| No (326) | 50 | |||||
| Perineural invasion | Yes (145) | 31 | <0.001 | 1.454 | 0.482–4.387 | 0.406 |
| No (347) | 47 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.E.; Choi, Y.S.; Kim, Y.H.; Heo, J.S.; Jeong, C.-Y.; Lee, W.J.; Seo, H.I.; Yoon, Y.-S.; Jang, J.-Y. Prognostic Significance of Tumor Location in T2 Gallbladder Cancer: A Korea Tumor Registry System Biliary Pancreas (KOTUS-BP) Database Analysis. J. Clin. Med. 2020, 9, 3268. https://doi.org/10.3390/jcm9103268
Lee SE, Choi YS, Kim YH, Heo JS, Jeong C-Y, Lee WJ, Seo HI, Yoon Y-S, Jang J-Y. Prognostic Significance of Tumor Location in T2 Gallbladder Cancer: A Korea Tumor Registry System Biliary Pancreas (KOTUS-BP) Database Analysis. Journal of Clinical Medicine. 2020; 9(10):3268. https://doi.org/10.3390/jcm9103268
Chicago/Turabian StyleLee, Seung Eun, Yoo Shin Choi, Yong Hoon Kim, Jin Seok Heo, Chi-Young Jeong, Woo Jung Lee, Hyung Il Seo, Yoo-Seok Yoon, and Jin-Young Jang. 2020. "Prognostic Significance of Tumor Location in T2 Gallbladder Cancer: A Korea Tumor Registry System Biliary Pancreas (KOTUS-BP) Database Analysis" Journal of Clinical Medicine 9, no. 10: 3268. https://doi.org/10.3390/jcm9103268
APA StyleLee, S. E., Choi, Y. S., Kim, Y. H., Heo, J. S., Jeong, C.-Y., Lee, W. J., Seo, H. I., Yoon, Y.-S., & Jang, J.-Y. (2020). Prognostic Significance of Tumor Location in T2 Gallbladder Cancer: A Korea Tumor Registry System Biliary Pancreas (KOTUS-BP) Database Analysis. Journal of Clinical Medicine, 9(10), 3268. https://doi.org/10.3390/jcm9103268