HbA1c and Aortic Calcification Index as Noninvasive Predictors of Pre-Existing Histopathological Damages in Living Donor Kidney Transplantation

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Pathological Diagnosis
2.3. Recording and Assessment of Clinical Data
2.4. Aortic Calcification Index
2.5. Third Lumber Psoas Muscle Index
2.6. Statistical Analysis
3. Results
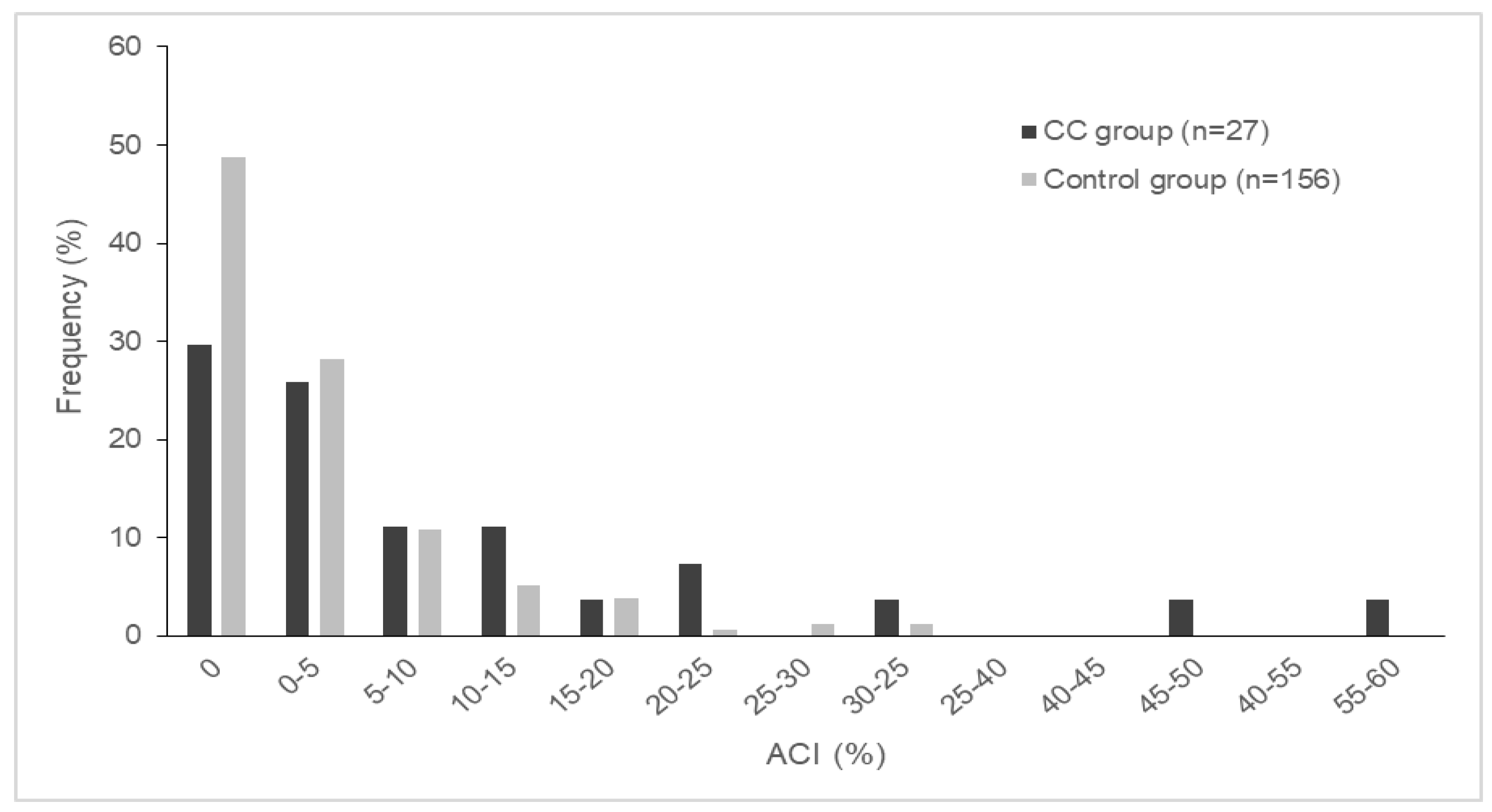
3.1. Donor Characteristics
3.2. Preoperative Predictors
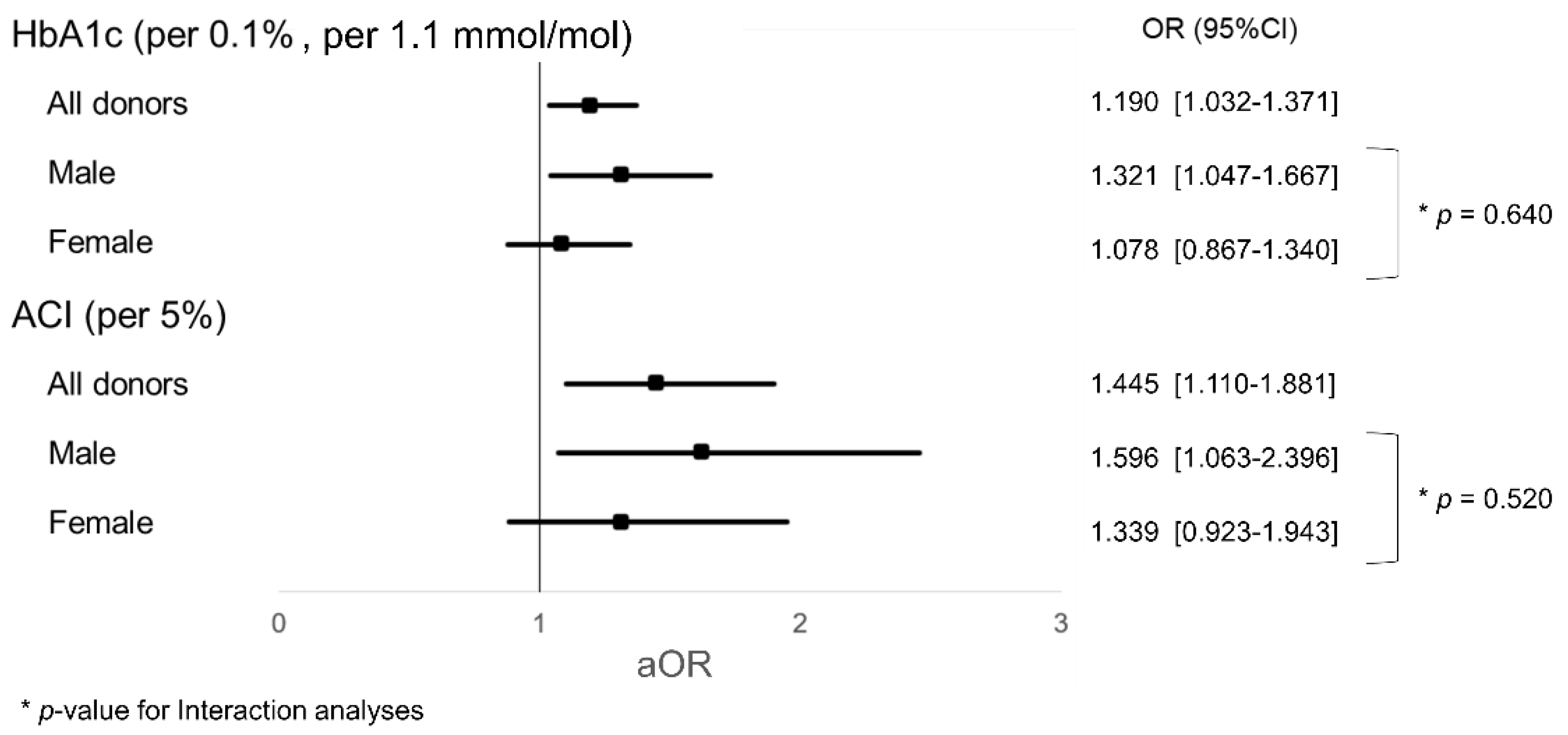
3.3. Interaction Analyses
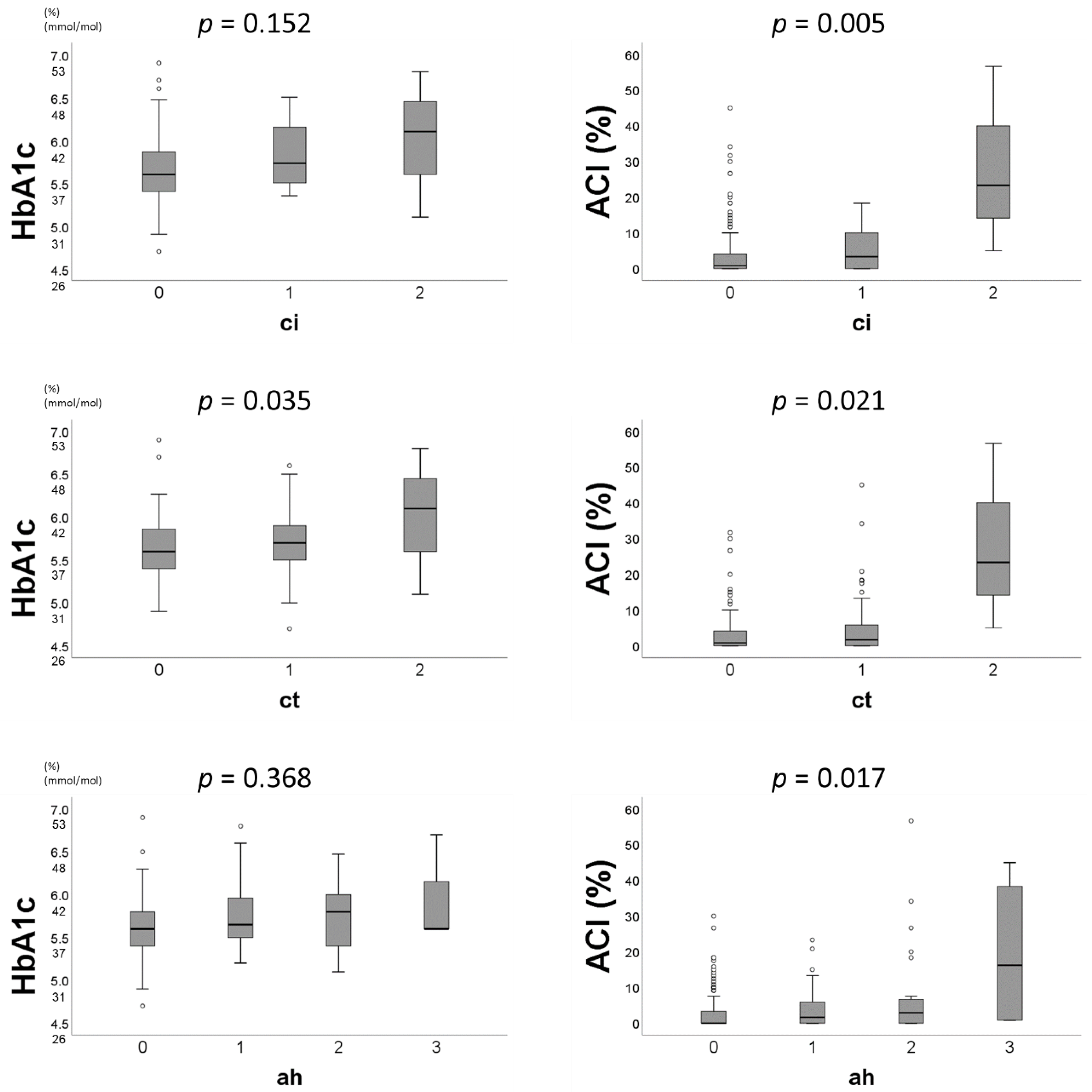
3.4. Distribution of Preoperative Predictors by Pathological Scores
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACI | Aortic calcification index |
| ah | Arteriolar hyalinosis |
| AUC | Area under the curve |
| CC | Chronic change |
| ci | Interstitial fibrosis |
| ct | Tubular atrophy |
| CT | Computed tomography |
| eGFR | estimated glomerular filtration rate |
| ESRD | End-stage renal disease |
| GFR | Glomerular filtration rate |
| HbA1c | Hemoglobin A1c |
| HU | Hounsfield unit |
| IFCC | International Federation of Clinical Chemistry and Laboratory Medicine |
| IF/TA | Interstitial fibrosis/tubular atrophy |
| JDS | Japan Diabetes Society |
| LDL | Low-density lipoprotein |
| NGSP | National Glycohemoglobin Standardization Program |
| OR | Odds ratio |
| PMI | Psoas muscle index |
| ROC | Receiver operating characteristic |
References
- Japanese Society for Clinical Renal Transplantation; The Japan Society for Transplantation. Annual Progress Report from the Japanese Renal Transplant Registry: Number of Renal Transplantations in 2018 and Follow-up Survey. Jpn. J. Transplant. 2019, 54, 61–80. [Google Scholar] [CrossRef]
- Mjoen, G.; Hallan, S.; Hartmann, A.; Foss, A.; Midtvedt, K.; Oyen, O.; Reisaeter, A.; Pfeffer, P.; Jenssen, T.; Leivestad, T.; et al. Long-term risks for kidney donors. Kidney Int. 2014, 86, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Muzaale, A.D.; Massie, A.B.; Wang, M.C.; Montgomery, R.A.; McBride, M.A.; Wainright, J.L.; Segev, D.L. Risk of end-stage renal disease following live kidney donation. JAMA 2014, 311, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.C.; Muzaale, A.D.; James, N.; Hoque, M.; Wang, J.M.; Montgomery, R.A.; Massie, A.B.; Hall, E.C.; Segev, D.L. Living kidney donors ages 70 and older: Recipient and donor outcomes. Clin. J. Am. Soc. Nephrol. 2011, 6, 2887–2893. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Delmonico, F. A Report of the Amsterdam Forum On the Care of the Live Kidney Donor: Data and Medical Guidelines. Transplantation 2005, 79, S53–S66. [Google Scholar]
- Noppakun, K.; Cosio, F.G.; Dean, P.G.; Taler, S.J.; Wauters, R.; Grande, J.P. Living donor age and kidney transplant outcomes. Am. J. Transpl. 2011, 11, 1279–1286. [Google Scholar] [CrossRef]
- Nishida, S.; Hidaka, Y.; Toyoda, M.; Kinoshita, K.; Tanaka, K.; Kawabata, C.; Hamanoue, S.; Inadome, A.; Yokomizo, H.; Takeda, A.; et al. Factors related to suboptimal recovery of renal function after living donor nephrectomy: A retrospective study. BMC Nephrol. 2019, 20, 403. [Google Scholar] [CrossRef]
- Roufosse, C.; Simmonds, N.; Clahsen-van Groningen, M.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasinska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef]
- Hommos, M.S.; Rule, A.D. Should We Always Defer Treatment of Kidney Disease When There Is Extensive Interstitial Fibrosis on Biopsy? Am. J. Nephrol. 2016, 44, 286–288. [Google Scholar] [CrossRef] [PubMed]
- Nangaku, M. Chronic hypoxia and tubulointerstitial injury: A final common pathway to end-stage renal failure. J. Am. Soc. Nephrol. 2006, 17, 17–25. [Google Scholar] [CrossRef]
- Fioretto, P.; Steffes, M.W.; Sutherland, D.E.; Mauer, M. Sequential renal biopsies in insulin-dependent diabetic patients: Structural factors associated with clinical progression. Kidney Int. 1995, 48, 1929–1935. [Google Scholar] [CrossRef] [PubMed]
- Zamami, R.; Kohagura, K.; Miyagi, T.; Kinjyo, T.; Shiota, K.; Ohya, Y. Modification of the impact of hypertension on proteinuria by renal arteriolar hyalinosis in nonnephrotic chronic kidney disease. J. Hypertens. 2016, 34, 2274–2279. [Google Scholar] [CrossRef]
- Tozawa, M.; Iseki, K.; Iseki, C.; Kinjo, K.; Ikemiya, Y.; Takishita, S. Blood pressure predicts risk of developing end-stage renal disease in men and women. Hypertension 2003, 41, 1341–1345. [Google Scholar] [CrossRef] [PubMed]
- Vupputuri, S.; Batuman, V.; Muntner, P.; Bazzano, L.A.; Lefante, J.J.; Whelton, P.K.; He, J. Effect of blood pressure on early decline in kidney function among hypertensive men. Hypertension 2003, 42, 1144–1149. [Google Scholar] [CrossRef] [PubMed]
- Yamagata, K.; Ishida, K.; Sairenchi, T.; Takahashi, H.; Ohba, S.; Shiigai, T.; Narita, M.; Koyama, A. Risk factors for chronic kidney disease in a community-based population: A 10-year follow-up study. Kidney Int. 2007, 71, 159–166. [Google Scholar] [CrossRef]
- Adler, A.I.; Stevens, R.J.; Manley, S.E.; Bilous, R.W.; Cull, C.A.; Holman, R.R. Development and progression of nephropathy in type 2 diabetes: The United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int. 2003, 63, 225–232. [Google Scholar] [CrossRef]
- Echouffo-Tcheugui, J.B.; Narayan, K.M.; Weisman, D.; Golden, S.H.; Jaar, B.G. Association between prediabetes and risk of chronic kidney disease: A systematic review and meta-analysis. Diabet Med. 2016, 33, 1615–1624. [Google Scholar] [CrossRef]
- Mänttäri, M.; Tiula, E.; Alikoski, T.; Manninen, V. Effects of hypertension and dyslipidemia on the decline in renal function. Hypertension 1995, 26, 670–675. [Google Scholar] [CrossRef]
- Schaeffner, E.S.; Kurth, T.; Curhan, G.C.; Glynn, R.J.; Rexrode, K.M.; Baigent, C.; Buring, J.E.; Gaziano, J.M. Cholesterol and the risk of renal dysfunction in apparently healthy men. J. Am. Soc. Nephrol. 2003, 14, 2084–2091. [Google Scholar]
- Peeters, M.J.; van den Brand, J.A.; van Zuilen, A.D.; Koster, Y.; Bots, M.L.; Vervloet, M.G.; Blankestijn, P.J.; Wetzels, J.F. Abdominal aortic calcification in patients with CKD. J. Nephrol. 2017, 30, 109–118. [Google Scholar] [CrossRef]
- Souza, V.A.; Oliveira, D.; Barbosa, S.R.; Correa, J.; Colugnati, F.A.B.; Mansur, H.N.; Fernandes, N.; Bastos, M.G. Sarcopenia in patients with chronic kidney disease not yet on dialysis: Analysis of the prevalence and associated factors. PLoS ONE 2017, 12, e0176230. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, M.; Charchar, F.J.; Maric, C.; McClure, J.; Crawford, L.; Grzeszczak, W.; Sattar, N.; Zukowska-Szczechowska, E.; Dominiczak, A.F. Glomerular hyperfiltration: A new marker of metabolic risk. Kidney Int. 2007, 71, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Helal, I.; Fick-Brosnahan, G.M.; Reed-Gitomer, B.; Schrier, R.W. Glomerular hyperfiltration: Definitions, mechanisms and clinical implications. Nat. Rev. Nephrol. 2012, 8, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, T.; Hariharan, S.; Alon, U.S.; McCarthy, E.T.; Sharma, R.; El-Meanawy, A.; Savin, V.J.; Sharma, M. Hyperfiltration-mediated Injury in the Remaining Kidney of a Transplant Donor. Transplantation 2018, 102, 1624–1635. [Google Scholar] [CrossRef]
- Morozumi, K. Clinical practice guidelines for renal transplant donors and recipients in Japan. Jpn. J. Transplant. 2014, 49, 410–416. [Google Scholar] [CrossRef]
- Sakai, K.; Oguchi, H.; Muramatsu, M.; Shishido, S. Protocol graft biopsy in kidney transplantation. Nephrol. (Carlton) 2018, 23 (Suppl. S2), 38–44. [Google Scholar] [CrossRef]
- Kashiwagi, A.; Kasuga, M.; Araki, E.; Oka, Y.; Hanafusa, T.; Ito, H.; Tominaga, M.; Oikawa, S.; Noda, M.; Kawamura, T.; et al. International clinical harmonization of glycated hemoglobin in Japan: From Japan Diabetes Society to National Glycohemoglobin Standardization Program values. J. Diabetes Investig. 2012, 3, 39–40. [Google Scholar] [CrossRef]
- Sacks, D.B. Measurement of hemoglobin A(1c): A new twist on the path to harmony. Diabetes Care 2012, 35, 2674–2680. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Taniwaki, H.; Ishimura, E.; Tabata, T.; Tsujimoto, Y.; Shioi, A.; Shoji, T.; Inaba, M.; Inoue, T.; Nishizawa, Y. Aortic calcification in haemodialysis patients with diabetes mellitus. Nephrol. Dial. Transpl. 2005, 20, 2472–2478. [Google Scholar] [CrossRef]
- Furusawa, K.; Takeshita, K.; Suzuki, S.; Tatami, Y.; Morimoto, R.; Okumura, T.; Yasuda, Y.; Murohara, T. Assessment of abdominal aortic calcification by computed tomography for prediction of latent left ventricular stiffness and future cardiovascular risk in pre-dialysis patients with chronic kidney disease: A single center cross-sectional study. Int. J. Med. Sci. 2019, 16, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, Y.; Kaido, T.; Okumura, S.; Kobayashi, A.; Hammad, A.; Tamai, Y.; Inagaki, N.; Uemoto, S. Proposal for new diagnostic criteria for low skeletal muscle mass based on computed tomography imaging in Asian adults. Nutrition 2016, 32, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- Shehab-Eldin, W.; Shoeb, S.; Khamis, S.; Salah, Y.; Shoker, A. Susceptibility to insulin resistance after kidney donation: A pilot observational study. Am. J. Nephrol. 2009, 30, 371–376. [Google Scholar] [CrossRef]
- Singleton, J.R.; Smith, A.G.; Russell, J.W.; Feldman, E.L. Microvascular complications of impaired glucose tolerance. Diabetes 2003, 52, 2867–2873. [Google Scholar] [CrossRef]
- Okamoto, M.; Suzuki, T.; Fujiki, M.; Nobori, S.; Ushigome, H.; Sakamoto, S.; Yoshimura, N. The consequences for live kidney donors with preexisting glucose intolerance without diabetic complication: Analysis at a single Japanese center. Transplantation 2010, 89, 1391–1395. [Google Scholar] [CrossRef]
- Okada, T.; Nagao, T.; Matsumoto, H.; Nagaoka, Y.; Wada, T.; Nakao, T. Histological predictors for renal prognosis in diabetic nephropathy in diabetes mellitus type 2 patients with overt proteinuria. Nephrol. (Carlton) 2012, 17, 68–75. [Google Scholar] [CrossRef]
- Mise, K.; Hoshino, J.; Ubara, Y.; Sumida, K.; Hiramatsu, R.; Hasegawa, E.; Yamanouchi, M.; Hayami, N.; Suwabe, T.; Sawa, N.; et al. Renal prognosis a long time after renal biopsy on patients with diabetic nephropathy. Nephrol. Dial. Transpl. 2014, 29, 109–118. [Google Scholar] [CrossRef]
- Guthoff, M.; Nadalin, S.; Fritsche, A.; Königsrainer, A.; Häring, H.U.; Heyne, N. The Medically Complex Living Kidney Donor: Glucose Metabolism as Principal Cause of Donor Declination. Ann. Transpl. 2016, 21, 39–45. [Google Scholar] [CrossRef]
- Yoon, Y.E.; Han, W.K.; Lee, H.H.; Chang, M.Y.; Huh, K.H.; Jung, D.C.; Kim, Y.S.; Oh, Y.T. Abdominal Aortic Calcification in Living Kidney Donors. Transpl. Proc. 2016, 48, 720–724. [Google Scholar] [CrossRef]
- Bahous, S.A.; Stephan, A.; Blacher, J.; Safar, M. Cardiovascular and renal outcome in recipients of kidney grafts from living donors: Role of aortic stiffness. Nephrol. Dial. Transpl. 2012, 27, 2095–2100. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.H.; Wojciechowski, D.; Chandran, S.; Yeh, B.M.; Park, M.; Westphalen, A.; Wang, Z.J. Prevalence of abdominal aortic calcifications in older living renal donors and its effect on graft function and histology. Transpl. Int. 2015, 28, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Choi, S.R.; Choi, M.J.; Kim, S.G.; Lee, Y.K.; Noh, J.W.; Kim, H.J.; Song, Y.R. Prevalence of and factors associated with sarcopenia in elderly patients with end-stage renal disease. Clin. Nutr. 2014, 33, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Garonzik-Wang, J.M.; Govindan, P.; Grinnan, J.W.; Liu, M.; Ali, H.M.; Chakraborty, A.; Jain, V.; Ros, R.L.; James, N.T.; Kucirka, L.M.; et al. Frailty and delayed graft function in kidney transplant recipients. Arch. Surg. 2012, 147, 190–193. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Law, A.; King, E.; Orandi, B.; Salter, M.; Gupta, N.; Chow, E.; Alachkar, N.; Desai, N.; Varadhan, R.; et al. Frailty and mortality in kidney transplant recipients. Am. J. Transpl. 2015, 15, 149–154. [Google Scholar] [CrossRef]
- McAdams-DeMarco, M.A.; Law, A.; Salter, M.L.; Chow, E.; Grams, M.; Walston, J.; Segev, D.L. Frailty and early hospital readmission after kidney transplantation. Am. J. Transpl. 2013, 13, 2091–2095. [Google Scholar] [CrossRef]
- Streja, E.; Molnar, M.Z.; Kovesdy, C.P.; Bunnapradist, S.; Jing, J.; Nissenson, A.R.; Mucsi, I.; Danovitch, G.M.; Kalantar-Zadeh, K. Associations of pretransplant weight and muscle mass with mortality in renal transplant recipients. Clin. J. Am. Soc. Nephrol. 2011, 6, 1463–1473. [Google Scholar] [CrossRef]
- Tziomalos, K.; Giampatzis, V.; Baltatzi, M.; Efthymiou, E.; Psianou, K.; Papastergiou, N.; Magkou, D.; Bougatsa, V.; Savopoulos, C.; Hatzitolios, A.I. Sex-specific differences in cardiovascular risk factors and blood pressure control in hypertensive patients. J. Clin. Hypertens. (Greenwich) 2014, 16, 309–312. [Google Scholar] [CrossRef]
- Sullivan, J.C.; Gillis, E.E. Sex and gender differences in hypertensive kidney injury. Am. J. Physiol. Ren. Physiol. 2017, 313, F1009–F1017. [Google Scholar] [CrossRef]
- Muiesan, M.L.; Ambrosioni, E.; Costa, F.V.; Leonetti, G.; Pessina, A.C.; Salvetti, M.; Trimarco, B.; Volpe, M.; Pontremoli, R.; Deferrari, G.; et al. Sex differences in hypertension-related renal and cardiovascular diseases in Italy: The I-DEMAND study. J. Hypertens. 2012, 30, 2378–2386. [Google Scholar] [CrossRef]
- Dols, L.F.; Kok, N.F.; Roodnat, J.I.; Tran, T.C.; Terkivatan, T.; Zuidema, W.C.; Weimar, W.; Ijzermans, J.N. Living kidney donors: Impact of age on long-term safety. Am. J. Transpl. 2011, 11, 737–742. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, M.; Yamanaga, S.; Kawabata, C.; Hidaka, Y.; Inadome, A.; Arakane, F.; Uekihara, S.; Seishi, I. Long-term safety of living kidney donors aged 60 and older. Transpl. Proc. 2014, 46, 318–320. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Donors (n = 183) | Chronic Change (CC) (n = 27) | Control (n = 156) | p Value | |
|---|---|---|---|---|
| Sex: male (%) | 65 (35.3) | 13 (48.1) | 52 (33.3) | 0.138 |
| Age (years) | 58 (51.0-65.0) | 60 (52.0–69.0) | 58 (50.0–65.0) | 0.174 |
| Tobacco use, n (%) | 0.035 | |||
| Nonsmoker | 102 (55.4) | 10 (37.0) | 92 (59.0) | |
| Current smoker | 32 (17.4) | 9 (33.3) | 23 (14.7) | |
| Ex-smoker | 18 (9.8) | 3 (11.1) | 14 (9.0) | |
| BP (mmHg) | 124 (115.0–136.0) | 124 (118.0–133.0) | 123 (114.3–136.8) | 0.381 |
| Hypertension, n (%) | 59 (32.1) | 11 (40.7) | 48 (30.8) | 0.306 |
| HbA1c (%) | 5.6 (5.4–5.9) | 5.7 (5.5–6.1) | 5.6 (5.4–5.8) | 0.057 |
| (mmol/mol) | 38.0 (36.0–41.0) | 39.0 (37.0–43.0) | 38.0 (36.0–40.0) | |
| Uric acid (mg/dl) | 4.9 (4.2–5.7) | 5.4 (4.6–6.3) | 4.8 (4.1–5.6) | 0.029 |
| LDL (mg/dl) | 120 (102.0–138.0) | 123. (101.0–137.0) | 118 (103.3–138.8) | 0.766 |
| ACI (%) | 0.83 (0.0–5.0) | 3.33 (0.0–13.3) | 0.83 (0.0–4.2) | 0.009 |
| BMI (kg/m2) | 22.9 (20.9–25.1) | 22.7 (21.5–25.4) | 22.9 (20.8–24.9) | 0.473 |
| PMI (cm2/m2) | 4.40 (3.69–5.57) | 4.68 (3.72–5.68) | 4.36 (3.69–5.56) | 0.511 |
| eGFR (ml/min/1.73m2) | 81.1 (73.0–91.8) | 86.2 (74.0–94.7) | 81.1 (73.0–91.6) | 0.386 |
| ci, n (%) | <0.001 | |||
| 0 | 160 (87.4) | 18 (66.7) | 142 (91.0) | |
| 1 | 20 (10.9) | 6 (22.2) | 14 (9.0) | |
| 2 | 3 (1.6) | 3 (11.1) | 0 (0) | |
| 3 | 0 (0) | 0 (0) | 0 (0) | |
| ct, n (%) | <0.001 | |||
| 0 | 114 (62.3) | 1 (3.7) | 113 (72.4) | |
| 1 | 66 (36.1) | 23 (85.2) | 43 (27.6) | |
| 2 | 3 (1.6) | 3 (11.1) | 0 (0) | |
| 3 | 0 (0) | 0(0) | 0 (0) | |
| ci + ct ≥ 1, n (%) | 71 (38.8) | 27 (100) | 44 (28.2) | <0.001 |
| ah, n (%) | <0.001 | |||
| 0 | 123 (67.2) | 0 (0) | 123 (78.8) | |
| 1 | 30 (16.4) | 13 (48.1) | 17 (10.9) | |
| 2 | 26 (14.2) | 13 (48.1) | 13 (8.3) | |
| 3 | 4 (2.2) | 1 (3.7) | 3 (1.9) |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| OR (95%CI) | p Value | OR (95%CI) | p Value | |
| Sex (ref. female) | 0.538 (0.236–1.229) | 0.141 | ||
| Age (years, per 1) | 1.030 (0.987–1.076) | 0.176 | ||
| Tobacco use | 1.704 (0.945–3.073) | 0.076 | 1.485 (0.769–2.868) | 0.239 |
| BP (mmHg, per 1) | 1.013 (0.987–1.039) | 0.343 | ||
| Hypertension | 1.547 (0.668–3.582) | 0.309 | ||
| HbA1c (%, per 0.1) (mmol/mol, per 1.1) | 1.144 (1.023–1.278) | 0.018 | 1.190 (1.032–1.371) | 0.016 |
| Uric acid (mg/dl, per 1) | 1.369 (1.011–1.853) | 0.042 | 1.087 (0.747–1.583) | 0.663 |
| LDL (mg/dl, per 1) | 1.001 (0.988–1.015) | 0.843 | ||
| ACI (%, per 5) | 1.413 (1.132–1.763) | 0.002 | 1.445 (1.110–1.881) | 0.006 |
| BMI (kg/m2, per 1) | 1.050 (0.918–1.201) | 0.473 | ||
| PMI (cm2/m2, per 1) | 1.032 (0.806–1.323) | 0.801 | ||
| eGFR (ml/min/1.73m2, per 1) | 1.010 (0.983–1.037) | 0.483 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, K.; Yamanaga, S.; Hidaka, Y.; Nishida, S.; Kinoshita, K.; Kaba, A.; Ishizuka, T.; Hamanoue, S.; Okumura, K.; Kawabata, C.; et al. HbA1c and Aortic Calcification Index as Noninvasive Predictors of Pre-Existing Histopathological Damages in Living Donor Kidney Transplantation. J. Clin. Med. 2020, 9, 3266. https://doi.org/10.3390/jcm9103266
Tanaka K, Yamanaga S, Hidaka Y, Nishida S, Kinoshita K, Kaba A, Ishizuka T, Hamanoue S, Okumura K, Kawabata C, et al. HbA1c and Aortic Calcification Index as Noninvasive Predictors of Pre-Existing Histopathological Damages in Living Donor Kidney Transplantation. Journal of Clinical Medicine. 2020; 9(10):3266. https://doi.org/10.3390/jcm9103266
Chicago/Turabian StyleTanaka, Kosuke, Shigeyoshi Yamanaga, Yuji Hidaka, Sho Nishida, Kohei Kinoshita, Akari Kaba, Toshinori Ishizuka, Satoshi Hamanoue, Kenji Okumura, Chiaki Kawabata, and et al. 2020. "HbA1c and Aortic Calcification Index as Noninvasive Predictors of Pre-Existing Histopathological Damages in Living Donor Kidney Transplantation" Journal of Clinical Medicine 9, no. 10: 3266. https://doi.org/10.3390/jcm9103266
APA StyleTanaka, K., Yamanaga, S., Hidaka, Y., Nishida, S., Kinoshita, K., Kaba, A., Ishizuka, T., Hamanoue, S., Okumura, K., Kawabata, C., Toyoda, M., Takeda, A., Miyata, A., Kashima, M., & Yokomizo, H. (2020). HbA1c and Aortic Calcification Index as Noninvasive Predictors of Pre-Existing Histopathological Damages in Living Donor Kidney Transplantation. Journal of Clinical Medicine, 9(10), 3266. https://doi.org/10.3390/jcm9103266