Abstract
Pulmonary rehabilitation (PR) improves lower-limb muscle function in patients with chronic obstructive pulmonary disease (COPD). However, it remains unclear whether patients improve gait characteristics, in particular stride-to-stride fluctuations that are associated with fall risks. This study aims to identify whether, and to what extent, PR affects positively gait characteristics in COPD. In this prospective observational study, 44 COPD patients (aged: 62 ± 7 years; Forced expiratory volume in 1 s 56 ± 20% predicted) performed self-paced, treadmill 6-min-walk tests (Gait Real-time Analysis Interactive Lab) before and after PR, while spatiotemporal parameters and center of mass position were recorded (100 Hz, Vicon Nexus). Standard deviation, coefficient of variation, predictability (sample entropy), and consistency in organization (local divergence exponent) were calculated. Sub-analysis was performed to identify gait differences between good and poor responders (<30 m change in a 6-min-walk distance). Patients demonstrated shorter stride times (p = 0.001) and improved lower-limb muscle function (p < 0.001) following PR. The good responders had a greater increase in stride length (p < 0.001) and a greater decrease in stride time (p < 0.001) compared to the poor responders. Current PR improved stride time in patients, while movement patterns within stride-to-stride fluctuations did not change. Training programs specifically targeting balance issues and gait function may be beneficial in improving gait characteristics in COPD.
Keywords:
gait variability; locomotion; lung disease; entropy; Lyapunov exponent; 3D motion analysis 1. Introduction
Walking has been reported as a problematic activity in daily life in patients with chronic obstructive pulmonary disease (COPD) [1,2]. Patients with COPD are characterized by gait alterations as compared to healthy older adults [3,4,5,6,7]. These gait alterations, in particular changes in the inherent stride-to-stride fluctuations, have been associated with non-communicable diseases [8,9] and falls in the aging population [10,11,12,13]. Moreover, stride-to-stride fluctuations may represent the capability of the locomotor system to make flexible adaptations during walking, characterized by a healthy amount of, and patterns within, these fluctuations [14]. Alterations in the amount and patterns of stride-to-stride fluctuations, whether too rigid or too random, are associated with aging, disease and falls [6,9,10,15] in many cases. In addition, gait deficits have been suggested to be an intrinsic risk factor for fall risk in COPD [16], indicating the clinical value of gait assessment in COPD. Improved insight into gait deficits in patients with COPD may direct future training programs focusing on gait function.
Gait function has been associated with muscle capacity in many older adults, suggesting a link between lower-limb muscle weakness and altered gait [17,18]. Exercise training has a beneficial effect on gait characteristics in older adults, including increased walking speed, cadence, stride length and shorter stride times [19]. Lower-limb muscle dysfunction and impaired exercise capacity are often reported in COPD [3,20]. However, pulmonary rehabilitation (PR) has proven to be an effective intervention for improving lower-limb muscle function and exercise capacity in patients with COPD [21,22,23]. Consequently, PR may have beneficial effects on gait characteristics in patients with COPD. However, whether and to what extent PR improves gait characteristics in patients with COPD is currently unknown. In addition, improvements in gait characteristics may differ between patients with COPD as their responses to PR are differential [24,25].
Within PR for COPD, the 6-min-walk test (6MWT) is used to evaluate response to treatment [26]. It has been shown that the 6-min-walk distance (6MWD) and gait characteristics can be obtained during a self-paced, treadmill 6MWT in COPD [4,27]. In the present study, we aimed to identify whether a comprehensive PR program affects gait characteristics in patients with COPD during a self-paced, treadmill 6MWT. Patients with COPD are able to walk faster during the 6MWT after PR [26]. Consequently, it is hypothesized that stride length will increase, whereas stride time and step width will decrease. In addition, we hypothesized that the amount of stride-to-stride fluctuations will decrease, and the patterns within stride-to-stride fluctuations will be less predictable and more consistent in the organization after PR, resulting in improved movement patterns. Response to PR is heterogeneous in COPD, we therefore hypothesized that good responders will demonstrate more improvements in gait characteristics as compared to poor responders.
2. Experimental Section
2.1. Study Population
This study included 44 patients with COPD who were referred for a PR program in the specialized rehabilitation center CIRO in Horn, The Netherlands. COPD diagnosis was diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, including post-bronchodilator spirometry (MasterScreen Body, Carefusion, Houten, The Netherlands) [28]. Patients with COPD were eligible if they were between 40–85 years of age and clinically stable evaluated by the physician. In addition, electrocardiography was conducted during pre-rehabilitation assessment and evaluated by the physician. Patients were excluded when they presented other lung diseases (e.g., asthma, lung cancer, sarcoidosis, tuberculosis or lung fibrosis), neuromuscular or orthopedic ailments affecting their gait, and/or if they used supplemental oxygen and/or walking aids. The study was approved by the Medical Research Ethics Committees United, The Netherlands (M13-1374) and registered in the Dutch Trial Registers (NTR4421). This study complied with the Declaration of Helsinki. All patients gave written informed consent prior to participating this study.
2.2. Study Design
This was a prospective, observational trial. Patients underwent a routine 3-day pre-rehabilitation assessment [29], in which patients performed, amongst other things, a maximal incremental cycle test during which peak work rate was determined. Patients performed a constant work rate test at 75% of the determined peak work rate and regular 6MWTs. In addition, a careful characterization of the extra-pulmonary features and comorbidities of patients with COPD were performed, which determined the application of various treatments: physical exercise training, occupational therapy, dietary counselling, psychosocial counselling, education and exacerbation management.
The pre-rehabilitation assessment was followed by a PR program in line with the American Thoracic Society/European Respiratory Society Statement on pulmonary rehabilitation [23]. PR consisted of 40 sessions that could be offered inpatient (8 weeks for 5 days/week) or outpatient (8 weeks for 3 days/week; followed by 8 weeks for 2 days/week). Physical exercise training was the cornerstone of the PR program, comprising of exercises to strengthen muscle groups in the upper and lower extremities, treadmill walking, and stationary cycling. All exercises were performed at moderate-to-high intensity to obtain an overload training stimulus, conform the Frequency, Intensity, Time, Type (FITT) principle as described by the American College of Sports Medicine [30]. The training intensity increased during the PR period, based on dyspnea and fatigue symptom scores. In addition, all patients underwent flexibility exercises, general physical exercise for lower and upper extremities, and daily supervised 30-min outdoor walks [25]. The program was implemented by an interdisciplinary team including a chest physician, respiratory nurse, dietician, occupational therapist, physiotherapist, psychologist, and social worker.
Finally, a 2-day routine outcome assessment was conducted to evaluate the effects of the PR program for each patient. The response of PR on functional exercise capacity was assessed using the overground 6MWT [26]. Functional mobility was assessed using the Timed Up and Go test (TUG test) [31]. Body composition was assessed using dual energy X-ray absorptiometry (Prodigy, DEXAtech Benelux B.V., Ridderkerk, The Netherlands) [32]. Quadriceps muscle function (peak strength and endurance) was evaluated with a Biodex system 3 (Biodex Medical Systems Inc., New York, NY, USA). Patients performed thirty volitional maximal knee extensions at an angular velocity of 90° per second, while seated upright and with the hip joint in 90° of flexion [33].
2.3. Experimental Setup
Before and after PR, patients were instructed to walk on a split-belt instrumented treadmill within a virtual reality environment of a hallway (Gait Real-time Analysis Interactive Lab, GRAIL, Motek Medical B.V., The Netherlands). A Vicon motion tracking system with 10 Bonita cameras (Vicon Nexus, Oxford, UK) was used to track markers at 100 Hz [4]. These markers were placed on anatomical landmarks of the patient, according to the Human Body Model of the lower-limb (HBM1) [34]. Force plate data were sampled at 1000 Hz in synchronization with the motion capture system. Self-paced treadmill walking was enabled via a built-in controller algorithm that regulates the belt’s speed, as described in [4]. Patients performed one familiarization session. Then, two GRAIL-based 6MWTs were performed between pre-rehabilitation assessment and the first week of PR. Perceived dyspnea and fatigue (Borg scale), heart rate and pulse oxygen saturation levels were measured prior and post each 6MWT [27]. Patients performed two additional GRAIL-based 6MWTs between the last week of PR and the outcome assessment.
2.4. Data Analyses
The GRAIL-based 6MWT with the longest walk distance for each subject in pre and post PR was used for analyses. The first 60 s (to minimize start-up effects) and the last 15 s (to minimize deceleration effects of the treadmill) were excluded. Marker and force plate date were processed in custom MATLAB software (Mathworks Inc., Natick, MA, USA), as previously described [4].
All data-analysis of gait was performed on 444 consecutive steps per trial, based on the lowest number of steps of all GRAIL-based 6MWTs (range 444–684). Gait characteristics can be evaluated by computing spatiotemporal gait parameters (stride time, stride length and step width) and movement patterns of the center of mass of the subject’s body. Stride time was calculated as the time from one heel contact to the next ipsilateral heel contact. Stride length was defined as the distance between the toe marker and the ipsilateral toe marker at each heel contact in the anteroposterior direction, accounted for treadmill speed. Step width was defined as the distance between the toe markers in mediolateral direction between both feet at heel strike. The center of mass velocity (CoMvel) was computed using the position of the four pelvis markers.
The amount of stride-to-stride fluctuations in gait parameters was quantified by the standard deviation and coefficient of variation of spatiotemporal gait parameters (CoV = (standard deviation/mean)). Increased standard deviation and CoV values reflect a disturbed gait, as has been found in aging and disease [15].
The patterns within stride-to-stride fluctuations were assessed using various measures, including sample entropy and local divergence exponent (See Supplementary Materials for further description of the calculation of these measures) [8,35,36]. In short, sample entropy is a measure of predictability in the time series [36]. Sample entropy was calculated using m = 2, r = 0.2 and n = 444. Reduced sample entropy values reflect a more predictable gait pattern, which has been associated with a less healthy locomotor system [37]. Stride time sample entropy seemed to be a product of the parameter selection, therefore only stride length and step width sample entropy were reported.
The CoMvel was subjected to consistency analysis, in which the local divergence exponent is calculated. The method to compute this has been described elsewhere [35]. Increased local divergent exponents reflected less consistent organization of movement patterns of the patient during walking, which has been found in falls and disease [9,10,35]. Briefly, the center of mass velocity time series was reconstructed into a multidimensional space and the distances between these points were calculated as a function of time and averaged over all data points to obtain the average logarithmic rate of divergence. The slope of the divergence curve provided an estimate of the local divergence exponent, which quantifies the separation of the center of mass trajectories over time.
2.5. Statistics
Data are presented as mean difference (95% Confidence Interval) unless otherwise stated. Differences in the 6MWT outcome parameters and gait characteristics between pre and post PR were compared using either paired sample T-tests or nonparametric Wilcoxon signed-rank tests. A sub-analysis was performed on good and poor responders. The minimal important difference of 30 m has been used to differentiate poor responders (<30 m improvement) and good responders (≥30 m improvement) to PR in the GRAIL-based 6MWT [26,38]. Either independent sample T-tests or nonparametric Mann–Whitney U tests were conducted to assess the differences between poor responders and good responders at baseline and the amount of changes after PR. All statistical analyses were performed in SPSS Statistics software 22.0 (International Business Machines Corporation, New York, NY, USA). The level of significance for all analyses was set at p ≤ 0.01.
3. Results
3.1. Baseline Subject Characteristics
Patients had mild to severe COPD (Table 1). Mean body mass index (BMI) was 26.9 ± 5.2 kg/m2. Patients performed the TUG test in 8.8 ± 1.3 s (Table 2). Mean quadriceps muscle strength was 71 ± 14% predicted. Patients walked 512 ± 67 m during the best overground 6MWT, corresponding to 80 ± 10% predicted, and 506 ± 75 m during the best pre-rehabilitation GRAIL-based 6MWT (Table 3). Most patients achieved their largest distance during the second 6MWT in both overground and GRAIL setting, 68% and 66%, respectively.

Table 1.
Patient demographic characteristics at baseline.
Table 2.
Clinical outcomes before and after pulmonary rehabilitation.
Table 3.
The 6MWT outcomes and gait parameters during the GRAIL-based 6MWT before and after pulmonary rehabilitation.
3.2. Changes after Pulmonary Rehabilitation
Fat-free mass and fat-free mass index, quadriceps muscle strength and endurance, and overground 6MWD increased significantly after PR (Table 2). The GRAIL-based 6MWD increased with 30 m after PR (95% CI (95% Confidence Interval): 14–46 m, p < 0.001; Table 3). Mean stride time reduced after PR (mean difference (MD): −0.02 s, 95% CI: −0.03–0.01 s, p = 0.001). Patients with COPD did not demonstrate significant changes in the standard deviation, CoV or predictability of spatiotemporal gait parameters; no change in consistency in the organization of center of mass patterns was found after PR.
3.3. Good versus Poor Responders
Twenty-four patients (55%) achieved an improvement of 30 m or more on the GRAIL-based 6MWT, which qualified them as good responders. At baseline, no differences in 6MWT outcomes and gait characteristics were found between good and poor responders, except for mean step width, which was significantly lower in the good responders at baseline (Table 3 and Table 4). The good responders had a significantly greater improvement in 6MWD, both overground and using the GRAIL, compared to the poor responders (Figure 1). The good responders had a significantly greater increase in stride length and a greater decrease in stride time as compared to the poor responders (MD: 0.14 m, 95% CI: 0.09–0.19 m, p < 0.001; MD: −0.05 s, 95% CI: −0.07–0.03, p < 0.001, respectively, Table 5). No differences were found in the change in CoV of spatiotemporal gait parameters between the groups after PR. The change in predictability in spatiotemporal gait parameters and the change in local dynamic stability of the CoMvel did not reach a statistically significant difference after PR.
Table 4.
Clinical outcomes of good and poor responders before and after pulmonary rehabilitation.
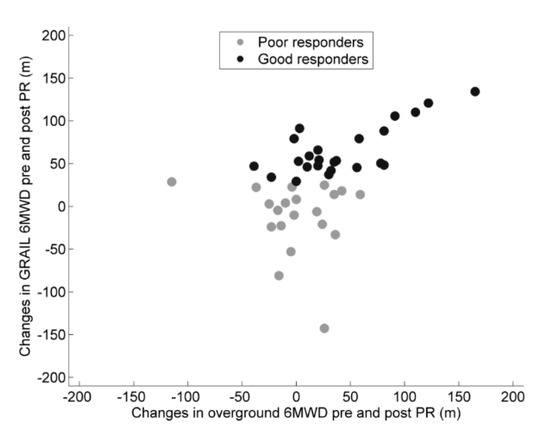
Figure 1.
Changes in 6MWD (6-min walk distance) in good and poor responders following pulmonary rehabilitation (PR) in the overground and GRAIL condition. The good responders are depicted in black dots and the poor responders in grey dots.
Table 5.
The 6MWT outcomes and gait parameters in good and poor responders during the GRAIL-based 6MWT before and after pulmonary rehabilitation.
4. Discussion
This study aimed to evaluate whether, and to what extent, a comprehensive PR program affects gait characteristics in patients with COPD during the GRAIL-based 6MWT. Patients with COPD demonstrated shorter mean stride times during the post PR GRAIL-based 6MWT. No changes in the amount of, and patterns within stride-to-stride fluctuations were found in patients following PR. In addition, good responders to PR showed improvements in mean stride time and stride length as compared to poor responders. No differences in stride-to-stride fluctuations were found between these groups after PR. The present findings suggest that a comprehensive PR program does improve walking speed in patients with COPD, whereas stride-to-stride fluctuations did not change. Research on gait impairments in COPD and identifying training modalities that improve gait function in COPD are therefore recommended.
Gait assessment may be of clinical value as gait abnormalities have been reported in patients with COPD, including reduced cadence, reduced stride length and increased double support time as compared to healthy subjects [3,4,5,6,7]. Though PR has proven to increase gait speed in patients with COPD [39], a comprehensive analysis of gait characteristics after PR is lacking. In the current study, patients with COPD improved their walk distance during the GRAIL-based 6MWT after PR, which also reached a clinically significant improvement [26]. This improvement in walking distance was achieved by a reduced mean stride time, and thus faster walking speeds. Moreover, patients with COPD tended to take longer strides contributing to an increased 6MWD. However, stride length changes were not found to be statistically significant.
Stride-to-stride fluctuations in gait may represent the capability of the locomotor system to make flexible adaptations during walking [14]. Healthy subjects are characterized by a healthy amount of, and patterns within stride-to-stride fluctuations [40]. These stride-to-stride fluctuations are associated with fall risk and may deteriorate with aging and disease [4,6,9,10,11,41,42]. In community dwelling older adults, improvements in stride-to-stride fluctuations can be achieved following physical training [43,44]. Exercise training is a key element in PR [23] and has demonstrated to improve skeletal muscle function [22,45,46]. As skeletal muscles are important components of the locomotor system for walking, PR was hypothesized to have beneficial effects on the amount of fluctuations, predictability and consistency of movement patterns in patients with COPD. In the current study, patients with COPD did not demonstrate less variable gait characteristics, less predictable patterns of gait characteristics and increased consistency of the center of mass movement patterns. Patients did show increased fat-free mass (e.g., muscle mass), and lower-limb muscle strength and endurance. The combination of individualized strength, interval and endurance training resulted in improvements in lower-limb muscle function. However, these improvements do not necessarily translate into improvements in stride-to-stride fluctuations in patients with COPD.
Interventions to improve walking have traditionally been multifactorial (i.e., strengthening, endurance and flexibility programs). These interventions focus on improving the physiologic capacity in body systems (i.e., musculoskeletal and cardiopulmonary systems) that contribute to walking, but do not include task specific exercises necessary to make use of the physiological capacity in body systems for walking (e.g., integrate movement and posture to improve efficiency of the physiological capacity) [47]. Therefore, task-oriented exercise training of walking could be beneficial to improve gait function, and more specifically in stride-to-stride fluctuations in COPD.
Response to PR differs in patients with COPD [25]. The current study showed that 55% of the patients were good responders in terms of improved functional exercise capacity during the GRAIL-based 6MWT (≥30 m), with an average increase in the 6MWD of 66 m after PR. The poor responders showed a decrease of 12 m during the GRAIL-based 6MWT after PR. The difference in step width at baseline was minimal between the groups and after PR this was minimal between the groups. This difference was not considered as clinically relevant. The good responders were therefore considered similar to the poor responders in terms of mean gait characteristics. Larger increase in mean walking speed for the good responders was accompanied by a shorter mean stride time and longer mean stride lengths.
In contrast to mean spatiotemporal gait parameters between the good and poor responders, the change in the amount of, and patterns within, stride-to-stride fluctuations did not reach significance. This could be partially explained by that exercise training in PR was not specifically targeted to systems that contribute to balance and gait control. Other parameters may have contributed to the faster walking speed in the good responders. The good responders tended to start with lower dyspnea and fatigue levels compared to the poor responders during the post PR GRAIL-based 6MWT. Interestingly, some poor responders showed improvements in lower-limb muscle function. This indicates that other factors may be associated with decreased walking speed, such as higher fatigue levels prior to the post PR GRAIL-based 6MWT. Furthermore, differences in ventilator reserve may be important. However, this was not assessed in the present study.
The present study has some limitations. Externally paced treadmill walking affects gait parameters and its stride-to-stride fluctuations. The GRAIL system, however, enables self-paced treadmill walking, using a feedback-controlled algorithm to adapt treadmill speed to the user while walking. The GRAIL system has shown to increase walking speed variability [48], thereby suggesting that self-paced treadmill walking allows for a more natural control of walking speed [49]. Patients with COPD who were most severely limited in their mobility and therefore using a walking aid were not eligible for the GRAIL-based 6MWT. It would be interesting to investigate whether alterations in gait characteristics are present for patients with more severe COPD, especially given the trend that lower-limb muscle weakness is more prevalent with more severe COPD [50]. Another limitation is that the assessment of lower-limb muscle strength and endurance in our study only targeted the quadriceps muscles. Reduced muscle strength has also been observed in the distal muscles of the lower-limbs [51]. Future studies should include the assessment of distal lower-limbs to gain a better understanding of distal lower-limb muscle dysfunction and gait characteristics in patients with COPD.
It was postulated that exercise training, and in particular, changes in lower-limb muscle function, could have positive effects on gait characteristics in COPD. This was partially confirmed by the findings of the present study, as walking speed increased. However, stride-to-stride fluctuations did not improve following PR. The current PR program was not specifically aimed to improve gait function and balance in patients with COPD. Moreover, in contrast to the study by Wang et al. [44], our study did not incorporate balance training specifically in PR. Consequently, this might explain the lack of changes in stride-to-stride fluctuations. It may be important to present exercises targeting to various systems for balance control and in different situations. We, therefore, propose to perform future research on gait and balance training in PR for patients with COPD. To date, different modalities of gait training are available, including perturbation training and dual task training [52,53], that could be used to assess the effect of gait and/or balance training on gait characteristics in COPD. In particular, improvements in stride-to-stride fluctuations will be important, as these measures are associated with increased fall risk in older adults and the high incidence of fall risk present in COPD [13].
5. Conclusions
This study showed that patients with COPD demonstrate shorter stride times during the GRAIL-based 6MWT after a comprehensive PR program. Though improvements in exercise capacity, body composition and quadriceps strength were found in patients with COPD following PR, stride-to-stride fluctuations did not improve. In addition, differences in mean gait characteristics were found between good and poor responders, while stride-to-stride fluctuations were not discriminative. These findings indicate that the current PR does not alter stride-to-stride fluctuations in patients with COPD. Additional training programs specifically targeting balance and gait function may be beneficial in improving gait characteristics in patients with COPD.
Supplementary Materials
The following are available online at https://www.mdpi.com/2077-0383/8/4/459/s1, Supplementary Materials title: Measures to quantify the patterns within stride-to-stride fluctuations.
Author Contributions
Individual contributions are listed as: “conceptualization, M.A.S., K.M. and W.-Y.L.; methodology, M.A.S., K.M. and W.-Y.L.; software, P.J.W. and W.-Y.L.; validation, n.a.; formal analysis, W.-Y.L.; investigation, W.-Y.L. and J.M.D.; resources, M.A.S., K.M. and E.F.M.W.; data curation, n.a.; writing—original draft preparation, W.-Y.L.; writing—review and editing, W.-Y.L., M.A.S., K.M., P.J.W., E.F.M.W., J.M.D.; visualization, W.-Y.L.; supervision, M.A.S., K.M. and E.F.M.W.; project administration, W.-Y.L.; funding acquisition, E.F.M.W.”
Acknowledgments
The authors thank S.M. Bruijn and J.M. Yentes for assistance with data-analysis. We are grateful to the study participants and the staff of CIRO.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Annegarn, J.; Meijer, K.; Passos, V.L.; Stute, K.; Wiechert, J.; Savelberg, H.H.; Schols, A.M.; Wouters, E.F.; Spruit, M.A. Problematic activities of daily life are weakly associated with clinical characteristics in COPD. J. Am. Med. Dir. Assoc. 2012, 13, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Nakken, N.; Janssen, D.J.; Bootsma, G.P.; Gronenschild, M.H.; Delbressine, J.M.; Muris, J.W.; Wouters, E.F.; Bogaart, E.H.V.D.; Van Vliet, M.; De Vries, G.J.; et al. Patient versus proxy-reported problematic activities of daily life in patients with COPD. Respirology 2016, 22, 307–314. [Google Scholar] [CrossRef]
- Annegarn, J.; Spruit, M.A.; Savelberg, H.H.C.M.; Willems, P.J.B.; Van De Bool, C.; Schols, A.M.W.J.; Wouters, E.F.M.; Meijer, K. Differences in walking pattern during 6-min walk test between patients with copd and healthy subjects. PLoS ONE 2012, 7, e37329. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.-Y.; Spruit, M.A.; Delbressine, J.M.; Willems, P.J.; Franssen, F.M.E.; Wouters, E.F.M.; Meijer, K. Spatiotemporal gait characteristics in patients with COPD during the gait real-time analysis interactive lab-based 6-minute walk test. PLoS ONE 2017, 12, e0190099. [Google Scholar] [CrossRef]
- Nantsupawat, N.; Lane, P.; Siangpraipunt, O.; Gadwala, S.; Nugent, K. Gait characteristics in patients with chronic obstructive pulmonary disease. J. Prim. Care Health 2015, 6, 222–226. [Google Scholar] [CrossRef]
- Yentes, J.M.; Rennard, S.I.; Schmid, K.K.; Blanke, D.; Stergiou, N. Patients with chronic obstructive pulmonary disease walk with altered step time and step width variability as compared with healthy control subjects. Ann. Am. Thorac. Soc. 2017, 14, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Zago, M.; Sforza, C.; Bonardi, D.R.; Guffanti, E.E.; Galli, M. Gait analysis in patients with chronic obstructive pulmonary disease: A systematic review. Gait Posture 2018, 61, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Mitchell, S.L.; Firtion, R.; Peng, C.K.; Cudkowicz, M.E.; Wei, J.Y.; Goldberger, A.L. Altered fractal dynamics of gait: Reduced stride-interval correlations with aging and Huntington’s disease. J. Appl. Physiol. 1997, 82, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.A.; Johanning, J.M.; Stergiou, N.; Celis, R.I.; Robinson, L.; Pipinos, I.I. Gait variability is altered in patients with peripheral arterial disease. J. Vasc. Surg. 2009, 49, 924–931.e1. [Google Scholar] [CrossRef] [PubMed]
- Buzzi, U.H.; Stergiou, N.; Kurz, M.J.; Hageman, P.; Heidel, J. Nonlinear dynamics indicates aging affects variability during gait. Clin. Biomech. 2003, 18, 435–443. [Google Scholar]
- Maki, B.E. Gait changes in older adults: Predictors of falls or indicators of fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Moe-Nilssen, R.; Helbostad, J.L. Interstride trunk acceleration variability but not step width variability can differentiate between fit and frail older adults. Gait Posture 2005, 21, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, N.; Harbourne, R.; Cavanaugh, J. Optimal movement variability: A new theoretical perspective for neurologic physical therapy. J. Neurol. Phys. Ther. 2006, 30, 120–129. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Cudkowicz, M.E.; Firtion, R.; Wei, J.Y.; Goldberger, A.L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 1998, 13, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Roig, M.; Eng, J.J.; Road, J.D.; Reid, W.D. Falls in patients with chronic obstructive pulmonary disease: A call for further research. Respir. Med. 2009, 103, 1257–1269. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Valentine, R.J.; Evans, E.M.; Sosnoff, J.J. Lower extremity muscle quality and gait variability in older adults. Age Ageing 2012, 41, 595–599. [Google Scholar] [CrossRef] [PubMed]
- Marques, N.R.; Laroche, D.P.; Hallal, C.Z.; Crozara, L.F.; Morcelli, M.H.; Karuka, A.H.; Navega, M.T.; Gonçalves, M. Association between energy cost of walking, muscle activation, and biomechanical parameters in older female fallers and non-fallers. Clin. Biomech. 2013, 28, 330–336. [Google Scholar] [CrossRef]
- Lord, S.R.; Lloyd, D.G.; Nirui, M.; Raymond, J.; Williams, P.; Stewart, R.A. The effect of exercise on gait patterns in older women: A randomized controlled trial. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1996, 51, M64–M70. [Google Scholar] [CrossRef]
- Mathur, S.; Brooks, D.; Carvalho, C.R.F. Structural alterations of skeletal muscle in COPD. Front. Physiol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- De Brandt, J.; Spruit, M.A.; Derave, W.; Hansen, D.; Vanfleteren, L.E.; Burtin, C. Changes in structural and metabolic muscle characteristics following exercise-based interventions in patients with COPD: A systematic review. Rev. Respir. Med. 2016, 10, 521–545. [Google Scholar] [CrossRef] [PubMed]
- De Brandt, J.; A Spruit, M.; Hansen, D.; Franssen, F.M.; Derave, W.; Sillen, M.J.; Burtin, C. Changes in lower limb muscle function and muscle mass following exercise-based interventions in patients with chronic obstructive pulmonary disease: A review of the English-language literature. Respir. Dis. 2017, 15, 182–219. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Augustin, I.M.L.; Wouters, E.F.M.; Houben-Wilke, S.; Gaffron, S.; Janssen, D.J.A.; Franssen, F.M.E.; Spruit, M.A. Comprehensive lung function assessment does not allow to infer response to pulmonary rehabilitation in patients with COPD. J. Clin. Med. 2018, 8, 27. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Augustin, I.M.; Vanfleteren, L.E.; Janssen, D.J.; Gaffron, S.; Pennings, H.-J.; Smeenk, F.; Pieters, W.; Bergh, J.J.V.D.; Michels, A.-J.; et al. Differential response to pulmonary rehabilitation in COPD: Multidimensional profiling. Eur. Respir. J. 2015, 46, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.-Y.; Meijer, K.; Delbressine, J.M.; Willems, P.J.; Franssen, F.M.E.; Wouters, E.F.M.; Spruit, M.A. Reproducibility and validity of the 6-minute walk test using the gait real-time analysis interactive lab in patients with COPD and healthy elderly. PLoS ONE 2016, 11, e0162444. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed]
- A Spruit, M.; Vanderhoven-Augustin, I.; Janssen, P.P.; Wouters, E.F. Integration of pulmonary rehabilitation in COPD. Lancet 2008, 371, 12–13. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; LaMonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “up & go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Van De Bool, C.; Mattijssen-Verdonschot, C.; Van Melick, P.P.M.J.; A Spruit, M.; E Franssen, F.M.; Wouters, E.F.M.; Schols, A.M.W.J.; A Rutten, E.P. Quality of dietary intake in relation to body composition in patients with chronic obstructive pulmonary disease eligible for pulmonary rehabilitation. Eur. J. Clin. Nutr. 2013, 68, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Makrides, L.; Hernandez, P. Test-retest reliability of isometric and isokinetic torque in patients with chronic obstructive pulmonary disease. Physiother. Can. 2004, 56, 94. [Google Scholar] [CrossRef]
- Bogert, A.J.V.D.; Geijtenbeek, T.; Even-Zohar, O.; Steenbrink, F.; Hardin, E.C.; Bogert, A.V.D. A real-time system for biomechanical analysis of human movement and muscle function. Med. Boil. Eng. Comput. 2013, 51, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Bruijn, S.M.; Meijer, O.G.; Beek, P.J.; Van Dieen, J.H.; Bruijn, S. Assessing the stability of human locomotion: A review of current measures. J. R. Soc. 2013, 10, 20120999. [Google Scholar] [CrossRef]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The appropriate use of approximate entropy and sample entropy with short data sets. Ann. Biomed. Eng. 2012, 41, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Chen, C.; Cao, Z.; Sun, B.; Lo, I.L.; Liu, T.-M.; Zheng, J.; Sun, S.; Shi, Y.; Zhang, X.D. Entropy change of biological dynamics in COPD. Int. J. Obstr. Pulm. Dis. 2017, 12, 2997–3005. [Google Scholar] [CrossRef] [PubMed]
- Polkey, M.I.; Spruit, M.A.; Edwards, L.D.; Watkins, M.L.; Pinto-Plata, V.; Vestbo, J.; Calverley, P.M.A.; Tal-Singer, R.; Agusti, A.; Bakke, P.S.; et al. Six-minute-walk test in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 382–386. [Google Scholar] [CrossRef] [PubMed]
- McClellan, R.; Amiri, H.M.; Limsuwat, C.; Nugent, K.M. pulmonary rehabilitation increases gait speed in patients with chronic lung diseases. Health Serv. Res. Manag. Epidemiol. 2014, 1. [Google Scholar] [CrossRef]
- Stergiou, N.; Decker, L.M. Human movement variability, nonlinear dynamics, and pathology: Is there a connection? Hum. Mov. Sci. 2011, 30, 869–888. [Google Scholar] [CrossRef] [PubMed]
- Lipsitz, L.A. Loss of ‘complexity’ and aging. Potential applications of fractals and chaos theory to senescence. JAMA 1992, 267, 1806–1809. [Google Scholar] [CrossRef] [PubMed]
- Dingwell, J.B.; Cusumano, J.P. Nonlinear time series analysis of normal and pathological human walking. Chaos Interdiscip. J. Sci. 2000, 10, 848. [Google Scholar] [CrossRef]
- Beauchet, O.; Launay, C.; Annweiler, C.; Fantino, B.; Allali, G.; De Decker, L. Physical training-related changes in gait variability while single and dual tasking in older adults: Magnitude of gait variability at baseline matters. Eur. J. Phys. Rehabil. Med. 2013, 49, 857–864. [Google Scholar] [PubMed]
- Wang, R.-Y.; Wang, Y.-L.; Cheng, F.-Y.; Chao, Y.-H.; Chen, C.-L.; Yang, Y.-R. Effects of combined exercise on gait variability in community-dwelling older adults. AGE 2015, 37, 9780. [Google Scholar] [CrossRef] [PubMed]
- Nici, L.; Donner, C.; Wouters, E.; ZuWallack, R.; Ambrosino, N.; Bourbeau, J.; Carone, M.; Celli, B.; Engelen, M.; Fahy, B.; et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2006, 173, 1390–1413. [Google Scholar] [CrossRef] [PubMed]
- Mador, M.J.; Bozkanat, E.; Aggarwal, A.; Shaffer, M.; Kufel, T.J. Endurance and strength training in patients with COPD. Chest 2004, 125, 2036–2045. [Google Scholar] [CrossRef] [PubMed]
- Brach, J.S.; Van Swearingen, J.M. Interventions to improve walking in older adults. Curr. Transl. Geriatr. Exp. Gerontol. Rep. 2013, 2, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Sloot, L.; Van Der Krogt, M.; Harlaar, J. Self-paced versus fixed speed treadmill walking. Gait Posture 2014, 39, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Plotnik, M.; Azrad, T.; Bondi, M.; Bahat, Y.; Gimmon, Y.; Zeilig, G.; Inzelberg, R.; Siev-Ner, I. Self-selected gait speed—Over ground versus self-paced treadmill walking, a solution for a paradox. J. Neuroeng. Rehabil. 2015, 12, 17. [Google Scholar] [CrossRef] [PubMed]
- Seymour, J.M.; Spruit, M.A.; Hopkinson, N.S.; Sathyapala, S.; Man, W.D.-C.; Jackson, A.; Gosker, H.R.; Schols, A.M.W.J.; Moxham, J.; Polkey, M.I.; et al. The prevalence of quadriceps weakness in COPD and the relationship with disease severity. Eur. Respir. J. 2009, 36, 81–88. [Google Scholar] [CrossRef]
- Gagnon, P.; Maltais, F.; Bouyer, L.; Ribeiro, F.; Coats, V.; Brouillard, C.; Noël, M.; Rousseau-Gagnon, M.; Saey, D. Distal leg muscle function in patients with COPD. COPD J. Obstr. Pulm. Dis. 2013, 10, 235–242. [Google Scholar] [CrossRef] [PubMed]
- McCrum, C.; Gerards, M.H.G.; Karamanidis, K.; Zijlstra, W.; Meijer, K. A systematic review of gait perturbation paradigms for improving reactive stepping responses and falls risk among healthy older adults. Eur. Rev. Phys. Act. 2017, 14, 1224. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Rochester, L.; Reelick, M.; Nieuwhof, F.; Pelosin, E.; Abbruzzese, G.; Dockx, K.; Nieuwboer, A.; Hausdorff, J.M. V-TIME: A treadmill training program augmented by virtual reality to decrease fall risk in older adults: Study design of a randomized controlled trial. BMC Neurol. 2013, 13, 15. [Google Scholar] [CrossRef] [PubMed]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).