Abstract
Background: Lung transplantation has been increasingly performed worldwide and is considered an effective therapy for patients with various causes of end-stage lung diseases. We performed a systematic review to assess the incidence and impact of acute kidney injury (AKI) and severe AKI requiring renal replacement therapy (RRT) in patients after lung transplantation. Methods: A literature search was conducted utilizing Ovid MEDLINE, EMBASE, and Cochrane Database from inception through June 2019. We included studies that evaluated the incidence of AKI, severe AKI requiring RRT, and mortality risk of AKI among patients after lung transplantation. Pooled incidence and odds ratios (ORs) with 95% confidence interval (CI) were obtained using random-effects meta-analysis. The protocol for this meta-analysis is registered with PROSPERO (International Prospective Register of Systematic Reviews; no. CRD42019134095). Results: A total of 26 cohort studies with a total of 40,592 patients after lung transplantation were enrolled. Overall, the pooled estimated incidence rates of AKI (by standard AKI definitions) and severe AKI requiring RRT following lung transplantation were 52.5% (95% CI: 45.8–59.1%) and 9.3% (95% CI: 7.6–11.4%). Meta-regression analysis demonstrated that the year of study did not significantly affect the incidence of AKI (p = 0.22) and severe AKI requiring RRT (p = 0.68). The pooled ORs of in-hospital mortality in patients after lung transplantation with AKI and severe AKI requiring RRT were 2.75 (95% CI, 1.18–6.41) and 10.89 (95% CI, 5.03–23.58). At five years, the pooled ORs of mortality among patients after lung transplantation with AKI and severe AKI requiring RRT were 1.47 (95% CI, 1.11–1.94) and 4.79 (95% CI, 3.58–6.40), respectively. Conclusion: The overall estimated incidence rates of AKI and severe AKI requiring RRT in patients after lung transplantation are 52.5% and 9.3%, respectively. Despite advances in therapy, the incidence of AKI in patients after lung transplantation does not seem to have decreased. In addition, AKI after lung transplantation is significantly associated with reduced short-term and long-term survival.
1. Introduction
Acute kidney injury (AKI) is a complex clinical syndrome characterized by a sharp reduction in the glomerular filtration rate (GFR) followed by elevated serum creatinine or oliguria, and is associated with various etiologies and pathophysiological pathways. AKI is a major global health problem with a steadily increasing incidence in recent years [1,2,3]. The global burden of AKI is 13.3 million cases per year and is associated with significant mortality, resulting in 1.4 million deaths per year [4,5,6]. Mortality rates from AKI range from 16% to 50% according to the stage and vary widely according to etiology and patient comorbidities [7,8]. Those who survive the AKI are at increased risk for hypertension and progressive chronic kidney disease (CKD), including end-stage kidney disease (ESKD) [9].
Since the first human lung transplant was performed in 1963, almost 55,000 lung transplantations have been performed worldwide, now with nearly 4600 lung transplantations performed annually [10]. Up to 68% of lung transplant recipients develop AKI, which has been associated with increased one-year mortality, length of hospital stay, higher resource utilization, and related health care burden [10,11,12,13,14,15,16,17,18,19,20,21,22]. Though survival following lung transplantation has improved over the past few decades, morbidity and mortality related to AKI after lung transplantation and resultant progressive CKD remain relatively high and is a cause for increasing concern [16,23,24,25]. The incidence of AKI following lung transplantation varies widely, estimated to be as high as two-thirds of recipients, with up to 5% to 8% requiring dialysis in the initial few months post lung transplantation [11,13,14,15,21,24,26,27,28,29]. Differences in the definition of AKI may account for the variance of incidence of post-lung-transplant AKI [28].
Despite significant advances in lung transplantation surgical and medical practices, the epidemiology, risk factors, and mortality associated with AKI among post-lung-transplant recipients and their trends remain unclear. Therefore, we conducted a systematic review to summarize and trend the incidence of AKI (utilizing standard AKI definitions including AKIN (acute kidney injury network) [30], RIFLE (risk, injury, failure, loss of kidney function, and end-stage kidney disease) [31], and KDIGO (kidney disease: Improving global outcomes) [32] classifications) and mortality risk of AKI in lung transplant recipients.
2. Methods
2.1. Information Sources and Search Strategy
The protocol for this meta-analysis is registered with PROSPERO (International Prospective Register of Systematic Reviews (CRD42019134095)). A systematic literature search of Ovid MEDLINE, EMBASE, and the Cochrane Database from database inceptions through June 2019 was performed to summarize the incidence and impact of AKI on mortality risk among adult patients following lung transplantation. Two investigators (P.L. and C.T.) individually performed a systematic literature search utilizing the search approach that consolidated the search terms of “lung” OR “pulmonary” AND “transplant” OR “transplantation” AND “acute kidney injury” OR “acute renal failure” OR “renal replacement therapy”. Detailed information on the search strategy from each database is provided in Online Supplementary Data 1. No language limitation was implemented. A manual review for conceivably-related studies employing references of the included studies was additionally performed. Grey literature was also searched for further relevant information. This systematic review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) statement [33].
2.2. Study Selection
Studies were included in this meta-analysis if they were observational studies or clinical trials that provided data on incidence of AKI (utilizing standard AKI definitions including AKIN [30], RIFLE [31], and KDIGO [32] classifications), AKI requiring renal replacement therapy (RRT), and mortality risk of AKI in adult patients after lung transplantation (age ≥ 18 years old). Eligible studies needed to provide data to assess the incidence or mortality rate of AKI with 95% confidence intervals (CIs). Retrieved articles were individually examined for eligibility by the two investigators (P.L. and C.T.). Inconsistencies were discussed with the third reviewer (W.C.) and solved by common agreement. The size of the study did not limit inclusion.
2.3. Data Collection Process
A structured data collecting form was used to collect the following data from individual studies including title, name of authors, year of the study, publication year, country where the study was conducted, patient characteristics, AKI definition, incidence of AKI, incidence of severe AKI requiring RRT, and mortality risk of AKI among patients after lung transplantation.
2.4. Statistical Analysis
Comprehensive Meta-Analysis software version 3.3.070 (Biostat Inc., Englewood, NJ, USA) was used to perform meta-analysis. Adjusted point estimates of included studies were incorporated by the generic inverse variance method of DerSimonian–Laird, which assigned the weight of an individual study based on its variance [34]. Due to the probability of between-study variance, we applied a random-effects model to pool outcomes of interest, including incidence of AKI and mortality risk. Statistical heterogeneity of studies was assessed by the Cochran’s Q test (p < 0.05 for a statistical significance) and the I2 statistic (≤25% represents insignificant heterogeneity, 26% to 50% represents low heterogeneity, 51% to 75% represents moderate heterogeneity, and ≥75% represents high heterogeneity) [35]. The presence of publication bias was assessed by both funnel ploy and the Egger test [36].
3. Results
The search yielded a total of 1809 articles for initial screening. After removal of 714 duplicates, the titles and abstracts of 1095 articles were screened for eligibility. A total of 922 articles were excluded (due to in vitro studies, pediatric patient population, animal studies, case reports, correspondences, or review articles). A total of 173 potentially relevant studies were included for full-length article review; 147 of them were additionally excluded from the full-text review as they did not provide the outcome of interest (n = 77) or were not observational studies (n = 48), or did not use a standard AKI definition (n = 22).
Thus, 26 cohort studies [10,11,13,14,19,21,24,28,29,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53] with 40,592 patients undergoing lung transplantation were identified. Figure 1 shows a flowchart outlining identification of papers for inclusion. Table 1 presents the characteristics of the included studies. The kappa for systematic searches, selection of studies and data extraction were 0.98, 0.87, and 0.98, respectively.
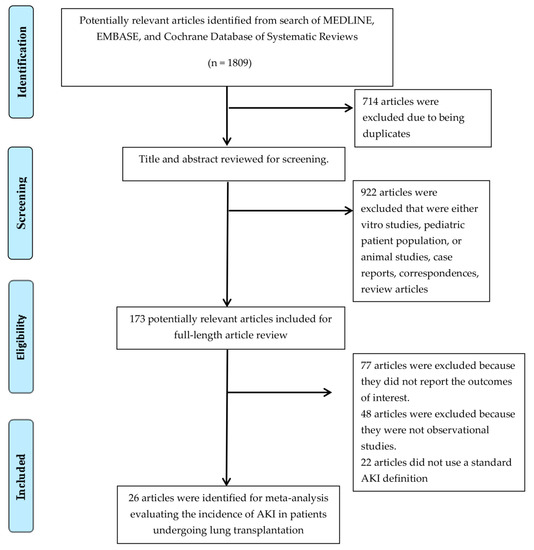
Figure 1.
Outline of our search methodology. AKI, Acute kidney injury.

Table 1.
Main characteristic of studies included in analysis assessing the incidence of acute kidney injury in patients after lung transplantation.
3.1. Incidence of Acute Kidney Injury among Patients after Lung Transplantation
The pooled estimated incidence rates of AKI and severe AKI requiring RRT after lung transplantation were 52.5% (95% CI: 45.8–59.1%, I2 = 89%, Figure 2) and 9.3% (95% CI: 7.6–11.4%, I2 = 90%, Figure 3). Subgroup analysis based on the AKI definition was performed and demonstrated a pooled estimated incidence of AKI after lung transplantation of 49% (95% CI: 38.3–59.8%, I2 = 86%, Figure 2) by RIFLE criteria, 55.5% (95% CI: 45.2–65.4%, I2 = 71%, Figure 2) by AKIN criteria, and 53.0% (95% CI: 38.2–67.3%, I2 = 91%, Figure 2) by KDIGO criteria.
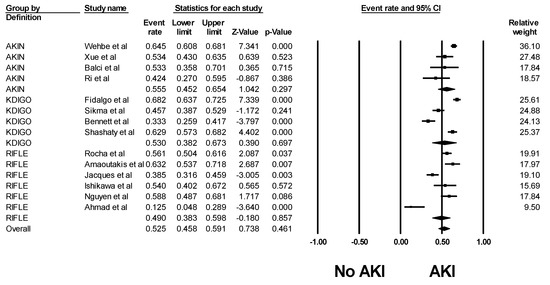
Figure 2.
Forest plots of the included studies evaluating incidence rates of AKI after lung transplantation. AKI, Acute kidney injury.

Figure 3.
Forest plots of the included studies evaluating incidence rates of AKI requiring RRT after lung transplantation. AKI, Acute kidney injury; RRT, renal replacement therapy.
Meta-regression analysis demonstrated that year of study did not significantly affect the incidence of AKI (p = 0.22) and severe AKI requiring RRT (p = 0.68) among patients after lung transplantation, as shown in Figure 4.
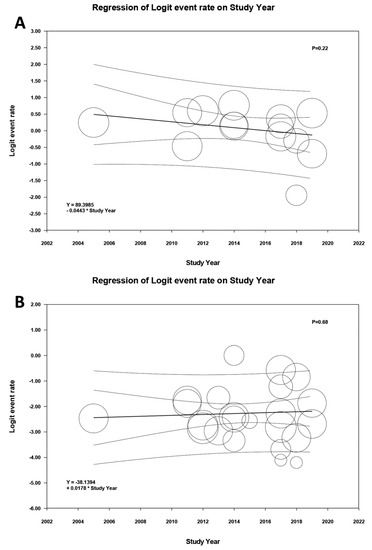
Figure 4.
Meta-regression analyses showed that year of study did not significantly affect (A) the incidence of AKI (p = 0.11) and (B) severe AKI requiring RRT (p = 0.54) among patients after lung transplantation. AKI, acute kidney injury; RRT, renal replacement therapy.
3.2. Mortality Risk of Acute Kidney Injury in Patients after Lung Transplantation
Data on mortality risk from included studies are shown in Table 2. The pooled OR of hospital mortality among patients after lung transplantation with AKI and severe AKI requiring RRT were 2.75 (95% CI, 1.18–6.41, I2 = 69%, Figure 5A) and 10.89 (95% CI, 5.03–23.58, I2 = 82%, Figure 5B), respectively. At one year, the pooled OR of mortality among patients after lung transplantation with AKI and severe AKI requiring RRT were 2.99 (95% CI, 1.72–5.18, I2 = 74%, Figure S1) and 8.32 (95% CI, 5.95–11.63, I2 = 70%, Figure S2), respectively. At five years, the pooled OR of mortality among patients after lung transplantation with AKI and severe AKI requiring RRT were 1.47 (95% CI, 1.11–1.94, I2 = 0%, Figure S3) and 4.79 (95% CI, 3.58–6.40, I2 = 81%, Figure S4), respectively.
Table 2.
Mortality risk of AKI in patients after lung transplantation.
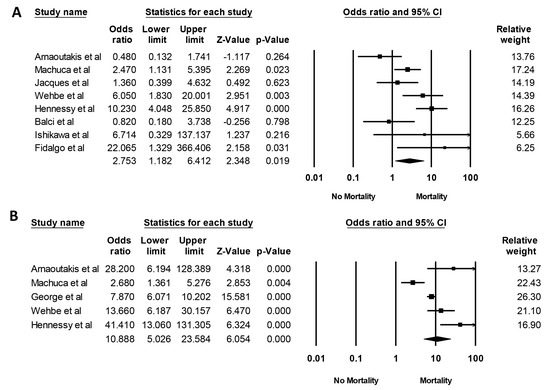
Figure 5.
Forest plots of the included studies evaluating hospital mortality of (A) AKI and (B) AKI requiring RRT after lung transplantation. AKI, acute kidney injury; RRT, renal replacement therapy.
3.3. Evaluation for Publication Bias
Funnel plot (Figures S5 and S6) and Egger’s regression asymmetry tests were performed to assess publication bias in analysis evaluating mortality risk of AKI in patients after lung transplant with AKI and severe AKI requiring RRT, respectively. We found no significant publication bias in meta-analysis evaluating mortality risk of patients after lung transplant with AKI (p = 0.99) and severe AKI requiring RRT (p = 0.50).
4. Discussion and Conclusions
In this systematic review, we demonstrated that AKI in patients after lung transplantation is common, with pooled incidence rates of AKI and severe AKI requiring RRT in patients after lung transplantation of 52.5% and 9.3%, respectively. We also showed that the incidence of AKI in patients after lung transplantation has not improved, despite advances in therapy. Compared to those without AKI, patients with post-lung-transplant AKI had increased short and long-term mortality.
Some specific factors related to AKI after lung transplant include hypercapnia/hypoxemia-mediated impaired renal blood flow (RBF), hemodynamics during lung transplant surgery, and the use of extracorporeal membrane oxygenation (ECMO) and cardio-pulmonary bypass (CPB) during lung transplant surgery [12,28,44,54]. Postoperative respiratory failure is common after lung transplantation; reported to be as high as 55% [55]. Hypoxemia is associated with reduced RBF in a dose-dependent relationship [56,57,58] thought to be related to stimulation of adrenergic neurons and alterations in nitric oxide metabolism [59]. In addition, studies have shown that hypercapnia can induce peripheral vasodilatation and decreased systemic vascular resistance, with a compensatory neurohormonal vasoconstriction response. This leads to activation of the renin-angiotensin-aldosterone system (RAAS) and direct renal vasoconstriction, resulting in a reduction in RBF and GFR [56,60,61,62]. Furthermore, poorly controlled hemodynamics during lung transplant surgery can result in intraoperative hypotension, one of the most significant risk factors for the development of AKI after lung transplantation [10,24]. Currently, CPB remains a standard method used in lung transplantation for intraoperative cardiorespiratory support, especially in cases of poor hemodynamic tolerance or severe pulmonary arterial hypertension [63]. However, CPB is commonly associated with inflammatory reactions and bleeding complications [64]. ECMO has more recently been used as an alternative option to CPB for intraoperative cardiopulmonary support during lung transplantation [63]. When compared to CPB, studies have demonstrated beneficial effects of intraoperative ECMO support, with lower rates of primary graft dysfunction, acute post-operative bleeding, AKI requiring RRT, and length of hospital stay [63]. However, the use of ECMO itself may also cause a renal insult related to the activation of proinflammatory mediators caused by the continuous exposure of blood to the non-biological and non-endothelialized ECMO interface [65]. Therefore, our study demonstrated that patients undergoing lung transplantation more frequently develop AKI and AKI requiring RRT than abdominal solid organ transplantation, such as liver transplantation (incidence of AKI and AKI requiring RRT of 41% and 7%, respectively) [66].
As there are currently no effective targeted pharmacotherapies available for AKI, treatment is limited to supportive strategies and RRT when indicated [4,5,6,8]. Patients who recover from AKI continue to have an increased risk of mortality on either short or long-term follow-up [9]. Following post-lung-transplant AKI, patients may develop CKD, with rates of progression to ESKD as high as 3.8%, 7.2%, and 7.9% at one, five, and ten years after lung transplant, respectively [17,46,67]. Therefore, prevention and early identification of AKI in patients at risk for post-lung-transplant AKI may potentially play an important role in improving patient outcomes. Important risk factors for AKI in patients after lung transplantation include bilateral lung transplantation [19,21,29,68], lower baseline estimated GFR [13,19,38,46,68], pulmonary hypertension [19,38,46], duration of mechanical ventilation requirement [13,14,24,28,46,53], the need for ECMO support [19,46,68], intraoperative hypotension, and vasopressor requirement [10,24] (Table 3).
Table 3.
Reported risk factors for AKI after lung transplantation.
There is experimental data that injurious ventilation strategies, such as a high tidal volume, low positive end-expiratory pressure approach can cause renal epithelial cell apoptosis and dysregulation of extracellular ligands that control renal vascular tone and endothelial integrity, resulting in AKI [69,70]. Among patients with acute respiratory distress syndrome, protective lung ventilation is associated with a reduced risk for AKI requiring dialysis and improves dialysis-free survival [71]. Therefore, future studies are needed to assess whether maintaining perioperative lung-protective ventilation helps to prevent AKI following lung transplantation [12]. Moreover, ECMO management may also play an important role in the prevention of post lung transplant AKI. High ECMO pump speed is associated with hemolysis and AKI development [65]. Future prospective studies are needed to assess the effects of ECMO pump speed on the risk of post-lung-transplantation AKI. Finally, immunosuppressive medications may also play an important role in AKI development following lung transplantation [12,72]. AKI related to calcineurin inhibitor (CNI)-induced thrombotic microangiopathy (TMA) has been reported in lung transplant recipients and is often missed or recognized late in the ICU setting [12,72]. Although TMA in lung transplant recipients is a rare condition, early recognition and management can potentially reduce post lung transplant-related morbidity and mortality [12,72,73].
Our study has some limitations. Firstly, there are statistical heterogeneities in our meta-analysis. Subgroup analyses were performed using differing AKI definitions, including RIFLE criteria AKIN criteria and KDIGO criteria. Meta-regression analysis assessing the effect of year of study on the incidence of AKI was also performed, and we found no significant correlation between year of study and incidence of AKI post lung transplantation. Secondly, AKI diagnosis from the included studies was based on changes in serum creatinine, and data on urine output and AKI biomarkers was limited. Lastly, this systematic review is primarily based on observational studies, as the data from clinical trials or population-based studies were limited. Thus, it can, at best, demonstrate an association between AKI and increased short-term and long-term mortality post lung transplant, but not a causal relationship.
In summary, AKI and severe AKI requiring RRT are common in patients after lung transplantation, with overall estimated incidence rates of 52.5% and 9.3%, respectively. Post-lung-transplant AKI is significantly associated with reduced short-term and long-term survival. Despite advances in transplantation therapy, the incidence of AKI in patients after lung transplantation does not appear to have improved.
Supplementary Materials
The following are available online at https://www.mdpi.com/2077-0383/8/10/1713/s1, Search terms for systematic review; Figure S1. Forest plots of the included studies assessing the pooled OR of mortality at one year among patients after lung transplantation with AKI; Figure S2: Forest plots of the included studies assessing the pooled OR of mortality at one year among patients after lung transplantation with severe AKI requiring RRT; Figure S3: Forest plots of the included studies assessing the pooled OR of mortality at five years among patients after lung transplantation with AKI; Figure S4: Forest plots of the included studies assessing the pooled OR of mortality at five years among patients after lung transplantation with severe AKI requiring RRT; Figure S5: Funnel plot evaluating for publication bias evaluating mortality risk of AKI in patients after lung transplant with AKI; Figure S6: Funnel plot evaluating for publication bias evaluating mortality risk of AKI in patients after lung transplant with severe AKI requiring RRT.
Author Contributions
Conceptualization, W.C., N.S., T.B., K.W. (Kanramon Watthanasuntorn), N.R.A., S.A.S., E.A.G., (K.W.) Karn Wijarnpreecha, M.A.M. and W.K.; data curation, P.L., C.T. and O.A.O.; formal analysis, W.C.; funding acquisition, T.B.; investigation, P.L., C.T., W.C., E.A.G. and W.K.; methodology, C.T, O.A.O., N.R.A., S.A.S., P.U., K.W. (Karn Wijarnpreecha), M.A.M. and W.K.; project administration, W.C., T.B. and K.W. (Kanramon Watthanasuntorn); resources, W.C., T.B., K.W. (Kanramon Watthanasuntorn) and W.K.; software, K.W. (Kanramon Watthanasuntorn); supervision, N.S., N.R.A., S.A.S., P.U., E.A.G., K.W. (Karn Wijarnpreecha), M.A.M. and W.K.; validation, P.L., W.C., N.S., T.B., P.U. and W.K.; visualization, O.A.O., P.U. and W.K.; writing—original draft, P.L. and W.K.; writing—review and editing, C.T., W.C., O.A.O., N.S., T.B., K.W. (Kanramon Watthanasuntorn), N.R.A., S.A.S., P.U., E.A.G., K.W. (Karn Wijarnpreecha), M.A.M. and W.K.
Acknowledgments
None. All authors had access to the data and had important roles in the writing of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gameiro, J.; Agapito Fonseca, J.; Jorge, S.; Lopes, J.A. Acute Kidney Injury Definition and Diagnosis: A Narrative Review. J. Clin. Med. 2018, 7, 307. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Harrison, A.M.; Erickson, S.B. Elevated admission serum calcium phosphate product as an independent risk factor for acute kidney injury in hospitalized patients. Hosp Pract (1995) 2019, 47, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Sakhuja, A.; Kashani, K. U-shape association of serum albumin level and acute kidney injury risk in hospitalized patients. PLoS ONE 2018, 13, e0199153. [Google Scholar] [CrossRef]
- Kashani, K.; Cheungpasitporn, W.; Ronco, C. Biomarkers of acute kidney injury: The pathway from discovery to clinical adoption. Clin. Chem. Lab. Med. 2017, 55, 1074–1089. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fang, Y.; Teng, J.; Ding, X. Acute Kidney Injury Epidemiology: From Recognition to Intervention. Contrib. Nephrol. 2016, 187, 1–8. [Google Scholar] [PubMed]
- Negi, S.; Koreeda, D.; Kobayashi, S.; Yano, T.; Tatsuta, K.; Mima, T.; Shigematsu, T.; Ohya, M. Acute kidney injury: Epidemiology, outcomes, complications, and therapeutic strategies. Semin. Dial. 2018, 31, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.J.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensiv. Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Kashani, K. Electronic Data Systems and Acute Kidney Injury. Contrib. Nephrol. 2016, 187, 73–83. [Google Scholar]
- Sawhney, S.; Marks, A.; Fluck, N.; Levin, A.; McLernon, D.; Prescott, G.; Black, C. Post-discharge kidney function is associated with subsequent ten-year renal progression risk among survivors of acute kidney injury. Kidney Int. 2017, 92, 440–452. [Google Scholar] [CrossRef]
- Nguyen, A.P.; Gabriel, R.A.; Golts, E.; Kistler, E.B.; Schmidt, U. Severity of Acute Kidney Injury in the Post-Lung Transplant Patient Is Associated with Higher Healthcare Resources and Cost. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1361–1369. [Google Scholar] [CrossRef]
- Arnaoutakis, G.J.; George, T.J.; Robinson, C.W.; Gibbs, K.W.; Orens, J.B.; Merlo, C.A.; Shah, A.S. Severe acute kidney injury according to the RIFLE (risk, injury, failure, loss, end stage) criteria affects mortality in lung transplantation. J. Heart Lung Transplant. 2011, 30, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Puttarajappa, C.M.; Bernardo, J.F.; Kellum, J.A. Renal Complications Following Lung Transplantation and Heart Transplantation. Crit. Care Clin. 2019, 35, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Rocha, P.N.; Rocha, A.T.; Palmer, S.M.; Davis, R.D.; Smith, S.R. Acute renal failure after lung transplantation: Incidence, predictors and impact on perioperative morbidity and mortality. Am. J. Transplant. 2005, 5, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo, P.; Ahmed, M.; Meyer, S.R.; Lien, D.; Weinkauf, J.; Cardoso, F.S.; Jackson, K.; Bagshaw, S.M. Incidence and outcomes of acute kidney injury following orthotopic lung transplantation: A population-based cohort study. Nephrol. Dial. Transplant. 2014, 29, 1702–1709. [Google Scholar] [CrossRef]
- Fidalgo, P.; Ahmed, M.; Meyer, S.R.; Lien, D.; Weinkauf, J.; Kapasi, A.; Cardoso, F.S.; Jackson, K.; Bagshaw, S.M. Association between transient acute kidney injury and morbidity and mortality after lung transplantation: A retrospective cohort study. J. Crit. Care 2014, 29, 1028–1034. [Google Scholar] [CrossRef]
- Wehbe, E.; Duncan, A.E.; Dar, G.; Budev, M.; Stephany, B. Recovery from AKI and short- and long-term outcomes after lung transplantation. Clin. J. Am. Soc. Nephrol. 2013, 8, 19–25. [Google Scholar] [CrossRef]
- Chambers, D.C.; Yusen, R.D.; Cherikh, W.S.; Goldfarb, S.B.; Kucheryavaya, A.Y.; Khusch, K.; Levvey, B.J.; Lund, L.H.; Meiser, B.; Rossano, J.W.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Lung and Heart-Lung Transplantation Report—2017; Focus Theme: Allograft ischemic time. J. Heart Lung Transplant. 2017, 36, 1047–1059. [Google Scholar] [CrossRef]
- Bloom, R.; Doyle, A. Kidney Disease after Heart and Lung Transplantation. Arab. Archaeol. Epigr. 2006, 6, 671–679. [Google Scholar] [CrossRef]
- George, T.J.; Arnaoutakis, G.J.; Beaty, C.A.; Pipeling, M.R.; Merlo, C.A.; Conte, J.V.; Shah, A.S. Acute kidney injury increases mortality after lung transplantation. Ann. Thorac. Surg. 2012, 94, 185–192. [Google Scholar] [CrossRef]
- Lafrance, J.P.; Miller, D.R. Acute kidney injury associates with increased long-term mortality. J. Am. Soc. Nephrol. JASN 2010, 21, 345–352. [Google Scholar] [CrossRef]
- Jacques, F.; El-Hamamsy, I.; Fortier, A.; Maltais, S.; Perrault, L.P.; Liberman, M.; Noiseux, N.; Ferraro, P. Acute renal failure following lung transplantation: Risk factors, mortality, and long-term consequences. Eur. J. Cardiothorac. Surg. 2012, 41, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Jardel, S.; Reynaud, Q.; Durieu, I. Long-term extrapulmonary comorbidities after lung transplantation in cystic fibrosis: Update of specificities. Clin. Transplant. 2018, 32, e13269. [Google Scholar] [CrossRef] [PubMed]
- Yusen, R.D.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Dipchand, A.I.; Goldfarb, S.B.; Levvey, B.J.; Lund, L.H.; Meiser, B.; Rossano, J.W.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-second Official Adult Lung and Heart-Lung Transplantation Report—2015; Focus Theme: Early Graft Failure. J. Heart Lung Transplant. 2015, 34, 1264–1277. [Google Scholar] [CrossRef] [PubMed]
- Balci, M.; Vayvada, M.; Salturk, C.; Kutlu, C.; Ari, E. Incidence of Early Acute Kidney Injury in Lung Transplant Patients: A Single-Center Experience. Transplant. Proc. 2017, 49, 593–598. [Google Scholar] [CrossRef]
- De La Morena, M.P.; Bravos, M.D.L.T.; Prado, R.F.; Roel, M.D.; Salcedo, J.G.; Costa, E.F.; Rivas, D.G.; Maté, J.B. Chronic Kidney Disease After Lung Transplantation: Incidence, Risk Factors, and Treatment. Transplant. Proc. 2010, 42, 3217–3219. [Google Scholar] [CrossRef]
- Hornum, M.; Iversen, M.; Steffensen, I.; Hovind, P.; Carlsen, J.; Andersen, L.W.; Steinbrüchel, D.A.; Feldt-Rasmussen, B.; Feldt-Rasmussen, B.; Feldt-Rasmussen, B. Rapid Decline in51Cr-EDTA Measured Renal Function During the First Weeks Following Lung Transplantation. Arab. Archaeol. Epigr. 2009, 9, 1420–1426. [Google Scholar] [CrossRef]
- Castro, A.G.; Llorca, J.; Cañas, B.S.; Fernández-Miret, B.; Zurbano, F.; Miñambres, E. Acute renal failure in lung transplantation: Incidence, correlation with subsequent kidney disease, and prognostic value. Arch. Bronconeumol. 2008, 44, 353–359. [Google Scholar] [CrossRef]
- Xue, J.; Wang, L.; Chen, C.-M.; Chen, J.-Y.; Sun, Z.-X. Acute kidney injury influences mortality in lung transplantation. Ren. Fail. 2014, 36, 541–545. [Google Scholar] [CrossRef]
- Ishikawa, S.; Griesdale, D.E.; Lohser, J. Acute Kidney Injury within 72 Hours After Lung Transplantation: Incidence and Perioperative Risk Factors. J. Cardiothorac. Vasc. Anesth. 2014, 28, 931–935. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; George, C.; Bellomo, R. A comparison of the RIFLE and AKIN criteria for acute kidney injury in critically ill patients. Nephrol. Dial. Transplant. 2008, 23, 1569–1574. [Google Scholar] [CrossRef]
- Uchino, S.; Bellomo, R.; Goldsmith, D.; Bates, S.; Ronco, C. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit. Care Med. 2006, 34, 1913–1917. [Google Scholar] [CrossRef] [PubMed]
- Palevsky, P.M.; Liu, K.D.; Brophy, P.D.; Chawla, L.S.; Parikh, C.R.; Thakar, C.V.; Tolwani, A.J.; Waikar, S.S.; Weisbord, S.D. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for Acute Kidney Injury. Am. J. Kidney Dis. 2013, 61, 649–672. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Easterbrook, P.; Gopalan, R.; Berlin, J.; Matthews, D. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Machuca, T.N.; Schio, S.M.; Camargo, S.M.; Lobato, V.; Costa, C.D.O.; Felicetti, J.C.; Moreira, J.S.; Camargo, J.J. Prognostic Factors in Lung Transplantation: The Santa Casa de Porto Alegre Experience. Transplantation 2011, 91, 1297–1303. [Google Scholar] [CrossRef]
- Wehbe, E.; Brock, R.; Budev, M.; Xu, M.; Demirjian, S.; Schreiber, M.J.; Stephany, B. Short-term and long-term outcomes of acute kidney injury after lung transplantation. J. Heart Lung Transplant. 2012, 31, 244–251. [Google Scholar] [CrossRef]
- Hennessy, S.A.; Gillen, J.R.; Hranjec, T.; Kozower, B.D.; Jones, D.R.; Kron, I.L.; Lau, C.L. Influence of hemodialysis on clinical outcomes after lung transplantation. J. Surg. Res. 2013, 183, 916–921. [Google Scholar] [CrossRef]
- Shigemura, N.; D’Cunha, J.; Bhama, J.K.; Shiose, A.; El Ela, A.A.; Hackmann, A.; Zaldonis, D.; Toyoda, Y.; Pilewski, J.M.; Luketich, J.D.; et al. Lobar Lung Transplantation: A Relevant Surgical Option in the Current Era of Lung Allocation Score. Ann. Thorac. Surg. 2013, 96, 451–456. [Google Scholar] [CrossRef]
- Silhan, L.L.; Shah, P.D.; Chambers, D.C.; Snyder, L.D.; Riise, G.C.; Wagner, C.L.; Hellström-Lindberg, E.; Orens, J.B.; Mewton, J.F.; Danoff, S.K.; et al. Lung transplantation in telomerase mutation carriers with pulmonary fibrosis. Eur. Respir. J. 2014, 44, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Tokman, S.; Singer, J.P.; Devine, M.S.; Westall, G.P.; Aubert, J.-D.; Tamm, M.; Snell, G.I.; Lee, J.S.; Goldberg, H.J.; Kukreja, J.; et al. Clinical outcomes of lung transplant recipients with telomerase mutations. J. Heart Lung Transplant. 2015, 34, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Carillo, C.; Pecoraro, Y.; Anile, M.; Mantovani, S.; Oliva, A.; D’Abramo, A.; Amore, D.; Pagini, A.; De Giacomo, T.; Pugliese, F.; et al. Evaluation of Renal Function in Patients Undergoing Lung Transplantation. Transplant. Proc. 2017, 49, 699–701. [Google Scholar] [CrossRef] [PubMed]
- Sikma, M.A.; Hunault, C.C.; Van De Graaf, E.A.; Verhaar, M.C.; Kesecioglu, J.; De Lange, D.W.; Meulenbelt, J. High tacrolimus blood concentrations early after lung transplantation and the risk of kidney injury. Eur. J. Clin. Pharmacol. 2017, 73, 573–580. [Google Scholar] [CrossRef]
- Newton, C.A.; Kozlitina, J.; Lines, J.R.; Kaza, V.; Torres, F.; Garcia, C.K. Telomere length in patients with pulmonary fibrosis associated with chronic lung allograft dysfunction and post-lung transplantation survival. J. Heart Lung Transplant. 2017, 36, 845–853. [Google Scholar] [CrossRef]
- Banga, A.; Mohanka, M.; Mullins, J.; Bollineni, S.; Kaza, V.; Tanriover, B.; Torres, F. Characteristics and outcomes among patients with need for early dialysis after lung transplantation surgery. Clin. Transplant. 2017, 31, e13106. [Google Scholar] [CrossRef]
- Cosgun, T.; Tomaszek, S.; Opitz, I.; Wilhelm, M.; Schuurmans, M.M.; Weder, W.; Inci, I. Single-center experience with intraoperative extracorporeal membrane oxygenation use in lung transplantation. Int. J. Artif. Organs 2017. [Google Scholar] [CrossRef]
- Ahmad, O.; Shafii, A.E.; Mannino, D.M.; Choate, R.; Baz, M.A. Impact of donor lung pathogenic bacteria on patient outcomes in the immediate post-transplant period. Transpl. Infect. Dis. 2018, 20, e12986. [Google Scholar] [CrossRef]
- Iyengar, A.; Kwon, O.J.; Sanaiha, Y.; Eisenring, C.; Biniwale, R.; Ross, D.; Ardehali, A. Lung transplantation in the Lung Allocation Score era: Medium-term analysis from a single center. Clin. Transplant. 2018, 32, e13298. [Google Scholar] [CrossRef]
- Ri, H.S.; Son, H.J.; Oh, H.B.; Kim, S.Y.; Park, J.Y.; Kim, J.Y.; Choi, Y.J. Inhaled nitric oxide therapy was not associated with postoperative acute kidney injury in patients undergoing lung transplantation: A retrospective pilot study. Medicine 2018, 97, e10915. [Google Scholar] [CrossRef]
- Calabrese, D.R.; Florez, R.; Dewey, K.; Hui, C.; Torgerson, D.; Chong, T.; Faust, H.; Rajalingam, R.; Hays, S.R.; Golden, J.A.; et al. Genotypes associated with tacrolimus pharmacokinetics impact clinical outcomes in lung transplant recipients. Clin. Transplant. 2018, 32, e13332. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.; Fossi, A.; Marchetti, L.; Lanzarone, N.; Sisi, S.; Refini, R.M.; Sestini, P.; Luzzi, L.; Paladini, P.; Rottoli, P. Postoperative acute kidney injury in lung transplant recipients. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Shashaty, M.G.S.; Forker, C.M.; Miano, T.A.; Wu, Q.; Yang, W.; Oyster, M.L.; Porteous, M.K.; Cantu, E.E., III; Diamond, J.M.; Christie, J.D. The association of post-lung transplant acute kidney injury with mortality is independent of primary graft dysfunction: A cohort study. Clin. Transplant. 2019, e13678. [Google Scholar] [CrossRef]
- Sharma, P.; Welch, K.; Eikstadt, R.; Marrero, J.A.; Fontana, R.J.; Lok, A.S. Renal outcomes after liver transplantation in the model for end-stage liver disease era. Liver Transplant. 2009, 15, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Chatila, W.M.; Furukawa, S.; Gaughan, J.P.; Criner, G.J. Respiratory failure after lung transplantation. Chest 2003, 123, 165–173. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Husain-Syed, F.; Slutsky, A.S.; Ronco, C. Lung–Kidney Cross-Talk in the Critically Ill Patient. Am. J. Respir. Crit. Care Med. 2016, 194, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, R.; Mulloy, E.; O’Neill, S. Acute effects of hypoxaemia, hyperoxaemia and hypercapnia on renal blood flow in normal and renal transplant subjects. Eur. Respir. J. 1998, 12, 653–657. [Google Scholar] [CrossRef]
- Hemlin, M.; Ljungman, S.; Carlson, J.; Maljukanovic, S.; Mobini, R.; Bech-Hanssen, O.; Skoogh, B.-E.; Skoogh, B. The effects of hypoxia and hypercapnia on renal and heart function, haemodynamics and plasma hormone levels in stable COPD patients. Clin. Respir. J. 2007, 1, 80–90. [Google Scholar] [CrossRef]
- Sharkey, R.A.; Mulloy, E.M.; O’Neill, S.J. The Acute Effects of Oxygen and Carbon Dioxide on Renal Vascular Resistance in Patients with an Acute Exacerbation of COPD. Chest 1999, 115, 1588–1592. [Google Scholar] [CrossRef]
- Anand, I.S.; Chandrashekhar, Y.; Ferrari, R.; Sarma, R.; Guleria, R.; Jindal, S.K.; Wahi, P.L.; Poole-Wilson, P.A.; Harris, P. Pathogenesis of congestive state in chronic obstructive pulmonary disease. Studies of body water and sodium, renal function, hemodynamics, and plasma hormones during edema and after recovery. Circulation 1992, 86, 12–21. [Google Scholar] [CrossRef]
- Sharkey, R.A.; Mulloy, E.M.; Kilgallen, I.A.; O’Neill, S.J. Renal functional reserve in patients with severe chronic obstructive pulmonary disease. Thorax 1997, 52, 411–415. [Google Scholar] [CrossRef] [PubMed]
- MacNee, W. Pathophysiology of cor pulmonale in chronic obstructive pulmonary disease. Part One. Am. J. Respir. Crit. Care Med. 1994, 150, 833–852. [Google Scholar] [CrossRef] [PubMed]
- Magouliotis, D.E.; Tasiopoulou, V.S.; Svokos, A.A.; Svokos, K.A.; Zacharoulis, D. Extracorporeal membrane oxygenation versus cardiopulmonary bypass during lung transplantation: A meta-analysis. Gen. Thorac. Cardiovasc. Surg. 2018, 66, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Srivali, N.; O′corragain, O.A.; Edmonds, P.J.; Ratanapo, S.; Spanuchart, I.; Erickson, S.B. Comparison of Renal Outcomes in Off-Pump Versus On-Pump Coronary Artery Bypass Grafting: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Nephrology 2015, 20, 727–735. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Salim, S.A.; Ungprasert, P.; Wijarnpreecha, K.; et al. Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 372. [Google Scholar] [CrossRef]
- Ojo, A.O.; Held, P.J.; Port, F.K.; Wolfe, R.A.; Leichtman, A.B.; Young, E.W.; Arndorfer, J.; Christensen, L.; Merion, R.M. Chronic Renal Failure after Transplantation of a Nonrenal Organ. N. Engl. J. Med. 2003, 349, 931–940. [Google Scholar] [CrossRef]
- Grimm, J.C.; Lui, C.; Kilic, A.; Valero, V., 3rd; Sciortino, C.M.; Whitman, G.J.; Shah, A.S. A risk score to predict acute renal failure in adult patients after lung transplantation. Ann. Thorac. Surg. 2015, 99, 251–257. [Google Scholar] [CrossRef]
- Imai, Y.; Parodo, J.; Kajikawa, O.; De Perrot, M.; Fischer, S.; Edwards, V.; Cutz, E.; Liu, M.; Keshavjee, S.; Martin, T.R.; et al. Injurious Mechanical Ventilation and End-Organ Epithelial Cell Apoptosis and Organ Dysfunction in an Experimental Model of Acute Respiratory Distress Syndrome. JAMA 2003, 289, 2104–2112. [Google Scholar] [CrossRef]
- Koyner, J.L.; Murray, P.T. Mechanical ventilation and the kidney. Blood Purif. 2010, 29, 52–68. [Google Scholar] [CrossRef]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Ojo, A.O. Renal Disease in Recipients of Nonrenal Solid Organ Transplantation. Semin. Nephrol. 2007, 27, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Clajus, C.; Hanke, N.; Gottlieb, J.; Stadler, M.; Weismüller, T.J.; Strassburg, C.P.; Bröcker, V.; Bara, C.; Lehner, F.; Drube, J.; et al. Renal Comorbidity After Solid Organ and Stem Cell Transplantation. Arab. Archaeol. Epigr. 2012, 12, 1691–1699. [Google Scholar] [CrossRef] [PubMed]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).